Abstract
Background/objectives: Robotic-assisted partial nephrectomy (RAPN) is increasingly utilised for the management of renal masses, with the growing use of different robotic platforms and increasing complexity of renal masses managed robotically. Appropriate patient selection, the development of operative skills and experience and sensible surgical decision making are required to optimise the outcomes of RAPN and minimise the risk of complications. We provide a comprehensive review of strategies to predict, avoid and manage the complications of RAPN. Methods: We conducted a comprehensive literature review to outline many of the reported complications arising from RAPN, with a focus on preoperative considerations (patient selection, imaging, 3D modelling and predictive models), intraoperative considerations (positioning and kidney exposure complications) and practical management strategies to identify and manage the complications of this procedure. Results: Many complications of RAPN can be predicted, and we outline strategies to mitigate these risks through careful preparation prior to surgery, including descriptions of preventative strategies and important preoperative considerations. We also present a detailed outline of management for the most common complications of RAPN, including bleeding/haemorrhage, urine leak and intraoperative complications such as adjacent organ injuries. Conclusions: RAPN can be a challenging procedure with a significant risk of complications. Assiduous preoperative planning, thoughtful intraoperative decision making and the early recognition and management of complications are essential to optimise patient outcomes following RAPN.
1. Introduction
Minimally invasive techniques for partial nephrectomy, including utilising robotic assistance, are well established for the treatment of small renal masses [1]. Appropriate patient selection, development of operative skills and experience, and sensible surgical decision making are required to optimise outcomes of robotic-assisted partial nephrectomy and minimise the risk of complications. Early recognition and management of complications are essential to maintain a good outcome for the patient. We aim to outline a range of preoperative, intraoperative, and postoperative considerations and recommendations for management approaches to many of the complications of robotic-assisted partial nephrectomy.
2. Preoperative Considerations
Appropriate case selection for partial nephrectomy is a key component in minimising the complications of this procedure, optimising the surgical outcome, and maximising the benefits of utilising a robotic-assisted approach.
2.1. Patient Selection and Planning
In selecting a patient for minimally invasive renal surgery, patient factors, tumour factors, renal factors, and institutional factors (including the skill and experience of the operating surgeon) must all be carefully considered. A thoughtful and comprehensive evaluation through history and examination must be performed to assess suitability for robotic surgery and the patient’s ability to cope with the anaesthetic demands of the procedure, particularly in relation to the tolerability of pneumoperitoneum. Attention must be made to body habitus, underlying significant respiratory, cardiac, or hepatic disease, or anatomical issues (such as scoliosis) that may preclude safe completion of robotic renal surgery. Given the high bleeding risk associated with partial nephrectomy, careful consideration must be made to temporary cessation of anticoagulation in the perioperative period; the indication for anticoagulation is important in determining an appropriate duration for this cessation and in our centre, liaison with the relevant cardiologist or haematologist, to make a plan for the need or otherwise for a bridging regimen.
In planning surgical approach, decisions regarding partial versus radical nephrectomy, open versus laparoscopic versus robotic and transperitoneal versus retroperitoneal surgery are often based on surgeon preference, training and experience; factors including those related to the tumour (size, focality, location), patient (renal function, co-morbidity, life expectancy) and surgeon factors (experience, technology available). Many of the procedure-specific complications arising from partial nephrectomy are associated with the renorrhaphy of the kidney following tumour excision; an estimation of tumour complexity and surgeon experience is important in the preoperative selection of patients.
While the advantage of robotic over pure laparoscopic approaches to renal surgery is difficult to measure, we believe that, where available, robotic assistance is preferred. Owing to the greater speed of suturing (and faster reconstruction), the utility of the fourth robotic arm for assistance and the ability to selectively clamp smaller, segmental branches [2]—all factors which may shorten ischaemic time compared to pure laparoscopy, for many years at our centre we have now performed minimally invasive partial nephrectomy exclusively with robotic assistance.
2.1.1. Imaging
A key component in the safe performance of robotic partial nephrectomy is the availability of contemporary cross-sectional imaging, which is invaluable. Where practical, we aim to obtain imaging within one month of the date of surgery to ensure that there has not been any undue clinical progression or radiological change in the lesion. The important information to glean from the imaging (either multiphase CT or MRI) is:
- Renal vascular anatomy (number, location, branching);
- Tumour size, location (polar location, depth, relationship to hilum and collecting system), and margin/boundary (well defined, irregular, vascular invasion);
- Relationship of the kidney and the tumour to surrounding structures;
- Patient anatomical variations—spinal abnormalities, aberrant abdominal vasculature (such as superior mesenteric artery origin).
2.1.2. Three Dimensional (3D) Models
Increasingly, the use of 3D models has gained popularity in urology, particularly in the perioperative planning of partial nephrectomy [3,4]. The ability to visualise the tumour location, relationship to vasculature and collecting system, and vascular anatomy has been shown to improve perioperative outcomes [5,6]. These models are generated from cross-sectional imaging and, in many centres, are produced using artificial intelligence techniques; both physical printed models and computer-based models are commercially available, and we often use these when performing complex cases, multifocal resections, or when the vascular anatomy is unusual or dissection is predicted to be difficult. Image guided surgery for complex renal masses, utilising the integration of a virtual 3D model map generated from preoperative imaging and overlaid into the robotic surgery console for live intra-operative anatomical navigation, is soon to be evaluated in a randomised, prospective trial and promises to inform of the potential benefits to renal function, oncological outcomes and patient safety outcomes [7]. This type of innovation promises to improve precision and reduce complication rates in complex scenarios. Novel volumetric and morphological parameters derived from 3D models (such as tumour volume itself and relative to volume of the kidney, endophycity of the tumour and blood supply characteristics) have been described that can predict complication rates after RAPN and may allow a greater understanding of tumour complexity than traditional nephrometry scores derived from cross sectional imaging alone [4].
2.1.3. Nephrometry Scores
The location of the tumour and size are correlated with the risk of intra-operative and perioperative complications [8]. Nephrometry scoring systems such as RENAL and PADUA have attempted to objectively quantify these parameters [8,9,10,11]. These scoring systems permit the standardisation of reporting renal masses and take into account tumour location, size, depth of invasion, endophytic nature, and involvement of the collecting system on preoperative CT or MRI [10,11]. The use of the RENAL and PADUA scores for robotic-assisted partial nephrectomy allows for the prediction of warm ischaemic time, urine leak, and high-grade postoperative complications [8].
