
Bilateral Strength Asymmetry in Elite Youth Soccer Players: Differences between Age Categories

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Procedures
2.4. Statistical Analyses
3. Results
3.1. Isokinetic Strength of Knee Extensors and Flexors
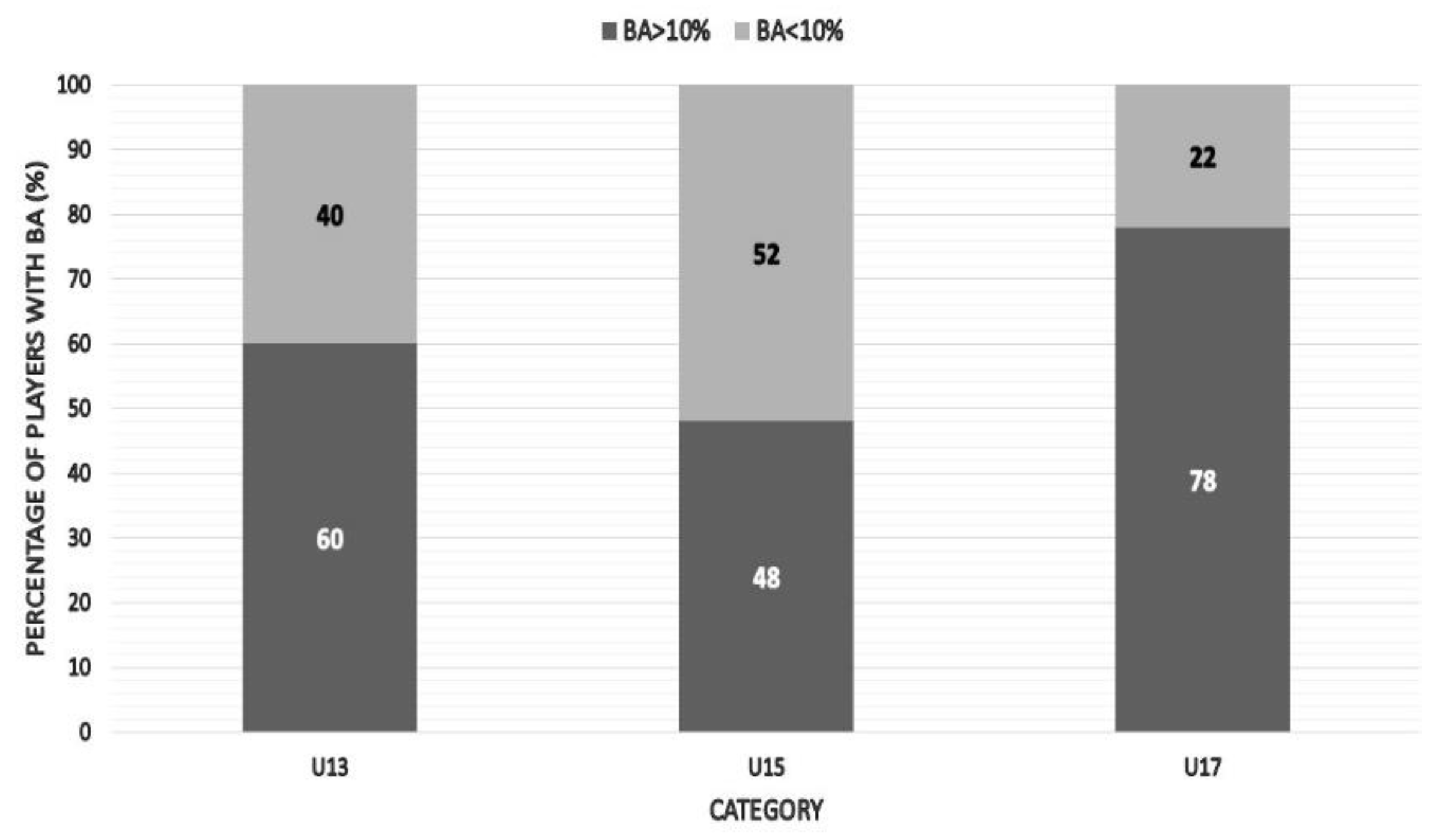
3.2. Bilateral Ratio of Knee Extensors
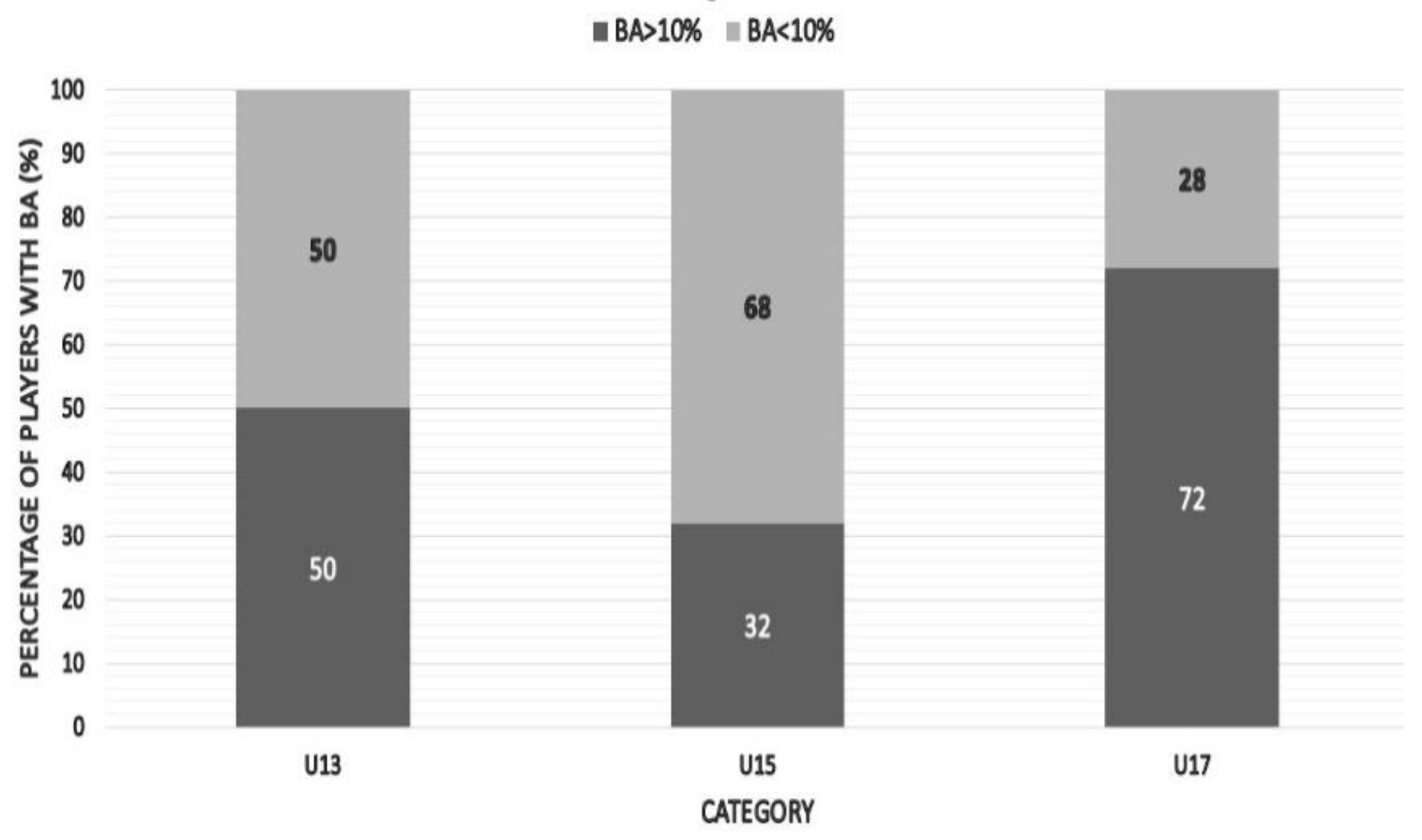
3.3. Bilateral Ratio of Knee Flexors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnes, C.; Archer, D.; Hogg, B.; Bush, M.; Bradley, P. The evolution of physical and technical performance parameters in the English Premier League. Int. J. Sports Med. 2014, 35, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, F.; Carling, C.; Reilly, T.; Vandewalle, H.; Church, J.; Rochcongar, P. Incidence of injuries in elite French youth soccer players: A 10-season study. Am. J. Sports Med. 2006, 34, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Dauty, M.; Menu, P.; Fouasson-Chailloux, A.; Ferréol, S.; Dubois, C. Prediction of hamstring injury in professional soccer players by isokinetic measurements. Muscles Ligaments Tendons J. 2016, 6, 116. [Google Scholar] [CrossRef] [PubMed]
- Liporaci, R.F.; Saad, M.; Grossi, D.B.; Riberto, M. Clinical features and isokinetic parameters in assessing injury risk in elite football players. Int. J. Sports Med. 2019, 40, 903–908. [Google Scholar] [CrossRef]
- Daneshjoo, A.; Rahnama, N.; Mokhtar, A.H.; Yusof, A. Bilateral and unilateral asymmetries of isokinetic strength and flexibility in male young professional soccer players. J. Hum. Kinet. 2013, 36, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Grygorowicz, M.; Kubacki, J.; Pilis, W.; Gieremek, K.; Rzepka, R. Selected isokinetic tests in knee injury prevention. Biol. Sport 2010, 27, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Hong, J. Hamstring to quadriceps strength ratio and noncontact leg injuries: A prospective study during one season. Isokinet. Exerc. Sci. 2011, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Fousekis, K.; Tsepis, E.; Vagenas, G. Lower limb strength in professional soccer players: Profile, asymmetry, and training age. J. Sports Sci. Med. 2010, 9, 364. [Google Scholar]
