A Portrait of SARS-CoV-2 Infection in Patients Undergoing Hematopoietic Cell Transplantation: A Systematic Review of the Literature

Abstract
:1. Introduction
2. Methods
2.1. Literature Search Strategy
2.2. Eligibility Criteria
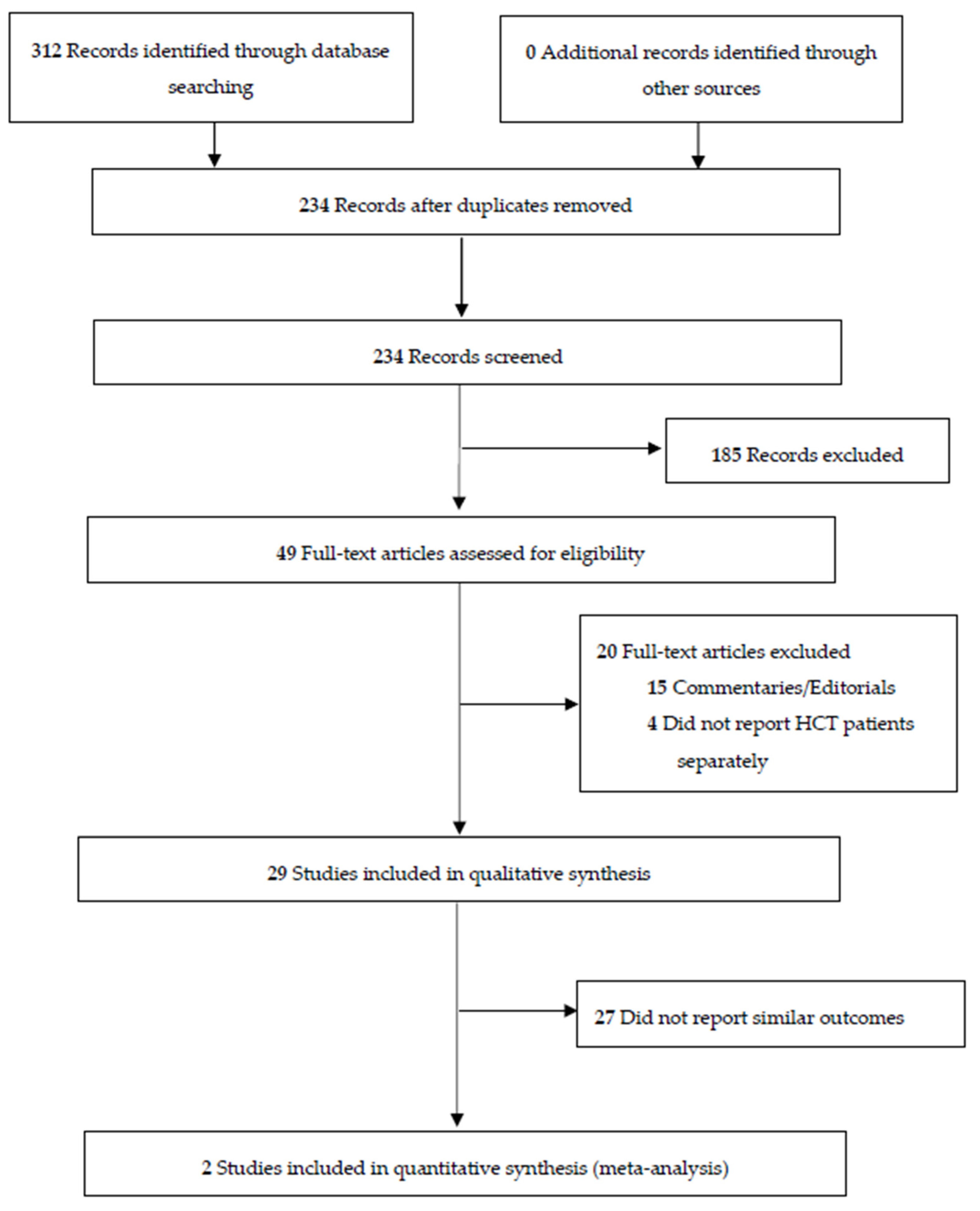
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias
2.6. Meta-Analysis
3. Results
3.1. Clinical Characteristics
3.1.1. Adult Population
3.1.2. Pediatric Population
3.2. Predictors of Mortality Reported in Identified Studies
3.2.1. Age
3.2.2. Sex
3.2.3. Time from Transplant
3.2.4. Autologous Versus Allogeneic HCT
3.2.5. Comorbidities
3.2.6. Underlying Disease
3.2.7. Immunosuppressive Treatment
3.2.8. Cytopenias
3.3. Other Factors
3.4. Treatment
3.5. Risk of Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef]
- MacKenzie, J.S.; Smith, D.W. COVID-19: A novel zoonotic disease caused by a coronavirus from China: What we know and what we don’t. Microbiol. Aust. 2020, 41, 45–50. [Google Scholar] [CrossRef]
- Esiashvili, N.; Pulsipher, M.A. Hematopoietic stem cell transplantation. In: Pediatric Oncology. N. Engl. J. Med. 2018, 354, 1813–1826. [Google Scholar] [CrossRef]
- Angelucci, E.; Matthes-Martin, S.; Baronciani, D.; Bernaudin, F.; Bonanomi, S.; Cappellini, M.D.; Dalle, J.H.; Di Bartolomeo, P.; de Heredia, C.D.; Dickerhoff, R.; et al. Hematopoietic stem cell transplantation in thalassemia major and sickle cell disease: Indications and management recommendations from an international expert panel. Haematologica 2014, 99, 811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchlaka, M.N.; Redelman, D.; Murphy, W.J. Immunotherapy following hematopoietic stem cell transplantation: Potential for synergistic effects. Immunotherapy 2010, 2, 399–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ASTCT. ASH-ASTCT COVID-19 Vaccination for HCT and CAR T Cell Recipients. 2021. Available online: https://www.hematology.org/covid-19/ash-astct-covid-19-vaccination-for-hct-and-car-t-cell-recipients (accessed on 21 December 2021).
- Malard, F.; Genthon, A.; Brissot, E.; van de Wyngaert, Z.; Marjanovic, Z.; Ikhlef, S.; Banet, A.; Lapusan, S.; Sestilli, S.; Corre, E.; et al. COVID-19 outcomes in patients with hematologic disease. Bone Marrow Transplant. 2020, 55, 2180–2184. [Google Scholar] [CrossRef] [PubMed]
- Rickman, H.M.; Rampling, T.; Shaw, K.; Martinez-Garcia, G.; Hail, L.; Coen, P.; Shahmanesh, M.; Shin, G.Y.; Nastouli, E.; Houlihan, C.F. Nosocomial Transmission of Coronavirus Disease 2019: A Retrospective Study of 66 Hospital-acquired Cases in a London Teaching Hospital. Clin. Infect. Dis. 2020, 72, 690–693. [Google Scholar] [CrossRef]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control COVID-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef]
