Abstract
The pancreas is a vital organ nestled deep within the abdomen, playing a crucial role in both endocrine and exocrine functions. It is elongated and tadpole-shaped, with a head, body, and tail. The intricate connections to adjacent structures through a network of blood vessels, ducts, and supportive tissue transform pancreatic cancer into one of the most fatal malignancies globally as a result of a typically late diagnosis and metastatic form of the disease. Lymph node metastasis (LNM) is prevalent in the majority of individuals diagnosed with pancreatic cancer, signifying a critical factor influencing prognostic outcomes. The para-aortic lymph nodes (PALN) play an important role in the lymphatic drainage of various organs, including the kidneys, pancreas, and parts of the gastrointestinal tract. In pancreatic cancer, the risk of PALN metastasis holds considerable clinical significance, and diagnosing your involvement is primordial to therapeutic decisions and to increase the survival expectations of these patients.
1. Pancreatic Cancer
1.1. Epidemiology
Pancreatic cancer epidemiology is characterized by a comparably low incidence relative to other malignancies but exhibits a disproportionately high mortality rate, ranking prominently among the leading causes of cancer-related deaths globally [1]. The susceptibility to pancreatic cancer escalates with age, predominantly affecting individuals over 60 [2]. Established risk factors include smoking, obesity, and a familial history of pancreatic cancer. Unfortunately, the disease often manifests at an advanced stage, contributing significantly to its bleak prognosis. Despite ongoing research endeavors and advancements in treatment modalities, the overall survival (OS) rate remains distressingly low [1]. The imperative for continued exploration into early detection methods and innovative therapies is underscored, presenting a critical avenue for enhancing outcomes in the face of this formidable and challenging cancer. To obtain the most current and precise epidemiological information, consulting the recent medical literature or authoritative health organizations is advised [3].
As one of the most fatal malignancies globally, pancreatic cancer poses a substantial challenge in the global burden of disease. In 2020, there were approximately 500,000 new cases and 470,000 deaths attributed to pancreatic cancer worldwide. The global incidence rate for pancreatic cancer in 2020 was 4.9 per 100,000 for both sexes combined, with a mortality rate of 4.5 per 100,000. Most countries witnessed increasing trends in both the incidence and mortality of pancreatic cancer. Delving into the underlying reasons for variations in international patterns of pancreatic cancer incidence and mortality is crucial for informing global cancer control strategies [4].
1.2. Pancreas Anatomy
The pancreas is a vital organ nestled deep within the abdomen, playing a crucial role in both endocrine and exocrine functions. It is situated behind the stomach and spans horizontally across the posterior abdominal wall. Structurally, the pancreas is elongated and tadpole-shaped, with a head, body, and tail [5]. The head of the pancreas lies nestled within the concavity of the duodenum, forming a close anatomical relationship with it. The body extends horizontally across the posterior abdominal cavity, while the tail extends towards the spleen on the left side. The pancreas is intricately connected to adjacent structures through a network of blood vessels, ducts, and supportive tissue [2]. Functionally, the pancreas is a dual-purpose organ. Exocrine cells, arranged in clusters, known as acini, produce digestive enzymes that are carried through a network of ducts into the duodenum. These enzymes play a crucial role in breaking down fats, proteins, and carbohydrates during the digestive process. Simultaneously, the pancreas houses clusters of endocrine cells, primarily in the islets of Langerhans scattered throughout the organ. These cells, including alpha and beta cells, release hormones like insulin and glucagon directly into the bloodstream. These hormones are vital in regulating glucose levels, playing a key role in metabolic processes throughout the body [6].
1.3. Pancreatic Cancer Subtypes
Pancreatic cancer includes various distinct types, each defined by its unique anatomical location within the pancreas and specific cellular components. The most common form, pancreatic ductal adenocarcinoma (PDAC), originates in the ducts that transport digestive enzymes, typically in the pancreas’s head, comprising most cases [6]. Less common subtypes include acinar cell carcinoma, from enzyme-producing cells, and pancreatic neuroendocrine tumors, from hormone-producing cells. Pre-cancerous lesions like intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neoplasms (MCNs) can transform malignantly. This diversity necessitates personalized diagnosis, treatment, and management approaches tailored to each subtype’s characteristics [7,8,9].
1.4. Diagnosis
The American Joint Committee on Cancer (AJCC) 8th edition staging system for pancreatic cancer offers a comprehensive framework for stratifying the disease based on tumor characteristics, lymph node involvement, and the presence of metastasis. In this classification, the T (tumor) category delineates the extent of the primary tumor. T1 signifies tumors confined to the pancreas, while T2 indicates localized spread beyond the pancreas. T3 involves the nearby structure invasion, such as blood vessels, and T4 encompasses extensive invasion into adjacent organs. The N (nodal) category assesses regional lymph node involvement. N0 indicates the absence of regional lymph node metastasis (LNM), while N1 denotes the presence of cancer cells in nearby lymph nodes. Further stratification is provided by N2, which indicates more distant or numerous lymph node involvement. Metastasis is captured by the M (metastasis) category. M0 signifies the absence of distant metastasis, whereas M1 indicates the presence of cancer that has spread to distant organs or tissues. Combining T, N, and M classifications yields the overall stage grouping. Stage 0 represents localized disease, Stages I and II involve locally advanced tumors, and Stages III and IV signify more advanced disease with regional or distant spread. This detailed AJCC classification system serves as a crucial tool for clinicians, facilitating precise staging, treatment planning, and assessment of prognosis in pancreatic cancer management [10,11,12].