- Kalata, M.; Maly, T.; Hank, M.; Michalek, J.; Bujnovsky, D.; Kunzmann, E.; Zahalka, F. Unilateral and bilateral strength asymmetry among young elite athletes of various sports. Medicina 2020, 56, 683. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; Myer, G.D.; Croix, M.B.D.S.; Lloyd, R.S. The effects of maturation on measures of asymmetry during neuromuscular control tests in elite male youth soccer players. Pediatr. Exerc. Sci. 2018, 30, 168–175. [Google Scholar] [CrossRef]
- Gray, J.; Aginsky, K.D.; Derman, W.; Vaughan, C.L.; Hodges, P.W. Symmetry, not asymmetry, of abdominal muscle morphology is associated with low back pain in cricket fast bowlers. J. Sci. Med. Sport 2016, 19, 222–226. [Google Scholar] [CrossRef]
- Maly, T.; Sugimoto, D.; Izovska, J.; Zahalka, F.; Mala, L. Effect of muscular strength, asymmetries and fatigue on kicking performance in soccer players. Int. J. Sports Med. 2018, 39, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.L.; Norton, K.I. Evolution of World Cup soccer final games 1966–2010: Game structure, speed and play patterns. J. Sci. Med. Sport 2014, 17, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Weigelt, M.; Memmert, D. Goal-side selection in soccer penalty kicking when viewing natural scenes. Front. Psychol. 2012, 3, 312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahnama, N.; Lees, A.; Bambaecichi, E. A comparison of muscle strength and flexibility between the preferred and non-preferred leg in English soccer players. Ergonomics 2005, 48, 1568–1575. [Google Scholar] [CrossRef]
- Atkins, S.J.; Bentley, I.; Hurst, H.T.; Sinclair, J.K.; Hesketh, C. The presence of bilateral imbalance of the lower limbs in elite youth soccer players of different ages. J. Strength Cond. Res. 2016, 30, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Maly, T.; Ford, K.R.; Sugimoto, D.; Izovska, J.; Bujnovsky, D.; Hank, M.; Cabell, L.; Zahalka, F. Isokinetic strength, bilateral and unilateral strength differences: Variation by age and laterality in elite youth football players. Int. J. Morphol. 2021, 39. [Google Scholar] [CrossRef]
