Impact of Body Composition on Postoperative Outcomes in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
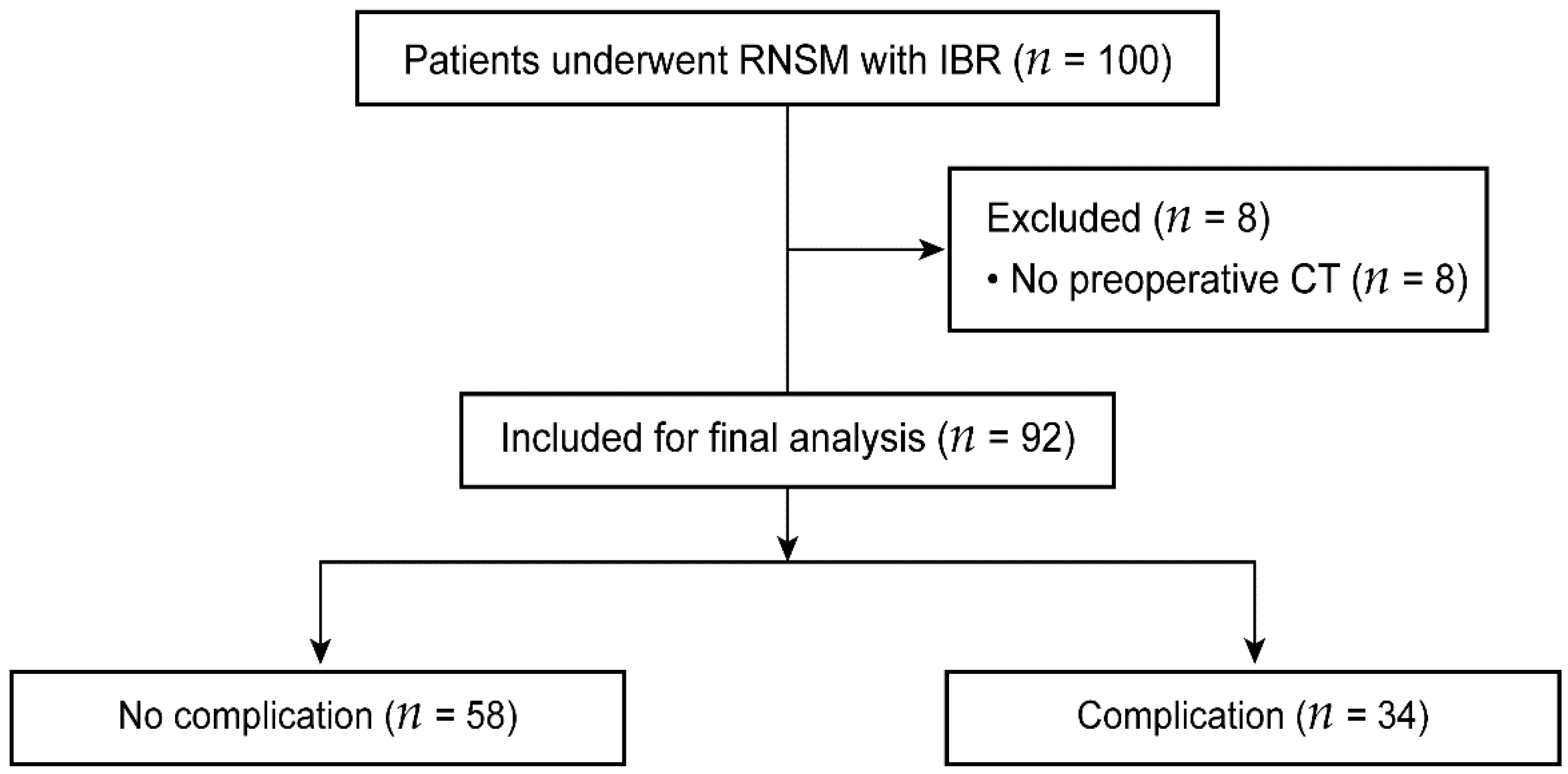
2.1. Patient Population
2.2. Procedures
2.3. Complications
2.4. Body Composition Assessment on CT Images
2.5. Data Collection
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahn, S.J.; Woo, T.Y.; Lee, D.W.; Lew, D.H.; Song, S.Y. Nipple-areolar complex ischemia and necrosis in nipple-sparing mastectomy. Eur. J. Surg. Oncol. 2018, 44, 1170–1176. [Google Scholar] [CrossRef]
- Moyer, H.R.; Ghazi, B.; Daniel, J.R.; Gasgarth, R.; Carlson, G.W. Nipple-Sparing Mastectomy Technical Aspects and Aesthetic Outcomes. Ann. Plast. Surg. 2012, 68, 446–450. [Google Scholar] [CrossRef] [PubMed]
- de Alcantara Filho, P.; Capko, D.; Barry, J.M.; Morrow, M.; Pusic, A.; Sacchini, V.S. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: The Memorial Sloan-Kettering Cancer Center experience. Ann. Surg. Oncol. 2011, 18, 3117–3122. [Google Scholar] [CrossRef]
- Crowe, J.P.; Patrick, R.J.; Yetman, R.J.; Djohan, R. Nipple-sparing mastectomy update: One hundred forty-nine procedures and clinical outcomes. Arch. Surg. 2008, 143, 1106–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frey, J.D.; Salibian, A.A.; Karp, N.S.; Choi, M. The Impact of Mastectomy Weight on Reconstructive Trends and Outcomes in Nipple-Sparing Mastectomy: Progressively Greater Complications with Larger Breast Size. Plast. Reconstr. Surg. 2018, 141, 795e–804e. [Google Scholar] [CrossRef] [PubMed]
- Chirappapha, P.; Petit, J.Y.; Rietjens, M.; De Lorenzi, F.; Garusi, C.; Martella, S.; Barbieri, B.; Gottardi, A.; Andrea, M.; Giuseppe, L.; et al. Nipple sparing mastectomy: Does breast morphological factor related to necrotic complications? Plast. Reconstr. Surg. Glob. Open 2014, 2, e99. [Google Scholar] [CrossRef] [PubMed]
- Colwell, A.S.; Tessler, O.; Lin, A.M.; Liao, E.; Winograd, J.; Cetrulo, C.L.; Tang, R.; Smith, B.L.; Austen, W.G. Breast Reconstruction following Nipple-Sparing Mastectomy: Predictors of Complications, Reconstruction Outcomes, and 5-Year Trends. Plast. Reconstr. Surg. 2014, 133, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yoon, C.; Bae, S.J.; Cha, C.; Kim, D.; Lee, J.; Ahn, S.G.; Roh, T.S.; Kim, Y.S.; Jeong, J. Comparison of complications according to incision types in nipple-sparing mastectomy and immediate reconstruction. Breast 2020, 53, 85–91. [Google Scholar] [CrossRef]
