

Susceptibility Patterns in Staphylococcus and Klebsiella Causing Nosocomial Infections upon Treatment with E-Anethole-Rich Essential Oil from Clausena anisata

 , and
, and
Abstract
1. Introduction
2. Results and Discussion
2.1. Results
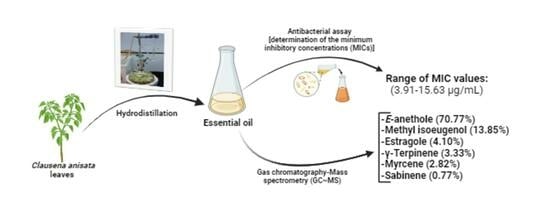
2.1.1. Extraction of the Essential Oil
2.1.2. Chemical Composition
2.1.3. Antibacterial Activity
2.2. Discussion
3. Material and Methods
3.1. Material
3.1.1. Plant Material
3.1.2. Bacterial Strains
3.1.3. Material for Bacterial Cell Culture
3.2. Methods
3.2.1. Extraction of the Essential Oil
- Y = yield of essential oil in percentage
- Me = mass of essential oil in grams
- Mp = mass of plant biomass in grams
3.2.2. GC-MS Analysis of Essential Oil of C. anisata
- IK = Kovats retention index
- Tr (Cn) = retention time of alkane at n atoms of carbons
- Tr (Cn + 1) = retention time of alkane at (n + 1) atoms of carbons
- Tr (x) = retention time for compound x
3.2.3. Antibacterial Activity
3.3. Statistical Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thorley, K.; Charles, H.; Greig, D.R.; Prochazka, M.; Mason, L.C.E.; Baker, K.S.; Godbole, G.; Sinka, K.; Jenkins, C. Emergence of extensively drug-resistant and multidrug-resistant Shigella flexneri serotype 2a associated with sexual transmission among gay, bisexual, and other men who have sex with men, in England: A descriptive epidemiological study. Lancet Infect. Dis. 2023, 23, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.A.; Baig, F.K.; Mehboob, R. Nosocomial infections: Epidemiology, prevention, control and surveillance. Asian Pac. J. Trop. Biomed. 2017, 7, 478–482. [Google Scholar] [CrossRef]
- Revelas, A. Healthcare-associated infections: A public health problem. Niger. Med. J. 2012, 53, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Emily, R.M.; Sydnor, T.M.P. Hospital epidemiology and infection control in acute-care settings. Clin. Microbiol. Rev. 2011, 24, 141–173. [Google Scholar]
- Anderson, D.J. Surgical site infections. Infect. Dis. Clin. N. Am. 2011, 25, 135–153. [Google Scholar] [CrossRef]
- Raoofi, S.; Pashazadeh Kan, F.; Rafiei, S.; Hosseinipalangi, Z.; Noorani Mejareh, Z.; Khani, S.; Abdollahi, B.; Seyghalani Talab, F.; Sanaei, M.; Zarabi, F.; et al. Global prevalence of nosocomial infection: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0274248. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.E. Risk factors in acquiring multidrug-resistant Klebsiella pneumoniae infections in a hospital setting in Saudi Arabia. Sci. Rep. 2023, 13, 11626. [Google Scholar] [CrossRef]
- Dadi, N.C.T.; Radochová, B.; Vargová, J.; Bujdáková, H. Impact of healthcare-associated infections connected to medical devices-an update. Microorganisms 2021, 9, 2332. [Google Scholar] [CrossRef]
- Wareth, G.; Neubauer, H. The Animal-foods-environment interface of Klebsiella pneumoniae in Germany: An observational study on pathogenicity, resistance development and the current situation. Vet. Res. 2021, 52, 16. [Google Scholar] [CrossRef]
- Zhu, L.; Liang, L.; Hui, J.; Lu, J.; Yang, R.; He, Q.; Tian, N.; Bai, T.; Li, X. Relationship between antibiotic exposure and carbapenem-resistant Klebsiella pneumoniae infection within four types of control patients: A systematic review and meta-analysis. J. Glob. Antimicrob. Resist. 2023, 33, 137–151. [Google Scholar] [CrossRef]
- Moehring, R.; Mahlen, S. Infections Due to Serratia species. Available online: https://www.uptodate.com/contents/infections-due-to-serratia-species (accessed on 3 January 2024).