2. Lymphatic System
2.1. Background
The lymphatic system has been described in the history of medicine for many centuries; Hippocrates wrote about “white blood in the nodes”, and Aristotle reiterated the presence of fibers containing colorless fluid between blood vessels and nerves. Gasparo Aselli, in 1627, was the first to officially recognize the lymphatic system, which was continuously studied during the XVII and XVIII centuries when medicine began to seek to understand better aspects of lymph, lymphatic drainage, and lymphatic anatomy. However, it was only in the last few decades that we observed a boom in scientific studies related to this system and related to the fact that this incredible physiological chain is involved in a multitude of diseases, such as cancer [13,14].
The lymphatic system, facilitated by lymphatic vessels, is a vascular network in higher vertebrates responsible for vital functions, including tissue pressure regulation, immunological surveillance, and the absorption of dietary fats. Lymphatic vessels are part of a unidirectional chain, which transports fluids and proteins, absorbing them from the interstitial space and returning them to blood circulation [15].
In addition to regulating tissue fluids, these vessels also function as an essential transport pathway for immune cells. Lymph nodes are like potent retention reservoirs, where white blood cells proliferate. The relationship between the lymphatic system and the dissemination of tumor cells, and consequently, metastasis in cancer has been an exciting subject of studies over the last few years. Cancer cells can infiltrate lymphatic vessels, migrate to tumor-draining lymph nodes, proliferate, and, in some cases, metastasize to other organs [13,15].
2.2. Lymphatic System in Metastasis
Lymphatic vessels serve as conduits for immune cell reabsorption, a process that may inadvertently facilitate the transport of cancer cells to regional lymph nodes and distant organs. The involvement of lymph nodes in oncological diagnoses holds profound prognostic implications for therapeutic strategies and predicting patient survival rates [13]. Lymphatic metastasis is primarily a passive phenomenon, often facilitated by peritumoral lymphatic tissue presence enveloping malignant tumors. However, this process is intricately regulated by various mechanical and chemotactic factors. Discrepancies in hydrostatic pressure following cancer cell infiltration into the extracellular matrix result in fluid flow, aiding the transport of cancer cells to peritumoral lymphatic capillaries. Upon reaching these capillaries, cytoplasmic mechanisms drive the mobilization of cancer cells along the endothelial surface. This migratory phenomenon and subsequent invasion of the lymphatic lumen entail a continuous induction of gap formation or the exploitation of pre-existing interendothelial spaces [15].
As tumors grow, the intratumoral interstitial fluid pressure increases, altering the lymphatic flow towards peritumoral lymphatic tissues and consequently augmenting the interstitial fluid volume. Smooth muscles lining lymphatic vessel walls facilitate lymph propulsion through rhythmic contractions, ensuring access to the lymphatic lumen. Consequently, cancer cells, either individually or in clusters, embolize, traversing the subcapsular sinus and penetrating the nodule cortex. This migration may entail bypassing the nodular structure through lymphatic–venous connections or infiltrating the nodule entirely, subsequently progressing towards efferent lymphatic vessels and adjacent lymph nodes [15].
Tumors typically exhibit elevated interstitial fluid pressure, facilitating the infiltration of cancer cells into the lymphatic vessels enveloping the tumor. Consequently, interstitial flow impacts the migratory behavior of cancer cells extending beyond mechanical forces, encompassing autologous chemotaxis mechanisms [13]. These mechanisms enable the detachment of cell clusters from the primary tumor, mediated by migratory flow from the tumor to the lymphatic vessels. Cancer cells can navigate toward and invade lymphatic vessels via chemokine gradients generated by lymphatic endothelial cells, which are physiologically predisposed to attract leukocytes under normal conditions. While hematogenous dissemination remains a possibility, metastasis predominantly occurs through association with tumor lymphangiogenesis. This sequential model of metastasis evolution involves the initial spread of tumor cells to the lymphatic system, followed by dissemination to the circulatory system [15].
Lymphatic endothelial cells undergo dynamic alterations during tumor progression, fostering metastatic dissemination and augmenting immunoregulatory functions, thereby enhancing the likelihood of metastasis. In essence, the beneficial effects of lymphatic tissues on tumor immunity can be reversed, thereby promoting tumor growth. Normally, lymphatic endothelial cells transport immune mediators from peripheral organs to lymph nodes, thereby initiating immune responses. Additionally, they facilitate T-cell responses through various mechanisms [13,14].
2.3. Pancreatic Lymphatic System
The lymphatic ducts of the pancreas arise from the interlobular grid within the pancreatic parenchyma. Lymphatic capillaries consist of a monolayer of endothelial cells featuring intermittent intercellular connections and are devoid of a basal lamina. Lymph and its cellular constituents are conveyed to larger lymphatic conduits, comprising smooth muscle elements to promote circulation. The incoming collecting lymphatic vessels enter lymph nodes for filtration, while the outgoing vessels, termed efferent collecting vessels, guide the lymph through the principal conduits of the lymphatic system, the thoracic duct and the right lymphatic trunk, eventually reintegrating it into the circulatory system [16,17,18].
