
Effects of 12 Weeks Cosmos caudatus Supplement among Older Adults with Mild Cognitive Impairment: A Randomized, Double-Blind and Placebo-Controlled Trial

 ,
, 
 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
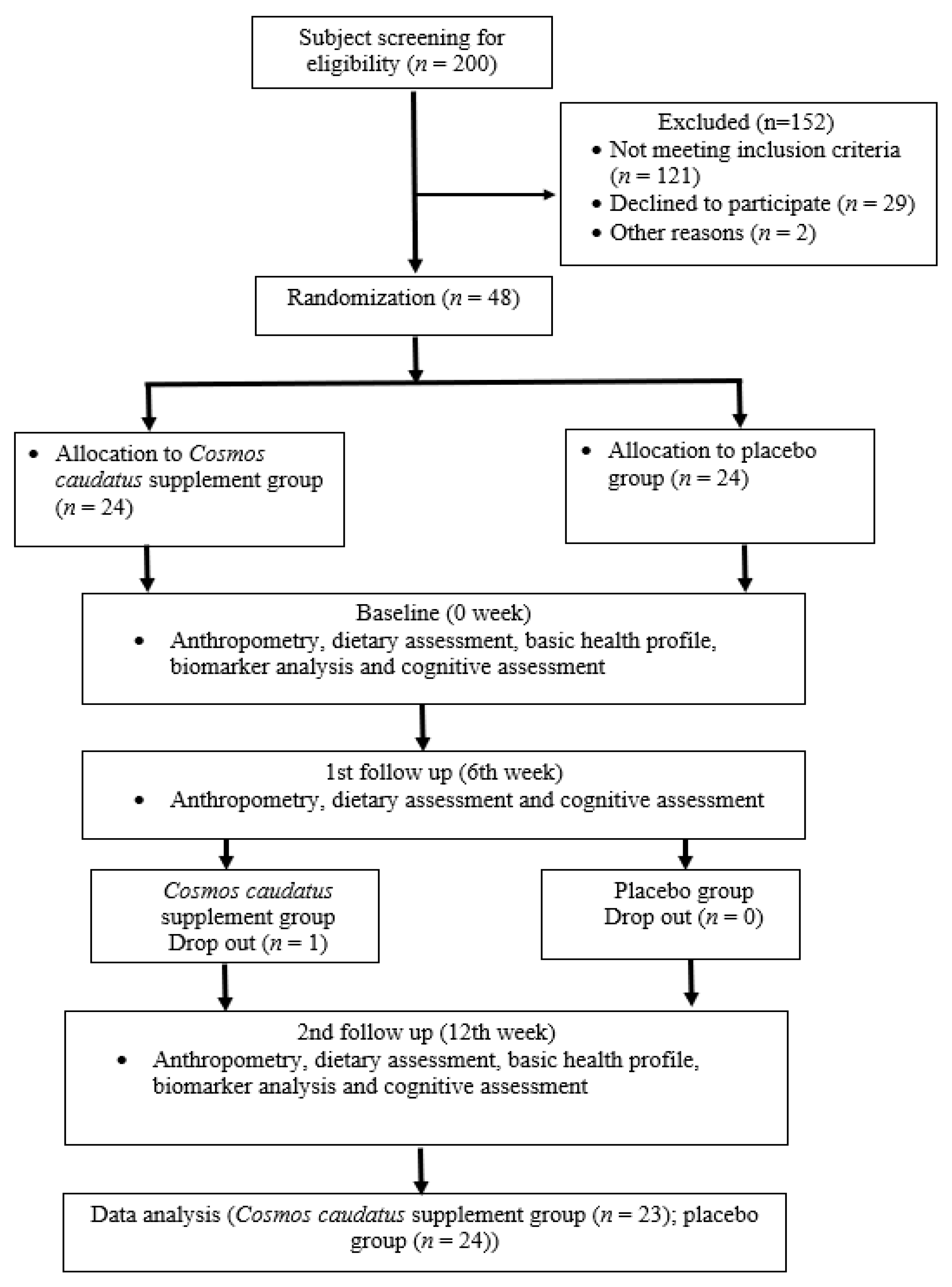
2.1. Study Design and Subject’s Selection
2.2. Study Product and Dosage
2.3. Study Procedures
2.3.1. Cognitive Function Assessment
2.3.2. Blood Biochemical Profile and Blood Biomarkers Tests
2.4. Statistical Analysis
3. Results
3.1. Subjects’ Characteristics
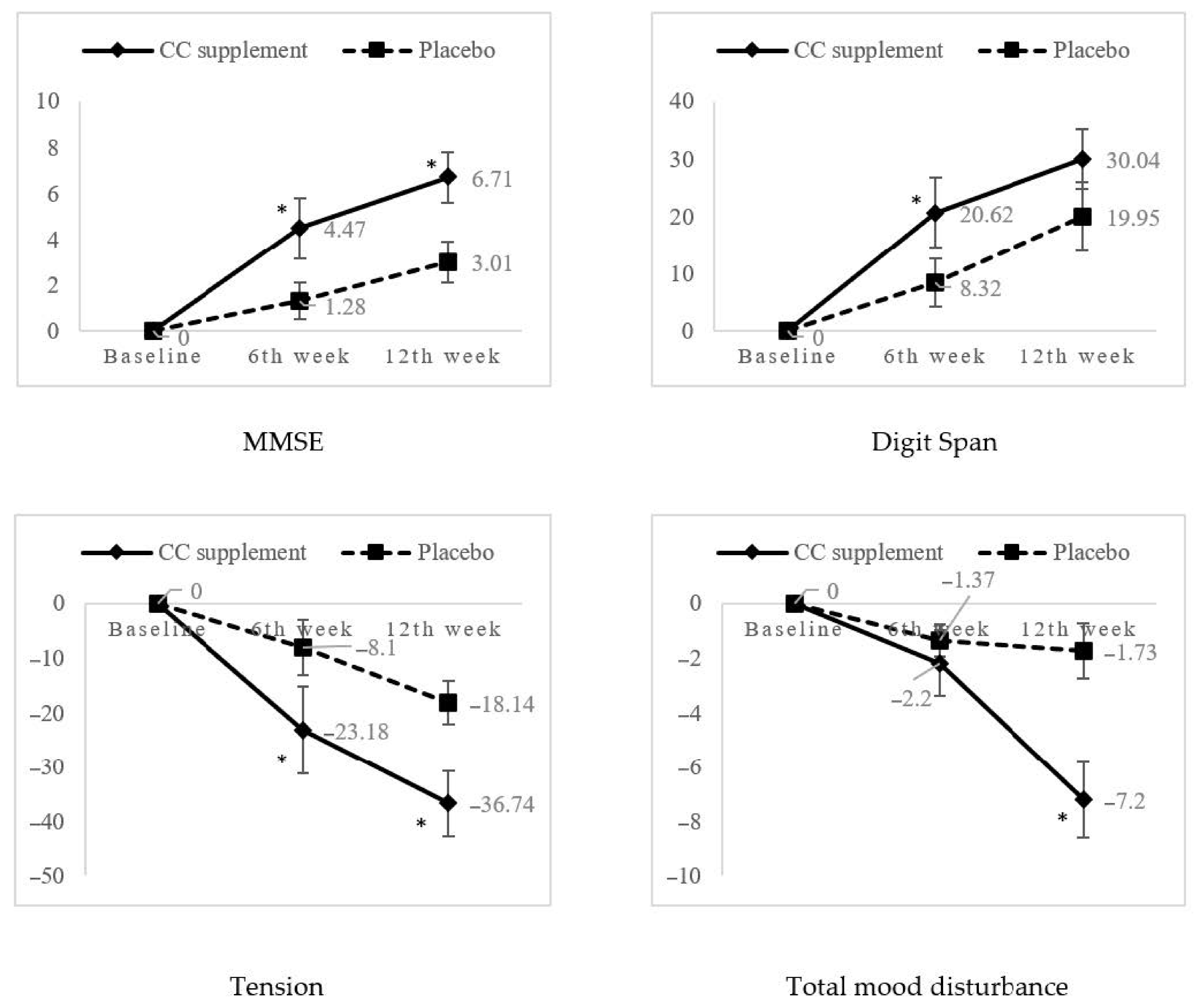
3.2. Cognitive Function and Mood Status
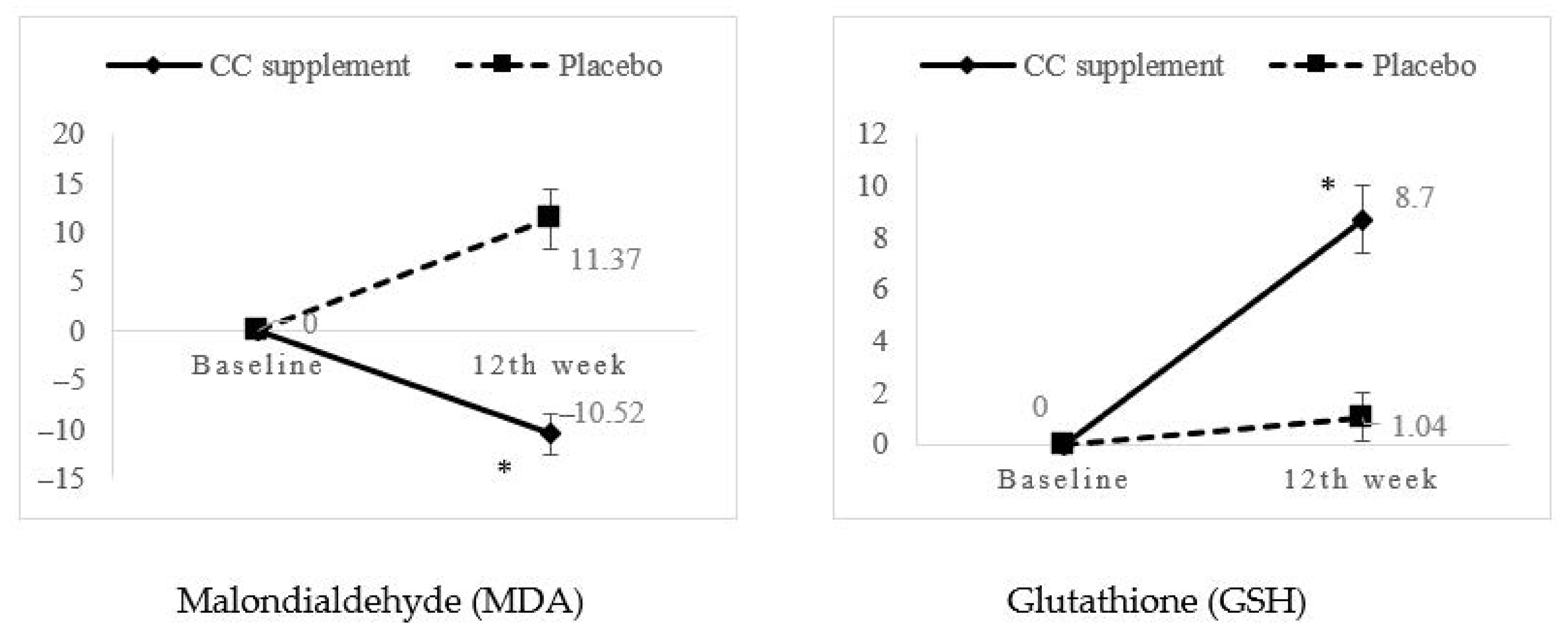
3.3. Biochemical Profiles and Biomarker Analysis
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. World Populaton Ageing; United Nations: New York, NY, USA, 2015. [Google Scholar]
- United Nations. World Populaton Ageing; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Tey, N.P.; Siraj, S.B.; Kamaruzzaman, S.B.; Chin, A.V.; Tan, M.P.; Sinnappan, G.S.; Muller, A.M. Aging in Multi-ethnic Malaysia. Gerontologist 2016, 56, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics Malaysia. Current Population Estimates Malaysia 2018–2019; Department of Statistics: Putrajaya, Malaysia, 2019. [Google Scholar]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Vanoh, D.; Shahar, S.; Din, N.C.; Omar, A.; Vyrn, C.A.; Razali, R.; Ibrahim, R.; Hamid, T.A. Predictors of poor cognitive status among older Malaysian adults: Baseline findings from the LRGS TUA cohort study. Aging Clin. Exp. Res. 2017, 29, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Boccardi, V.; Baroni, M.; Mangialasche, F.; Mecocci, P. Vitamin E family: Role in the pathogenesis and treatment of Alzheimer’s disease. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2016, 2. [Google Scholar] [CrossRef]
- Mostafavi, S.-A.; Hosseini, S. Chapter 7—Foods and Dietary Supplements in the Prevention and Treatment of Neurodegenerative Diseases in Older Adults. In Foods and Dietary Supplements in the Prevention and Treatment of Disease in Older Adults; Watson, R.R., Ed.; Academic Press: San Diego, CA, USA, 2015; pp. 63–67. [Google Scholar] [CrossRef]
- Nuzzo, D.; Amato, A.; Picone, P.; Terzo, S.; Galizzi, G.; Bonina, F.P.; Mulè, F.; Di Carlo, M. A Natural Dietary Supplement with a Combination of Nutrients Prevents Neurodegeneration Induced by a High Fat Diet in Mice. Nutrients 2018, 10, 1130. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.; Mangialasche, F.; Ngandu, T.; Solomon, A.; Kivipelto, M. Multidomain Interventions to Prevent Cognitive Impairment, Alzheimer’s Disease, and Dementia: From FINGER to World-Wide FINGERS. J. Prev. Alzheimer’s Dis. 2020, 7, 29–36. [Google Scholar] [CrossRef]
- Lau, H.; Shahar, S.; Mohamad, M.; Rajab, N.F.; Yahya, H.M.; Din, N.C.; Hamid, H.A. The effects of six months Persicaria minor extract supplement among older adults with mild cognitive impairment: A double-blinded, randomized, and placebo-controlled trial. BMC Complement. Med. Ther. 2020, 20, 315. [Google Scholar] [CrossRef]