- Nakamura, H.; Makiguchi, T.; Yamaguchi, T.; Fujii, T.; Shirabe, K.; Yokoo, S. Impact of skeletal muscle mass on complications following expander breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.T.; Hanwright, P.J.; Smetona, J.T.; Hirsch, E.M.; Seth, A.K.; Kim, J.Y. Body mass index as a continuous predictor of outcomes after expander-implant breast reconstruction. Ann. Plast. Surg. 2014, 73, 19–24. [Google Scholar] [CrossRef]
- Fischer, J.P.; Nelson, J.A.; Serletti, J.M.; Wu, L.C. Peri-operative risk factors associated with early tissue expander (TE) loss following immediate breast reconstruction (IBR): A review of 9305 patients from the 2005-2010 ACS-NSQIP datasets. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1504–1512. [Google Scholar] [CrossRef] [PubMed]
- Caan, B.J.; Cespedes Feliciano, E.M.; Prado, C.M.; Alexeeff, S.; Kroenke, C.H.; Bradshaw, P.; Quesenberry, C.P.; Weltzien, E.K.; Castillo, A.L.; Olobatuyi, T.A.; et al. Association of Muscle and Adiposity Measured by Computed Tomography with Survival in Patients with Nonmetastatic Breast Cancer. JAMA Oncol. 2018, 4, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Toesca, A.; Peradze, N.; Galimberti, V.; Manconi, A.; Intra, M.; Gentilini, O.; Sances, D.; Negri, D.; Veronesi, G.; Rietjens, M.; et al. Robotic Nipple-sparing Mastectomy and Immediate Breast Reconstruction with Implant: First Report of Surgical Technique. Ann. Surg. 2017, 266, e28–e30. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, B.; Struk, S.; Leymarie, N.; Honart, J.F.; Alkhashnam, H.; Tran de Fremicourt, K.; Conversano, A.; Rimareix, F.; Simon, M.; Michiels, S.; et al. Robotic Prophylactic Nipple-Sparing Mastectomy with Immediate Prosthetic Breast Reconstruction: A Prospective Study. Ann. Surg. Oncol. 2018, 25, 2579–2586. [Google Scholar] [CrossRef]