2.1.4. Transperitoneal Versus Retroperitoneal Approach
The choice between a transperitoneal and a retropertitoneal robotic approach is often heavily influenced by the tumour’s location in relation to Brodel’s line, previous transperitoneal abdominal surgery, and surgeon familiarity with a particular approach [12]. In our centre, we are most familiar with transperitoneal surgery, utilising retroperitoneal access in patients with previous abdominal surgery in order to avoid intra-abdominal adhesions. A retroperitoneal approach has a smaller working space than transperitoneal, but can be favourable for posteriorly located tumours as it reduces the need for kidney mobilisation to visualise and remove the tumour. It can allow for more direct access to the posterior aspect of the kidney and its hilar structures, with a lower likelihood of bowel injury or ileus compared to the transperitoneal approach. With the arrival of the Single Port robot, the retroperitoneal approach is likely to increase in popularity.
2.1.5. Prediction of Postoperative Complications
There is increasing interest in clinical decision-making tools that may assist in the prediction of complications following robotic-assisted partial nephrectomy. Using data from a large multicentric dataset in Italy (n = 2584), a nomogram consisting of age, ASA score, ECOG score, preoperative anaemia and creatinine, surgical indication (relative, absolute), cT stage, PADUA score and surgical approach (RAPN, open, laparoscopic) was developed which enabled improved decision making when the predicted risk of complications was >5% [13]. Approximately 65% of the patients in the reference cohort had undergone minimally invasive PN [13]. Similarly, other groups have demonstrated that patient-specific factors such as increased co-morbidity and presence of cardiovascular disease were more predictive of postoperative complications than nephrometry scores [14,15].
With regard to learning curves and surgical experience, early studies of the RAPN learning curve were performed during the adoption phase of RAPN and demonstrated lower warm ischaemic time and console time after 30 cases, but did not allow for any learning effect assessment [2]. More contemporary series have shown that increasing optimal outcomes rates are seen with up to 300 cases, especially in relation to complications [16,17]. Warm ischaemic times appear to plateau after 150 cases, but there is continued improvement in complication rates even after 300 cases, with the authors suggesting that there may possibly be an endless learning curve with respect to complications [17].
Emerging data have shown the potential promise of urine and serum biomarkers that may predict the incidence of postoperative complications following RAPN [18]. A few small studies have shown the potential use of biomarkers in the prediction of acute kidney injury following RAPN (serum cystatin C, urinary neutrophil gelatinase-associated lipocalin), though these have not been validated in larger clinical cohorts [18,19,20] and are not yet widely used in clinical practice.
3. Procedural Considerations
3.1. Positioning
Meticulous and diligent patient positioning for robotic-assisted partial nephrectomy can minimise the risks of rhabdomyolysis, nerve injury, and compartment syndromes as positioning-related complications occur in approximately 6% of robotic-assisted urological surgery [21]. Careful attention to the judicious use of operating table flexion is important as overflexion can increase the risk of neuromuscular injuries, without greatly improving operative exposure [22]. Padding of bony prominences in the lateral decubitus position, such as the fibular head and lateral malleolus, can reduce peripheral neuropraxia. Use of an axillary roll can reduce the risk of brachial plexus injury; the surgeon must ensure that there is not undue pressure on the upper arm. Support of the upper arm and wrist is important to avoid wrist drop. Rhabdomyolysis is a rare complication, but it can potentially be devastating in robotic renal surgery in patients with single kidneys, for example [23]. Careful attention to the hip positioning at the time of operating table flexion to ensure pressure is directed through the hip rather than the gluteal region is key; this may be more challenging in an obese patient. Correct positioning can be ensured with flexion of the operative table at the level of the patient’s umbilicus, along with alignment of the patient’s shoulders, hips, and spine [24]. A high index of suspicion is required, as signs of elevated creatine kinase and myoglobinuria may be delayed well after the onset of symptoms. Early intravenous hydration and urinary alkalisation may reduce the impact of rhabdomyolysis on renal function, and consideration of fasciotomy when compartment syndrome is suspected can be life-saving. The minimisation of operating time can reduce the incidence and impact of many of the positioning-related complications [25].
3.2. Kidney Exposure Complications
During the mobilisation and exposure of the kidney during any laparoscopic surgery, there is the potential for significant intra-operative complications causing organ loss (for example, splenic injury) or life-threatening bleeding. We describe techniques to minimise the structures at risk during this stage of the operation and their management if they unfortunately arise.
3.2.1. Vascular
For left-sided procedures, a key vascular landmark is the identification of the left gonadal vein; it most commonly drains directly into the left renal vein and thus provides a pathway to the identification of the main renal hilum. Undue tension or traction on the vein itself or its surrounding structures can cause significant bleeding, which can be ligated with clips, bipolar diathermy, or a stapler, if it is particularly large. The accompanying gonadal artery is often not visualised separately, but should it bleed, it likewise can easily be ligated with one of the above methods. During the dissection of the mid-ureter and the descending colon, the common iliac vessels are at risk and should be approached with caution. Mesenteric arteries such as the superior mesenteric and inferior mesenteric arteries are very rarely injured, but these can result from undue medial dissection owing to large upper pole and lower pole tumours, respectively. Injury to the inferior mesenteric vein can occur when the dissection veers into the colonic mesentery. An injury to the superior mesenteric artery necessitates an urgent intraoperative vascular surgery consultation owing to the lethality of delayed management and restoration of perfusion to ischaemic small bowel. This artery has more lymphatic coverings than a renal artery, arises anteriorly, and is too large for a standard locking clip, allowing improved identification. Inferior mesenteric artery and vein injury can be safely managed with ligation of the bleeding vessel. Aortic injuries are also very rare and can often occur due to arterial misidentification or during the dissection of an atherosclerotic renal artery ostium. Open conversion is often required as robotic repair of aortic injuries can be difficult with laparoscopic instruments.
For right-sided procedures, the right gonadal vein drains directly into the inferior vena cava; further cranial dissection along the vena cava will lead to the identification of the right renal artery and vein. Right gonadal vein injury can be troublesome given its direct insertion into the vena cava, and thus, dissection is best commenced laterally and inferiorly. Care must be taken not to inadvertently dissect under the gonadal and elevate it, causing damage or avulsion. The short right adrenal vein also drains directly into the inferior vena cava, and should bleeding eventuate, it can be ligated purposefully or its insertion into the vena cava repaired with a Prolene suture. We recommend the use of sharp dissection preferentially around the vessels on the right, as venous structures are more delicate and prone to injury compared to arteries. When the inferior vena cava is torn or a venotomy is performed, increased pneumoperitoneum and caudal vascular compression can facilitate the vessel repair. Should robotic repair not be feasible, then leaving the vascular control in place until open surgical instruments are readily available will minimise bleeding, as increased pneumoperitoneum may help to control other venous bleeding sources. A consistent and stable orientation of the camera, with the psoas muscle maintained horizontally, can ensure that correct vascular identification is performed.
