Antioxidant Barrier, Redox Status, and Oxidative Damage to Biomolecules in Patients with Colorectal Cancer. Can Malondialdehyde and Catalase Be Markers of Colorectal Cancer Advancement?

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Collection
2.3. Determination of Redox Markers
2.4. Enzymatic and Non-Enzymatic Antioxidants
2.5. Total Antioxidant/Oxidant Status
2.6. Oxidative Damage Products
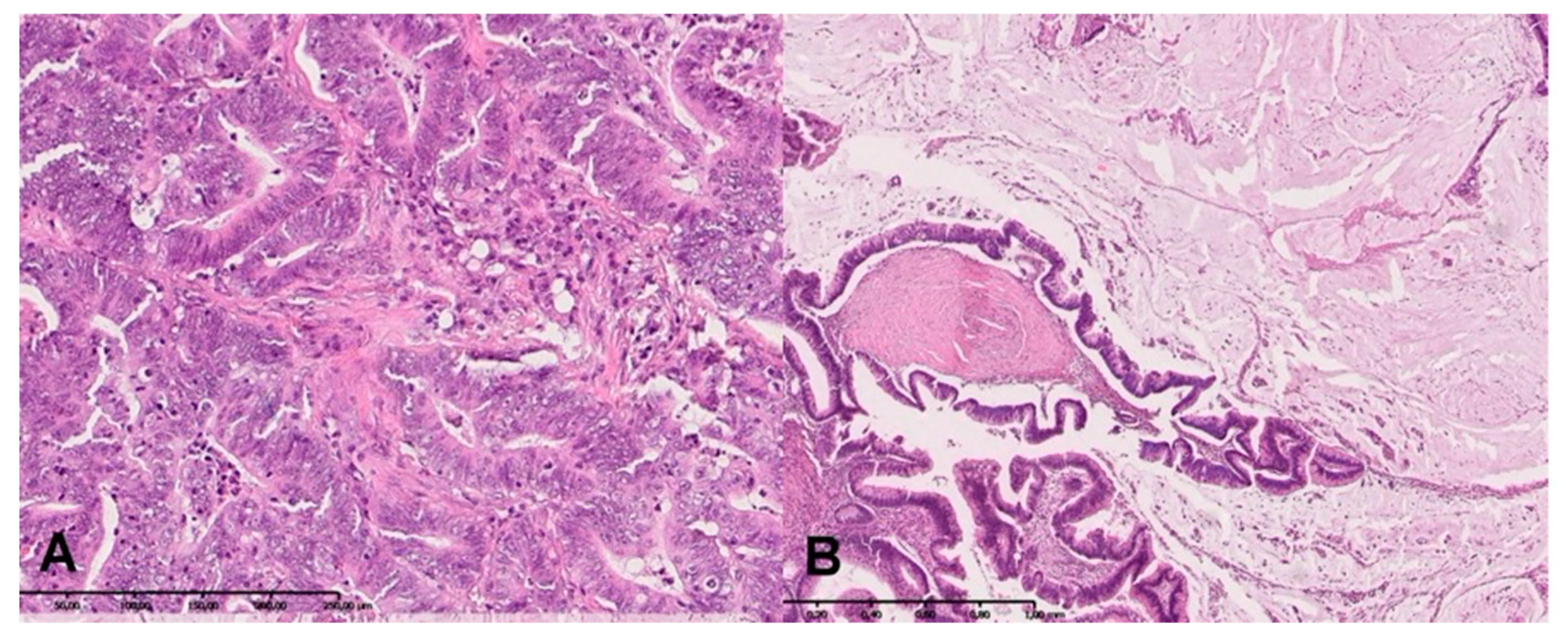
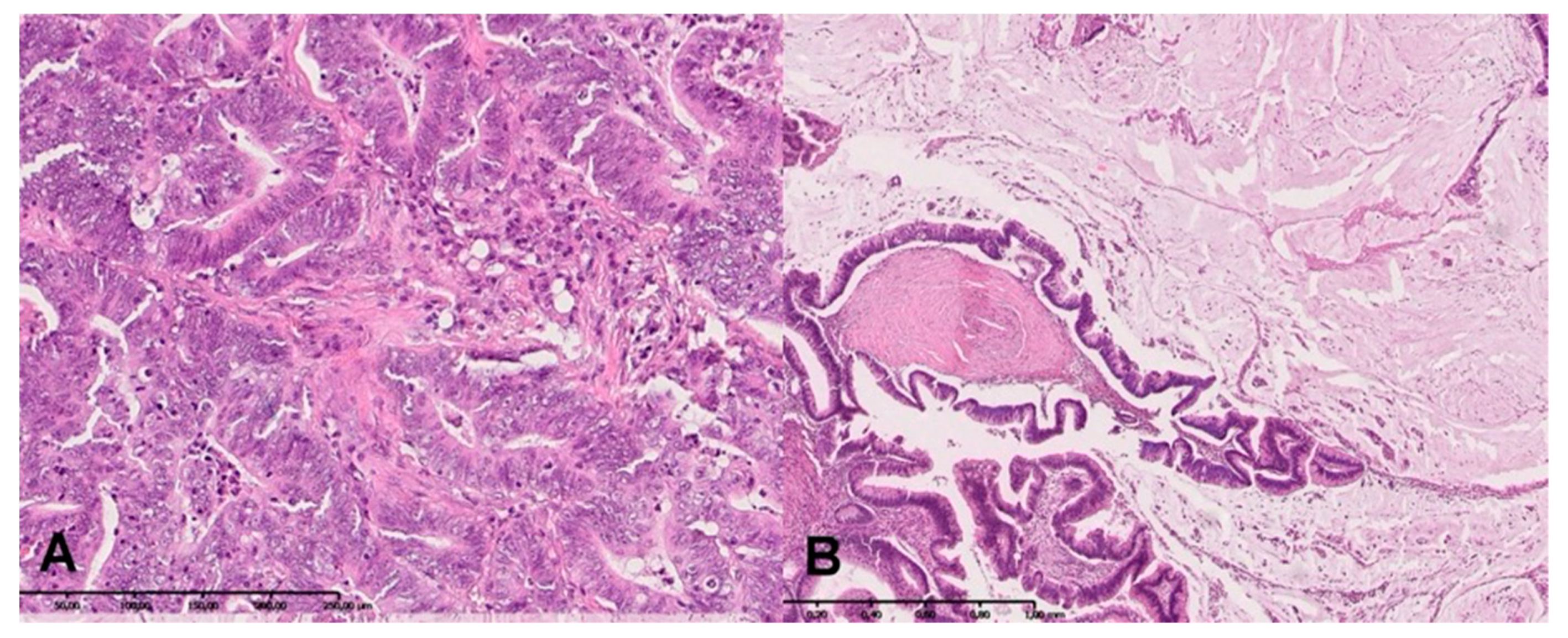
2.7. H + E Staining
2.8. Statistical Analysis
3. Results
3.1. Clinical Findings
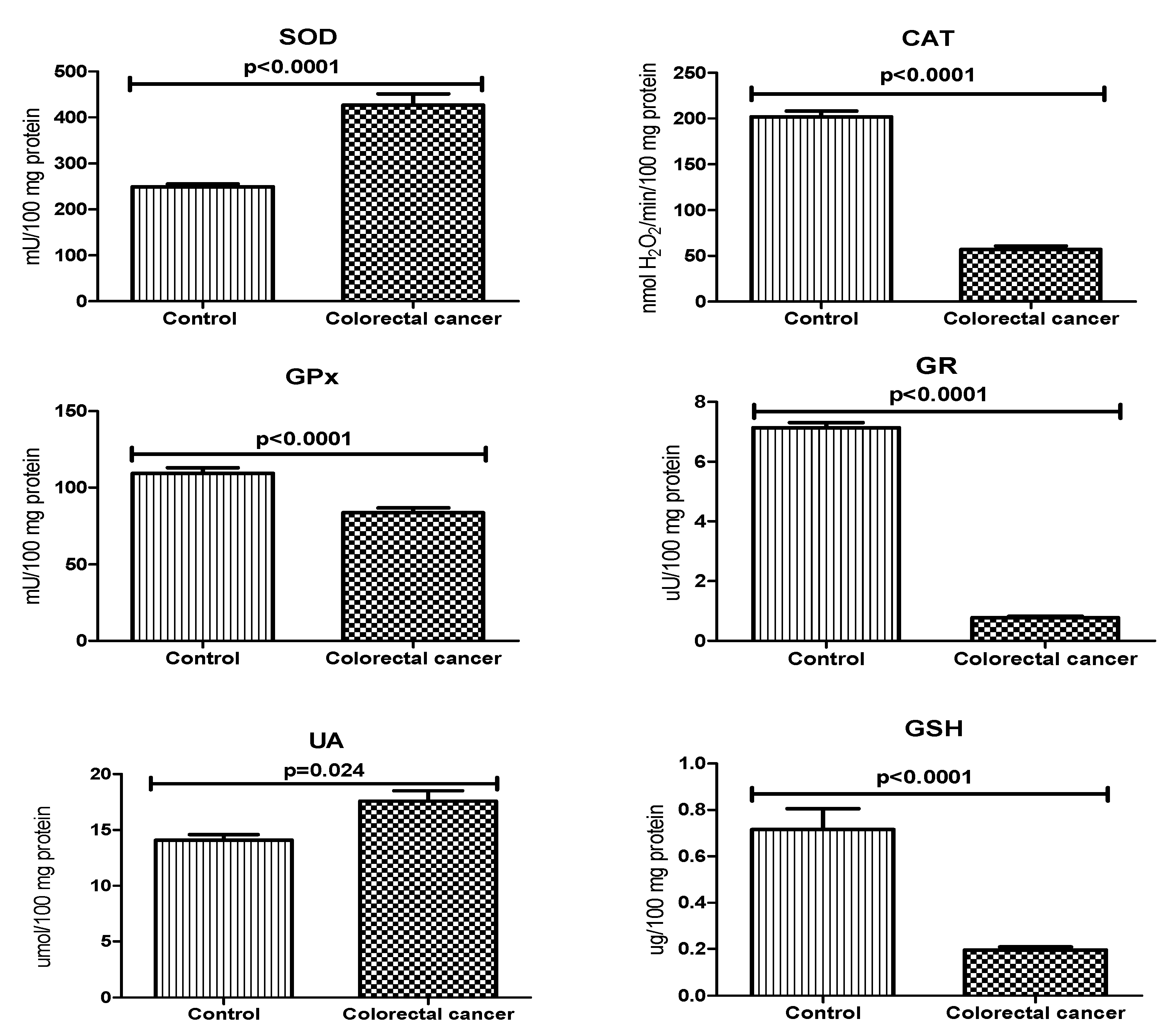
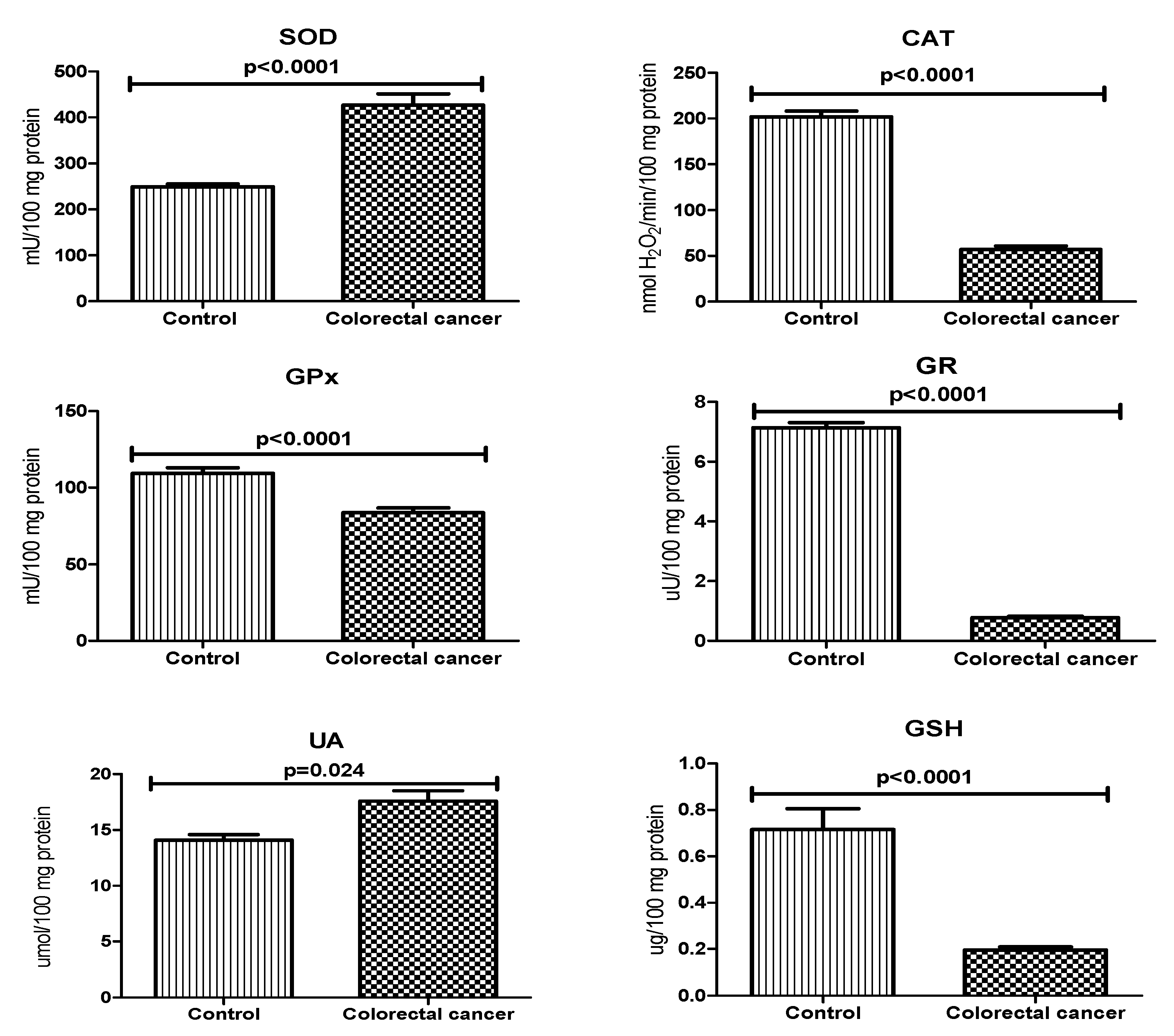
3.2. Antioxidant Defence
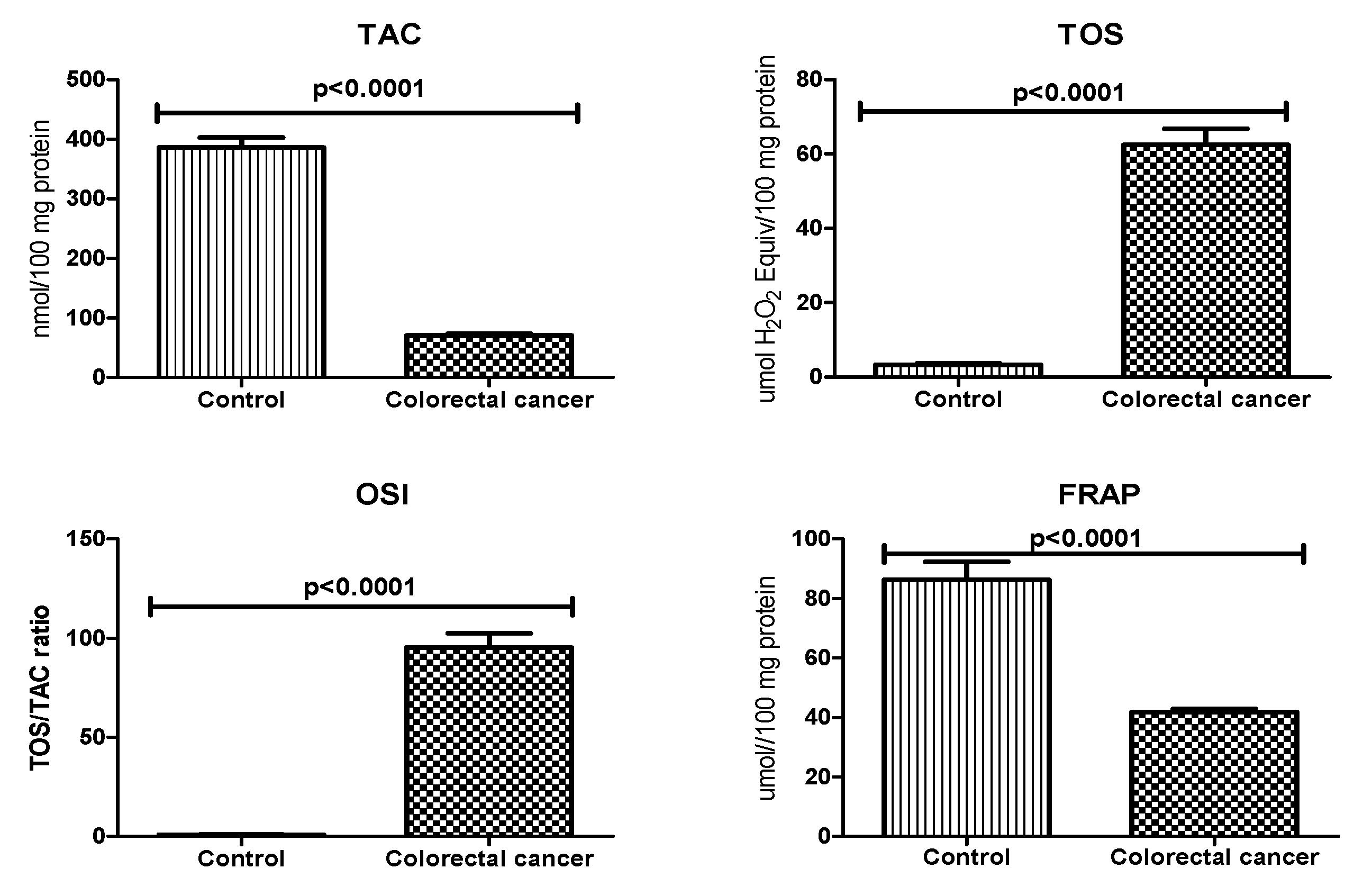
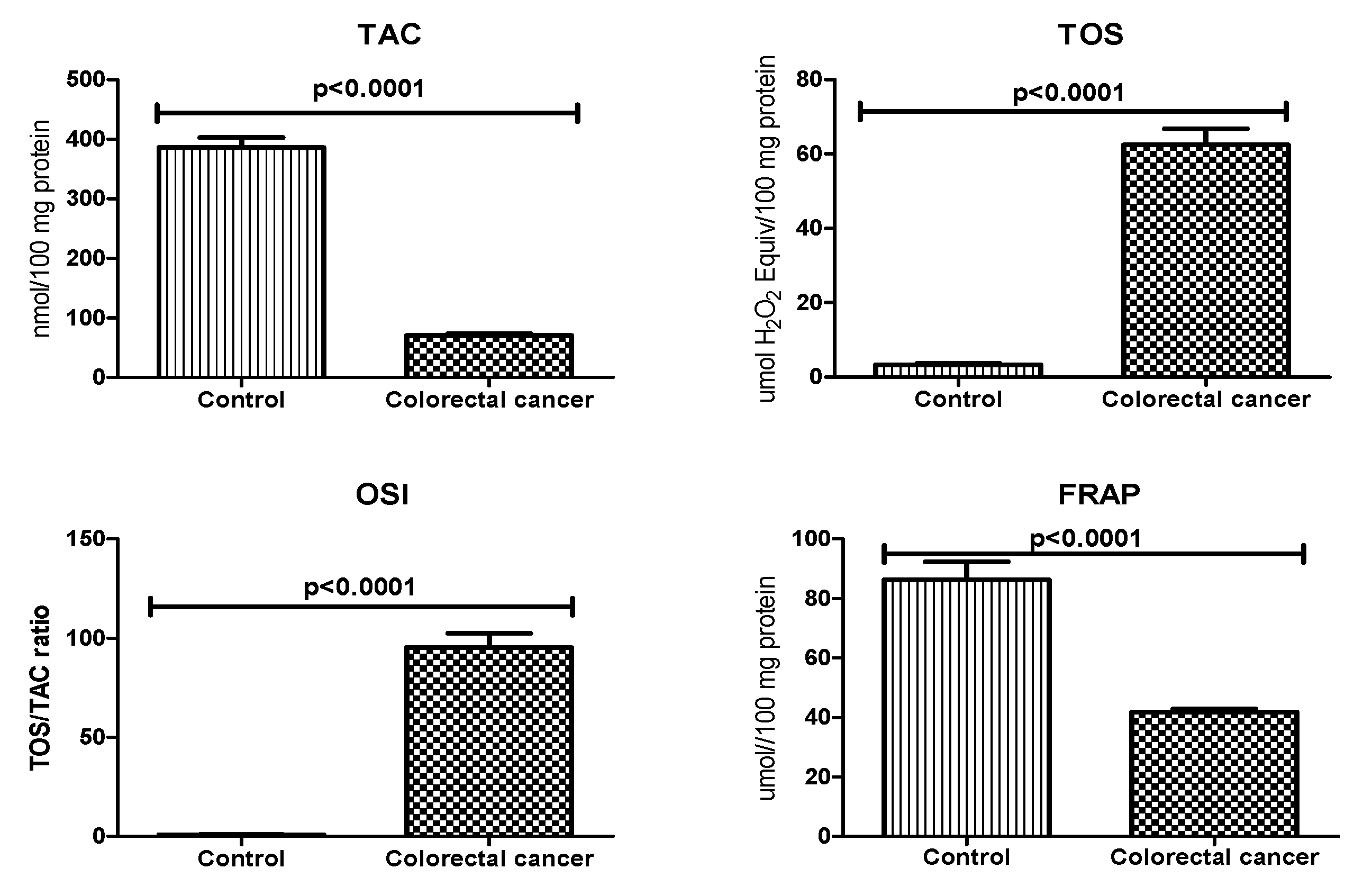
3.3. Total Antioxidant/Oxidant Status
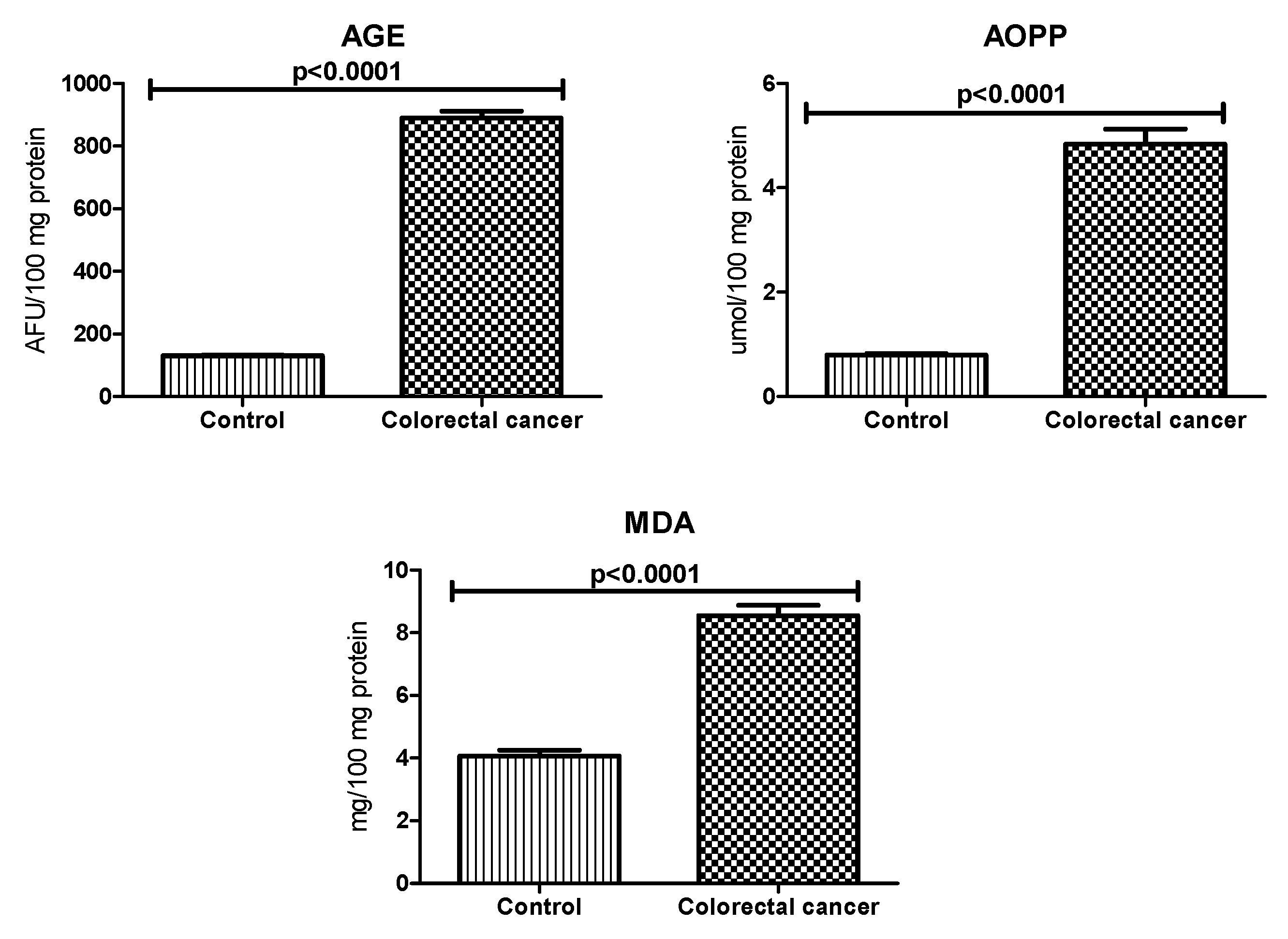
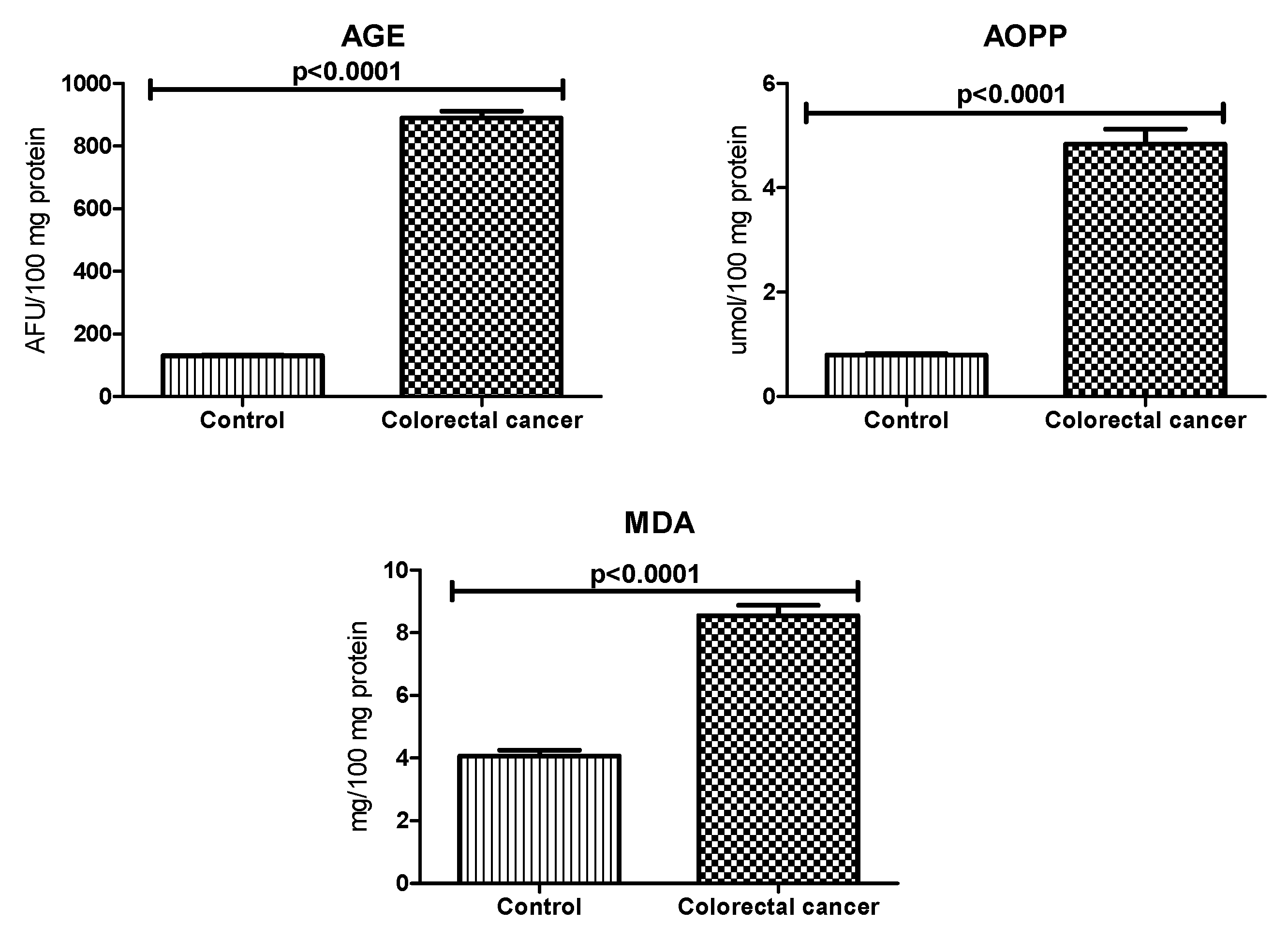
3.4. Oxidative Damage Products
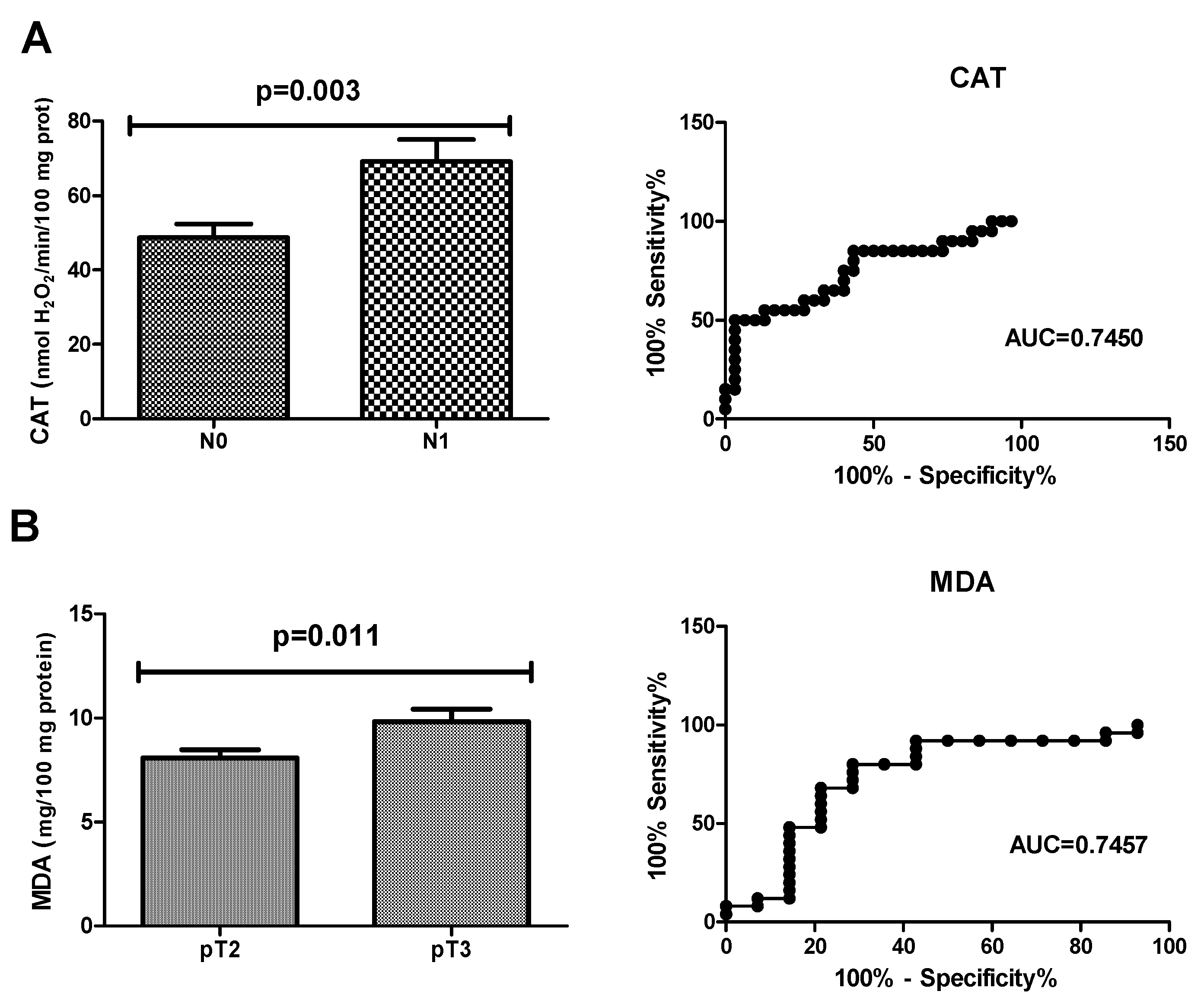
3.5. ROC Analysis
3.6. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Das, V.; Kalita, J.; Pal, M. Predictive and prognostic biomarkers in colorectal cancer: A systematic review of recent advances and challenges. Biomed. Pharmacother. 2017, 87, 8–19. [Google Scholar] [CrossRef]
- Pino, M.S.; Chung, D.C. The chromosomal instability pathway in colon cancer. Gastroenterology 2010, 138, 2059–2072. [Google Scholar] [CrossRef]
- Limoli, C.L.; Giedzinski, E. Induction of Chromosomal Instability by Chronic Oxidative Stress. Neoplasia 2003, 5, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Mena, S.; Ortega, A.; Estrela, J.M. Oxidative stress in environmental-induced carcinogenesis. Mutat. Res. Toxicol. Environ. Mutagen. 2009, 674, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Carini, F.; Mazzola, M.; Rappa, F.; Jurjus, A.; Geagea, A.G.; Al Kattar, S.; Bou-Assi, T.; Jurjus, R.; Damiani, P.; Leone, A.; et al. Colorectal Carcinogenesis: Role of Oxidative Stress and Antioxidants. Anticancer. Res. 2017, 37, 4759–4766. [Google Scholar] [PubMed] [Green Version]
- Mandal, P. Potential biomarkers associated with oxidative stress for risk assessment of colorectal cancer. Naunyn-Schmiedeberg’s Arch. Pharm. 2017, 390, 557–565. [Google Scholar] [CrossRef]
- Poprac, P.; Jomova, K.; Simunkova, M.; Kollar, V.; Rhodes, C.J.; Valko, M. Targeting Free Radicals in Oxidative Stress-Related Human Diseases. Trends Pharmacol. Sci. 2017, 38, 592–607. [Google Scholar] [CrossRef]
- Friguet, B. Oxidized protein degradation and repair in ageing and oxidative stress. FEBS Lett. 2006, 580, 2910–2916. [Google Scholar] [CrossRef] [Green Version]