- Toesca, A.; Invento, A.; Massari, G.; Girardi, A.; Peradze, N.; Lissidini, G.; Sangalli, C.; Maisonneuve, P.; Manconi, A.; Gottardi, A.; et al. Update on the Feasibility and Progress on Robotic Breast Surgery. Ann. Surg. Oncol. 2019, 26, 3046–3051. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.W.; Chen, S.T.; Lin, S.L.; Chen, C.J.; Lin, Y.L.; Pai, S.H.; Chen, D.R.; Kuo, S.J. Robotic Nipple-Sparing Mastectomy and Immediate Breast Reconstruction with Gel Implant: Technique, Preliminary Results and Patient-Reported Cosmetic Outcome. Ann. Surg. Oncol. 2019, 26, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Toesca, A.; Peradze, N.; Manconi, A.; Galimberti, V.; Intra, M.; Colleoni, M.; Bonanni, B.; Curigliano, G.; Rietjens, M.; Viale, G.; et al. Robotic nipple-sparing mastectomy for the treatment of breast cancer: Feasibility and safety study. Breast 2017, 31, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angarita, F.A.; Castelo, M.; Englesakis, M.; McCready, D.R.; Cil, T.D. Robot-assisted nipple-sparing mastectomy: Systematic review. Br. J. Surg. 2020, 107, 1580–1594. [Google Scholar]
- Komorowski, A.L.; Zanini, V.; Regolo, L.; Carolei, A.; Wysocki, W.M.; Costa, A. Necrotic complications after nipple- and areola-sparing mastectomy. World J. Surg. 2006, 30, 1410–1413. [Google Scholar] [CrossRef]
- Algaithy, Z.K.; Petit, J.Y.; Lohsiriwat, V.; Maisonneuve, P.; Rey, P.C.; Baros, N.; Lai, H.; Mulas, P.; Barbalho, D.M.; Veronesi, P.; et al. Nipple sparing mastectomy: Can we predict the factors predisposing to necrosis? EJSO-Eur. J. Surg. Oncol. 2012, 38, 125–129. [Google Scholar] [CrossRef]
- Carlson, G.W.; Chu, C.K.; Moyer, H.R.; Duggal, C.; Losken, A. Predictors of Nipple Ischemia after Nipple Sparing Mastectomy. Breast J. 2014, 20, 69–73. [Google Scholar] [CrossRef]
- Park, H.S.; Lee, J.; Lee, D.W.; Song, S.Y.; Lew, D.H.; Kim, S.I.; Cho, Y.U. Robot-assisted Nipple-sparing Mastectomy with Immediate Breast Reconstruction: An Initial Experience. Sci. Rep. 2019, 9, 15669. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Kim, J.H.; Lee, D.W.; Song, S.Y.; Park, S.; Kim, S.I.; Ryu, D.H.; Cho, Y.U. Gasless Robot-Assisted Nipple-Sparing Mastectomy: A Case Report. J. Breast Cancer 2018, 21, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Song, E.J.; Lee, C.W.; Jung, S.Y.; Kim, B.N.; Lee, K.S.; Lee, S.; Kang, H.S.; Park, I.H.; Lee, M.H.; Kim, Y.J.; et al. Prognostic impact of skeletal muscle volume derived from cross-sectional computed tomography images in breast cancer. Breast Cancer Res. Treat. 2018, 172, 425–436. [Google Scholar] [CrossRef]