3.2.2. Bowel
Descending colon mobilisation is required on the left side to access the kidney; often, a more limited colonic mobilisation of the hepatic flexure is required to access the right kidney. Colonic injuries during dissection or abdominal access are uncommon, estimated to occur in approximately 1.5% of cases [26]. Although there is conflicting evidence regarding the preferred method for establishment of pneumoperitoneum, in our centre we favour an open Hasson technique (over Veress needle) as it allows the early identification and management of a bowel injury should it occur during the initial access [27]. Careful placement of the trocars under direct vision and careful passage of instruments will also reduce the risk of bowel injuries. Techniques to reduce the risk of a thermal injury include the use of an athermal dissection, incision of the peritoneum along the white line of Toldt lateral to the bowel, and using blunt dissection to mobilise the bowel, without undue traction. Thermal injuries to the colon can initially be underestimated at the time of injury, their extent becoming more apparent during the ensuing dissection. Injury to both the small and large bowel is possible during more medial dissection and the duodenum should be handled with care during medial dissection of the right kidney. Small serosal injuries can be managed with a continuous absorbable monofilament suture (our preference is polydioxanone). Full thickness injuries to the bowel can be managed with primary closure, but we would recommend intra-operative consultation with a general surgeon should this arise [28]; resection and re-anastomosis of the affected segment can also be performed with either a hand-sewn or stapled anastomosis [29].
3.2.3. Spleen
Injuries to the spleen during left-sided nephrectomy are uncommon, with an estimated incidence of 1% [26]. Minor injuries caused by thermal energy or small lacerations can be managed with gentle direct pressure or haemostatic agents (our preference is to use human gelatine-thrombin matrix for this indication, if available) [30]. Splenic injuries can be notoriously difficult to manage, and where bleeding is sustained despite these manoeuvres, or if the injury is larger, a splenectomy may be necessary. Seemingly small splenic injuries noted intra-operatively can have a delayed presentation with shock [31]. A contrast-enhanced CT scan may demonstrate a spectrum of injuries ranging from a small haematoma to free intraperitoneal haemorrhage. Supportive measures with close haemodynamic monitoring, bed rest, and blood transfusion to treat symptomatic anaemia may be all that is required [31]. In more extreme cases or where there is evidence of fluid unresponsive haemodynamic instability, angioembolisation or splenectomy may be necessary. Consideration of appropriate vaccination and prophylactic antibiotics should be made for asplenic patients.
3.2.4. Pleura
Pleural injuries most commonly occur at the extremes of mobilisation: of the spleen on the left and the liver on the right. Small injuries can be repaired with sutures, and we advocate for cinching the suture during a Valsalva manoeuvre [32]. If the injury is large or unable to be repaired with sutures, placement of a chest tube at the conclusion of the case is recommended [32].
3.2.5. Pancreas
The tail of the pancreas is at risk during dissection to visualise the left renal hilum, and care should be taken to handle the pancreas minimally by using gentle retraction and minimsation of thermal energy. Small injuries are often managed with drainage and can be removed if output does not increase once a normal diet is introduced [33]. Larger injuries or those with suspected pancreatic duct injury should invite consultation with a hepatobiliary surgeon, as, rarely, a distal pancreatectomy may be required [33]. Late identification of a pancreatic injury often manifests with abdominal pain, nausea, vomiting, fever, and elevated amylase and lipase [33]. Minor injuries can be managed with a combination of gut rest, total parenteral nutrition (TPN), and drainage of peripancreatic fluid collections. Liaison with a hepatobiliary surgeon to assist with management is prudent, as these injuries can require a prolonged and slow, but eventual, recovery.
3.2.6. Liver
The liver is at risk of thermal injury, traction injury, and direct laceration during right kidney mobilisation. Minor injuries typically do not require any specific intra-operative management, but larger injuries involving capsular tears or parenchymal incisions may require placement of haemostatic agents with direct pressure or the use of argon plasma coagulation [31]. Gallbladder injury may occur during adhesiolysis, and consultation with a general surgeon may be required, though cholecystectomy can usually be completed without overt difficulty [34].
3.2.7. Lymphatic
The formation of lymphatic collections following the mobilisation required for a partial nephrectomy is rare. Disruption to lymphatics during the mobilisaton of the left renal hilar vascular structures is the cause, and is more often seen when a concomitant para-aortic lymphadenectomy is performed [35]. In severe cases with the formation of chylous ascites, conservative management with percutaneous drainage, TPN, medium-chain triglyceride diets, and somatostatin may be required [36]. Surgical ligation or radiological embolisation of the source of the leak is rarely required, and biologic adhesives have been used successfully in this setting [36]. Table 1 summarises estimated rates of intra-operative complications from a large (n = 545), single-centre comparative series in the USA of T1a renal masses treated by robotic-assisted partial nephrectomy [37].

Table 1.
Estimated rates of intra-operative injuries during RAPN in a series of 575 cases (Ramirez et al.) [37].
4. Specific Complications to Robotic-Assisted Partial Nephrectomy
4.1. Bleeding
Bleeding, either intraoperative or postoperative, is the most common complication specific to partial nephrectomy. Careful evaluation of the preoperative imaging to assess tumour size, depth of invasion, and relationship to vascular structures is important in planning the excision technique for the tumour. We have generally used renal ischaemia for all but the smallest and most exophytic tumours, appreciating the consistency of technique and valuing a bloodless field for tumour excision to ensure we obtain negative tumour margins. This approach has also allowed us to assess for the presence of additional arterial supply not previously identified, especially relevant if we encounter pulsatile arterial bleeding early on during tumour excision. Off-clamp techniques for tumour excision, which minimise renal ischaemia, may be beneficial in selected cases, but may come at the cost of a more challenging tumour excision. Intra-operative bleeding is usually from the incised excision bed of renal parenchyma at the time of tumour excision, but can also be from hilar vessels if not carefully dissected during the initial exposure. If there is brisk bleeding on initial tumour dissection, we make an assessment about our vision and ability to complete an excision with negative margin; should we be unable to carry on, we make a swift decision to explore for any missed arterial supply. Failing that, an additional port can be placed and a laparoscopic renal pedicle clamp can be applied to allow the dissection to proceed (care must be taken to avoid inadvertent clamping of the superior mesenteric artery or the aorta with this manoeuvre). It would be rare to subsequently require conversion to a radical nephrectomy for bleeding at this point. When incising deep into the renal sinus and large veins are encountered, we increase the pneumoperitoneum initially and then consider a renal vein clamp to control retrograde haemorrhage.