- Valko, M.; Rhodes, C.; Moncol, J.; Izakovic, M.; Mazur, M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem. Interact. 2006, 160, 1–40. [Google Scholar] [CrossRef]
- Fejfer, K.; Buczko, P.; Niczyporuk, M.; Ładny, J.R.; Hady, H.R.; Knaś, M.; Waszkiel, D.; Klimiuk, A.; Zalewska, A.; Maciejczyk, M. Oxidative Modification of Biomolecules in the Nonstimulated and Stimulated Saliva of Patients with Morbid Obesity Treated with Bariatric Surgery. BioMed Res. Int. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouvreau, C.; Dayre, A.; Butkowski, E.G.; De Jong, B.; Jelinek, H.F. Inflammation and oxidative stress markers in diabetes and hypertension. J. Inflamm. Res. 2018, 11, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Maciejczyk, M.; Szulimowska, J.; Skutnik, A.; Taranta-Janusz, K.; Wasilewska, A.; Wiśniewska, N.; Zalewska, A. Salivary Biomarkers of Oxidative Stress in Children with Chronic Kidney Disease. J. Clin. Med. 2018, 7, 209. [Google Scholar] [CrossRef] [PubMed]
- Klimiuk, A.; Maciejczyk, M.; Choromańska, M.; Fejfer, K.; Waszkiewicz, N.; Zalewska, A. Salivary Redox Biomarkers in Different Stages of Dementia Severity. J. Clin. Med. 2019, 8, 840. [Google Scholar] [CrossRef] [PubMed]
- Sawczuk, B.; Maciejczyk, M.; Sawczuk-Siemieniuk, M.; Posmyk, R.; Zalewska, A.; Car, H. Salivary Gland Function, Antioxidant Defence and Oxidative Damage in the Saliva of Patients with Breast Cancer: Does the BRCA1 Mutation Disturb the Salivary Redox Profile? Cancers 2019, 11, 1501. [Google Scholar] [CrossRef]
- Bosman, F.; Carneiro, F.; Hruban, R.; Theise, N. WHO Classification of Tumours of the Digestive System, 4th ed.; International World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Kołodziej, U.; Maciejczyk, M.; Miąsko, A.; Matczuk, J.; Knaś, M.; Żukowski, P.; Żendzian-Piotrowska, M.; Borys, J.; Zalewska, A. Oxidative Modification in the Salivary Glands of High Fat-Diet Induced Insulin Resistant Rats. Front. Physiol. 2017, 8, 736. [Google Scholar] [CrossRef]
- Walker, J.M. The bicinchoninic acid (BCA) assay for protein quantitation. Methods Mol. Biol. 1994, 32, 5–8. [Google Scholar]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J. Boil. Chem. 1972, 247, 3170–3175. [Google Scholar]
- Aebi, H. Catalase in vitro. Methods Enzym. 1984, 105, 121–126. [Google Scholar]
- E Paglia, D.; Valentine, W.N. Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J. Lab. Clin. Med. 1967, 70, 158–169. [Google Scholar]
- Mize, C.E.; Langdon, R.G. Hepatic glutathione reductase. I. Purification and general kinetic properties. J. Biol. Chem. 1962, 237, 1589–1595. [Google Scholar] [PubMed]