The organization and interplay of lymphatic vessels and lymph nodes within the pancreas present a complex conundrum due to their close association with blood vessels. Generally, pancreatic lymph nodes are classified into distinct regions based on their proximity to the drainage areas of the pancreatic gland. In instances of inflammation and tumor progression, an influx of growth factors and chemokines triggers the remodeling and expansion of lymphovascular tissue, which correlates with the invasiveness of cancer. Elevated lymphatic vessel density in tumors located at the pancreas head of PDAC has been demonstrated to correlate with heightened LNM and with poor survival rates linked to adverse tumor differentiation status [16,18,19,20].
3. LNM in Pancreatic Cancer
3.1. Background
The significance of detecting and evaluating LNM in pancreatic cancer cannot be overstated, given its profound implications for prognosis and treatment planning. Lymph node involvement serves as an important factor influencing the staging of pancreatic cancer, providing crucial insights into the extent of disease dissemination. The identification of metastasis in regional lymph nodes not only aids in categorizing the cancer’s stage but also facilitates a more nuanced and precise prognosis. Furthermore, the status of lymph nodes informs treatment decisions, guiding clinicians in determining the most appropriate therapeutic interventions tailored to the individual patient’s needs [21]. In the complex landscape of pancreatic cancer, where early detection remains challenging and the disease often presents at an advanced stage, the presence or absence of LNM emerges as a key indicator in prognosis. Understanding the comprehensive extent of lymphatic involvement is imperative for tailoring surgical approaches and making informed decisions regarding adjuvant therapies such as chemotherapy or radiation, which may confer benefits. Therefore, the accurate detection and thorough evaluation of LNM are integral elements in shaping comprehensive and effective strategies for managing patients with pancreatic cancer [22].
LNM is very often found in individuals diagnosed with pancreatic cancer, signifying an analytical factor influencing prognostic outcomes. Notable strides in the field involve innovative staging classifications for pancreatic, gastric, and colorectal cancers, incorporating metrics such as metastatic lymph node ratio and count. The exploration of pancreatectomy with extended lymphadenectomy, aimed at improving prognostic indicators, has stirred debate, with conflicting evidence on its impact on patient survival. Varied prospective studies offer differing perspectives; some suggest prolonged lymphadenectomy contributes to long-term survival, while others emphasize heightened morbidity without substantial survival advantages. The ongoing controversy stems from the intricate and ambiguous patterns of LNM dissemination in pancreatic cancer [23].
Recent findings propose that neoadjuvant chemotherapy or chemoradiation holds promise in augmenting long-term survival for pancreatic cancer patients, presenting a comparable efficacy to traditional adjuvant therapy. Nevertheless, persistent challenges exist in identifying suitable candidates for neoadjuvant therapy, particularly those with potentially systemic disease. Effectively addressing these intricacies demands continuous research efforts and a more profound comprehension of the complex dynamics underlying pancreatic cancer and its intricate interplay with LNM [21,23].
3.2. Clinical–Anatomical Classification
The Japanese Pancreatic Society (JPS) has formulated a detailed classification system based on extensive data on pancreatic carcinoma, described in Figure 1, that categorizes regional and nearby lymph nodes. This classification system provides a comprehensive nomenclature for lymph node stations relevant to pancreatic cancer surgery. This standardized nomenclature has gained international recognition and has paved the way for establishing global standards for the extent of lymphadenectomy in pancreatic cancer procedures. In 2014, the International Study Group on Pancreatic Surgery (ISGPS) released consensus recommendations aligning with the JPS classification [24]. An alternative drainage route has been identified, wherein lymphatic drainage follows the posterior superior pancreaticoduodenal artery to the pyloric node. These pathways, also referred to as superior or ascending pathways, ultimately drain into the celiac node [11]. Conversely, for the caudal portion of the pancreatic head and the uncinate process, lymphatic drainage follows the inferior pancreaticoduodenal vessels to the lymph nodes around the superior mesenteric artery, subsequently draining into the retroperitoneal para-aortic lymph nodes (PALN) [25]. This pathway is recognized as an inferior or descending pathway. In pancreatic cancer, lymph node infiltration stands out as a critical prognostic marker, alongside other influential factors such as tumor histology, size, resection margin status, grade, and lymphovascular invasion. Predominantly, metastases in LNM are detected within the peripancreatic nodal cluster, encompassing anterior and posterior peripancreatic nodes, as well as pancreaticoduodenal, pyloric, and inferior nodes. Tumor size correlates with the likelihood of lymph node positivity, with larger tumors more commonly metastasizing to PALN [24].
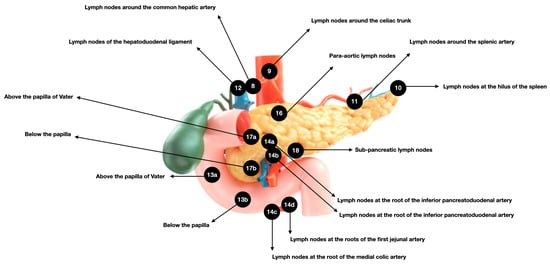
Figure 1.