- Chen, L.-E.; Wu, F.; Zhao, A.; Ge, H.; Zhan, H. Protection Efficacy of the Extract ofGinkgo biloba against the Learning and Memory Damage of Rats under Repeated High Sustained +Gz Exposure. Evid. Based Complement. Altern. Med. 2016, 2016, 6320586. [Google Scholar] [CrossRef]
- Gschwind, Y.J.; Bridenbaugh, S.A.; Reinhard, S.; Granacher, U.; Monsch, A.U.; Kressig, R.W. Ginkgo biloba special extract LI 1370 improves dual-task walking in patients with MCI: A randomised, double-blind, placebo-controlled exploratory study. Aging Clin. Exp. Res. 2017, 29, 609–619. [Google Scholar] [CrossRef]
- Puttarak, P.; Dilokthornsakul, P.; Saokaew, S.; Dhippayom, T.; Kongkaew, C.; Sruamsiri, R.; Chuthaputti, A.; Chaiyakunapruk, N. Effects of Centella asiatica (L.) Urb. on cognitive function and mood related outcomes: A Systematic Review and Meta-analysis. Sci. Rep. 2017, 7, 10646. [Google Scholar] [CrossRef]
- Yahya, H.; Shahar, S.; Nur Arina Ismail, S.; Aziz, A.; Normah, C.D.; Hakim, B.N. Mood, Cognitive Function and Quality of Life Improvements in Middle Aged Women Following Supplementation with Polygonum minus Extract. Sains Malays. 2017, 46, 245–254. [Google Scholar] [CrossRef]
- Hooshmand, B.; Mangialasche, F.; Kalpouzos, G.; Solomon, A.; Kåreholt, I.; Smith, D.; Refsum, H.; Wang, R.; Muehlmann, M.; Birgit, E.-W.; et al. Association of Vitamin B12, Folate, and Sulfur Amino Acids with Brain Magnetic Resonance Imaging Measures in Older Adults: A Longitudinal Population-Based Study. JAMA Psychiatry 2016, 73. [Google Scholar] [CrossRef] [PubMed]
- Mangialasche, F.; Solomon, A.; Kåreholt, I.; Hooshmand, B.; Cecchetti, R.; Fratiglioni, L.; Soininen, H.; Laatikainen, T.; Mecocci, P.; Kivipelto, M. Serum levels of vitamin E forms and risk of cognitive impairment in a Finnish cohort of older adults. Exp. Gerontol. 2013, 48. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.; Shahar, S.; Mohamad, M.; Rajab, N.F.; Yahya, H.M.; Din, N.C.; Hamid, H.A. Relationships between dietary nutrients intake and lipid levels with functional MRI dorsolateral prefrontal cortex activation. Clin. Interv. Aging 2018, 14, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Moshawih, S.; Cheema, M.; Ahmad, Z.; Zakaria, Z.A.; Nazrul Hakim, M. A Comprehensive Review on Cosmos caudatus (Ulam Raja): Pharmacology, Ethnopharmacology, and Phytochemistry. Int. Res. J. Educ. Sci. 2017, 1, 14–31. [Google Scholar]
- Sumazian, Y.; Ahmad, S.; Hakiman, M.; Maziah, M. Antioxidant Activities, Flavonoids, Ascorbic Acid and Phenolic Content of Malaysian Vegetables. J. Med. Plants Res. 2010, 4, 881–890. [Google Scholar] [CrossRef]
- You, Y.; Shahar, S.; Haron, H.; Yahya, H. More Ulam for Your Brain: A Review on the Potential Role of Ulam in Protecting Against Cognitive Decline. Sains Malays. 2018, 47, 2713–2729. [Google Scholar] [CrossRef]
- You, Y.X.; Shahar, S.; Mohamad, M.; Yahya, H.M.; Haron, H.; Abdul Hamid, H. Does traditional asian vegetables (ulam) consumption correlate with brain activity using fMRI? A study among aging adults from low-income households. J. Magn. Reson. Imaging 2019, 51. [Google Scholar] [CrossRef]