- Williams, D.J.; Grimont, P.A.D.; Cazares, A.; Grimont, F.; Ageron, E.; Pettigrew, K.A.; Cazares, D.; Njamkepo, E.; Weill, F.-X.; Heinz, E.; et al. The genus Serratia revisited by genomics. Nat. Commun. 2022, 13, 5195. [Google Scholar] [CrossRef]
- Zhu, Q.; Xu, J.; Chen, X.; Ren, Y.; Zhao, L. Risk factors and molecular epidemiology of bloodstream infections due to carbapenem-resistant Klebsiella pneumoniae. Diagn. Microbiol. Infect. Dis. 2023, 106, 115955. [Google Scholar] [CrossRef]
- Karampatakis, T.; Tsergouli, K.; Behzadi, P. Carbapenem-resistant Klebsiella pneumoniae: Virulence factors, molecular epidemiology and latest updates in treatment options. Antibiotics 2023, 12, 234. [Google Scholar] [CrossRef] [PubMed]
- The World Health Organization (WHO). Antimicrobial Resistance. Facts Sheets. 2024. Available online: https://who.int/news-room/fact-sheets/detail/antimicrobial-resistance#:~:text=As%20a%20result%20of%20drug,severe%20illness%2C%20disability%20and%20death (accessed on 3 January 2024).
- National Institute of Diabetes and Digestive and Kidney Diseases (US). LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Luxton, T.N.; King, N.; Wälti, C.; Jeuken, L.J.C.; Sandoe, J.A.T. A Systematic review of the effect of therapeutic drug monitoring on patient health outcomes during treatment with carbapenems. Antibiotics 2022, 11, 1311. [Google Scholar] [CrossRef] [PubMed]
- Roger, C.; Louart, B. Beta-lactams toxicity in the intensive care unit: An underestimated collateral damage? Microorganisms 2021, 9, 1505. [Google Scholar] [CrossRef] [PubMed]
- Payne, L.E.; Gagnon, D.J.; Riker, R.R.; Seder, D.B.; Glisic, E.K.; Morris, J.G.; Fraser, G.L. Cefepime-induced neurotoxicity: A systematic review. Crit. Care 2017, 21, 276. [Google Scholar] [CrossRef] [PubMed]
- Bittner Fialová, S.; Rendeková, K.; Mučaji, P.; Nagy, M.; Slobodníková, L. Antibacterial activity of medicinal plants and their constituents in the context of skin and wound infections, considering European legislation and folk medicine—A review. Int. J. Mol. Sci. 2021, 22, 10746. [Google Scholar] [CrossRef]
- Ahmad, I.; Beg, A.Z. Antimicrobial and phytochemical studies on 45 Indian medicinal plants against multiple drug resistant human pathogens. J. Ethnopharmacol. 2001, 74, 113–123. [Google Scholar] [CrossRef]
- Aurelie, F.D.G.; Pierre, B.N.M.; Ascension, N.M.; Lebel, T.J. Chemical composition and biocide properties of Clausena anisata (Rutaceae) essential oil against developmental stages of the malaria vector Anopheles coluzzii. Am. J. Essent. Oils Nat. Prod. 2018, 6, 9–15. [Google Scholar]
- Senthilkumar, A.; Venkatesalu, V. Phytochemical analysis and antibacterial activity of essential oil of Clausena anisata (Wild). Hook. F. ex Benth. Int. J. Integr. Biol. 2009, 5, 116–120. [Google Scholar]
- Usman, L.A.; Hamid, A.A.; Olawore, N.O.; Fakunle, C.O.; Oladosu, I.A.; Zubair, M.F. Chemical composition of leaf essential oil of Clausena anisata growing in North Central Nigeria. JASR C. 2010, 6, 891–894. [Google Scholar]