- Knaus, H.A.; Rabitsch, W.; Buchtele, N.; Cserna, J.; Wohlfarth, P. Autologous hematopoietic stem cell transplantation with concomitant SARS-CoV-2 infection. Ann. Hematol. 2021, 1–4. [Google Scholar] [CrossRef] [PubMed]
- CIHCTR. Chinese Clinical Trial Registry. Available online: https://www.chictr.org.cn/enindex.aspx (accessed on 21 December 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Altuntas, F.; Ata, N.; Yigenoglu, T.N.; Bascı, S.; Dal, M.S.; Korkmaz, S.; Namdaroglu, S.; Basturk, A.; Hacıbekiroglu, T.; Dogu, M.H.; et al. COVID-19 in hematopoietic cell transplant recipients. Bone Marrow Transplant. 2020, 56, 952–955. [Google Scholar] [CrossRef] [PubMed]
- Camargo, J.F.; Mendoza, M.A.; Lin, R.; Moroz, I.V.; Anderson, A.D.; Morris, M.I.; Natori, Y.; Natori, A.; Raja, M.; Lekakis, L.; et al. Clinical presentation and outcomes of COVID-19 following hematopoietic cell transplantation and cellular therapy. Transpl. Infect. Dis. 2021, 23, e13625. [Google Scholar] [CrossRef]
- Coll, E.; Fernández-Ruiz, M.; Sánchez-Álvarez, J.E.; Martínez-Fernández, J.R.; Crespo, M.; Gayoso, J.; Bada-Bosch, T.; Oppenheimer, F.; Moreso, F.; López-Oliva, M.O.; et al. COVID-19 in transplant recipients: The Spanish experience. Am. J. Transplant. 2021, 21, 1825–1837. [Google Scholar] [CrossRef]
- El Fakih, R.; Haroon, A.; Alfraih, F.; Al-Khabori, M.K.; Alzahrani, M.; Alhuraiji, A.; Hamadah, A.; AlJohani, N.I.; Alahmari, B.; Essa, M.F.; et al. Clinical course and outcomes of COVID-19 in hematopoietic cell transplant patients, a regional report from the Middle East. Bone Marrow Transplant. 2021, 56, 2144–2151. [Google Scholar] [CrossRef] [PubMed]
- Karataş, A.; İnkaya, A.Ç.; Demiroğlu, H.; Aksu, S.; Haziyev, T.; Çınar, O.E.; Alp, A.; Uzun, Ö.; Sayınalp, N.; Göker, H. Prolonged viral shedding in a lymphoma patient with COVID-19 infection receiving convalescent plasma. Transfus. Apher. Sci. 2020, 59, 102871. [Google Scholar] [CrossRef]
- Ljungman, P.; de la Camara, R.; Mikulska, M.; Tridello, G.; Aguado, B.; Al Zahrani, M.; Apperley, J.; Berceanu, A.; Bofarull, R.M.; Calbacho, M.; et al. COVID-19 and stem cell transplantation; results from an EHCT and GETH multicenter prospective survey. Leukemia 2021, 35, 2885–2894. [Google Scholar] [CrossRef]
- Piñana, J.L.; Martino, R.; García-García, I.; Parody, R.; Morales, M.D.; Benzo, G.; Gómez-Catalan, I.; Coll, R.; De La Fuente, I.; Luna, A.; et al. Risk factors and outcome of COVID-19 in patients with hematological malignancies. Exp. Hematol. Oncol. 2020, 9, 21. [Google Scholar] [CrossRef]