- Spencer, B.; Verma, I.; Desplats, P.; Morvinski, D.; Rockenstein, E.; Adame, A.; Masliah, E. A neuroprotective brain-penetrating endopeptidase fusion protein ameliorates Alzheimer disease pathology and restores neurogenesis. J. Biol. Chem. 2014, 289, 17917–17931. [Google Scholar] [CrossRef]
- Lei, X.; Chao, H.; Zhang, Z.; Lv, J.; Li, S.; Wei, H.; Xue, R.; Li, F.; Li, Z. Neuroprotective effects of quercetin in a mouse model of brain ischemic/reperfusion injury via anti-apoptotic mechanisms based on the Akt pathway. Mol. Med. Rep. 2015, 12, 3688–3696. [Google Scholar] [CrossRef]
- Chan, Y.H. Randomised controlled trials (RCTs)—Sample size: The magic number? Singap. Med. J. 2003, 44, 172–174. [Google Scholar]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild cognitive impairment: A concept in evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.; Ehsan, S.Z.; Noor ‘Adilah, K.; Lee, C.P.; Farhana, E.; Derick, P.; Soelaiman, I.; Nazrun, A.S.; Muhammad, N. Acute Toxicity Study of Cosmos caudatus on Biochemical Parameters in Male Rats. Sains Malays. 2013, 42, 1247–1251. [Google Scholar]
- Abdullah, A.; Kaur Dhaliwal, K.; Nabillah, N.; Roslan, F.; Chai, H.; Lee, M.; Miszard Kalaiselvam, H.; Radman, Q.; Haji, M.; Saad, K.; et al. The Effects of Cosmos caudatus (Ulam Raja) on Detoxifying Enzymes in Extrahepatic Organs in Mice ARTICLE INFO ABSTRACT. J. Appl. Pharm. Sci. 2015, 5, 82–88. [Google Scholar] [CrossRef]
- Shahar, S.; Earland, J.; Abdulrahman, S. Validation of a Dietary History Questionnaire against a 7-D Weighed Record for Estimating Nutrient Intake among Rural Elderly Malays. Malays. J. Nutr. 2000, 6, 33–44. [Google Scholar]
- Ibrahim, N.M.; Shohaimi, S.; Chong, H.T.; Rahman, A.H.; Razali, R.; Esther, E.; Basri, H.B. Validation study of the Mini-Mental State Examination in a Malay-speaking elderly population in Malaysia. Dement. Geriatr. Cogn. Disord. 2009, 27, 247–253. [Google Scholar] [CrossRef]
- Weshsler, D. Wechsler Adult Intelligence Scale-III; The Psychological Corporation San Antonio: San Antonio, TX, USA, 1997. [Google Scholar]
- Jamaluddin, R.; Othman, Z.; Musa, K.I.; Alwi, M.N.M. Validation of The Malay Version of Auditory Verbal Learning Test (Mvavlt) Among Schizophrenia Patients In Hospital Universiti Sains Malaysia (Husm), Malaysia. Asean J. Psychiatry 2009, 10, 54–68. [Google Scholar]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Profile of Mood States; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Gupta, U.; Verma, M. Placebo in clinical trials. Perspect. Clin. Res. 2013, 4, 49–52. [Google Scholar] [CrossRef]
- Ferri, P.; Angelino, D.; Gennari, L.; Benedetti, S.; Ambrogini, P.; Del Grande, P.; Ninfali, P. Enhancement of flavonoid ability to cross the blood-brain barrier of rats by co-administration with α-tocopherol. Food Funct. 2015, 6, 394–400. [Google Scholar] [CrossRef]
- Youdim, K.; Shukitt-Hale, B.; Joseph, J. Flavonoids and the brain: Interactions at the blood-brain barrier and their physiological effects on the central nervous system. Free Radic. Biol. Med. 2005, 37, 1683–1693. [Google Scholar] [CrossRef]
- Figueira, I.; Garcia, G.; Pimpão, R.C.; Terrasso, A.P.; Costa, I.; Almeida, A.F.; Tavares, L.; Pais, T.F.; Pinto, P.; Ventura, M.R.; et al. Polyphenols journey through blood-brain barrier towards neuronal protection. Sci. Rep. 2017, 7, 11456. [Google Scholar] [CrossRef] [PubMed]