Regional lymph nodes of the pancreas classification according to JPS. The subdivided regions: 13 refers to the posterior pancreaticoduodenal lymph nodes, 14 to the lymph nodes around the superior mesenteric artery, and 17 to the anterior pancreaticoduodenal lymph nodes.
3.3. PALN
The PALN, also known as retro aortic lymph nodes, are a group of lymph nodes situated along the para-aortic region, which runs parallel to the aorta in the abdominal cavity. These nodes play an essential function in lymphatic drainage of various organs, including the kidneys, pancreas, and parts of the gastrointestinal tract [25]. The PALN serves as a key filtering station for lymphatic fluid, facilitating the removal of waste products, pathogens, and cellular debris [26]. Due to their strategic location, these nodes are often examined in the context of cancer staging and metastasis assessment, particularly in abdominal and pelvic malignancies [27]. The status of the PALN is significant in understanding the potential spread of cancer cells and is instrumental in determining the appropriate course of treatment, such as surgery, radiation therapy, or systemic therapies. A detailed examination of this lymph node offers valuable insights into overall lymphatic drainage patterns, aiding clinicians in formulating comprehensive and tailored treatment strategies for patients with various medical conditions, including cancer [24,28]. PALNs are considered “extra-regional” lymph nodes, becoming involved only after metastatic spread has already affected the peri-pancreatic first-echelon lymph nodes [29]. Several reports, although most of them share the bias of retrospective analysis, describe that the prognosis of patients with metastatic PALN is significantly worse if compared with patients with negative metastatic cases [30].
In pancreatic cancer, the risk of PALN metastasis holds considerable clinical significance. Due to the intricate lymphatic drainage patterns in the abdominal region, pancreatic tumors are prone to spreading to this lymph node [27]. The PALN is a primary site for regional metastasis, providing a conduit for cancer cells to move beyond the primary tumor site. The PALN assessment involvement is essential in determining the extent of disease spread and plays an important role in cancer staging. The presence of metastasis in these nodes may influence treatment decisions, including considering more aggressive surgical interventions or targeted therapies [29]. Consequently, a thorough understanding of the risk and detection of PALN metastasis in pancreatic cancer is imperative for clinicians to devise effective and personalized treatment strategies that address the complexities of the disease and improve patient outcomes [24,27,30].
4. Imaging Diagnosis and Sentinel Lymph Node
In radiologic diagnostic imaging, it is imperative to morphologically differentiate between enlarged lymph nodes indicative of metastasis and those that are normal or reactive. Computed tomography (CT) scans, in particular, offer discernment capability in malignancy through contrast enhancement [31]. Typically, normal or reactive lymph nodes exhibit homogeneous enhancement despite their enlargement. Enlarged nodes observed in the periportal and common hepatic nodal groups are nonspecific findings that may also be present in patients with jaundice and indwelling stents, chronic pancreatitis, or node-negative pancreatic cancer [32]. Nevertheless, a comprehensive understanding of preoperative imaging scans is essential before surgical resection, as it enables surgeons to navigate the procedure effectively and potentially circumvent unnecessary laparotomies. The sentinel lymph node technique in pancreatic cancer has been assessed to enable the preoperative identification of patients with lymphatic spread, enhancing staging accuracy and reducing unnecessary morbidity [33].
5. Management of Para-Aortic Lymph Node Metastasis
Diagnosing PALN involvement in pancreatic cancer preoperatively is exceptionally challenging [24,31]. Various imaging modalities, including computed tomography (CT), magnetic resonance imaging (MRI), and (18) F-fluorodeoxyglucose positron-emission tomography (FDG-PET), are utilized for preoperative detection, but their effectiveness remains conflictive [34]. Recent deep learning based on pancreatic cancer detection with artificial intelligence (PANDA), a type of machine learning, sheds light on LNM diagnosis and can detect and classify pancreatic lesions with high accuracy via non-contrast CT [35]. In cases where radical resection is considered, intraoperative histopathological examination of frozen PALN sections becomes necessary, which is particularly valuable for certain subsets of patients to inform surgical decision-making and guide the extent of surgery. The subsets of patients who typically benefit from this procedure include patients with resectable or borderline resectable pancreatic cancer who may undergo frozen section analysis of PALN to determine the extent of lymph node involvement. Positive findings might lead to a decision against proceeding with extensive surgery due to the poor prognosis associated with metastatic spread [24].
A prevailing sentiment among surgeons is that PALN metastases often signify systemic disease. Consequently, many advocate against radical surgery, including extended lymphadenectomy, for patients with positive metastasis in this lymph node [24]. The detection of PALN metastasis significantly influences surgical strategy, with most surgeons opting for less aggressive approaches if these metastases are present [30]. Notably, PALN metastasis frequently coexists with distant metastases, such as liver involvement or peritoneal dissemination. In the absence of these distant metastases, the presence of PALN metastasis becomes a crucial factor in defining the resectability of the disease. Therefore, identifying PALN metastasis presence is a crucial factor in determining the overall surgical approach for patients with pancreatic cancer [24,28,29].