- Shah, G.L.; DeWolf, S.; Lee, Y.J.; Tamari, R.; Dahi, P.B.; Lavery, J.A.; Ruiz, J.; Devlin, S.M.; Cho, C.; Peled, J.U.; et al. Favorable outcomes of COVID-19 in recipients of hematopoietic cell transplantation. J. Clin. Investig. 2020, 130, 6656–6667. [Google Scholar] [CrossRef]
- Sharma, A.; Bhatt, N.S.; St Martin, A.; Abid, M.B.; Bloomquist, J.; Chemaly, R.F.; Dandoy, C.; Gauthier, J.; Gowda, L.; Perales, M.A.; et al. Clinical characteristics and outcomes of COVID-19 in haematopoietic stem-cell transplantation recipients: An observational cohort study. Lancet Haematol. 2021, 8, e185–e193. [Google Scholar] [CrossRef]
- Varma, A.; Kosuri, S.; Ustun, C.; Ibrahim, U.; Moreira, J.; Bishop, M.R.; Nathan, S.; Mehta, J.; Moncayo, D.; Heng, J.; et al. COVID-19 infection in hematopoietic cell transplantation: Age, time from transplant and steroids matter. Leukemia 2020, 34, 2809–2812. [Google Scholar] [CrossRef] [PubMed]
- Xhaard, A.; Xhaard, C.; D’Aveni, M.; Salvator, H.; Chabi, M.L.; Berceanu, A.; Coman, T.; Beguin, Y.; Chalandon, Y.; Poiré, X.; et al. Risk factors for a severe form of COVID-19 after allogeneic haematopoietic stem cell transplantation: A Societe Francophone de Greffe de Moelle et de Therapie cellulaire (SFGM-TC) multicentre cohort study. Br. J. Haematol. 2021, 192, e121–e124. [Google Scholar] [CrossRef] [PubMed]
- Al Yazidi, L.S.; Al Rawas, A.; Wali, Y. COVID-19 in Children With Cancers and Post-Hematopoietic Stem Cell Transplantation (HSCT) in Oman. J. Pediatr. Hematol. Oncol. 2021, 43, e741–e742. [Google Scholar] [CrossRef] [PubMed]
- Balashov, D.; Trakhtman, P.; Livshits, A.; Kovalenko, I.; Tereshenko, G.; Solopova, G.; Petraikina, E.; Maschan, A.; Novichkova, G. SARS-CoV-2 convalescent plasma therapy in pediatric patient after hematopoietic stem cell transplantation. Transfus. Apher. Sci. 2021, 60, 102983. [Google Scholar] [CrossRef] [PubMed]
- Bisogno, G.; Provenzi, M.; Zama, D.; Tondo, A.; Meazza, C.; Colombini, A.; Galaverna, F.; Compagno, F.; Carraro, F.; De Santis, R.; et al. Clinical Characteristics and Outcome of Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Italian Pediatric Oncology Patients: A Study From the Infectious Diseases Working Group of the Associazione Italiana di Oncologia e Ematologia Pediatrica. J. Pediatric. Infect. Dis. Soc. 2020, 9, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Doná, D.; Torres Canizales, J.; Benetti, E.; Cananzi, M.; De Corti, F.; Calore, E.; Hierro, L.; Ramos Boluda, E.; Melgosa Hijosa, M.; Garcia Guereta, L.; et al. Pediatric transplantation in Europe during the COVID-19 pandemic: Early impact on activity and healthcare. Clin. Transplant. 2020, 34, e14063. [Google Scholar] [CrossRef]