After tumour excision, our process for renal reconstruction is to close any large collecting system defects, suture any larger central vessels (where possible and feasible), and parenchymal compression (which often also controls bleeding from smaller, cortical vessels). Most commonly, we perform a continuous, ‘deep layer’ suture that incorporates the collecting system and larger central vessels with wide but shallow passes of the needle through the cortico-medullary tissue junction perpendicular to the long axis of the parenchymal defect. We utilise a 3-0 Monocryl suture knotted at one end with a Hem-o-lok clip (Teleflex, Wayne, PA, USA) placed below it and commence it by passage through the renal capsule at one end of the defect and complete it by exiting the defect at the opposite end and locking the suture with another Hem-o-lok clip (see Figure 1a,b). This allows tension to be applied to the suture to increase compression before the ends of the suture are ‘double’ locked with an additional Hem-o-lok clip at each end. Small parenchymal vessels that continue to bleed after the placement of the deep-layer suture can be controlled with diathermy. Often, we advocate for early arterial unclamping at this point to assess for any further bleeding that we control with individual suture ligation. Our renorrhaphy is performed with an interrupted, sliding clip technique with 0 Vicryl, with each end of the suture secured with Hem-o-lok clips, sequentially tightened (see Figure 1c,d). We also utilise Veraseal (Johnson and Johnson, New Brunswick, NJ, USA) fibrin sealant into the defect once the reconstruction has been completed. In our institutional series of over 1200 cases utilising this renorrhaphy technique, we have a urine leak rate < 1% and an angioembolisation rate of 1% for control of pseudoaneurysm/arterio-venous fistula.
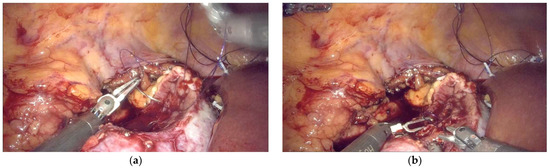
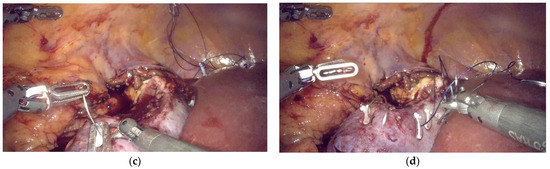
Figure 1.
(a) Commencement of the ‘deep layer’ renorrhaphy suture from ‘outside’ the defect to ‘inside’ the defect, incorporating renal capsule at least 1 cm from the edge of the defect to prevent ‘cheese wiring’ when tightened; (b) Shallow, but wide passes of the ‘deep layer’ suture are made perpendicular to the long axis of the defect through the corticomedullary junction on each side of the defect; (c) Completion of the ‘deep layer’ suture with passage of the suture from ‘inside’ the defect to ‘outside’ the defect and locking of the suture with Hem-o-lok clip with incorporation of the renal capsule at least 1 cm from the edge of the defect to prevent ‘cheese wiring’ when tightened; (d) Interrupted sliding clip renorrhaphy technique with 0 Vicryl sutures placed serially perpendicular across the defect at least 5 mm from the edge of the defect to prevent ‘cheese wiring’ when tightened, serial tension is applied to the sutures in the direction of suture passage with double locking with Hem-o-lok clips.
Recent work has attempted to assess the outcomes of alternative renorrhaphy techniques, given the importance of maintaining renal function following nephron-sparing surgery and minimising postoperative complications. Systematic reviews assessing the impact of a single-layer and double-layer technique have shown that utilisation of a single-layer technique results in a more favourable GFR outcome than a double-layer technique, but may come at the expense of a higher rate (though not significantly) of postoperative complications, particularly urine leak [38,39]. This may be in part explained by the shorter operative time needed to complete a single-layered closure [38,39]. Proponents of the double-layered technique point to evidence showing no differences in renal function outcomes when compared to a single-layer closure, but lower rates of postoperative complications (though not significantly different) [40,41]. Comparisons of running and interrupted renorrhaphy suturing techniques have indicated shorter operative times with a continuous closure, but no significant difference in postoperative renal function [38]. For these reasons, we advocate for the utilisation of a double-layered closure technique.
For early postoperative bleeding, we recommend initial management with blood transfusion, bed rest, and close haemodynamic monitoring. If there is an ongoing transfusion requirement or evidence of haemodynamic instability, we recommend early CT imaging with consideration of selective arterial embolisation.
In cases of delayed postoperative bleeding (often manifested as profuse haematuria, flank pain, and hypovolaemic shock), typically in the first 7–14 days (but can be as late as 60 days), the commonest causes are renal pseudoaneurysm rupture or arterio-venous fistula (AVF). A low threshold for CT angiographic imaging and a high index of suspicion for these complications should allow for expeditious identification and treatment with selective angioembolisation [42]. This occurs in 1% of cases in our institutional series of over 1200 cases. It is rare to need to re-explore the kidney for bleeding, and attempts to salvage the kidney following failed angioembolisation are often difficult; radical nephrectomy in this instance may be the necessary management.
4.2. Urine Leak
Urine leak after robotic-assisted partial nephrectomy is estimated to occur in 1% of cases [43]. Given that the majority of robotic partial nephrectomies are performed with a transperitoneal approach, the risk of urinary ascites with resulting ileus is higher than with a retroperitoneal approach. As discussed in the nephrometry score section, the risk factors for urine leak include high complexity lesions with large tumour size, hilar location, prolonged operative time, prolonged warm ischaemic time, and the necessity for collecting system repair [43]. Our practice is to leave a drain near the tumour resection bed when the collecting system has been entered, and we routinely leave a urethral catheter in post-operatively for all cases. If there is minimal drain output on the first postoperative day, the urethral catheter is removed, followed by the drain if there is no increased output once the urethral catheter is removed. We check a drain fluid creatinine level only if there is high output, but not routinely. The majority of urine leaks occur early in the postoperative period with high drain output, which can be confirmed with drain fluid creatinine. Should a urine leak be detected in this fashion, we advocate for performing a CT with a delayed phase protocol to assess for the presence of an undrained urinoma, hydronephrosis, and ensure there is no ureteric injury. In the absence of any of these complicating factors, the patient can be discharged home with a urethral catheter and drain until resolution of the leak, which can take several weeks. As the drain output reduces, the drain can be shortened and gradually withdrawn to allow for the tract to scar and close the leak. Unless there is evidence of obstruction in the operated kidney, we generally avoid ureteric stents or nephrostomy insertion. High volume leaks of > 500 mL output per day may suggest an anatomical abnormality or result from tissue infarction; in this instance, we would consider the placement of a ureteric stent or nephrostomy. Symptomatic, large or persistent urinomas, particularly those around the anastomosis or proximal ureter, can be percutaneously drained; most often, though, delayed urinomas can be managed conservatively. The delayed presentation of a urine leak can be caused by a renal infundibular injury, whereby the urine leak originates from an isolated calyx due to infundibular stenosis. This is a rare presentation and can be difficult to manage with options described, including balloon dilation of the affected infundibulum, percutaneous or retrograde endoscopic treatment of the stenosis (laser ablation of suture material), or as a last resort, selective renal arterial embolisation of the isolated calyx [44]. Hem-o-lok clips used during renorrhaphy can rarely migrate into the collecting system and act as a nidus for stone formation or propagate a urine leak. Endoscopic treatment of the stone/removal of the clip can manage this complication, with short-term insertion of a ureteric stent recommended after treatment to facilitate low-pressure urine drainage to allow any residual collecting system injury to resolve [45]. Table 2 presents the incidence rates of procedure-specific complications from selected comparative series and demonstrates the variability, but overall low rates, of complications of RAPN.