- Griffith, O.W. Determination of glutathione and glutathione disulfide using glutathione reductase and 2-vinylpyridine. Anal. Biochem. 1980, 106, 207–212. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef]
- Knaś, M.; Maciejczyk, M.; Daniszewska, I.; Klimiuk, A.; Matczuk, J.; Kołodziej, U.; Waszkiel, D.; Ładny, J.R.; Żendzian-Piotrowska, M.; Zalewska, A. Oxidative Damage to the Salivary Glands of Rats with Streptozotocin-Induced Diabetes-Temporal Study: Oxidative Stress and Diabetic Salivary Glands. J. Diabetes Res. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Benzie, I.F.; Strain, J. The Ferric Reducing Ability of Plasma (FRAP) as a Measure of “Antioxidant Power”: The FRAP Assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef]
- Kalousová, M.; Skrha, J.; Zima, T. Advanced glycation end-products and advanced oxidation protein products in patients with diabetes mellitus. Physiol. Res. 2002, 51, 597–604. [Google Scholar]
- Buege, J.A.; Aust, S.D. Microsomal lipid peroxidation. Methods Enzym. 1978, 52, 302–310. [Google Scholar]
- Maciejczyk, M.; Żebrowska, E.; Chabowski, A. Insulin Resistance and Oxidative Stress in the Brain: What’s New? Int. J. Mol. Sci. 2019, 20, 874. [Google Scholar] [CrossRef]
- Gopcevic, K.R.; Rovčanin, B.R.; Tatić, S.B.; Krivokapić, Z.V.; Gajic, M.M.; Dragutinović, V.V. Activity of Superoxide Dismutase, Catalase, Glutathione Peroxidase, and Glutathione Reductase in Different Stages of Colorectal Carcinoma. Dig. Dis. Sci. 2013, 58, 2646–2652. [Google Scholar] [CrossRef]
- Chiang, F.-F.; Wang, H.-M.; Lan, Y.-C.; Yang, M.-H.; Huang, S.-C.; Huang, Y.-C. High homocysteine is associated with increased risk of colorectal cancer independently of oxidative stress and antioxidant capacities. Clin. Nutr. 2014, 33, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Lushchak, V.I. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Interactions 2014, 224, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Mayo, J.C.; Tan, D.-X.; Sainz, R.M.; Lopez-Burillo, S.; Reiter, R.J. Oxidative damage to catalase induced by peroxyl radicals: Functional protection by melatonin and other antioxidants. Free. Radic. Res. 2003, 37, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Perše, M. Oxidative stress in the pathogenesis of colorectal cancer: Cause or consequence? Biomed Res. Int. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Perše, M.; Injac, R.; Štrukelj, B.; Cerar, A. High fat mixed lipid diet modifies protective effects of exercise on 1,2 dimethylhydrazine induced colon cancer in rats. Technol. Cancer Res. Treat. 2012, 11, 289–299. [Google Scholar] [CrossRef]