- Faura, A.; Rives, S.; Lassaletta, Á.; Sebastián, E.; Madero, L.; Huerta, J.; García-Morín, M.; Martínez, A.P.; Sisinni, L.; Astigarraga, I.; et al. Initial report on Spanish pediatric oncologic, hematologic, and post stem cell transplantation patients during SARS-CoV-2 pandemic. Pediatr. Blood Cancer 2020, 67, e28557. [Google Scholar] [CrossRef]
- Fisler, G.; Haimed, A.; Levy, C.F.; Stiles, J.; Capone, C.A.; Fish, J.D.; Brochstein, J.A.; Taylor, M.D. Severe Coronavirus Disease 2019 Infection in an Adolescent Patient After Hematopoietic Stem Cell Transplantation. Chest 2020, 158, e139–e142. [Google Scholar] [CrossRef]
- García-Salido, A.; Leoz-Gordillo, I.; de Azagra-Garde, A.M.; Nieto-Moro, M.; Iglesias-Bouzas, M.I.; García-Teresa, M.Á.; Cabrero-Hernández, M.; Caro-Patón, G.D.L.; Valdovinos, A.G.; González-Brabin, A.; et al. Children in Critical Care Due to Severe Acute Respiratory Syndrome Coronavirus 2 Infection: Experience in a Spanish Hospital. Pediatr. Crit. Care Med. 2020, 21, e576–e580. [Google Scholar] [CrossRef]
- Alicea Marrero, M.M.; Silio, M.; McQueen-Amaker, K.; Español, M.; Velez, M.; LeBlanc, Z. Posthematopoietic stem cell transplant COVID-19 infection in a pediatric patient with IPEX syndrome. Pediatr. Blood Cancer 2020, e28578. [Google Scholar] [CrossRef]
- Nazon, C.; Velay, A.; Radosavljevic, M.; Fafi-Kremer, S.; Paillard, C. Coronavirus disease 2019 3 months after hematopoietic stem cell transplant: A pediatric case report. Pediatr. Blood Cancer 2020, e28545. [Google Scholar] [CrossRef]
- Rossoff, J.; Patel, A.B.; Muscat, E.; Kociolek, L.K.; Muller, W.J. Benign course of SARS-CoV-2 infection in a series of pediatric oncology patients. Pediatr. Blood Cancer 2020, e28504. [Google Scholar] [CrossRef]
- Zamperlini-Netto, G.; Fernandes, J.F.; Garcia, J.L.; Ribeiro, A.A.F.; Camargo, L.F.A.; de Moraes Terra, C.; Hamerschlak, N. COVID-19 after hematopoietic stem cell transplantation: Report of two children. Bone Marrow Transplant. 2020, 56, 713–715. [Google Scholar] [CrossRef]
- Jarmoliński, T.; Matkowska-Kocjan, A.; Rosa, M.; Olejnik, I.; Gorczyńska, E.; Kałwak, K.; Ussowicz, M. SARS-CoV-2 viral clearance during bone marrow aplasia after allogeneic hematopoietic stem cell transplantation-A case report. Pediatr. Transplant. 2020, 25, e13875. [Google Scholar] [CrossRef]
- André, N.; Rouger-Gaudichon, J.; Brethon, B.; Phulpin, A.; Thébault, É.; Pertuisel, S.; Gandemer, V. COVID-19 in pediatric oncology from French pediatric oncology and hematology centers: High risk of severe forms? Pediatr. Blood Cancer 2020, e28392. [Google Scholar] [CrossRef] [PubMed]