- Makirita, W.E.; Chauka, L.; Chacha, M. Larvicidal activity of Clausena anisata fruits and leaves extracts against Anopheles gambiae Giless., Culex quinquefasciatus Say and Aedes egyptiae. Spatula DD-Peer Rev. J. Complement. Med. Drug Discov. 2015, 5, 147. [Google Scholar] [CrossRef]
- Sekar, D.K.; Kumar, G.; Karthik, L.; Bhaskara, K.V. A review on pharmacological and phytochemical properties of Aegle marmelos (L.) Corr. Serr. (Rutaceae). Asian J. Plant Sci. Res. 2011, 1, 8–17. [Google Scholar]
- Arbab, I.A.; Abdul, A.B.; Aspollah, M.; Abdullah, R.; Abdelwahab, S.I.; Ibrahim, M.Y.; Ali, L.Z. A review of traditional uses, phytochemical and pharmacological aspects of selected members of Clausena genus (Rutaceae). J. Med. Plant Res. 2012, 6, 5107–5118. [Google Scholar]
- Njonkep, S.N.J. Etude Phytochimique d’une Rutacee du Cameroun: Clausena anisata (Will). Hook f.ex.Benth. Ph.D. Thesis, University of the Mountains, Hazard, KY, USA, 2014. [Google Scholar]
- Musa, A.; Aminah, N.S.; Davies-Bolorunduro, O.F.; Kristanti, A.N.; Suhaili; Islami, A.I.; Wai, T.S.; Naing, T.T.S.P. Antimicrobial activities of the extracts and secondary metabolites from Clausena genus—A review. Open Chem. 2022, 20, 627–650. [Google Scholar] [CrossRef]
- Mouahid, A.; Dufour, C.; Badens, E. Supercritical CO2 extraction from endemic Corsican plants; comparison of oil composition and extraction yield with hydrodistillation method. J. CO2 Util. 2017, 20, 263–273. [Google Scholar] [CrossRef]
- Kaya, D.A.; Ghica, M.V.; Dănilă, E.; Öztürk, Ş.; Türkmen, M.; Albu Kaya, M.G.; Dinu-Pîrvu, C.E. Selection of optimal operating conditions for extraction of Myrtus communis L. essential oil by the steam distillation method. Molecules 2020, 25, 2399. [Google Scholar] [CrossRef]
- Naqvi, S.R.A.; Shahid, H.; Zahoor, A.F.; Saeed, M.; Usman, M.; Abbas, A.; Rasheed, M.U.; Hussain, T. Classical Methods for Obtaining Essential Oils; Chapter 25; Inamuddin, Ed.; Wiley. Scrivener Publishing LLC: Austin, TX, USA, 2023; pp. 565–582. [Google Scholar] [CrossRef]
- Bolouri, P.; Salami, R.; Kouhi, S.; Kordi, M.; Asgari Lajayer, B.; Hadian, J.; Astatkie, T. Applications of essential oils and plant extracts in different industries. Molecules 2022, 27, 8999. [Google Scholar] [CrossRef]
- De Almeida-Couto, J.M.F.; Ressutte, J.B.; Cardozo-Filho, L.; Cabral, V.F. Current extraction methods and potential use of essential oils for quality and safety assurance of foods. Chemical Sciences. An. Acad. Bras. Ciênc. 2022, 94, e20191270. [Google Scholar] [CrossRef] [PubMed]
- Agyepong, N.; Agyare, C.; Adarkwa-Yiadom, M.; Gbedema, S.Y. Phytochemical investigation and anti-microbial activity of Clausena anisata (Willd), Hook. Afr. J. Tradit. Complement. Altern. Med. 2014, 11, 200–209. [Google Scholar] [CrossRef]
- Lawal, I.O.; Grieson, D.S.; Afolayan, A.J. The antibacterial activity of Clausena anisata Hook, a South African medicinal plant. Afr. J. Tradit. Complement. Altern. Med. 2015, 12, 23–27. [Google Scholar] [CrossRef][Green Version]
- De Canha, M.N.; Kishore, N.; Kumar, V.; Meyer, D.; Nehar, S.; Singh, S.; Lall, N. The potential of Clausena anisata (Willd.) Hook.f. ex Benth against Propionibacterium acnes. S. Afr. J. Bot. 2018, 119, 410–419. [Google Scholar]