- Oh, R.K.; Ko, H.M.; Lee, J.E.; Lee, K.H.; Kim, J.Y.; Kim, J.S. Clinical impact of sarcopenia in patients with colon cancer undergoing laparoscopic surgery. Ann. Surg. Treat. Res. 2020, 99, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, Y.S.; Kim, E.Y.; Jin, W. Prognostic significance of CT-determined sarcopenia in patients with advanced gastric cancer. PLoS ONE 2018, 13, e0202700. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.W.; Chen, C.Y.; Mok, C.W.; Liao, C.Y.; Chen, C.J.; Chen, S.T.; Lin, S.L.; Chen, D.R.; Kuo, S.J. Robotic nipple-sparing mastectomy: A preliminary report of a single institute and joint collective analysis of current reported series. Formos. J. Surg. 2019, 52, 175–182. [Google Scholar] [CrossRef]
- Lee, J.; Park, H.S.; Lee, H.; Lee, D.W.; Song, S.Y.; Lew, D.H.; Kim, J.Y.; Park, S.; Kim, S.I. Post-Operative Complications and Nipple Necrosis Rates Between Conventional and Robotic Nipple-Sparing Mastectomy. Front. Oncol. 2020, 10, 594388. [Google Scholar] [CrossRef]
- O’Dey, D.M.; Prescher, A.; Pallua, N. Vascular reliability of nipple-areola complex-bearing pedicles: An anatomical microdissection study. Plast. Reconstr. Surg. 2007, 119, 1167–1177. [Google Scholar] [CrossRef]
- van Deventer, P.V.; Graewe, F.R. The Blood Supply of the Breast Revisited. Plast. Reconstr. Surg. 2016, 137, 1388–1397. [Google Scholar] [CrossRef]
- McCarthy, C.M.; Mehrara, B.J.; Riedel, E.; Davidge, K.; Hinson, A.; Disa, J.J.; Cordeiro, P.G.; Pusic, A.L. Predicting complications following expander/implant breast reconstruction: An outcomes analysis based on preoperative clinical risk. Plast. Reconstr. Surg. 2008, 121, 1886–1892. [Google Scholar] [CrossRef]
- Hirsch, E.M.; Seth, A.K.; Kim, J.Y.S.; Dumanian, G.A.; Mustoe, T.A.; Galiano, R.D.; Fine, N.A. Analysis of risk factors for complications in expander/implant breast reconstruction by stage of reconstruction. Plast. Reconstr. Surg. 2014, 134, 692e–699e. [Google Scholar] [CrossRef]