- Perse, M.; Injac, R.; Strukelj, B.; Cerar, A. Effects of high-fat mixed-lipid diet and exercise on the antioxidant system in skeletal and cardiac muscles of rats with colon carcinoma. Pharmacol. Rep. 2009, 61, 909–916. [Google Scholar] [CrossRef]
- Perše, M.; Cerar, A. Morphological and molecular alterations in 1,2 dimethylhydrazine and azoxymethane induced colon carcinogenesis in rats. J. Biomed. Biotechnol. 2011, 2011, 473964. [Google Scholar]
- Zalewska, A.; Ziembicka, D.; Żendzian-Piotrowska, M.; Maciejczyk, M. The Impact of High-Fat Diet on Mitochondrial Function, Free Radical Production, and Nitrosative Stress in the Salivary Glands of Wistar Rats. Oxid. Med. Cell. Longev. 2019, 2019. [Google Scholar] [CrossRef]
- Aleksandrova, K.; Nimptsch, K.; Pischon, T. Influence of Obesity and Related Metabolic Alterations on Colorectal Cancer Risk. Curr. Nutr. Rep. 2013, 2, 1–9. [Google Scholar] [CrossRef]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [Green Version]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid Peroxidation: Production, Metabolism, and Signaling Mechanisms of Malondialdehyde and 4-Hydroxy-2-Nonenal. Oxidative Med. Cell. Longev. 2014, 2014, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Klaunig, J.E.; Kamendulis, L.M. Therole Ofoxidativestress Incarcinogenesis. Annu. Rev. Pharmacol. Toxicol. 2004, 44, 239–267. [Google Scholar] [CrossRef] [PubMed]
- Adams, S. Reactive carbonyl formation by oxidative and non-oxidative pathways. Front. Biosci. 2001, 6, a17. [Google Scholar] [CrossRef]
- Alderman, C.J.J.; Shah, S.; Foreman, J.C.; Chain, B.M.; Katz, D.R. The role of advanced oxidation protein products in regulation of dendritic cell function. Free. Radic. Boil. Med. 2002, 32, 377–385. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, L.; Rong, S.; Qu, H.; Zhang, Y.; Chang, D.; Pan, H.; Wang, W. Relation between Gastric Cancer and Protein Oxidation, DNA Damage, and Lipid Peroxidation. Oxidative Med. Cell. Longev. 2013, 2013, 1–6. [Google Scholar] [CrossRef]
- Kosova, F.; Çetin, B.; Akıncı, M.; Aslan, S.; Arı, Z.; Sepici, A.; Altan, N.; Cetin, A.; Akinci, M.; Ari, Z. Advanced Oxidation Protein Products, Ferrous Oxidation in Xylenol Orange, and Malondialdehyde Levels in Thyroid Cancer. Ann. Surg. Oncol. 2007, 14, 2616–2620. [Google Scholar] [CrossRef]
- Kiliç, N.; Taslipinar, M.Y.; Guney, Y.; Tekin, E.; Onuk, E. An Investigation into the Serum Thioredoxin, Superoxide Dismutase, Malondialdehyde, and Advanced Oxidation Protein Products in Patients with Breast Cancer. Ann. Surg. Oncol. 2014, 21, 4139–4143. [Google Scholar] [CrossRef]
- Nayyar, A.S.; Khan, M.; Vijayalakshmi, K.R.; Suman, B.; Gayitri, H.C.; Anitha, M. Serum total protein, albumin and advanced oxidation protein products (AOPP)--implications in oral squamous cell carcinoma. Malays. J. Pathol. 2012, 34, 47–52. [Google Scholar]