Table 2.
Comparison of procedure-specific complications in selected series.
4.3. Positive Surgical Margin
Obtaining a negative surgical margin remains essential in the management of renal masses with renal-sparing surgical approaches. Many studies have demonstrated that the thickness of the margin does not appear to influence the likelihood of recurrence-free survival, but the presence of a negative margin is paramount [54,55]. We routinely use intra-operative ultrasound to plan our margin at the initial renal parenchymal incision and utilise arterial ischaemia to allow optimal visualisation during tumour resection to ensure we reduce the risk of incision into the tumour or dissection that risks obtaining a positive margin. Exophytic tumours allow for parenchymal scoring with the monopolar diathermy to plan the initial renal incision, and the aim is to perform an enuceloresection removing the tumour with a small rim of normal tissue covering it. For endophytic tumours, the options are a true ‘resection’ where the tumour edge is not seen or dissecting onto the tumour capsule and then performing a true enucleation technique. The use of intra-operative ultrasound for these tumours is essential to clearly locate the mass and ensure a negative margin is obtained. If there is an incision into the tumour, or dissection is too close to it, a deeper repeat incision starting wider and more proximal to the previous leading edge can correct this. Knowledge of the preoperative location of the tumour in relation to adjacent structures, such as the renal sinus or collecting system, can be confirmed if these structures are then subsequently entered during the dissection, ensuring the sufficiency of the margin.
4.4. Renal Function
Prolonged renal ischaemia can result in postoperative acute tubular necrosis and acute failure of the kidney; this can be especially challenging where there is an absolute indication for partial nephrectomy (single kidney, existing poor renal function) [56]. Deeper tumours often necessitate greater care with reconstruction, and thus operative time, so we would advocate for the performance of smaller, exophytic tumours early in the learning curve of RAPN to ensure facility with the operative technique. Most partial nephrectomies should reasonably be completed with clamp times <25 min, although there have been reports of warm ischaemic times <60 min still being safe [56,57]. Apart from the warm ischaemic time during partial nephrectomy, the quality and quantity of the kidney remaining after resection and preoperative renal function are key factors associated with postoperative renal function recovery [56]. Techniques we utilise if prolonged ischaemic time is anticipated include using selective/segmental arterial clamping [58,59], rather than main renal artery clamping, to induce ischaemia only to the renal segment in which the tumour is located, rather than causing total renal ischaemia. We frequently use early arterial unclamping [59] and occasionally off-clamp partial nephrectomy [59,60], which are both techniques to reduce the ischaemic time of the renal tissue. Intra-corporeal cooling techniques have been described for RAPN, though we have used these rarely, as most tumour resections can be completed without this, even if highly complex [61]. In less experienced centres, if contemplating the use of intra-corporeal cooling, strong consideration should be made to performing the procedure with an open technique. In the postoperative period, we aim to avoid hypotension, nephrotoxic medications, and ensure adequate hydration; in rare instances, temporary dialysis is required, and this can be managed in conjunction with nephrology.
5. Conclusions
Robotic-assisted partial nephrectomy can be a challenging procedure with a significant risk of complications. Thorough preoperative planning, careful intraoperative decision making, and early identification and appropriate response to complications will ensure an optimal outcome for the patient after this procedure.
Author Contributions
Conceptualization, A.R.H.S. and B.J.C.; methodology, A.R.H.S. and B.J.C.; data curation, A.R.H.S.; writing—original draft preparation, A.R.H.S.; writing—review and editing, A.R.H.S. and B.J.C.; supervision, B.J.C. All authors have read and agreed to the published version of the manuscript.
Funding
A.R.H.S. was supported by the Pickard Robotic Training Grant from the Royal Australasian College of Surgeons and the Foundation for Surgery.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created during the preparation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest of the study.