- Vargas, V.Z.; Peres, B.; Vancini, R.L.; De Lira, C.; Andrade, M. Knee isokinetic muscle strength and balance ratio in female soccer players of different age groups: A cross-sectional study. Phys. Sportmed. 2020, 48, 105–109. [Google Scholar] [CrossRef]
- Armstrong, N.; Mcmanus, A.M. Physiology of elite young male athletes. In The Elite Young Athlete; Karger: Basel, Switzerland, 2011; Volume 56, pp. 1–22. [Google Scholar]
- Malina, R.M. Maturity status and injury risk in youth soccer players. Clin. J. Sport Med. 2010, 20, 132. [Google Scholar] [CrossRef]
- Renshaw, A.; Goodwin, P.C. Injury incidence in a Premier League youth soccer academy using the consensus statement: A prospective cohort study. BMJ Open Sport Exerc. Med. 2016, 2, e000132. [Google Scholar] [CrossRef] [Green Version]
- Impellizzeri, F.M.; Bizzini, M.; Rampinini, E.; Cereda, F.; Maffiuletti, N.A. Reliability of isokinetic strength imbalance ratios measured using the Cybex NORM dynamometer. Clin. Physiol. Funct. Imaging 2008, 28, 113–119. [Google Scholar] [CrossRef]
- Mota, S.; Brito, J.; Passos, E.; Marques, E.; Mota, J.; Seabra, A.; Rebelo, A. Variation of isokinetic strength and bone mineral density in youth portuguese soccer players with age. Open Sports Sci. J. 2010, 3, 49–51. [Google Scholar] [CrossRef]
- Andrade, M.S.; Junqueira, M.S.; Andre Barbosa De Lira, C.; Vancini, R.L.; Seffrin, A.; Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. Age-related differences in torque in angle-specific and peak torque hamstring to quadriceps ratios in female soccer players from 11 to 18 years old: A Cross-sectional study. Res. Sports Med. 2021, 29, 77–89. [Google Scholar] [CrossRef]
- Philippaerts, R.M.; Vaeyens, R.; Janssens, M.; Van Renterghem, B.; Matthys, D.; Craen, R.; Bourgois, J.; Vrijens, J.; Beunen, G.; Malina, R.M. The relationship between peak height velocity and physical performance in youth soccer players. J. Sports Sci. 2006, 24, 221–230. [Google Scholar] [CrossRef]