- Rendeiro, C.; Rhodes, J.S.; Spencer, J.P. The mechanisms of action of flavonoids in the brain: Direct versus indirect effects. Neurochem. Int. 2015, 89, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Jäger, K.A.; Saaby, L. Flavonoids and the CNS. Molecules 2011, 16, 1471–1485. [Google Scholar] [CrossRef] [PubMed]
- Vauzour, D.; Vafeiadou, K.; Rodriguez-Mateos, A.; Rendeiro, C.; Spencer, J.P.E. The neuroprotective potential of flavonoids: A multiplicity of effects. Genes Nutr. 2008, 3, 115–126. [Google Scholar] [CrossRef]
- Folch, J.; Ettcheto, M.; Petrov, D.; Abad, S.; Pedros, I.; Marin, M.; Olloquequi, J.; Camins, A. Review of the advances in treatment for Alzheimer disease: Strategies for combating beta-amyloid protein. Neurologia 2018, 33, 47–58. [Google Scholar] [CrossRef]
- Jiang, N.; Doseff, A.I.; Grotewold, E. Flavones: From Biosynthesis to Health Benefits. Plants 2016, 5, 27. [Google Scholar] [CrossRef]
- Costa, L.G.; Garrick, J.M.; Roquè, P.J.; Pellacani, C. Mechanisms of Neuroprotection by Quercetin: Counteracting Oxidative Stress and More. Oxid. Med. Cell Longev 2016, 2016, 2986796. [Google Scholar] [CrossRef]
- Bigelman, K.; Chapman, D.; Freese, E.; Trilk, J.; Cureton, K. Effects of 6 Weeks of Quercetin Supplementation on Energy, Fatigue, and Sleep in ROTC Cadets. Mil. Med. 2011, 176, 565–572. [Google Scholar] [CrossRef]
- Spencer, J.P.; Rice-Evans, C.; Williams, R.J. Modulation of pro-survival Akt/protein kinase B and ERK1/2 signaling cascades by quercetin and its in vivo metabolites underlie their action on neuronal viability. J. Biol. Chem. 2003, 278, 34783–34793. [Google Scholar] [CrossRef]
- Ma, J.Q.; Luo, R.Z.; Jiang, H.X.; Liu, C.M. Quercitrin offers protection against brain injury in mice by inhibiting oxidative stress and inflammation. Food Funct. 2016, 7, 549–556. [Google Scholar] [CrossRef]
- Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C. The Immunomodulatory and Anti-Inflammatory Role of Polyphenols. Nutrients 2018, 10, 1618. [Google Scholar] [CrossRef] [PubMed]
- Udani, J.K. Effects of SuperUlam on Supporting Concentration and Mood: A Randomized, Double-Blind, Placebo-Controlled Crossover Study. Evid. Based Complement. Altern. Med. Ecam 2013, 2013, 238454. [Google Scholar] [CrossRef] [PubMed]
- Sayeed, M.S.B.; Shams, T.; Fahim Hossain, S.; Rahman, M.R.; Mostofa, A.; Fahim Kadir, M.; Mahmood, S.; Asaduzzaman, M. Nigella sativa L. seeds modulate mood, anxiety and cognition in healthy adolescent males. J. Ethnopharmacol. 2014, 152, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Daramola, B. Preliminary investigation on antioxidant interactions between bioactive components of Solanum anguivi and Capsicum annuum. J. Food Sci. Technol. 2018, 55, 3827–3832. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Tse, C.S.; Leung, G.T.; Fung, A.W.; Hau, K.T.; Chiu, H.F.; Lam, L.C. Bias in discriminating very mild dementia for older adults with different levels of education in Hong Kong. Int. Psychogeriatr. 2014, 26, 995–1010. [Google Scholar] [CrossRef] [PubMed]