References
- Choi, J.E.; You, J.H.; Kim, D.K.; Rha, K.H.; Lee, S.H. Comparison of perioperative outcomes between robotic and laparoscopic partial nephrectomy: A systematic review and meta-analysis. Eur. Urol. 2015, 67, 891–901. [Google Scholar] [CrossRef]
- Mottrie, A.; De Naeyer, G.; Schatteman, P.; Carpentier, P.; Sangalli, M.; Ficarra, V. Impact of the Learning Curve on Perioperative Outcomes in Patients Who Underwent Robotic Partial Nephrectomy for Parenchymal Renal Tumours. Eur. Urol. 2010, 58, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Schiavina, R.; Bianchi, L.; Borghesi, M.; Chessa, F.; Cercenelli, L.; Marcelli, E.; Brunocilla, E. Three-dimensional digital reconstruction of renal model to guide preoperative planning of robot-assisted partial nephrectomy. Int. J. Urol. 2019, 26, 931–932. [Google Scholar] [CrossRef]
- Bianchi, L.; Schiavina, R.; Bortolani, B.; Cercenelli, L.; Gaudiano, C.; Mottaran, A.; Droghetti, M.; Chessa, F.; Boschi, S.; Molinaroli, E.; et al. Novel Volumetric and Morphological Parameters Derived from Three-dimensional Virtual Modeling to Improve Comprehension of Tumor’s Anatomy in Patients with Renal Cancer. Eur. Urol. Focus 2022, 8, 1300–1308. [Google Scholar] [CrossRef] [PubMed]
- Shirk, J.D.; Thiel, D.D.; Wallen, E.M.; Linehan, J.M.; White, W.M.; Badani, K.K.; Porter, J.R. Effect of 3-Dimensional Virtual Reality Models for Surgical Planning of Robotic-Assisted Partial Nephrectomy on Surgical Outcomes: A Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e1911598. [Google Scholar] [CrossRef] [PubMed]
- Michiels, C.; Khene, Z.E.; Prudhomme, T.; Boulenger de Hauteclocque, A.; Cornelis, F.H.; Percot, M.; Simeon, H.; Dupitout, L.; Bensadoun, H.; Capon, G.; et al. 3D-Image guided robotic-assisted partial nephrectomy: A multi-institutional propensity score-matched analysis (UroCCR study 51). World J. Urol. 2023, 41, 303–313. [Google Scholar] [CrossRef]
- Margue, G.; Bernhard, J.-C.; Giai, J.; Bouzit, A.; Ricard, S.; Jaffredo, M.; Guillaume, B.; Jambon, E.; Fiard, G.; Bigot, P.; et al. Clinical Trial Protocol for ACCURATE: A CCafU-UroCCR Randomized Trial: Three-dimensional Image-guided Robot-assisted Partial Nephrectomy for Renal Complex Tumor (UroCCR 99). Eur. Urol. Oncol. 2025, in press. [Google Scholar] [CrossRef]
- Schiavina, R.; Novara, G.; Borghesi, M.; Ficarra, V.; Ahlawat, R.; Moon, D.A.; Porpiglia, F.; Challacombe, B.J.; Dasgupta, P.; Brunocilla, E.; et al. PADUA and R.E.N.A.L. nephrometry scores correlate with perioperative outcomes of robot-assisted partial nephrectomy: Analysis of the Vattikuti Global Quality Initiative in Robotic Urologic Surgery (GQI-RUS) database. BJU Int. 2017, 119, 456–463. [Google Scholar] [CrossRef]
- Hew, M.N.; Baseskioglu, B.; Barwari, K.; Axwijk, P.H.; Can, C.; Horenblas, S.; Bex, A.; Rosette, J.J.; Pes, M.P. Critical appraisal of the PADUA classification and assessment of the R.E.N.A.L. nephrometry score in patients undergoing partial nephrectomy. J. Urol. 2011, 186, 42–46. [Google Scholar] [CrossRef]
- Kutikov, A.; Uzzo, R.G. The R.E.N.A.L. nephrometry score: A comprehensive standardized system for quantitating renal tumor size, location and depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef]
- Ficarra, V.; Novara, G.; Secco, S.; Macchi, V.; Porzionato, A.; De Caro, R.; Artibani, W. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery. Eur. Urol. 2009, 56, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Hughes-Hallett, A.; Patki, P.; Patel, N.; Barber, N.J.; Sullivan, M.; Thilagarajah, R. Robot-assisted partial nephrectomy: A comparison of the transperitoneal and retroperitoneal approaches. J. Endourol. 2013, 27, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Mari, A.; Campi, R.; Schiavina, R.; Amparore, D.; Antonelli, A.; Artibani, W.; Barale, M.; Bertini, R.; Borghesi, M.; Bove, P.; et al. Nomogram for predicting the likelihood of postoperative surgical complications in patients treated with partial nephrectomy: A prospective multicentre observational study (the RECORd 2 project). BJU Int. 2019, 124, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Khene, Z.E.; Peyronnet, B.; Kocher, N.J.; Robyak, H.; Robert, C.; Pradere, B.; Oger, E.; Kammerer-Jacquet, S.-F.; Verhoest, G.; Rioux-Leclercq, N.; et al. Predicting morbidity after robotic partial nephrectomy: The effect of tumor, environment, and patient-related factors. Urol. Oncol. Semin. Orig. Investig. 2018, 36, e319–e338. [Google Scholar] [CrossRef]
- Bauman, T.M.; Potretzke, A.M.; Vetter, J.M.; Bhayani, S.B.; Figenshau, R.S. Cerebrovascular Disease and Chronic Obstructive Pulmonary Disease Increase Risk of Complications with Robotic Partial Nephrectomy. J. Endourol. 2015, 30, 293–299. [Google Scholar] [CrossRef]
- Paulucci, D.J.; Abaza, R.; Eun, D.D.; Hemal, A.K.; Badani, K.K. Robot-assisted partial nephrectomy: Continued refinement of outcomes beyond the initial learning curve. BJU Int. 2017, 119, 748–754. [Google Scholar] [CrossRef]
- Larcher, A.; Muttin, F.; Peyronnet, B.; De Naeyer, G.; Khene, Z.-E.; Dell’Oglio, P.; Ferreiro, C.; Schatteman, P.; Capitanio, U.; D’Hondt, F.; et al. The Learning Curve for Robot-assisted Partial Nephrectomy: Impact of Surgical Experience on Perioperative Outcomes. Eur. Urol. 2019, 75, 253–256. [Google Scholar] [CrossRef]
- Antonelli, A.; Allinovi, M.; Cocci, A.; Russo, G.I.; Schiavina, R.; Rocco, B.; Giovannalberto, P.; Celia, A.; Galfano, A.; Varca, V.; et al. The Predictive Role of Biomarkers for the Detection of Acute Kidney Injury After Partial or Radical Nephrectomy: A Systematic Review of the Literature. Eur. Urol. Focus 2020, 6, 344–353. [Google Scholar] [CrossRef]