- Okokon, J.E.; Etebong, E.O.; Udobang, J.A.; Essien, G.E. Antiplasmodial and analgesic activities of Clausena anisata. Asian Pac. J. Trop. Med. 2012, 5, 214–219. [Google Scholar]
- Kumatia, E.K.; Zoiku, F.K.; Asase, A.; Tung, N.H. Antimalarial activity of the alkaloid, heptaphylline, and the furanocoumarin, imperatorin, from Clausena anisata against human Plasmodium falciparum malaria parasites: Ex vivo trophozoitocidal, schizonticidal and gametocytocidal approach. Malar. J. 2023, 22, 264. [Google Scholar] [CrossRef] [PubMed]
- Dzotam, J.K.; Touani, F.K.; Kuete, V. Antibacterial activities of the methanol extracts of Canarium schweinfurthii and four other Cameroonian dietary plants against multi-drug resistant Gram-negative bacteria. Saudi J. Biol. Sci. 2016, 23, 565–570. [Google Scholar] [CrossRef]
- Seukep, J.A.; Sandjo, L.P.; Ngadjui, B.T.; Kuete, V. Antibacterial activities of the methanol extracts and compounds from Uapaca togoensis against Gram-negative multi-drug resistant phenotypes. S. Afr. J. Bot. 2016, 103, 1–5. [Google Scholar] [CrossRef]
- Mogana, R.; Adhikari, A.; Tzar, M.N.; Ramliza, R.; Wiart, C. Antibacterial activities of the extracts, fractions and isolated compounds from Canarium patentinervium Miq. against bacterial clinical isolates. BMC Complement. Med. Ther. 2020, 20, 55. [Google Scholar] [CrossRef] [PubMed]
- Jung, I.G.; Jeong, J.Y.; Yum, S.H.; Hwang, Y.J. Inhibitory effects of selected medicinal plants on bacterial growth of methicillin-resistant Staphylococcus aureus. Molecules 2022, 27, 7780. [Google Scholar] [CrossRef]
- Said-Al Ahl, H.A.H.; Hikal, W.M.; Tkachenko, K.G. Essential oils with potential as insecticidal agents: A review. Int. J. Environ. Plan. Manag. 2017, 3, 23–33. [Google Scholar]
- Yaouba, A.; Tatsadjieu, N.L.; Jazet, P.M.; Etoa, F.X.; Mbofung, C.M. Antifungal properties of essential oils and some constituents to reduce foodborne pathogen. J. Yeast Fungal Res. 2010, 1, 001–008. [Google Scholar]
- Issakou. Determination des caractéristiques chimiques, des activités antiradicalaires, anti-inflammatoires et antifongiques des huiles essentielles de C. anisata et de Capsicum annum. Master’s Thesis, Université de Yaoundé I, Yaounde, Cameroon, 2010. [Google Scholar]
- Delamare, A.P.L.; Moschen-Pistorello, I.T. Antibacterial activity of the essential oil of Salvia officinalis L. and Salvia triloba L. cultivated in South Brazil. Food Chem. 2007, 100, 603–608. [Google Scholar] [CrossRef]
- Tepe, B.; Daferera, D. antimicrobial and antioxidant activities of the essential oil and various extractes of Salvia tomentosa Miller (Lamiaceae). Food Chem. 2005, 90, 333–340. [Google Scholar] [CrossRef]
- Konaté, K.; Mavoungou, J.F.; Lepengué, A.N.; Aworet-Samseny, R.R.R.; Hilou, A.; Souza, A.; Dicko, M.H.; M’Batchi, B. Antibacterial activity against β-lactamase producing methicillin and ampicillin-resistants Staphylococcus aureus: Fractional inhibitory concentration index (FICI) determination. Ann. Clin. Microbiol. Antimicrob. 2012, 11, 1–12. [Google Scholar] [CrossRef]