- Barhoom, D.; Mohseni, R.; Hamidieh, A.A.; Mohammadpour, M.; Sharifzadeh, M.; Navaeian, A.; Taebi, S.; Behfar, M. Clinical Effects of COVID-19 on Hematopoietic Stem Cell Transplant Outcomes in Pediatric Patients. Exp. Clin. Transplant. Off. J. Middle East Soc. Organ Transplant. 2021, 19, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Sarbay, H.; Atay, A.; Malbora, B. COVID-19 Infection in a Child with Thalassemia Major after Hematopoietic Stem Cell Transplant. J. Pediatr. Hematol. Oncol. 2021, 43, 33–34. [Google Scholar] [CrossRef] [PubMed]
- Vicent, M.G.; Martinez, A.P.; Del Castillo, M.T.; Molina, B.; Sisini, L.; Morón-Cazalilla, G.; Díaz, M.Á. COVID-19 in pediatric hematopoietic stem cell transplantation: The experience of Spanish Group of Transplant (GETMON/GETH). Pediatr. Blood Cancer 2020, e28514. [Google Scholar] [CrossRef]
- Rouger-Gaudichon, J.; Thébault, E.; Félix, A.; Phulpin, A.; Paillard, C.; Alimi, A.; Brethon, B.; Gouache, E.; Raimbault, S.; de Berranger, E.; et al. Impact of the first wave of COVID-19 on pediatric oncology and hematology: A report from the french society of pediatric oncology. Cancers 2020, 12, 3398. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, K.Y.; Kim, T.O.; Doherty, E.E.; Pfeiffer, T.M.; Qasim, S.L.; Suell, M.N.; Yates, A.M.; Blaney, S.M. COVID-19 outcomes in a large pediatric hematology-oncology center in Houston, Texas. Pediatr. Hematol. Oncol. 2021, 38, 695–706. [Google Scholar] [CrossRef]
- Wells, G.A.; Connell, D.O.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2014; pp. 2–4. [Google Scholar] [CrossRef]
- Islam, N.; Ebrahimzadeh, S.; Salameh, J.P.; Kazi, S.; Fabiano, N.; Treanor, L.; Absi, M.; Hallgrimson, Z.; Leeflang, M.M.; Hooft, L.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2020, 11, CD013639. [Google Scholar] [CrossRef]
- Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; Prudon, B.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate COVID-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2020, 384, 497–511. [Google Scholar] [CrossRef]
- Elsawah, H.K.; Elsokary, M.A.; Abdallah, M.S.; El Shafie, A.H. Efficacy and safety of remdesivir in hospitalized COVID-19 patients: Systematic review and meta-analysis including network meta-analysis. Rev. Med. Virol. 2020, 31, e2187. [Google Scholar] [CrossRef]
- Stauffer, W.M.; Alpern, J.D.; Walker, P.F. COVID-19 and Dexamethasone: A Potential Strategy to Avoid Steroid-Related Strongyloides Hyperinfection. JAMA 2020, 324, 623–624. [Google Scholar] [CrossRef] [PubMed]
- Chappell, L.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19—Preliminary Report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- van Paassen, J.; Vos, J.S.; Hoekstra, E.M.; Neumann, K.M.I.; Boot, P.C.; Arbous, S.M. Corticosteroid use in COVID-19 patients: A systematic review and meta-analysis on clinical outcomes. Crit. Care 2020, 24, 696. [Google Scholar] [CrossRef]