- Lane, B.R.; Babitz, S.K.; Vlasakova, K.; Wong, A.; Noyes, S.L.; Boshoven, W.; Grady, P.; Zimmerman, C.; Engerman, S.; Gebben, M.; et al. Evaluation of Urinary Renal Biomarkers for Early Prediction of Acute Kidney Injury Following Partial Nephrectomy: A Feasibility Study. Eur. Urol. Focus 2020, 6, 1240–1247. [Google Scholar] [CrossRef]
- Chen, J.; Lin, J.; Lin, C. Serum and urinary biomarkers for predicting acute kidney injury after partial nephrectomy. Clin. Investig. Med. 2015, 38, E82–E89. [Google Scholar] [CrossRef]
- Mills, J.T.; Burris, M.B.; Warburton, D.J.; Conaway, M.R.; Schenkman, N.S.; Krupski, T.L. Positioning injuries associated with robotic assisted urological surgery. J. Urol. 2013, 190, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Deane, L.A.; Lee, H.J.; Box, G.N.; Abraham, J.B.; Abdelshehid, C.S.; Elchico, E.R.; Alipanah, R.; Borin, J.F.; Johnson, R.W.; Jackson, D.J.; et al. Third place: Flank position is associated with higher skin-to-surface interface pressures in men versus women: Implications for laparoscopic renal surgery and the risk of rhabdomyolysis. J. Endourol. 2008, 22, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Pariser, J.J.; Pearce, S.M.; Patel, S.G.; Anderson, B.B.; Packiam, V.T.; Shalhav, A.L.; Bales, G.T.; Smith, N.D. Rhabdomyolysis After Major Urologic Surgery: Epidemiology, Risk Factors, and Outcomes. Urology 2015, 85, 1328–1332. [Google Scholar] [CrossRef] [PubMed]
- Saada, L.; Sapre, N.; Challacombe, B.J. Patient Positioning for Renal Surgery. In Robotic Urologic Surgery; Wiklund, P., Mottrie, A., Gundeti, M.S., Patel, V., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 441–446. [Google Scholar]
- Reisiger, K.E.; Landman, J.; Kibel, A.; Clayman, R.V. Laparoscopic renal surgery and the risk of rhabdomyolysis: Diagnosis and treatment. Urology 2005, 66, 29–35. [Google Scholar] [CrossRef]
- Pareek, G.; Hedican, S.P.; Gee, J.R.; Bruskewitz, R.C.; Nakada, S.Y. Meta-analysis of the complications of laparoscopic renal surgery: Comparison of procedures and techniques. J. Urol. 2006, 175, 1208–1213. [Google Scholar] [CrossRef]
- Dunne, N.; Booth, M.I.; Dehn, T.C. Establishing pneumoperitoneum: Verres or Hasson? The debate continues. Ann. R. Coll. Surg. Engl. 2011, 93, 22–24. [Google Scholar] [CrossRef]
- Meraney, A.M.; Samee, A.A.; Gill, I.S. Vascular and bowel complications during retroperitoneal laparoscopic surgery. J. Urol. 2002, 168, 1941–1944. [Google Scholar] [CrossRef]
- van der Voort, M.; Heijnsdijk, E.A.; Gouma, D.J. Bowel injury as a complication of laparoscopy. Br. J. Surg. 2004, 91, 1253–1258. [Google Scholar] [CrossRef]
- Canby-Hagino, E.D.; Morey, A.F.; Jatoi, I.; Perahia, B.; Bishoff, J.T. Fibrin sealant treatment of splenic injury during open and laparoscopic left radical nephrectomy. J. Urol. 2000, 164, 2004–2005. [Google Scholar] [CrossRef]
- Rosevear, H.M.; Montgomery, J.S.; Roberts, W.W.; Wolf, J.S., Jr. Characterization and management of postoperative hemorrhage following upper retroperitoneal laparoscopic surgery. J. Urol. 2006, 176, 1458–1462. [Google Scholar] [CrossRef]
- Del Pizzo, J.J.; Jacobs, S.C.; Bishoff, J.T.; Kavoussi, L.R.; Jarrett, T.W. Pleural injury during laparoscopic renal surgery: Early recognition and management. J. Urol. 2003, 169, 41–44. [Google Scholar] [CrossRef]
- Varkarakis, I.M.; Allaf, M.E.; Bhayani, S.B.; Inagaki, T.; Su, L.M.; Kavoussi, L.R.; Jarrett, T.W. Pancreatic injuries during laparoscopic urologic surgery. Urology 2004, 64, 1089–1093. [Google Scholar] [CrossRef]
- Sawaya, D.E., Jr.; Johnson, L.W.; Sittig, K.; McDonald, J.C.; Zibari, G.B. Iatrogenic and noniatrogenic extrahepatic biliary tract injuries: A multi-institutional review. Am. Surg. 2001, 67, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Shafizadeh, S.F.; Daily, P.P.; Baliga, P.; Rogers, J.; Baillie, G.M.; Rajagopolan, P.R.; Chavin, K.D. Chylous ascites secondary to laparoscopic donor nephrectomy. Urology 2002, 60, 345. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Yoo, E.S.; Kim, T.H.; Kwon, T.G. Chylous ascites as a complication of laparoscopic nephrectomy. J. Urol. 2010, 184, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, D.; Maurice, M.J.; Caputo, P.A.; Nelson, R.J.; Kara, Ö.; Malkoç, E.; Kaouk, J.H. Predicting complications in partial nephrectomy for T1a tumours: Does approach matter? BJU Int. 2016, 118, 940–945. [Google Scholar] [CrossRef]
- Bertolo, R.; Campi, R.; Mir, M.C.; Klatte, T.; Kriegmair, M.C.; Salagierski, M.; Ouzaid, I.; Capitanio, U. Systematic Review and Pooled Analysis of the Impact of Renorrhaphy Techniques on Renal Functional Outcome After Partial Nephrectomy. Eur. Urol. Oncol. 2019, 2, 572–575. [Google Scholar] [CrossRef]
- Bertolo, R.; Campi, R.; Klatte, T.; Kriegmair, M.C.; Mir, M.C.; Ouzaid, I.; Salagierski, M.; Bhayani, S.; Gill, I.; Kaouk, J.; et al. Suture techniques during laparoscopic and robot-assisted partial nephrectomy: A systematic review and quantitative synthesis of peri-operative outcomes. BJU Int. 2019, 123, 923–946. [Google Scholar] [CrossRef]
- Bertolo, R.; Ditonno, F.; Veccia, A.; De Marco, V.; Migliorini, F.; Porcaro, A.B.; Rizzetto, R.; Cerruto, M.A.; Autorino, R.; Antonelli, A. Single-layer versus double-layer renorrhaphy technique during robot-assisted partial nephrectomy: Impact on perioperative outcomes, complications, and functional outcomes. Minerva Urol. Nephrol. 2024, 76, 176–184. [Google Scholar] [CrossRef]
- Arora, S.; Bronkema, C.; Porter, J.R.; Mottrie, A.; Dasgupta, P.; Challacombe, B.; Rha, K.H.; Ahlawat, R.K.; Capitanio, U.; Yuvaraja, T.B.; et al. Omission of Cortical Renorrhaphy During Robotic Partial Nephrectomy: A Vattikuti Collective Quality Initiative Database Analysis. Urology 2020, 146, 125–132. [Google Scholar] [CrossRef]