- Suganthy, N.; Devi, K.P.; Nabavi, S.F.; Braidy, N.; Nabavi, S.M. Bioactive effects of quercetin in the central nervous system: Focusing on the mechanisms of actions. Biomed. Pharmacother. Biomed. Pharmacother. 2016, 84, 892–908. [Google Scholar] [CrossRef] [PubMed]
- García-Blanco, A.; Baquero, M.; Vento, M.; Gil, E.; Bataller, L.; Cháfer-Pericás, C. Potential oxidative stress biomarkers of mild cognitive impairment due to Alzheimer disease. J. Neurol. Sci. 2017, 373, 295–302. [Google Scholar] [CrossRef]
- Gaschler, M.M.; Stockwell, B.R. Lipid peroxidation in cell death. Biochem. Biophys. Res. Commun. 2017, 482, 419–425. [Google Scholar] [CrossRef]
- Wojsiat, J.; Zoltowska, K.M.; Laskowska-Kaszub, K.; Wojda, U. Oxidant/Antioxidant Imbalance in Alzheimer’s Disease: Therapeutic and Diagnostic Prospects. Oxid. Med. Cell Longev. 2018, 2018, 6435861. [Google Scholar] [CrossRef]
- Pisoschi, A.M.; Pop, A.; Cimpeanu, C.; Predoi, G. Antioxidant Capacity Determination in Plants and Plant-Derived Products: A Review. Oxid. Med. Cell Longev. 2016, 2016, 9130976. [Google Scholar] [CrossRef]
- Mandal, P.K.; Shukla, D.; Tripathi, M.; Ersland, L. Cognitive Improvement with Glutathione Supplement in Alzheimer’s Disease: A Way Forward. J. Alzheimer’s Dis. 2019, 68, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Youssef, P.; Chami, B.; Lim, J.; Middleton, T.; Sutherland, G.T.; Witting, P.K. Evidence supporting oxidative stress in a moderately affected area of the brain in Alzheimer’s disease. Sci. Rep. 2018, 8, 11553. [Google Scholar] [CrossRef] [PubMed]
- Winterbourn, C.C. Revisiting the reactions of superoxide with glutathione and other thiols. Arch. Biochem. Biophys. 2016, 595, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.J.; Prickril, B.; Rasooly, A. Mechanisms of Phytonutrient Modulation of Cyclooxygenase-2 (COX-2) and Inflammation Related to Cancer. Nutr. Cancer 2018, 70, 350–375. [Google Scholar] [CrossRef] [PubMed]
- Kelly, Á.M. Exercise-Induced Modulation of Neuroinflammation in Models of Alzheimer’s Disease. Brain Plast. 2018, 4, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.; Kondev, V.; Bedse, G.; Baldi, R.; Marcus, D.; Patel, S. Cyclooxygenase-2 inhibition reduces anxiety-like behavior and normalizes enhanced amygdala glutamatergic transmission following chronic oral corticosterone treatment. Neurobiol. Stress 2019, 11, 100190. [Google Scholar] [CrossRef]
- Newcombe, E.A.; Camats-Perna, J.; Silva, M.L.; Valmas, N.; Huat, T.J.; Medeiros, R. Inflammation: The link between comorbidities, genetics, and Alzheimer’s disease. J. Neuroinflamm. 2018, 15, 276. [Google Scholar] [CrossRef]
- Shahar, S.; Lau, H.; Puteh, S.E.W.; Amara, S.; Razak, N.A. Health, access and nutritional issues among low-income population in Malaysia: Introductory note. BMC Public Health 2019, 19, 552. [Google Scholar] [CrossRef]
- Siwek, M.; Dudek, D.; Rybakowski, J.; Łojko, D.; Pawłowski, T.; Kiejna, A. Mood Disorder Questionnaire—Characteristic and indications. Psychiatr. Pol. 2009, 43, 287–299. [Google Scholar]