- Piskounova, E.; Agathocleous, M.; Murphy, M.M.; Hu, Z.; Huddlestun, S.E.; Zhao, Z.; Leitch, A.M.; Johnson, T.M.; DeBerardinis, R.J.; Morrison, S.J. Oxidative stress inhibits distant metastasis by human melanoma cells. Nature 2015, 527, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Gao, P.; Zhang, H.; Dinavahi, R.; Li, F.; Xiang, Y.; Raman, V.; Bhujwalla, Z.M.; Felsher, D.W.; Cheng, L.; Pevsner, J.; et al. HIF-dependent antitumorigenic effect of antioxidants in vivo. Cancer Cell 2007, 12, 230–238. [Google Scholar] [CrossRef]
- Glasauer, A.; Chandel, N.S. Targeting antioxidants for cancer therapy. Biochem. Pharmacol. 2014, 92, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Glasauer, A.; Sena, L.A.; Diebold, L.P.; Mazar, A.P.; Chandel, N.S. Targeting SOD1 reduces experimental non–small-cell lung cancer. J. Clin. Invest. 2014, 124, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Mysliwiec, P.; Pawlak, K.; Kuklinski, A.; Kędra, B. Combined perioperative plasma endoglin and VEGF--a assessment in colorectal cancer patients. Folia Histochem. Cytobiol. 2009, 47, 231–236. [Google Scholar] [CrossRef]
- Kuklinski, A.; Kamocki, Z.; Koda, M.; Piotrowski, Z.; Sulkowski, S.; Leśniewicz, R.; Pawlak, K.; Myśliwiec, P.; Kedra, B. IGF-IR in patients with advanced colorectal cancer in correlation with certain clinico-morphological factors: Initial report. Oncol. Lett. 2011, 2, 1155–1159. [Google Scholar] [CrossRef] [PubMed]
- Lech, G.; Słotwiński, R.; Słodkowski, M.; Krasnodębski, I.W. Colorectal cancer tumour markers and biomarkers: Recent therapeutic advances. World J. Gastroenterol. 2016, 22, 1745–1755. [Google Scholar] [CrossRef] [PubMed]
- Pietrucha, B.; Heropolitańska-Pliszka, E.; Maciejczyk, M.; Car, H.; Sawicka-Powierza, J.; Motkowski, R.; Karpinska, J.; Hryniewicka, M.; Zalewska, A.; Pac, M.; et al. Comparison of Selected Parameters of Redox Homeostasis in Patients with Ataxia-Telangiectasia and Nijmegen Breakage Syndrome. Oxidative Med. Cell. Longev. 2017, 2017, 1–8. [Google Scholar] [CrossRef]
- Pallardó, F.V.; Lloret, A.; Lebel, M.; D’Ischia, M.; Cogger, V.C.; Le Couteur, D.G.; Gadaleta, M.N.; Castello, G.; Pagano, G. Mitochondrial dysfunction in some oxidative stress-related genetic diseases: Ataxia-Telangiectasia, Down Syndrome, Fanconi Anaemia and Werner Syndrome. Biogerontology 2010, 11, 401–419. [Google Scholar] [CrossRef]
- Catalán, V.; Frühbeck, G.; Gómez-Ambrosi, J. Inflammatory and Oxidative Stress Markers in Skeletal Muscle of Obese Subjects. In Obesity; Elsevier BV: Amsterdam, The Netherlands, 2018; pp. 163–189. [Google Scholar]