- Moore, C.J.; Rozen, S.M.; Fishman, E.K. Two cases of pseudoaneurysm of the renal artery following laparoscopic partial nephrectomy for renal cell carcinoma: CT angiographic evaluation. Emerg. Radiol. 2004, 10, 193–196. [Google Scholar] [CrossRef]
- Potretzke, A.M.; Knight, B.A.; Zargar, H.; Kaouk, J.H.; Barod, R.; Rogers, C.G.; Mass, A.; Stifelman, M.D.; Johnson, M.H.; Allaf, M.E.; et al. Urinary fistula after robot-assisted partial nephrectomy: A multicentre analysis of 1 791 patients. BJU Int. 2016, 117, 131–137. [Google Scholar] [CrossRef]
- Inoue, R.; Isoyama, N.; Ozawa, S.; Kobayashi, K.; Yamamoto, Y.; Yano, S.; Hirata, H.; Matsumoto, H.; Matsuyama, H. Endoscopic laser treatment for urine leakage caused by an isolated calyx after robot-assisted partial nephrectomy. IJU Case Rep. 2021, 4, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Dibitetto, F.; Russo, P.; Marino, F.; Ragonese, M.; Nigro, D.; Foschi, N. Staghorn Caliceal Hem-o-lok Stone: A Long-Term Complication of Robotic Partial Nephrectomy—A Case Report and Literature Review. Urol. Int. 2024, 108, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Bic, A.; Mazeaud, C.; Salleron, J.; Bannay, A.; Balkau, B.; Larose, C.; Hubert, J.; Eschwège, P. Complications after partial nephrectomy: Robotics overcomes open surgery and laparoscopy: The PMSI French national database. BMC Urol. 2023, 23, 146. [Google Scholar] [CrossRef] [PubMed]
- Bravi, C.A.; Larcher, A.; Capitanio, U.; Mari, A.; Antonelli, A.; Artibani, W.; Barale, M.; Bertini, R.; Bove, P.; Brunocilla, E.; et al. Perioperative Outcomes of Open, Laparoscopic, and Robotic Partial Nephrectomy: A Prospective Multicenter Observational Study (The RECORd 2 Project). Eur. Urol. Focus 2021, 7, 390–396. [Google Scholar] [CrossRef]
- Peyronnet, B.; Seisen, T.; Oger, E.; Vaessen, C.; Grassano, Y.; Benoit, T.; Carrouget, J.; Pradère, B.; Khene, Z.; Giwerc, A.; et al. Comparison of 1800 Robotic and Open Partial Nephrectomies for Renal Tumors. Ann. Surg. Oncol. 2016, 23, 4277–4283. [Google Scholar] [CrossRef]
- Tan, J.-L.; Frydenberg, M.; Grummet, J.; Hanegbi, U.; Snow, R.; Mann, S.; Begashaw, K.; Moon, D. Comparison of perioperative, renal and oncologic outcomes in robotic-assisted versus open partial nephrectomy. ANZ J. Surg. 2018, 88, E194–E199. [Google Scholar] [CrossRef]
- Grimm, M.O.; Bedke, J.; Nyarangi-Dix, J.; Khoder, W.; Foller, S.; Sommerfeld, H.J.; Giessing, M.; Heck, M.; Meißner, W.; Slee, A.; et al. Open versus robotic-assisted partial nephrectomy in patients with intermediate/high-complexity kidney tumours: Final results of the randomised, controlled, open-label, multicentre trial OpeRa. Ann. Oncol. 2025, 36, 988–998. [Google Scholar] [CrossRef]
- Wang, Y.; Shao, J.; Ma, X.; Du, Q.; Gong, H.; Zhang, X. Robotic and open partial nephrectomy for complex renal tumors: A matched-pair comparison with a long-term follow-up. World J. Urol. 2017, 35, 73–80. [Google Scholar] [CrossRef]
- Furukawa, J.; Kanayama, H.; Azuma, H.; Inoue, K.; Kobayashi, Y.; Kashiwagi, A.; Segawa, T.; Takahashi, Y.; Horie, S.; Ogawa, O.; et al. ‘Trifecta’ outcomes of robot-assisted partial nephrectomy: A large Japanese multicenter study. Int. J. Clin. Oncol. 2020, 25, 347–353. [Google Scholar] [CrossRef]
- Connor, J.; Doppalapudi, S.K.; Wajswol, E.; Ragam, R.; Press, B.; Luu, T.; Koster, H.; Tamang, T.-L.; Ahmed, M.; Lovallo, G.; et al. Postoperative Complications After Robotic Partial Nephrectomy. J. Endourol. 2020, 34, 42–47. [Google Scholar] [CrossRef]
- Yossepowitch, O.; Thompson, R.H.; Leibovich, B.C.; Eggener, S.E.; Pettus, J.A.; Kwon, E.D.; Herr, H.W.; Blute, M.L.; Russo, P. Positive surgical margins at partial nephrectomy: Predictors and oncological outcomes. J. Urol. 2008, 179, 2158–2163. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.H.; Moreira, D.M.; Okhunov, Z.; Patel, V.R.; Chopra, S.; Razmaria, A.A.; Alom, M.; George, A.K.; Yaskiv, O.; Schwartz, M.J.; et al. Positive Surgical Margins Increase Risk of Recurrence after Partial Nephrectomy for High Risk Renal Tumors. J. Urol. 2016, 196, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Volpe, A.; Blute, M.L.; Ficarra, V.; Gill, I.S.; Kutikov, A.; Porpiglia, F.; Rogers, C.; Touijer, K.A.; Van Poppel, H.; Thompson, R.H. Renal Ischemia and Function After Partial Nephrectomy: A Collaborative Review of the Literature. Eur. Urol. 2015, 68, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Parekh, D.J.; Weinberg, J.M.; Ercole, B.; Torkko, K.C.; Hilton, W.; Bennett, M.; Devarajan, P.; Venkatachalam, M.A. Tolerance of the human kidney to isolated controlled ischemia. J. Am. Soc. Nephrol. 2013, 24, 506–517. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Gan, M.; McClintock, T.R.; Volpe, A.; Borofsky, M.S.; Mottrie, A.; Stifelman, M.D. Near-infrared fluorescence imaging: Emerging applications in robotic upper urinary tract surgery. Eur. Urol. 2014, 65, 793–801. [Google Scholar] [CrossRef]
- Klatte, T.; Ficarra, V.; Gratzke, C.; Kaouk, J.; Kutikov, A.; Macchi, V.; Mottrie, A.; Porpiglia, F.; Porter, J.; Rogers, C.G.; et al. A Literature Review of Renal Surgical Anatomy and Surgical Strategies for Partial Nephrectomy. Eur. Urol. 2015, 68, 980–992. [Google Scholar] [CrossRef]
- Gill, I.S.; Eisenberg, M.S.; Aron, M.; Berger, A.; Ukimura, O.; Patil, M.B.; Campese, V.; Thangathurai, D.; Desai, M.M. “Zero ischemia” partial nephrectomy: Novel laparoscopic and robotic technique. Eur. Urol. 2011, 59, 128–134. [Google Scholar] [CrossRef]
- Rogers, C.G.; Ghani, K.R.; Kumar, R.K.; Jeong, W.; Menon, M. Robotic Partial Nephrectomy with Cold Ischemia and On-clamp Tumor Extraction: Recapitulating the Open Approach. Eur. Urol. 2013, 63, 573–578. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).