- Kowalczyk, P.; Koszelewski, D.; Brodzka, A.; Kramkowski, K.; Ostaszewski, R. Evaluation of antibacterial activity against nosocomial pathogens of an enzymatically derived α-aminophosphonates possessing coumarin scaffold. Int. J. Mol. Sci. 2023, 24, 14886. [Google Scholar] [CrossRef]
- Kuaté Tokam, C.R.; Bisso Ndezo, B.; Boulens, N.; Allémann, E.; Delie, F.; Dzoyem, J.P. Antibiofilm activity and synergistic effects of thymol-loaded poly (Lactic-Co-Glycolic Acid) nanoparticles with amikacin against four Salmonella enterica Serovars. Can. J. Infect. Dis. Med. Microbiol. 2023, 2023, 7274309. [Google Scholar] [CrossRef]
- Pichette, A.; Larouche, P.L.; Lebrun, M.; Legault, J. Composition and antibacterial activity of Abies balsamea essential oil. Phytother. Res. 2006, 20, 371–373. [Google Scholar] [CrossRef]
- de Sousa Eduardo, L.; Farias, T.C.; Ferreira, S.B.; Ferreira, P.B.; Lima, Z.N.; Ferreira, S.B. Antibacterial activity and time-kill kinetics of positive enantiomer of α-pinene against strains of Staphylococcus aureus and Escherichia coli. Curr. Top. Med. Chem. 2018, 18, 917–924. [Google Scholar] [CrossRef]
- Brice, R.P.; Boniface, P.K.; Eutrophe Le Doux, K.; Vincent, N.; Yanick, K.M.D.; Paul, K.L.; Fabrice, F.B. Extracts from Cardiospermum grandiflorum and Blighia welwitschii (Sapindaceae) reveal antibacterial activity against Shigella species. S. Afr. J. Bot. 2024, 164, 419–428. [Google Scholar]
- AlBalawi, A.N.; Elmetwalli, A.; Baraka, D.M.; Alnagar, H.A.; Alamri, E.S.; Hassan, M.G. Chemical constituents, antioxidant potential, and antimicrobial efficacy of Pimpinella anisum extracts against multidrug-resistant bacteria. Microorganisms 2023, 11, 1024. [Google Scholar] [CrossRef] [PubMed]
- Senatore, F.; Oliviero, F.; Scandolera, E.; Taglialatela-Scafati, O.; Roscigno, G.; Zaccardelli, M.; De Falco, E. Chemical composition, antimicrobial and antioxidant activities of anethole-rich oil from leaves of selected varieties of fennel [Foeniculum vulgare Mill. ssp. vulgare var. azoricum (Mill.) Thell]. Fitoterapia 2013, 90, 214–219. [Google Scholar] [PubMed]
- Kubo, I.; Fujita, K.-I.; Nihei, K.-I. Antimicrobial activity of anethole and related compounds from aniseed. J. Sci. Food Agric. 2008, 88, 242–247. [Google Scholar] [CrossRef]
- Kwiatkowski, P.; Pruss, A.; Masiuk, H.; Mnichowska-Polanowska, M.; Kaczmarek, M.; Giedrys-Kalemba, S.; Dołęgowska, B.; Zielińska-Bliźniewska, H.; Olszewski, J.; Sienkiewicz, M. The effect of fennel essential oil and trans-anethole on antibacterial activity of mupirocin against Staphylococcus aureus isolated from asymptomatic carriers. Postep. Dermatol. Allergol. 2019, 36, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, M.A.A.; Alves, M.S.; Santos, B.; Silva, E.V.A.; Araújo, F.S.M.; Bezerra, M.M.S.L.; Silva, P.O.A.; Rêgo, V.G.S.; Pessôa, H.L.F.; Oliveira Filho, A.A. Evaluation of the antibacterial activity of trans-anethole against Enterococcus cloacae and Enterococcus faecalis strains of food origin. Braz. J. Biol. 2023, 83, e269245. [Google Scholar] [CrossRef] [PubMed]