6. Para-Aortic Lymph Node Metastasis in Patient Prognosis
Over the past few years, numerous studies have consistently underscored the importance of detecting PALN metastasis as a significant prognostic indicator in pancreatic cancer. Its association with other clinicopathological factors can assist in therapeutic decision-making and predict metastasis to other organs, potential recurrences, and, most importantly, the patient’s likelihood of survival at diagnosis time. This emphasizes the importance of comprehensive assessment and monitoring of PALN involvement in pancreatic cancer patient management [30].
In patients with pancreatic cancer, the identification of metastasis to PALN is widely acknowledged as a significant harbinger of adverse prognosis. However, the substantial frequency of such metastases has prompted considerable debate regarding their prognostic implications [27]. There exists ambiguity regarding whether all individuals with PALN involvement inevitably experience poor surgical outcomes, thus engendering discourse on the nature of this association—whether it is directly indicative of prognosis or merely a coincidental finding [30]. Furthermore, the detection of micrometastases within PALNs, which often evade identification through routine hematoxylin and eosin (HE) staining, presents a significant challenge. These occult micrometastases may exert a notable influence on prognostic outcomes following potentially curative pancreatectomy for pancreatic cancer. Hence, the imperative for more refined diagnostic modalities to accurately delineate and evaluate PALN involvement, thereby enhancing patient prognostication and optimizing therapeutic strategies, becomes increasingly apparent [36,37].
Sho et al. demonstrated in their study that patients with metastatic PALN exhibited significantly poorer survival compared to those without (17 vs. 23 months; p < 0.001) [38]. Schwarz et al. demonstrate similar findings, but in addition to corroborating this association, they also assessed variations among different diagnostic analyses. They noted that the median OS for patients with and without the involvement of PALN in frozen section analysis was 9.7 vs. 28.5 months, respectively (p = 0.012), and 15.7 vs. 27.2 months (p = 0.050) when assessed using hematoxylin and eosin staining [39].
In their analysis, Doi et al. delineate metastasis to PALN as the sole independent factor significantly associated with mortality in pancreatic cancer. Approximately 84% of patients with positive PALN succumbed within one year, contrasting with 46% of those with negative status [40]. Paiella et al., in a 2016 meta-analysis, corroborate these findings. They ascertain that up to that time, metastasis to PALN was linked to heightened mortality compared to patients with negative PALN, irrespective of regional nodal status (p < 0.001). This was accompanied by a notably diminished median survival among patients with PALN metastasis [30]. In contrast, Sperti et al. and Hemdel et al. findings demonstrate that even though lymph node status and PALN metastases were associated with poor survival at univariate analysis, they were not independent prognostic factors [41,42].
Lee et al. analyzed the specific prognostic role in resectable pancreatic cancer, revealing that unexpected malignant PALN involvement has a comparable negative prognostic impact on radiologically evident PALN metastasis. These findings underscore the necessity for the immediate pathological evaluation of unexpected PALN enlargements and consideration of surgical strategy modification on-site [28]. Similar results were observed by Hempel, where all patients underwent curative pancreatoduodenectomy or total pancreatectomy, yielding a median OS of 14.1 and 20.2 months for patients with metastatic PALN and those without, respectively [42]. This aligns with the findings of Lin et al., who demonstrated in resectable pancreatic carcinoma that the 5-year survival rates in patients without PALN metastasis were 22.9%, while in those with PALN metastasis, it was 0% [29].
Kim et al. conducted an extensive analysis focusing on treatment response, unveiling that patients harboring metastatic PALN who underwent postoperative chemotherapy exhibited substantially augmented disease-specific survival (DFS) rates (p = 0.0003) [27]. This finding resonates with the study by Sho et al., where a multivariate analysis conducted on patients with PALN metastasis unveiled that adjuvant chemotherapy and the number of metastatic PALNs were significantly correlated with long-term survival. These results underscore the important role of adjuvant chemotherapy in mitigating disease progression and improving long-term survival outcomes in patients with metastatic para-aortic lymph nodes [38].
In concordance, Schwarz et al. demonstrated that DFS in patients with and without the involvement of PALN on frozen section examination was 5.6 vs. 12.9 months, respectively (p = 0.041), and 8.4 vs. 12.9 months (p = 0.038) for hematoxylin and eosin analysis [39]. However, in their meta-analysis, Paiella et al. confirmed that the impact of positive PALN on outcome might be more accurately assessed through DFS, owing to the necessity of robust studies that have thoroughly examined this association [30].
7. Pancreatic Cancer from the Present to the Future
Currently, no established diagnostic tools or screening methodologies are employed in clinical practice for pancreatic cancer detection. Consequently, there is a pressing need to explore risk factors, preclinical indicators, and surveillance strategies to enable early detection, an ongoing focus of research endeavors [43]. Nevertheless, screening asymptomatic individuals for pancreatic cancer currently poses challenges, given the propensity for false positive results and associated risks that may outweigh potential benefits. The use of detection of precise preoperative detection of pancreatic LNM can be a massive improvement in predicting the prognosis of these patients.