- Świderska, M.; Maciejczyk, M.; Zalewska, A.; Pogorzelska, J.; Flisiak, R.; Chabowski, A. Oxidative stress biomarkers in the serum and plasma of patients with non-alcoholic fatty liver disease (NAFLD). Can plasma AGE be a marker of NAFLD? Free Radic. Res. 2019, 53, 841–851. [Google Scholar] [CrossRef]
- Fortea-Sanchis, C.; Martínez-Ramos, D.; Escrig-Sos, J. The lymph node status as a prognostic factor in colon cancer: Comparative population study of classifications using the logarithm of the ratio between metastatic and nonmetastatic nodes (LODDS) versus the pN-TNM classification and ganglion ratio systems. BMC Cancer 2018, 18, 1208. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | n (%) |
|---|---|
| Age <60 >60 | 11 (22.0%) 39 (78.0%) |
| Sex male female | 31 (62.0%) 19 (38.0%) |
| Histological type adenocarcinoma mucinous adenocarcinoma | 40 (80.0%) 10 (20.0%) |
| Tumour location sigmoid colon rectum cecum ascending colon hepatic fold colon | 15 (30.0%) 15 (30.0%) 7 (14.0%) 6 (12.0%) 5 (10.0%) 2 (4.0%) |
| Tumour’s size <3cm >3cm | 15 (30.0%) 35 (70.0%) |
| pT—depth of invasion T1 T2 T3 T4 | 12 (24.0%) 14 (28.0%) 18 (36.0%) 6 (12.0%) |
| pN—lymph node metastasis N0 N1 N2 | 30 (60.0%) 12 (24.0%) 8 (16.0%) |
| pM—distant metastasis M0 M1 | 44 (88.0%) 6 (12.0%) |
| Stage at diagnosis I II III IV | 11 (22.0%) 16 (32.0%) 18 (36.0%) 5 (10.0%) |
| CEA level (ng/mL) 0–5.0 >5.0 | 36 (72.0%) 14 (28.0%) |
| Parameter | AUC | p-Value | Cut-Off | Sensitivity (%) | Specificity (%) | 95% Confidence Interval |
|---|---|---|---|---|---|---|
| Antioxidant defense | ||||||
| SOD (mU/100 mg protein) | 0.9048 | <0.0001 | >279.7 | 87.80 | 90.48 | 0.8242–0.9854 |
| CAT (nmol H2O2/min/100 mg protein) | 0.9988 | <0.0001 | <123.3 | 97.56 | 97.50 | 0.9955–1.002 |
| GPx (mU/100 mg protein) | 0.9209 | <0.0001 | <99.54 | 90.24 | 93.10 | 0.8387–1.003 |
| GR (uU/100 mg protein) | 1.000 | <0.0001 | <4.205 | 100.0 | 100.0 | 1.000–1.000 |
| UA (umol/100 mg protein) | 0.6880 | 0.002335 | >14.96 | 65.85 | 64.58 | 0.5756–0.8004 |
| GSH (ug/100 mg protein) | 0.9566 | <0.0001 | <0.2986 | 85.37 | 85.19 | 0.9124–1.001 |
| Redox status | ||||||
| TAC (nmol/100 mg protein) | 1.000 | <0.0001 | <168.5 | 100.0 | 100.0 | 1.000–1.000 |
| TOS (umol H2O2 Equiv/100 mg protein) | 1.000 | <0.0001 | >14.27 | 100.0 | 100.0 | 1.000–1.000 |
| OSI (TOS/TAC ratio) | 1.000 | <0.0001 | >15.49 | 100.0 | 100.0 | 1.000–1.000 |
| FRAP (umol/100 mg protein) | 0.9377 | <0.0001 | <49.49 | 90.24 | 89.47 | 0.8726–1.003 |
| Protein and lipid oxidative damage | ||||||