- Price, R.; Hawkins, R.; Hulse, M.; Hodson, A. The Football Association medical research programme: An audit of injuries in academy youth football. Br. J. Sports Med. 2004, 38, 466–471. [Google Scholar] [CrossRef] [Green Version]
- McGill, S.M. Low Back Disorders. Evidence Based Prevention and Rehabilitation; Human Kinetics: Champaign, IL, USA, 2002. [Google Scholar]
- Lehance, C.; Binet, J.; Bury, T.; Croisier, J.-L. Muscular strength, functional performances and injury risk in professional and junior elite soccer players. Scand. J. Med. Sci. Sports 2009, 19, 243–251. [Google Scholar] [CrossRef]
- Orchard, J.W. Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am. J. Sports Med. 2001, 29, 300–303. [Google Scholar] [CrossRef]
- Maly, T.; Zahalka, F.; Mala, L. Unilateral and ipsilateral strength asymmetries in elite youth soccer players with respect to muscle group and limb dominance. Int. J. Morphol. 2016, 34, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Iga, J.; George, K.; Lees, A.; Reilly, T. Cross-sectional investigation of indices of isokinetic leg strength in youth soccer players and untrained individuals. Scand. J. Med. Sci. Sports 2009, 19, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Alvares, J.B.; Dornelles, M.P.; Fritsch, C.G.; De Lima-E-Silva, F.X.; Medeiros, T.M.; Severo-Silveira, L.; Marques, V.B.; Baroni, B.M. Prevalence of hamstring strain injury risk factors in professional and under-20 male football (soccer) players. J. Sport Rehabil. 2020, 29, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Read, P.J.; Jimenez, P.; Oliver, J.L.; Lloyd, R.S. Injury prevention in male youth soccer: Current practices and perceptions of practitioners working at elite English academies. J. Sports Sci. 2018, 36, 1423–1431. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Mean ± SD | |||||||
|---|---|---|---|---|---|---|---|
| AgeCategory | Players (n) | Age (years) | Body Height(cm) | Body Weight (kg) | FieldTraining | ResistanceTraining | Match |