The clinical relevance of novel markers in para-aortic lymph nodes (PALN) lies in their potential to enhance diagnostic accuracy and treatment strategies for patients with resectable PDAC. By selectively harvesting PALN samples from PDAC patients exhibiting elevated levels of these novel markers, clinicians can achieve a more precise staging of the disease, identifying micrometastases that might not be detectable through conventional imaging techniques. This targeted approach allows for a more tailored surgical plan, as the presence of cancer cells in the PALN could indicate a higher likelihood of systemic disease, potentially altering the decision to proceed with extensive resection [44,45,46]. Furthermore, novel marker identification in PALN can provide critical prognostic information, helping to stratify patients based on their risk and guide adjuvant therapy decisions. Ultimately, novel marker integration in the assessment of PALN can lead to improved personalized treatment, better management of the disease, and potentially enhanced survival outcomes for PDAC patients [47,48].
Despite the promise of cancer biomarkers and the utilization of ‘omics’ technologies (such as genomics, transcriptomics, and metabolomics), their clinical translation remains elusive. Some associations of cancer biomarkers with pancreatic lymph node metastases have been studied over the last few decades; some examples are the Homing cell adhesion molecule (CD44) [49], Prominin-1 (CD133) [50], Bicaudal-C (BICC1) [51], Mothers against decapentaplegic homolog 4 (SMAD4) [52], Vascular endothelial growth factor D (VEGF-D) [53], M2-polarized tumor-associated macrophage (M2-TAM) [54], and Carbohydrate antigen sialyl Lewis A (CA19-9) [55], which can represent an important improvement in the management of pancreatic cancer.
Moreover, obtaining biopsies or tissue samples practice at the time of diagnosis in research settings undermines the utility of time-sensitive biomarkers for identifying preclinical, asymptomatic, yet surgically treatable cancers. Embracing novel technologies will be crucial in achieving early diagnosis, with emerging evidence from image-based radiomics, artificial intelligence, and machine learning offering promising avenues for enhanced detection capabilities [24,34,35,56,57].
8. Conclusions
In our study, we have delved deeply into the anatomical complexities essential for understanding pancreatic cancer. Our review underscored the intricate structures surrounding the pancreas that hinder precise clinicopathological diagnoses and promote the metastatic cascade, complicating therapeutic decisions and rendering prognosis predictions more uncertain. Furthermore, we have emphasized the critical role of the pancreatic lymphatic system in the spread of cancer, particularly through a detailed examination of its anatomy. Our findings demonstrated how metastasis to the PALN serves as a significant prognostic factor, influencing survival outcomes. Our study stresses the importance of considering these anatomical and pathological factors in the clinical management of pancreatic cancer, suggesting that a more comprehensive approach to diagnosis and treatment could significantly improve patient prognosis and survival rates.
Author Contributions
Conceptualization, F.F.V.e.S.; methodology, F.F.V.e.S.; data curation, F.F.V.e.S.; writing—original draft preparation, F.F.V.e.S.; writing—review and editing, F.F.V.e.S.; visualization, M.E.P.-I., M.D.D. and A.B.; supervision, M.E.P.-I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef]
- Stoffel, E.M.; Brand, R.E.; Goggins, M. Pancreatic Cancer: Changing Epidemiology and New Approaches to Risk Assessment, Early Detection, and Prevention. Gastroenterology 2023, 164, 752–765. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.X.; Lin, Y.Y.; Zhao, C.F.; Chen, W.B.; Liu, Q.C.; Li, Q.W.; Gao, F. Pancreatic cancer: A review of epidemiology, trend, and risk factors. World J. Gastroenterol. 2021, 27, 4298–4321. [Google Scholar] [CrossRef]
- Ilic, I.; Ilic, M. International patterns in incidence and mortality trends of pancreatic cancer in the last three decades: A joinpoint regression analysis. World J. Gastroenterol. 2022, 28, 4698–4715. [Google Scholar] [CrossRef]
- Covantsev, S.; Chicu, C.; Mazuruc, N.; Belic, O. Pancreatic ductal anatomy: More than meets the eye. Surg. Radiol. Anat. SRA 2022, 44, 1231–1238. [Google Scholar] [CrossRef]