| AGE (AFU/100 mg protein) | 1.000 | <0.0001 | >322.0 | 100.0 | 100.0 | 1.000–1.000 |
| AOPP (umol/100 mg protein) | 1.000 | <0.0001 | >1.637 | 100.0 | 100.0 | 1.000–1.000 |
| MDA (mg/100 mg protein) | 0.9815 | <0.0001 | >5.669 | 92.68 | 92.00 | 0.9561–1.007 |
| Parameter | AUC | p-Value | Cut-Off | Sensitivity (%) | Specificity (%) | 95% Confidence Interval |
|---|---|---|---|---|---|---|
| Antioxidant defense | ||||||
| SOD (mU/100 mg protein) | 0.5507 | 0.6013 | >426.9 | 53.33 | 52.17 | 0.3590–0.7425 |
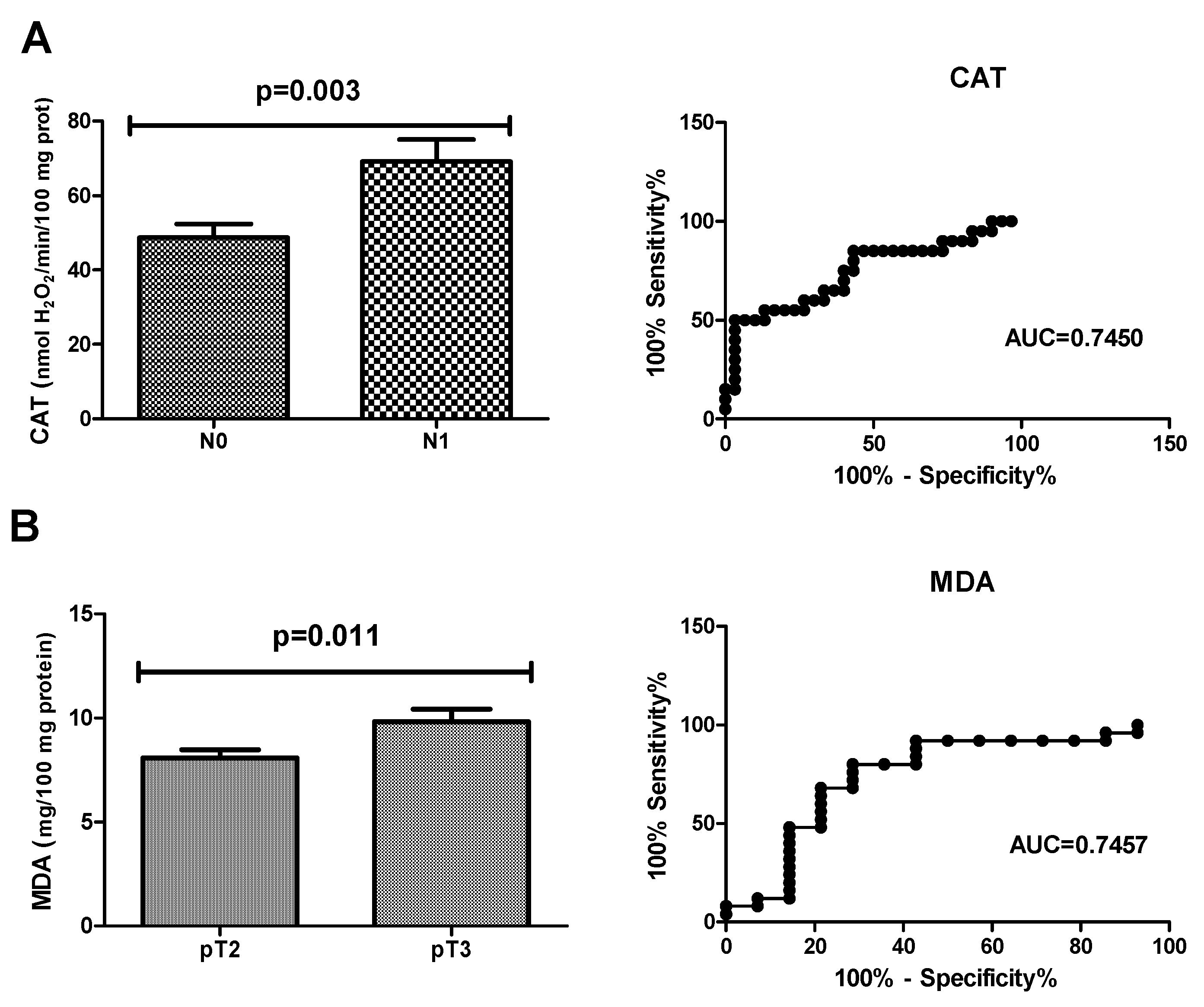
| CAT (nmol H2O2/min/100 mg protein) | 0.7450 | 0.0036 | >61.61 | 65.00 | 66.67 | 0.5989–0.8911 |
| GPx (mU/100 mg protein) | 0.6232 | 0.2044 | >79.95 | 53.33 | 56.52 | 0.4421–0.8043 |
| GR (uU/100 mg protein) | 0.6435 | 0.1394 | >0.7091 | 66.67 | 65.22 | 0.4677–0.8192 |
| UA (umol/100 mg protein) | 0.5681 | 0.4828 | >16.49 | 53.33 | 52.17 | 0.3825–0.7537 |
| GSH (ug/100 mg protein) | 0.6029 | 0.2891 | <0.1736 | 66.67 | 65.22 | 0.4185–0.7873 |
| Redox status | ||||||
| TAC (nmol/100 mg protein) | 0.5318 | 0.7544 | <70.33 | 46.15 | 47.83 | 0.3354–0.7282 |
| TOS (umol H2O2 Equiv/100 mg protein) | 0.5848 | 0.3864 | <48.65 | 53.33 | 54.55 | 0.3931–0.7766 |
| OSI (TOS/TAC ratio) | 0.5245 | 0.8111 | <85.56 | 53.85 | 54.55 | 0.3122–0.7368 |
| FRAP (umol//100 mg protein) | 0.5420 | 0.6650 | <41.71 | 60.00 | 60.87 | 0.3512–0.7329 |
| Protein and lipid oxidative damage | ||||||
| AGE (AFU/100 mg protein) | 0.6087 | 0.2628 | <873.3 | 53.33 | 52.17 | 0.4204–0.7970 |
| AOPP (umol/100 mg protein) | 0.6290 | 0.1839 | <4.388 | 66.67 | 65.22 | 0.4506–0.8074 |
| MDA (mg/100 mg protein) | 0.5188 | 0.8461 | <8.707 | 60.00 | 60.87 | 0.3293–0.7084 |
| Parameter | AUC | p-Value | Cut-Off | Sensitivity (%) | Specificity (%) | 95% Confidence Interval |
|---|---|---|---|---|---|---|
| Antioxidant defense | ||||||
| SOD (mU/100 mg protein) | 0.5500 | 0.6265 | >426.9 | 56.00 | 58.33 | 0.3361–0.7639 |
| CAT (nmol H2O2/min/100 mg protein) | 0.5633 | 0.5376 | >49.17 | 56.00 | 58.33 | 0.3758–0.7509 |
| GPx (mU/100 mg protein) | 0.5600 | 0.5592 | >79.22 | 48.00 | 50.00 | 0.3515–0.7685 |
| GR (uU/100 mg protein) | 0.6833 | 0.0744 | >0.6881 | 68.00 | 66.67 | 0.4925–0.8742 |
| UA (umol/100 mg protein) | 0.6067 | 0.2992 | >15.42 | 42.52 | 41.67 | 0.4228–0.7905 |
| GSH (ug/100 mg protein) | 0.5233 | 0.8203 | >0.1857 | 44.00 | 41.67 | 0.3302–0.7164 |
| Redox status | ||||||
| TAC (nmol/100 mg protein) | 0.5652 | 0.5316 | >70.33 | 56.52 | 58.33 | 0.3342–0.7962 |
| TOS (umol H2O2 Equiv/100 mg protein) | 0.5818 | 0.4397 | >47.87 | 56.00 | 54.55 | 0.3897–0.7739 |
| OSI (TOS/TAC ratio) | 0.5771 | 0.4729 | >85.56 | 52.17 | 54.55 | 0.3704–0.7837 |