- McGhie, T.K.; Rowan, D.D. Metabolomics for measuring phytochemicals, and assessing human and animal responses to phytochemicals, in food science. Mol. Nutr. Food Res. 2012, 56, 147–158. [Google Scholar] [CrossRef]
- Beckonert, O.; Keun, H.C.; Ebbels, T.M.; Bundy, J.; Holmes, E.; Lindon, J.C.; Nicholson, J.K. Metabolic profiling, metabolomic and metabonomic procedures for NMR spectroscopy of urine, plasma, serum and tissue extracts. Nat. Protoc. 2007, 2, 2692–2703. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Nutrients | CC Supplement | Placebo |
|---|---|---|
| Energy (kcal) | 284 ± 4 | 376 ± 3 |
| Carbohydrate (g) | 47.35 ± 0.92 | 94.05 ± 0.64 |
| Protein (g) | 20.30 ± 0.42 | 0 |
| Fat (g) | 1.40 ± 0.14 | 0 |
| Ash content (g) | 26.70 ± 1.27 | 0.05 ± 0.07 |
| Moisture content (g) | 4.25 ± 0.49 | 5.85 ± 0.50 |
| Vitamin A Retinol (mg) | 0 | 0 |
| Vitamin C (mg) | 100.50 ± 2.12 | 0 |
| Vitamin E Alpha-Tocopherol (mg) | 2.10 ± 0.42 | 0 |
| Calcium (mg) | 2255.00 ± 7.07 | 9.06 ± 0.54 |
| Iron (mg) | 7.69 ± 0.16 | 0.62 ± 0.13 |
| Potassium (mg) | 9610 ± 466.69 | 15.00 ± 0.71 |
| Sodium (mg) | 71.60 ± 5.52 | 69.15 ± 2.62 |
| Zinc (mg) | 2.77 ± 0.52 | 0.70 ± 0.14 |
| Total Dietary Fibre (g) | 7.80 ± 2.97 | 1.8 ± 0.14 |
| Total phenolic content (mg Gallic acid equivalent) | 1482 ± 101 | 3.56 ± 0.10 |
| DPPH (mmol Trolox equivalent) | 330.86 ± 9.48 | 4.57 ± 2.01 |
| FRAP (mmol Trolox equivalent) | 393.57 ± 9.78 | 1.45 ± 1.17 |
| Quercetin (%w/w) | 0.9 | NA |
| Quercitrin (%w/w) | 1.0 | NA |
| Outcomes | Neuropsychological Assessment |
|---|---|
| Primary outcomes | |
| MMSE | Global cognitive function |
| Digit Span | Attention and working memory |
| RAVLT (immediate and delayed recall) | Verbal immediate memory |
| VR (immediate and delayed recall) | Visuo–spatial function |
| Digit symbol substitution | Psychomotor speed |
| POMS | Tension, depression, anger, fatigue, esteem-related effect, vigor, and confusion |
| Secondary outcomes | |
| Biomarkers | BDNF, MDA, iNOS, COX-2, SOD, GSH |
| Biochemical profiles | Fasting blood sugar, lipid profile, liver function test, renal function test |
| Parameter | CC Supplement (n = 24) | Placebo (n = 24) | Total (n = 48) | p-Value |
|---|---|---|---|---|
| Age 1 | 65.83 ± 4.35 | 64.42 ± 3.71 | 65.11 ± 4.05 | 0.237 |
| Gender 2 | 0.917 | |||
| Male | 8 (33.33) | 8 (33.3) | 16 (33.3) | |
| Female | 16 (66.7) | 16 (66.7) | 32 (66.7) | |
| Ethnicity 2 | 0.483 | |||
| Malay | 16 (66.7) | 13 (54.2) | 29 (60.4) | |
| Chinese | 6 (25.0) | 10 (41.7) | 16 (33.3) | |
| Indian | 2 (8.3) | 1 (4.2) | 3 (6.3) | |
| Formal education (years) 1 | 11.39 ± 2.39 | 10.17 ± 3.20 | 10.77 ± 2.87 | 0.145 |
| Education level 2 | 0.184 | |||
| Primary school | 1 (4.2) | 3 (12.5) | 4 (8.3) | |
| Secondary school | 13 (54.2) | 17 (70.8) | 30 (62.5) | |
| Diploma/Certificate | 9 (37.5) | 3 (12.5) | 12 (25.0) | |
| Degree | 1 (4.2) | 1 (4.2) | 2 (4.2) | |
| Marital status 2 | 0.123 | |||
| Single | 1 (4.2) | 3 (12.5) | 4 (8.3) | |
| Married | 22 (91.7) | 15 (62.5) | 37 (77.1) | |
| Divorce | 0 (0) | 2 (8.3) | 2 (4.2) | |
| Widow/widower | 1 (4.2) | 4 (16.7) | 5 (10.4) | |
| Household income (RM) 1 | 2021.83 ± 904.81 | 1962.58 ± 801.86 | 1991.57 ± 844.94 | 0.813 |