- Trombetta, D.; Castelli, F.; Sarpietro, M.G.; Venuti, V.; Cristani, M.; Daniele, C.; Saija, A.; Mazzanti, G.; Bisignano, G. Mechanisms of antibacterial action of three monoterpenes. Antimicrob. Agents Chemother. 2005, 49, 2474–2478. [Google Scholar] [CrossRef] [PubMed]
- Badawy, M.E.I.; Marei, G.I.K.; Rabea, E.I.; Taktak, N.E.M. Antimicrobial and antioxidant activities of hydrocarbon and oxygenated monoterpenes against some foodborne pathogens through in vitro and in silico studies. Pestic. Biochem. Phys. 2019, 158, 185–200. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, A.C.; Meireles, L.M.; Lemos, M.F.; Guimarães, M.C.C.; Endringer, D.C.; Fronza, M.; Scherer, R. Antibacterial activity of terpenes and terpenoids present in essential oils. Molecules 2019, 24, 2471. [Google Scholar] [CrossRef]
- Masyita, A.; Mustika Sari, R.; Dwi Astuti, A.; Yasir, B.; Rahma Rumata, N.; Emran, T.B.; Nainu, F.; Simal-Gandara, J. Terpenes and terpenoids as main bioactive compounds of essential oils, their roles in human health and potential application as natural food preservatives. Food Chem. X 2022, 13, 100217. [Google Scholar] [CrossRef]
- Zengin, H.; Baysal, A.H. Antibacterial and antioxidant activity of essential oil terpenes against pathogenic and spoilage-forming bacteria and cell structure-activity relationships evaluated by SEM microscopy. Molecules 2014, 19, 17773–17798. [Google Scholar] [CrossRef]
- Roman, H.; Niculescu, A.G.; Lazăr, V.; Mitache, M.M. Antibacterial efficiency of Tanacetum vulgare essential oil against ESKAPE pathogens and synergisms with antibiotics. Antibiotics 2023, 12, 1635. [Google Scholar] [CrossRef]
- Li, H.; Song, X.; Li, H.; Zhu, L.; Cao, S.; Liu, J. Sesquiterpenes and monoterpenes from the leaves and stems of Illicium simonsii and their antibacterial activity. Molecules 2022, 27, 1115. [Google Scholar] [CrossRef]
- Mahizan, N.A.; Yang, S.K.; Moo, C.L.; Song, A.A.; Chong, C.M.; Chong, C.W.; Abushelaibi, A.; Lim, S.E.; Lai, K.S. Terpene derivatives as a potential agent against antimicrobial resistance (AMR) pathogens. Molecules 2019, 24, 2631. [Google Scholar] [CrossRef] [PubMed]
- da Silva, L.Y.S.; Paulo, C.L.R.; Moura, T.F.; Alves, D.S.; Pessoa, R.T.; Araújo, I.M.; de Morais Oliveira-Tintino, C.D.; Tintino, S.R.; Nonato, C.F.A.; da Costa, J.G.M.; et al. Antibacterial activity of the essential oil of Piper tuberculatum Jacq. Fruits against multidrug-resistant strains: Inhibition of efflux pumps and β-Lactamase. Plants 2023, 12, 2377. [Google Scholar] [CrossRef] [PubMed]
- Cruz, B.G.; de Freitas, T.S.; Costa, M.d.S.; da Silva, A.R.P.; Coutinho, H.D.M.; de Morais, S.M.; Marinho, E.S.; Teixeira, A.M.R.; dos Santos, H.S. Chemical composition, antibacterial and inhibitory activity of the efflux pump of essential oils from Croton piauhiensis Müll. Nutraceuticals 2023, 3, 591–604. [Google Scholar] [CrossRef]
- Songue, J.L.; Kouam; Dongo, E.; Mpondo, T.N.; White, R.L. Chemical constituents from stem bark and roots of Clausena anisata. Molecules 2012, 17, 13673–13686. [Google Scholar] [CrossRef]
- Ojewole, J.A. Hypoglycaemic effect of Clausena anisata (Willd, Hook) methanolic root extract in rats. J. Ethnopharmacol. 2012, 81, 231–725. [Google Scholar] [CrossRef]