| U13 | 32 | 11.74 ± 0.62 | 149.73 ± 7.08 | 39.95 ± 8.49 | 3–4×(60–90 min) | N | 2 × 35min |
| U15 | 25 | 14.02 ± 0.61 | 165.11 ± 8.24 | 52.36 ± 8.71 | 4–5×(60–90 min) | N | 2 × 40min |
| U17 | 33 | 15.77 ± 0.34 | 177.16 ± 5.11 | 68.41 ± 7.02 | 5–6×(60–90 min) | 1 × 60 min | 2 × 45min |
| U13Mean ± SD | U15Mean ± SD | U17Mean ± SD | F | p | ηp2 | |
|---|---|---|---|---|---|---|
| PTKE DL | 1.69 ± 0.53 | 2.47 ± 0.35 b | 2.97 ± 0.34 a | 53.364 | <0.001 | 0.629 |
| PTKE NDL | 1.68 ± 0.55 | 2.54 ± 0.29 b | 3.00 ± 0.36 a | 54.425 | <0.001 | 0.650 |
| PTKF DL | 1.25 ± 0.19 | 1.47 ± 0.23 b | 1.75 ± 0.20 a | 47.340 | <0.001 | 0.530 |
| PTKF NDL | 1.23 ± 0.19 | 1.38 ± 0.18 b | 1.75 ± 0.26 a | 46.977 | <0.001 | 0.528 |
| Q:Q (%) | 11.10 ± 7.59 | 10.49 ± 7.06 | 6.29 ± 5.61 c | 4.456 | <0.05 | 0.099 |
| H:H (%) | 11.87 ± 7.77 | 12.12 ± 5.52 | 7.79 ± 5.81 d | 3.547 | <0.05 | 0.081 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalata, M.; Hank, M.; Bujnovsky, D.; Michalek, J.; Varjan, M.; Kunzmann, E.; Zahalka, F.; Maly, T. Bilateral Strength Asymmetry in Elite Youth Soccer Players: Differences between Age Categories. Symmetry 2021, 13, 1982. https://doi.org/10.3390/sym13111982
Kalata M, Hank M, Bujnovsky D, Michalek J, Varjan M, Kunzmann E, Zahalka F, Maly T. Bilateral Strength Asymmetry in Elite Youth Soccer Players: Differences between Age Categories. Symmetry. 2021; 13(11):1982. https://doi.org/10.3390/sym13111982
Chicago/Turabian StyleKalata, Maros, Mikulas Hank, David Bujnovsky, Jakub Michalek, Matej Varjan, Egon Kunzmann, Frantisek Zahalka, and Tomas Maly. 2021. "Bilateral Strength Asymmetry in Elite Youth Soccer Players: Differences between Age Categories" Symmetry 13, no. 11: 1982. https://doi.org/10.3390/sym13111982
APA StyleKalata, M., Hank, M., Bujnovsky, D., Michalek, J., Varjan, M., Kunzmann, E., Zahalka, F., & Maly, T. (2021). Bilateral Strength Asymmetry in Elite Youth Soccer Players: Differences between Age Categories. Symmetry, 13(11), 1982. https://doi.org/10.3390/sym13111982