| Hypertension 2 | 0.159 | |||
| Yes | 6 (25.0) | 11 (45.8) | 17 (35.4) | |
| No | 18 (75.0) | 13 (54.2) | 31 (64.6) | |
| Diabetes 2 | 0.671 | |||
| Yes | 6 (25.0) | 5 (20.8) | 11 (22.9) | |
| No | 18 (75.0) | 19 (79.2) | 37 (77.1) | |
| Hyperlipidaemia 2 | 0.587 | |||
| Yes | 7 (29.2) | 8 (33.3) | 15 (31.3) | |
| No | 17 (70.8) | 16 (66.7) | 33 (68.7) | |
| Others 2 | 0.975 | |||
| Yes | 1 (4.2) | 1 (4.2) | 2 (4.2) | |
| No | 23 (95.8) | 23 (95.8) | 46 (95.8) | |
| Physical activity 2 | 0.591 | |||
| Everyday | 1 (4.2) | 0 (0) | 1 (2.1) | |
| 3–5 times per week | 7 (29.2) | 4 (16.7) | 11 (22.9) | |
| 1–2 times per week | 8 (33.3) | 11 (45.8) | 19 (39.6) | |
| None | 8 (33.3) | 9 (37.5) | 17 (35.4) | |
| Body mass index (kg/m2) | 25.67 ± 3.02 | 25.72 ± 2.29 | 25.70 ± 2.64 | 0.952 |
| CC Supplement (n = 23) | Placebo (n = 24) | Treatment × Time Effect | |||
|---|---|---|---|---|---|
| p | Partial Eta Squared | Power | |||
| Mini-mental State Examination (MMSE) | |||||
| Baseline | 27.09 ± 1.38 | 26.58 ± 1.35 | 0.049 * | 0.150 | 0.586 |
| 6th week | 28.30 ± 0.70 | 26.92 ± 1.02 | |||
| 12th week | 28.91 ± 0.95 | 27.38 ± 1.28 | |||
| Digit Span | |||||
| Baseline | 8.39 ± 1.23 | 7.92 ± 1.28 | 0.466 | 0.040 | 0.173 |
| 6th week | 10.09 ± 1.41 | 8.58 ± 2.34 | |||
| 12th week | 10.91 ± 1.70 | 9.50 ± 2.59 | |||
| RAVLT (Immediate Recall) | |||||
| Baseline | 6.30 ± 1.02 | 6.29 ± 1.12 | 0.058 | 0.143 | 0.560 |
| 6th week | 10.22 ± 1.28 | 8.96 ± 1.76 | |||
| 12th week | 11.26 ± 2.18 | 10.75 ± 2.29 | |||
| RAVLT (Delayed recall) | |||||
| Baseline | 5.74 ± 0.92 | 5.63 ± 1.24 | 0.070 | 0.068 | 0.529 |
| 6th week | 9.39 ± 1.37 | 7.83 ± 1.49 | |||
| 12th week | 9.96 ± 2.65 | 9.58 ± 3.02 | |||
| Digit Symbol | |||||
| Baseline | 8.87 ± 1.71 | 8.00 ± 2.63 | 0.264 | 0.069 | 0.278 |
| 6th week | 10.04 ± 2.01 | 8.88 ± 2.59 | |||
| 12th week | 10.48 ± 1.97 | 9.88 ± 2.89 | |||
| Visual Reproduction (Immediate recall) | |||||
| Baseline | 32.22 ± 4.62 | 29.50 ± 6.45 | 0.212 | 0.080 | 0.320 |
| 6th week | 34.83 ± 3.30 | 29.54 ± 7.25 | |||
| 12th week | 35.13 ± 3.94 | 30.88 ± 7.06 | |||
| Visual reproduction (delayed recall) | |||||
| Baseline | 31.61 ± 6.06 | 27.83 ± 7.98 | 0.242 | 0.074 | 0.295 |
| 6th week | 35.13 ± 4.35 | 28.88 ± 7.85 | |||
| 12th week | 35.30 ± 3.40 | 29.88 ± 8.73 | |||
| Tension | |||||
| Baseline | 5.09 ± 3.46 | 6.67 ± 3.95 | 0.018 * | 0.191 | 0.733 |
| 6th week | 3.91 ± 2.04 | 6.13 ± 2.53 | |||
| 12th week | 3.22 ± 1.65 | 5.46 ± 2.25 | |||
| Anger | |||||
| Baseline | 1.47 ± 0.92 | 2.58 ± 1.16 | 0.139 | 0.099 | 0.401 |
| 6th week | 1.13 ± 1.58 | 3.21 ± 1.83 | |||
| 12th week | 1.09 ± 0.64 | 3.08 ± 2.39 | |||
| Fatigue | |||||
| Baseline | 3.65 ± 2.53 | 5.17 ± 2.35 | 0.811 | 0.011 | 0.081 |
| 6th week | 4.17 ± 1.87 | 5.33 ± 2.91 | |||
| 12th week | 4.00 ± 1.57 | 5.54 ± 1.25 | |||
| Depression | |||||
| Baseline | 1.70 ± 0.36 | 3.00 ± 1.22 | 0.921 | 0.004 | 0.062 |
| 6th week | 1.39 ± 0.37 | 2.38 ± 2.20 | |||
| 12th week | 1.34 ± 0.77 | 2.17 ± 1.93 | |||
| Esteem-related effect | |||||
| Baseline | 16.74 ± 2.88 | 14.54 ± 3.06 | 0.149 | 0.095 | 0.387 |