- Chang, C.W.; Tai, H.C.; Cheng, N.C.; Li, W.T.; Lai, H.S.; Chien, H.F. Risk factors for complications following immediate tissue expander based breast reconstruction in Taiwanese population. J. Formos. Med. Assoc. 2017, 116, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Laporta, R.; Longo, B.; Sorotos, M.; Farcomeni, A.; Patti, C.; Mastrangeli, M.R.; Rubino, C.; Santanelli di Pompeo, F. Breast reconstruction following nipple-sparing mastectomy: Clinical outcomes and risk factors related complications. J. Plast. Surg. Hand Surg. 2017, 51, 427–435. [Google Scholar] [CrossRef]
- Woo, K.J.; Paik, J.; Mun, G.H.; Pyon, J.K.; Bang, S.I. Risk Factors for Complications in Immediate Expander-Implant Breast Reconstruction for Non-obese Patients: Impact of Breast Size on Complications. Aesthet. Plast. Surg. 2016, 40, 71–78. [Google Scholar] [CrossRef]
- Francis, S.H.; Ruberg, R.L.; Stevenson, K.B.; Beck, C.E.; Ruppert, A.S.; Harper, J.T.; Boehmler, J.H.T.; Miller, M.J. Independent risk factors for infection in tissue expander breast reconstruction. Plast. Reconstr. Surg. 2009, 124, 1790–1796. [Google Scholar] [CrossRef]
- Lanier, S.T.; Wang, E.D.; Chen, J.J.; Arora, B.P.; Katz, S.M.; Gelfand, M.A.; Khan, S.U.; Dagum, A.B.; Bui, D.T. The Effect of Acellular Dermal Matrix Use on Complication Rates in Tissue Expander/Implant Breast Reconstruction. Ann. Plast. Surg. 2010, 64, 674–678. [Google Scholar] [CrossRef]
- Deluche, E.; Leobon, S.; Desport, J.C.; Venat-Bouvet, L.; Usseglio, J.; Tubiana-Mathieu, N. Impact of body composition on outcome in patients with early breast cancer. Support. Care Cancer 2018, 26, 861–868. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | No Complication (n = 58) | Complication (n = 34) | p-Value |
|---|---|---|---|
| Age, years | 44 ± 7 | 45 ± 8 | 0.296 |
| Smoking history | 0.605 | ||
| Non-smoker | 57 (98%) | 33 (97%) | |
| Ex-smoker | 0 (0%) | 1 (3%) | |
| Current smoker | 1 (2%) | 0 (0%) | |
| ASA physical status | 0.358 | ||
| I | 34 (59%) | 16 (47%) | |
| II | 21 (36%) | 14 (41%) | |
| III | 3 (5%) | 4 (12%) | |
| Comorbidities | |||
| Hypertension | 3 (5%) | 2 (6%) | >0.999 |
| Diabetes mellitus | 1 (2%) | 1 (3%) | >0.999 |
| Menopause status | 0.690 | ||
| Premenopausal | 48 (83%) | 27 (79%) | |
| Postmenopausal | 10 (17%) | 7 (21%) | |
| Neoadjuvant chemotherapy | 5 (9%) | 4 (12%) | 0.721 |
| Body mass index, kg/m2 | 21.3 (20.1, 22.6) | 22.5 (20.4, 24.0) | 0.088 |
| Skeletal muscle index, cm2/m2 | 38.7 (36.4. 43.4) | 40.3 (37.6, 45.0) | 0.353 |