- Clinical Laboratory Standard Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard-Ninth Edition M07 A9. Clin. Lab. Stand. Inst. 2012, 29, 2012. [Google Scholar]


{kind=link}
{kind=link}
| Serial N° | RT | IK | Identified Compound | Percentage (%) |
|---|---|---|---|---|
| 1 | 10.547 | 933 | α-Pinene | 0.26 |
| 2 | 12.062 | 971 | Sabinene | 0.77 |
| 3 | 12.270 | 976 | β-Pinene | 0.26 |
| 4 | 12.640 | 986 | Myrcene | 2.82 |
| 5 | 14.195 | 1021 | p-Cymene | 0.52 |
| 6 | 14.407 | 1025 | Limonene | 0.77 |
| 7 | 15.118 | 1041 | E-β-Ocimene | 0.26 |
| 8 | 15.795 | 1055 | γ-Terpinene | 3.33 |
| 9 | 17.153 | 1084 | Terpinolene | 0.25 |
| 10 | 21.515 | 1171 | α-Terpineol | Nd |
| 11 | 22.562 | 1191 | Estragole | 4.10 |
| 12 | 25.115 | 1242 | para Anisaldehyde | 0.25 |
| 13 | 25.497 | 1250 | Z-Anethole | 0.25 |
| 14 | 27.515 | 1291 | E-Anethole | 0.77 |
| 15 | 28.195 | 1305 | Cinamyl alcool | Nd |
| 16 | 32.175 | 1387 | Cinamylacetate | 0.52 |
| 17 | 33.395 | 1413 | Methyleugenol | 0.52 |
| 18 | 34.552 | 1438 | β-Caryophyllene | Nd |
| 19 | 34.922 | 1447 | Isoeugenol | 0.25 |
| 20 | 36.123 | 1473 | γ-Gurjunene | 0.50 |
| 21 | 36.780 | 1487 | Methyl iso eugenol | 13.85 |
| Bacterial Strains | MIC (µg/mL) | MBC (µg/mL) | MIC/MBC |
|---|---|---|---|
| Bacillus spp. | 31.25 | 31.25 | 1 |
| Staphylococcus aureus | 15.63 | 15.63 | 1 |
| Klebsiella pneumoniae | 3.91 | 15.63 | 4 |
| Pseudomonas aeroginosa | 62.5 | 62.5 | 1 |
| Staphylococcus epidermidis | 3.91 | 7.81 | 2 |
| Serratia spp. | 3.91 | / | / |
| Escherichia coli | 31.25 | 62.5 | 2 |
| Salmonella typhimurium | 31.25 | 125 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguimatsia, F.; Momo, E.J.; Keilah Lunga, P.; Lum Tamanji, V.; Pone Kamdem, B.; Jazet Dongmo, P.M. Susceptibility Patterns in Staphylococcus and Klebsiella Causing Nosocomial Infections upon Treatment with E-Anethole-Rich Essential Oil from Clausena anisata. Drugs Drug Candidates 2024, 3, 244-255. https://doi.org/10.3390/ddc3010014
Nguimatsia F, Momo EJ, Keilah Lunga P, Lum Tamanji V, Pone Kamdem B, Jazet Dongmo PM. Susceptibility Patterns in Staphylococcus and Klebsiella Causing Nosocomial Infections upon Treatment with E-Anethole-Rich Essential Oil from Clausena anisata. Drugs and Drug Candidates. 2024; 3(1):244-255. https://doi.org/10.3390/ddc3010014
Chicago/Turabian StyleNguimatsia, François, Evariste Josué Momo, Paul Keilah Lunga, Virginia Lum Tamanji, Boniface Pone Kamdem, and Pierre Michel Jazet Dongmo. 2024. "Susceptibility Patterns in Staphylococcus and Klebsiella Causing Nosocomial Infections upon Treatment with E-Anethole-Rich Essential Oil from Clausena anisata" Drugs and Drug Candidates 3, no. 1: 244-255. https://doi.org/10.3390/ddc3010014
APA StyleNguimatsia, F., Momo, E. J., Keilah Lunga, P., Lum Tamanji, V., Pone Kamdem, B., & Jazet Dongmo, P. M. (2024). Susceptibility Patterns in Staphylococcus and Klebsiella Causing Nosocomial Infections upon Treatment with E-Anethole-Rich Essential Oil from Clausena anisata. Drugs and Drug Candidates, 3(1), 244-255. https://doi.org/10.3390/ddc3010014