- Mastracci, T.L.; Apte, M.; Amundadottir, L.T.; Alvarsson, A.; Artandi, S.; Bellin, M.D.; Bernal-Mizrachi, E.; Caicedo, A.; Campbell-Thompson, M.; Cruz-Monserrate, Z.; et al. Integrated Physiology of the Exocrine and Endocrine Compartments in Pancreatic Diseases: Workshop Proceedings. Pancreas 2022, 51, 1061–1073. [Google Scholar] [CrossRef]
- Torphy, R.J.; Fujiwara, Y.; Schulick, R.D. Pancreatic cancer treatment: Better, but a long way to go. Surg. Today 2020, 50, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Hezel, A.F.; Kimmelman, A.C.; Stanger, B.Z.; Bardeesy, N.; DePinho, R.A. Genetics and biology of pancreatic ductal adenocarcinoma. Genes Dev. 2006, 20, 1218–1249. [Google Scholar] [CrossRef] [PubMed]
- Tsvetkova, V.; Luchini, C. Mixed Neuroendocrine-Non-Neuroendocrine Neoplasms of the Pancreas. Surg. Pathol. Clin. 2022, 15, 555–563. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Burns, W.R.; Frankel, T.L.; Cho, C.S.; Nathan, H. Validation of the American Joint Commission on Cancer (AJCC) 8th Edition Staging System for Patients with Pancreatic Adenocarcinoma: A Surveillance, Epidemiology and End Results (SEER) Analysis. Ann. Surg. Oncol. 2017, 24, 2023–2030. [Google Scholar] [CrossRef]
- Kang, H.; Kim, S.S.; Sung, M.J.; Jo, J.H.; Lee, H.S.; Chung, M.J.; Park, J.Y.; Park, S.W.; Song, S.Y.; Park, M.S.; et al. Evaluation of the 8th Edition AJCC Staging System for the Clinical Staging of Pancreatic Cancer. Cancers 2022, 14, 4672. [Google Scholar] [CrossRef]
- Shin, D.W.; Kim, J. The American Joint Committee on Cancer 8th edition staging system for the pancreatic ductal adenocarcinoma: Is it better than the 7th edition? Hepatobiliary Surg. Nutr. 2020, 9, 98. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.C.; Itkin, M. Lymphatic Anatomy. Tech. Vasc. Interv. Radiol. 2016, 19, 247–254. [Google Scholar] [CrossRef]
- Swartz, M.A. The physiology of the lymphatic system. Adv. Drug Deliv. Rev. 2001, 50, 3–20. [Google Scholar] [CrossRef]
- Hu, D.; Li, L.; Li, S.; Wu, M.; Ge, N.; Cui, Y.; Lian, Z.; Song, J.; Chen, H. Lymphatic system identification, pathophysiology and therapy in the cardiovascular diseases. J. Mol. Cell. Cardiol. 2019, 133, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.; Komnick, M.R.; Brigleb, P.H.; Dermody, T.S.; Esterházy, D. Lymph node sharing between pancreas, gut, and liver leads to immune crosstalk and regulation of pancreatic autoimmunity. Immunity 2023, 56, 2070–2085. [Google Scholar] [CrossRef]
- Ps, L. Overview of the pancreas. Adv. Exp. Med. Biol. 2010, 690, 3–12. [Google Scholar] [CrossRef]
- Renard, Y.; de Mestier, L.; Perez, M.; Avisse, C.; Lévy, P.; Kianmanesh, R. Unraveling Pancreatic Segmentation. World J. Surg. 2018, 42, 1147–1153. [Google Scholar] [CrossRef]
- Fink, D.M.; Steele, M.M.; Hollingsworth, M.A. The lymphatic system and pancreatic cancer. Cancer Lett. 2016, 381, 217–236. [Google Scholar] [CrossRef] [PubMed]
- Cesmebasi, A.; Malefant, J.; Patel, S.D.; Plessis, M.D.; Renna, S.; Tubbs, R.S.; Loukas, M. The surgical anatomy of the lymphatic system of the pancreas. Clin. Anat. 2015, 28, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Ren, B.; Cui, M.; Yang, G.; Wang, H.; Feng, M.; You, L.; Zhao, Y. Tumor microenvironment participates in metastasis of pancreatic cancer. Mol. Cancer 2018, 17, 108. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Luo, G.; Liu, C.; Wu, C.; Liu, L.; Liu, Z.; Ni, Q.; Long, J.; Yu, X. Molecular mechanism underlying lymphatic metastasis in pancreatic cancer. BioMed Res. Int. 2014, 2014, 925845. [Google Scholar] [CrossRef] [PubMed]
- Keleg, S.; Büchler, P.; Ludwig, R.; Büchler, M.W.; Friess, H. Invasion and metastasis in pancreatic cancer. Mol. Cancer 2003, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, T.; Kobayashi, H.; Ueno, K.; Ohta, T.; Kayahara, M.; Mori, K.; Nakano, T.; Takeda, T.; Konishi, I.; Miyazaki, I. The pattern of lymph node involvement in carcinoma of the head of the pancreas—A histologic study of the surgical findings in patients undergoing extensive nodal dissections. Int. J. Pancreatol. 1993, 13, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Fodor, M.; Stättner, S. The Lymphatic System and Lymph Nodes of the Pancreas. In Textbook of Pancreatic Cancer; Søreid, K., Stättner, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2021; pp. 173–185. [Google Scholar] [CrossRef]