| 6th week | 17.30 ± 1.69 | 15.21 ± 3.46 | |||
| 12th week | 18.35 ± 1.34 | 15.00 ±2.83 | |||
| Vigor | |||||
| Baseline | 12.83 ± 3.39 | 10.25 ± 3.72 | 0.050 | 0.243 | 0.862 |
| 6th week | 13.30 ± 1.55 | 10.29 ± 2.16 | |||
| 12th week | 14.35 ± 2.17 | 9.00 ± 2.11 | |||
| Confusion | |||||
| Baseline | 2.74 ± 1.15 | 4.13 ± 1.84 | 0.983 | 0.001 | 0.052 |
| 6th week | 3.22 ± 2.15 | 3.88 ± 2.86 | |||
| 12th week | 2.00 ± 1.45 | 2.83 ± 1.34 | |||
| Total mood disturbance | |||||
| Baseline | 85.09 ± 10.58 | 96.75 ± 12.74 | 0.028 * | 0.171 | 0.672 |
| 6th week | 83.22 ± 6.18 | 95.42 ± 12.04 | |||
| 12th week | 78.96 ± 5.06 | 95.08 ± 9.08 | |||
| CC Supplement (n = 23) | Placebo (n = 24) | Treatment × Time Effect | |||
|---|---|---|---|---|---|
| p | Partial Eta Squared | Power | |||
| Brain derived neurotrophic factor (BDNF) (pg/mL) | |||||
| Baseline | 180.80 ± 86.42 | 180.09 ± 95.78 | 0.884 | 0.001 | 0.052 |
| 12th week | 194.74 ± 137.49 | 171.22 ± 113.87 | |||
| Inducible nitric oxide synthase (iNOS) (pg/mL) | |||||
| Baseline | 220.38 ± 66.56 | 218.99 ± 74.66 | 0.994 | 0.000 | 0.050 |
| 12th week | 216.34 ± 81.39 | 219.64 ± 80.67 | |||
| Cyclooxygenase-2 (COX-2) (ng/mL) | |||||
| Baseline | 0.86 ± 0.42 | 1.08 ± 0.59 | 0.867 | 0.001 | 0.053 |
| 12th week | 0.78 ± 0.43 | 1.15 ± 0.70 | |||
| Superoxide dismutase (SOD) (pg/mL) | |||||
| Baseline | 49.13 ± 3.81 | 49.46 ± 2.64 | 0.577 | 0.008 | 0.085 |
| 12th week | 51.63 ± 2.04 | 51.22 ± 3.50 | |||
| Malondialdehyde (MDA) (ng/mL) | |||||
| Baseline | 350.14 ±161.08 | 358.21 ± 172.59 | 0.047 * | 0.097 | 0.516 |
| 12th week | 313.32 ± 153.35 | 398.94 ± 181.85 | |||
| Glutathione (GSH) (mM) | |||||
| Baseline | 0.46 ± 0.09 | 0.48 ± 0.05 | 0.111 | 0.064 | 0.356 |
| 12th week | 0.50 ± 0.06 | 0.48 ± 0.07 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
You, Y.X.; Shahar, S.; Rajab, N.F.; Haron, H.; Yahya, H.M.; Mohamad, M.; Din, N.C.; Maskat, M.Y. Effects of 12 Weeks Cosmos caudatus Supplement among Older Adults with Mild Cognitive Impairment: A Randomized, Double-Blind and Placebo-Controlled Trial. Nutrients 2021, 13, 434. https://doi.org/10.3390/nu13020434
You YX, Shahar S, Rajab NF, Haron H, Yahya HM, Mohamad M, Din NC, Maskat MY. Effects of 12 Weeks Cosmos caudatus Supplement among Older Adults with Mild Cognitive Impairment: A Randomized, Double-Blind and Placebo-Controlled Trial. Nutrients. 2021; 13(2):434. https://doi.org/10.3390/nu13020434
Chicago/Turabian StyleYou, Yee Xing, Suzana Shahar, Nor Fadilah Rajab, Hasnah Haron, Hanis Mastura Yahya, Mazlyfarina Mohamad, Normah Che Din, and Mohamad Yusof Maskat. 2021. "Effects of 12 Weeks Cosmos caudatus Supplement among Older Adults with Mild Cognitive Impairment: A Randomized, Double-Blind and Placebo-Controlled Trial" Nutrients 13, no. 2: 434. https://doi.org/10.3390/nu13020434
APA StyleYou, Y. X., Shahar, S., Rajab, N. F., Haron, H., Yahya, H. M., Mohamad, M., Din, N. C., & Maskat, M. Y. (2021). Effects of 12 Weeks Cosmos caudatus Supplement among Older Adults with Mild Cognitive Impairment: A Randomized, Double-Blind and Placebo-Controlled Trial. Nutrients, 13(2), 434. https://doi.org/10.3390/nu13020434