| Subcutaneous adipose tissue index, cm2/m2 | 48.3 (34.9, 60.2) | 58.7 (47.0, 76.4) | 0.007 * |
| Visceral adipose tissue index, cm2/m2 | 15.7 (9.43, 21.1) | 27.0 (17.2, 37.7) | <0.001 * |
| Total adipose tissue index, cm2/m2 | 62.9 (48.3, 85.2) | 89.2 (70.1, 110.4) | <0.001 * |
| SMI/TATI | 66.6 (47.3, 83.6) | 46.3 (40.3, 55.5) | <0.001 * |
| Variable | No Complication (n = 58) | Complication (n = 34) | p-Value |
|---|---|---|---|
| Surgical extent | 0.367 | ||
| Unilateral | 47 (81%) | 30 (88%) | |
| Bilateral | 11 (19%) | 4 (12%) | |
| ALND | 11 (19%) | 4 (12%) | 0.367 |
| Type of reconstruction | 0.358 | ||
| Direct-to-implant | 41 (71%) | 27 (79%) | |
| Tissue expander insertion | 17 (29%) | 7 (21%) | |
| Reconstruction location | 0.367 | ||
| Pre-pectoral | 47 (81%) | 30 (88%) | |
| Sub-pectoral | 11 (19%) | 4 (12%) | |
| Combined other operation | 10 (17%) | 7 (21%) | 0.690 |
| Specimen weight, g | 313 (248, 395) | 387 (322, 471) | 0.004 * |
| Duration of anesthesia time, min | 346.5 (300, 425) | 362.5 (305, 445) | 0.247 |
| Duration of operation time, min | 299 (246, 372) | 305 (260, 387) | 0.509 |
| Duration of mastectomy time, min | 170 (142, 214) | 198 (168, 233) | 0.058 |
| Duration of reconstruction time, min | 110.5 (89, 133) | 122 (107, 157) | 0.088 |
| Intraoperative blood loss, mL | 50 (30, 70) | 50 (30, 150) | 0.144 |
| Intraoperative fluid input rate, mL/min | 6.1 ± 1.5 | 6.6 ± 1.5 | 0.209 |
| Intraoperative urine out, mL | 467.5 (340, 780) | 427.5 (280, 620) | 0.496 |
| Administered dose of remifentanil, mg | 0.9 (0.8, 1.1) | 1.0 (0.9, 1.3) | 0.091 |
| Postoperative hospital days | 9 (7, 11) | 10 (8, 12) | 0.085 |
| Variable | Number (%) |
|---|---|
| NAC | |
| NAC ischemic grade | |
| Grade 0 | 73 (79%) |
| Grade 1 | 7 (8%) |
| Grade 2 | 5 (5%) |
| Grade 3 | 4 (4%) |
| Grade 4 | 2 (2%) |
| Grade 5 | 1 (1%) |
| NAC ischemia (Resolved with conservative treatment) | 15 (16%) |
| NAC necrosis (Required Surgical treatment) | 4 (4%) |
| NAC loss | 2 (2%) |
| OTHERS | |
| Skin ischemia or necrosis | 7 (8%) |
| Implant loss | 2 (2%) |
| Wound dehiscence | 1 (1%) |
| Seroma | 6 (7%) |
| Infection | 7 (8%) |
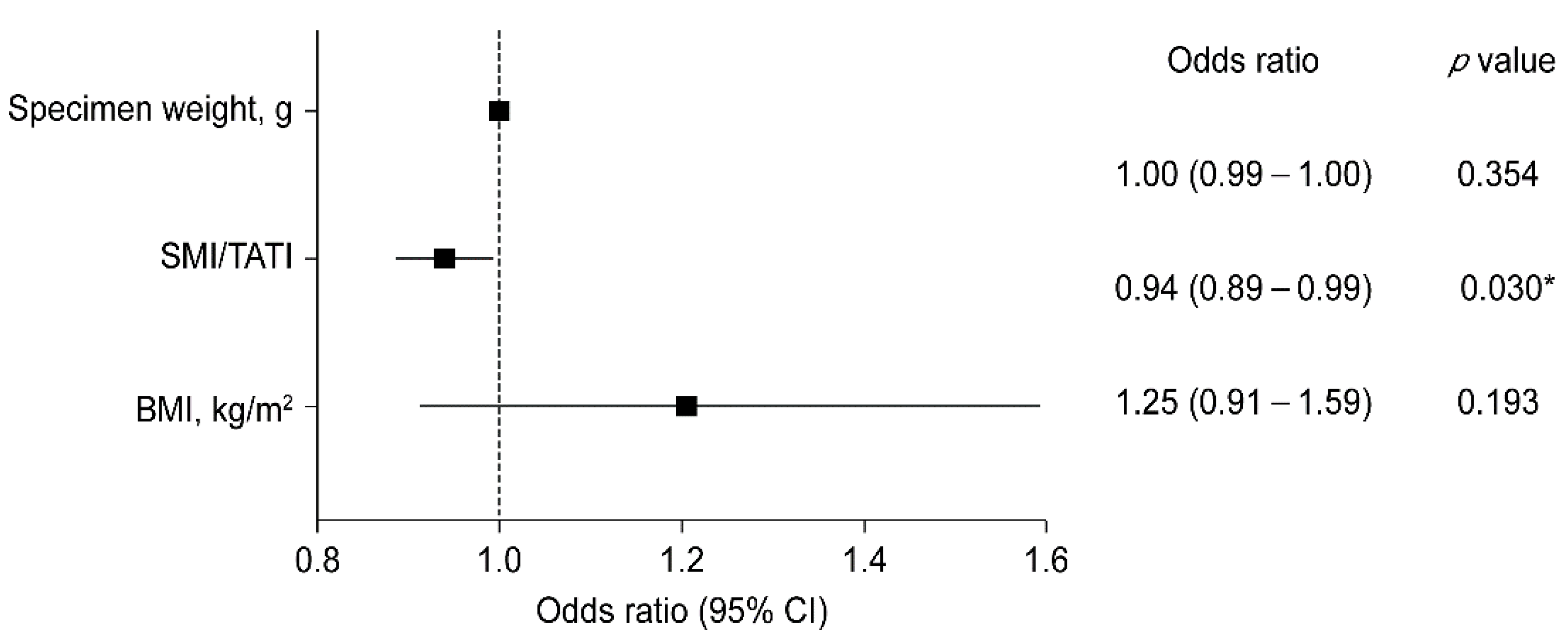
| Variable | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age, years | 1.06 | [0.99–1.14] | 0.087 |