| FRAP (umol//100 mg protein) | 0.5033 | 0.9741 | >43.19 | 40.00 | 41.67 | 0.2912–0.7154 |
| Protein and lipid oxidative damage | ||||||
| AGE (AFU/100 mg protein) | 0.5133 | 0.8967 | >873.3 | 48.00 | 50.00 | 0.3288–0.6978 |
| AOPP (umol/100 mg protein) | 0.5067 | 0.9483 | <4.475 | 52.00 | 50.00 | 0.3054–0.7079 |
| MDA (mg/100 mg protein) | 0.7457 | 0.0118 | <9.361 | 72.00 | 71.43 | 0.5678–0.9236 |
| Pair of Variables | r | p |
|---|---|---|
| GPx and GR | 0.575 | <0.0001 |
| FRAP and GSH | 0.575 | <0.0001 |
| UA and AGE | 0.407 | 0.008 |
| CAT and AOPP | −0.341 | 0.029 |
| GSH and AOPP | 0.351 | 0.024 |
| TOS and AOPP | 0.650 | <0.0001 |
| OSI and AOPP | 0.466 | 0.004 |
| UA and CA 19-9 | 0.509 | 0.026 |
| CAT and CA 19-9 | 0.642 | <0.0001 |
| GR and CA19-9 | 0.522 | 0.018 |
| GPx and CEA | −0.448 | 0.036 |
| MDA and CEA | 0.560 | 0.008 |
| UA and α1globulin | 0.547 | 0.028 |
| FRAP and location | 0.332 | 0.045 |
| MDA and pT | 0.460 | 0.008 |
| GPx and vascular invasion | 0.512 | 0.043 |
| MDA and CRP | 0.980 | <0.0001 |
| FRAP and total cholesterol | 0.670 | 0.009 |
| UA and total cholesterol | 0.565 | 0.035 |
| UA and eosinophils | −0.663 | 0.037 |
| SOD and monocytes | 0.745 | 0.013 |
| TOS and basophils | −0.735 | 0.016 |
| AGE and eosinophils | −0.717 | 0.020 |
| AGE and neutrophils | −0.636 | 0.047 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zińczuk, J.; Maciejczyk, M.; Zaręba, K.; Romaniuk, W.; Markowski, A.; Kędra, B.; Zalewska, A.; Pryczynicz, A.; Matowicka-Karna, J.; Guzińska-Ustymowicz, K. Antioxidant Barrier, Redox Status, and Oxidative Damage to Biomolecules in Patients with Colorectal Cancer. Can Malondialdehyde and Catalase Be Markers of Colorectal Cancer Advancement? Biomolecules 2019, 9, 637. https://doi.org/10.3390/biom9100637
Zińczuk J, Maciejczyk M, Zaręba K, Romaniuk W, Markowski A, Kędra B, Zalewska A, Pryczynicz A, Matowicka-Karna J, Guzińska-Ustymowicz K. Antioxidant Barrier, Redox Status, and Oxidative Damage to Biomolecules in Patients with Colorectal Cancer. Can Malondialdehyde and Catalase Be Markers of Colorectal Cancer Advancement? Biomolecules. 2019; 9(10):637. https://doi.org/10.3390/biom9100637
Chicago/Turabian StyleZińczuk, Justyna, Mateusz Maciejczyk, Konrad Zaręba, Wioletta Romaniuk, Adam Markowski, Bogusław Kędra, Anna Zalewska, Anna Pryczynicz, Joanna Matowicka-Karna, and Katarzyna Guzińska-Ustymowicz. 2019. "Antioxidant Barrier, Redox Status, and Oxidative Damage to Biomolecules in Patients with Colorectal Cancer. Can Malondialdehyde and Catalase Be Markers of Colorectal Cancer Advancement?" Biomolecules 9, no. 10: 637. https://doi.org/10.3390/biom9100637