- Malek, A.E.; Adachi, J.A.; Mulanovich, V.E.; Sassine, J.; Raad, I.I.; McConn, K.; Seiler, G.T.; Dhal, U.; Khawaja, F.; Chemaly, R.F. Immune reconstitution and severity of COVID-19 among hematopoietic cell transplant recipients. Transpl. Infect. Dis. 2021, 23, e13606. [Google Scholar] [CrossRef]
- Kanellopoulos, A.; Ahmed, M.Z.; Kishore, B.; Lovell, R.; Horgan, C.; Paneesha, S.; Lloyd, R.; Salhan, B.; Giles, H.; Chauhan, S.; et al. COVID-19 in bone marrow transplant recipients: Reflecting on a single centre experience. Br. J. Haematol. 2020, 190, e67–e70. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | n (Age Range) | Male, n (%) | Time Since Transplant, Mean Months (Range) | Graft Type, (%) Auto/Allo/CART | GVHD History, n (% of Allos) | ICU (%) | Deaths (%) |
|---|---|---|---|---|---|---|---|
| (14) | 32 (19–74) | 25 (78) | NR | 20/12/0 | NR | 7 (22) | 5 (16) |
| (15) | 28 (50–67) * | 16 (57) | 21.9 (11.1–42.5) | 12/15/1 | 7 (47) | 7 (25) | 5 (18) |
| (16) | 54 (0–73.5) | 31 (57) | 15.6 (0.3–228) | 0/54/0 | 54 (100) | 13 (24) | 13 (24) |
| (17) | 113 (34–64) | 64 (57) | 18 (4–53), Auto 15 (7–37), Allo | 42/71/0 | NR | 9 (8.0) | 18 (16) |
| (18) | 91 (NR) | 53 (58) | 14.9 (16.3–38.9) | 39/52/0 | 12 (23) | 13 (14) | 4 (4.4) |
| (19) | 33 (27–71) | 21 (64) | NR | 19/14/0 | 6 (43) | 4 (12) | 3 (9.0) |
| (20) | 382 (1–81.6) | 236 (62) | 24.6 (−0.9–350), Auto 15.8 (0.2–293), Allo | 146/236/0 | 89 (38) | 86 (22) | 107 (28) |
| (21) | 123 (1–75) | 74 (60) | 26.3, Auto14.7, Allo | 58/65/0 | NR | NR | 25 (20) |
| (22) | 77 (52–68) | 49 (64) | <6 months (n = 10) 6–12 months (n = 10), 12–36 months (n = 27), >36 months (n = 30) | 37/35/5 | 17 (49) | NR | 17 (22) |
| (23) | 318 (30–65) | 188 (59) | 23 (8–51), Auto 17 (8–46), Allo | 134/184/0 | 126 (68) | NR | 66 (21) ** |
| (24) | 34 (24–76) | 22 (65) | 17.4 (1–248.7) | 14/20/0 | 9 (45) | 11 (32) | 7 (21) |
| TOTAL | 1285 | 779 (60.6) | (−0.9–350) | 521 (40.5%)/ 758 (59.0%)/ 6 (0.5%) | 320/610 (52.5%) | 150/767 (19.6%) | 272/1285 (21.2%) |
| Study | n (Age Range) | Male, n (%) | Time Since Transplant, (Months) | Graft | GVHD History, n (%) | ICU (%) | Deaths (%) |
|---|---|---|---|---|---|---|---|
| (25) | 3 (NR) | NR | 25, 41, 41 | NR | NR | 0 (0%) | 0 (0%) |
| (26) | 1 (0.6) | 0 | 3 | Allo | 1 | NR | 0 (0%) |
| (27) | 3 (NR) | NR | 5–22 | Allo | NR | NR | 0 (0%) |
| (28) | 6 (NR) | NR | NR | NR | NR | 0 (0%) | 0 (0%) |
| (29) | 8 (NR) | NR | NR | NR | NR | NR | 2 (25%) |
| (30) | 1 (15) | 0 | 0.3 | Allo | 0 | 1 (100%) | 0 (0%) |
| (31) | 1 (8) | 1 | NR | Allo | NR | 1 (100%) | 0 (0%) |
| (32) | 1 (8) | 1 | 0.7 | Allo | 0 | NR | 1 (100%) |
| (33) | 1 (17) | 0 | 3 | NR | 1 | NR | 0 (0%) |