| Smoking | 1.07 | [0.11–10.34] | 0.951 |
| Diabetes mellitus | 5.43 | [0.32–91.99] | 0.241 |
| BMI, kg/m2 | 1.30 | [1.08–1.58] | 0.007 * |
| SMI, cm2/m2 | 1.01 | [0.96–1.06] | 0.773 |
| SATI, cm2/m2 | 1.03 | [1.01–1.06] | 0.018 * |
| VATI, cm2/m2 | 1.07 | [1.03–1.11] | 0.001 * |
| TATI, cm2/m2 | 1.03 | [1.01–1.05] | 0.002 * |
| SMI/TATI | 0.93 | [0.89–0.98] | 0.004 * |
| ALND | 0.32 | [0.04–2.65] | 0.292 |
| Type of reconstruction | |||
| DTI | ref | ||
| TE insertion | 0.39 | [0.08–1.85] | 0.233 |
| Location | |||
| Pre-pectoral | ref | ||
| Sub-pectoral | 0.76 | [0.15–3.77] | 0.734 |
| Combined with other surgery | 1.13 | [0.28–4.52] | 0.868 |
| Specimen weight, g | 1.00 | [1.00–1.01] | 0.026 * |
| Anesthesia duration, min | 1.00 | [1.00–1.01] | 0.911 |
| Operation duration, min | 1.00 | [0.99–1.01] | 0.958 |
| Blood loss >100mL | 1.77 | [0.53–5.87] | 0.354 |
| Fluid input rate, mL/kg/min | 1.04 | [0.72–1.51] | 0.832 |
| Urine out, mL | 1.00 | [1.00–1.00] | 0.460 |
| Postoperative hospital stays, days | 0.96 | [0.79–1.17] | 0.668 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, J.; Lee, J.; Lee, D.W.; Shin, H.J.; Lee, S.; Kang, Y.; Kim, N.Y.; Park, H.S. Impact of Body Composition on Postoperative Outcomes in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction. Curr. Oncol. 2022, 29, 350-359. https://doi.org/10.3390/curroncol29010031
Moon J, Lee J, Lee DW, Shin HJ, Lee S, Kang Y, Kim NY, Park HS. Impact of Body Composition on Postoperative Outcomes in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction. Current Oncology. 2022; 29(1):350-359. https://doi.org/10.3390/curroncol29010031
Chicago/Turabian StyleMoon, Jiae, Jeea Lee, Dong Won Lee, Hye Jung Shin, Sumin Lee, Yhenseung Kang, Na Young Kim, and Hyung Seok Park. 2022. "Impact of Body Composition on Postoperative Outcomes in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction" Current Oncology 29, no. 1: 350-359. https://doi.org/10.3390/curroncol29010031
APA StyleMoon, J., Lee, J., Lee, D. W., Shin, H. J., Lee, S., Kang, Y., Kim, N. Y., & Park, H. S. (2022). Impact of Body Composition on Postoperative Outcomes in Patients Undergoing Robotic Nipple-Sparing Mastectomy with Immediate Breast Reconstruction. Current Oncology, 29(1), 350-359. https://doi.org/10.3390/curroncol29010031