| (34) | 1 (5) | 1 | 5 | Allo | 1 | NR | 0 (0%) |
| (35) | 2 (2–17) | 1 | 5, 6 | Allo | 1 (50) | NR | 0 (0%) |
| (36) | 1 (9) | 0 | 0 | Allo | 0 | NR | 0 (0%) |
| (37) | 2 (5,13) | 1 | 2 | Allo | NR | 2 (100%) | 0 (0%) |
| (38) | 4 (3–10) | 3 | 0.6, 13, 15, 16 | Allo | 3 (75) | 1 (25%) | 1 (25%) |
| (39) | 1 (16) | 0 | 5 | Allo | 1 | NR | 0 (0%) |
| (40) | 8 (1–12) | 7 | 1–24 | Allo | 3 (38) | NR | 1 (12.5%) |
| (41) | 4 (NR) | NR | NR | NR | NR | 2 (50%) | 0 (0%) |
| (42) | 6 (1.9–12.6) | 4 | NR | Allo | NR | 0 (0%) | 0 (0%) |
| TOTAL | 54 | 19/30 (63) | 0–24 | 13/13 (100%) | 11/21 (52%) | 7/27 (26%) | 5/54 (9.3%) |
| Treatment | Adult HCT Patients, n (%) | Pediatric HCT Patients, n (%) |
|---|---|---|
| Hydroxychloroquine (HCQ) | 274 (21.3) | 15 (27.8) |
| Azithromycin (AZT) | 92 (7.2) | 9 (16.7) |
| Corticosteroids | 144 (11.2) | 5 (9.3) |
| Tocilizumab | 87 (6.8) | 5 (9.3) |
| Convalescent plasma | 42 (3.3) | 1 (1.9) |
| Remdesivir | 74 (5.8) | 6 (11.1) |
| Immune globulin * | 7 (0.5) | 2 (3.7) |
| Lopinavir/ritonavir | 52 (4.0) | 3 (5.6) |
| Ruxilotinib | 4 (0.3) | 0 (0.0) |
| Anakinra | 20 (1.6) | 2 (3.7) |
| Favipiravir | 39 (3.0) | 0 (0.0) |
| Oseltamivir | 18 (1.4) | 2 (3.7) |
| Methylprednisolone | 14 (1.1) | 1 (1.9) |
| Protease inhibitors | 47 (3.7) | 0 (0.0) |
| HCQ + AZT | 26 (2.0) | 0 (0.0) |
| HCQ + Lopinavir/Ritonavir | 22 (1.7) | 0 (0.0) |
| AZT + Lopinavir/Ritonavir | 14 (1.1) | 0 (0.0) |
| HCQ + AZT + Lopinavir/Ritonavir | 9 (0.7) | 0 (0.0) |
| Acyclovir or Valacyclovir | 23 (1.8) | 0 (0.0) |
| HCQ + Favipiravir | 5 (0.4) | 0 (0.0) |
| Siltuximab | 3 (0.2) | 1 (1.9) |
| No specific treatment | 268 (20.9) | 30 (55.6) |
| Other ** | 93 ** (7.2) | 22 *** (40.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bailey, A.J.M.; Kirkham, A.M.; Monaghan, M.; Shorr, R.; Buchan, C.A.; Bredeson, C.; Allan, D.S. A Portrait of SARS-CoV-2 Infection in Patients Undergoing Hematopoietic Cell Transplantation: A Systematic Review of the Literature. Curr. Oncol. 2022, 29, 337-349. https://doi.org/10.3390/curroncol29010030
Bailey AJM, Kirkham AM, Monaghan M, Shorr R, Buchan CA, Bredeson C, Allan DS. A Portrait of SARS-CoV-2 Infection in Patients Undergoing Hematopoietic Cell Transplantation: A Systematic Review of the Literature. Current Oncology. 2022; 29(1):337-349. https://doi.org/10.3390/curroncol29010030
Chicago/Turabian StyleBailey, Adrian J. M., Aidan M. Kirkham, Madeline Monaghan, Risa Shorr, C. Arianne Buchan, Christopher Bredeson, and David S. Allan. 2022. "A Portrait of SARS-CoV-2 Infection in Patients Undergoing Hematopoietic Cell Transplantation: A Systematic Review of the Literature" Current Oncology 29, no. 1: 337-349. https://doi.org/10.3390/curroncol29010030