- Choi, S.H.; Kim, S.H.; Choi, J.J.; Kang, C.M.; Hwang, H.K.; Lee, W.J. Clinical necessity of the immunohistochemical reassessment of para-aortic lymph nodes in resected pancreatic ductal adenocarcinoma. Oncol. Lett. 2013, 6, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Blomstrand, H.; Olsson, H.; Green, H.; Björnsson, B.; Elander, N.O. Impact of resection margins and para-aortic lymph node metastases on recurrence patterns and prognosis in resectable pancreatic cancer—A long-term population-based cohort study. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2023, 25, 1531–1544. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Hwang, H.K.; Lee, W.J.; Kang, C.M. Unexpected Para-aortic Lymph Node Metastasis in Pancreatic Ductal Adenocarcinoma: A Contraindication to Resection? J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2020, 24, 2789–2799. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Yoon, Y.S.; Han, H.S.; Lee, J.S.; Na, H.Y.; Ahn, S.; Park, J.; Jung, K.; Jung, J.H.; Kim, J.; et al. Clinical Impact of Unexpected Para-Aortic Lymph Node Metastasis in Surgery for Resectable Pancreatic Cancer. Cancers 2021, 13, 4454. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.Y.; Zhang, X.M.; Kou, J.T.; Fa, H.; Zhang, X.X.; Dai, Y.; He, Q. Analysis of prognostic factors for pancreatic head cancer according to para-aortic lymph node. Cancer Med. 2016, 5, 2701–2707. [Google Scholar] [CrossRef]
- Paiella, S.; Sandini, M.; Gianotti, L.; Butturini, G.; Salvia, R.; Bassi, C. The prognostic impact of para-aortic lymph node metastasis in pancreatic cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2016, 42, 616–624. [Google Scholar] [CrossRef]
- Burk, K.S.; Lo, G.C.; Gee, M.S.; Sahani, D.V. Imaging and Screening of Pancreatic Cancer. Radiol. Clin. N. Am. 2017, 55, 1223–1234. [Google Scholar] [CrossRef] [PubMed]
- Yamada, D.; Kobayashi, S.; Takahashi, H.; Yoshioka, T.; Iwagami, Y.; Tomimaru, Y.; Shigekawa, M.; Akita, H.; Noda, T.; Asaoka, T.; et al. Pancreatic CT density is an optimal imaging biomarker for earlier detection of malignancy in the pancreas with intraductal papillary mucinous neoplasm. Pancreatology 2022, 22, 488–496. [Google Scholar] [CrossRef]
- O’Neill, E.; Hammond, N.; Miller, F.H. MR imaging of the pancreas. Radiol. Clin. N. Am. 2014, 52, 757–777. [Google Scholar] [CrossRef]
- Kobi, M.; Veillette, G.; Narurkar, R.; Sadowsky, D.; Paroder, V.; Shilagani, C.; Gilet, A.; Flusberg, M. Imaging and Management of Pancreatic Cancer. Semin. Ultrasound CT MR 2020, 41, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Xia, Y.; Yao, J.; Han, X.; Lambert, L.; Zhang, T.; Tang, W.; Jin, G.; Jiang, H.; Fang, X.; et al. Large-scale pancreatic cancer detection via non-contrast CT and deep learning. Nat. Med. 2023, 29, 3033–3043. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.N.; Goh, K.S.; Huang, C.R.; Chiang, T.C.; Lee, C.Y.; Jeng, Y.M.; Peng, S.J.; Chien, H.J.; Chung, M.H.; Chou, Y.H.; et al. Lymphatic vessel remodeling and invasion in pancreatic cancer progression. eBioMedicine 2019, 47, 98–113. [Google Scholar] [CrossRef] [PubMed]
- Ettrich, T.J.; Seufferlein, T. Systemic Therapy for Metastatic Pancreatic Cancer. Curr. Treat. Options Oncol. 2021, 22, 106. [Google Scholar] [CrossRef] [PubMed]
- Sho, M.; Murakami, Y.; Motoi, F.; Satoi, S.; Matsumoto, I.; Kawai, M.; Honda, G.; Uemura, K.; Yanagimoto, H.; Kurata, M.; et al. Postoperative prognosis of pancreatic cancer with para-aortic lymph node metastasis: A multicenter study on 822 patients. J. Gastroenterol. 2015, 50, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, L.; Lupinacci, R.M.; Svrcek, M.; Lesurtel, M.; Bubenheim, M.; Vuarnesson, H.; Balladur, P.; Paye, F. Para-aortic lymph node sampling in pancreatic head adenocarcinoma. Br. J. Surg. 2014, 101, 530–538. [Google Scholar] [CrossRef]
- Doi, R.; Kami, K.; Ito, D.; Fujimoto, K.; Kawaguchi, Y.; Wada, M.; Kogire, M.; Hosotani, R.; Imamura, M.; Uemoto, S. Prognostic implication of para-aortic lymph node metastasis in resectable pancreatic cancer. World J. Surg. 2007, 31, 147–154. [Google Scholar] [CrossRef]
- Sperti, C.; Gruppo, M.; Valmasoni, M.; Pozza, G.; Passuello, N.; Beltrame, V.; Moletta, L.; Blandamura, S. Para-aortic node involvement is not an independent predictor of survival after resection for pancreatic cancer. World J. Gastroenterol. 2017, 23, 4399–4406. [Google Scholar] [CrossRef] [PubMed]
- Hempel, S.; Plodeck, V.; Mierke, F.; Distler, M.; Aust, D.E.; Saeger, H.D.; Weitz, J.; Welsch, T. Para-aortic lymph node metastases in pancreatic cancer should not be considered a watershed for curative resection. Sci. Rep. 2017, 7, 7688. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lu, Y.; Luo, G.; Cheng, H.; Guo, M.; Liu, Z.; Xu, J.; Long, J.; Liu, L.; Fu, D.; et al. Which patients with para-aortic lymph node (LN16) metastasis will truly benefit from curative pancreaticoduodenectomy for pancreatic head cancer? Oncotarget 2016, 7, 29177–29186. [Google Scholar] [CrossRef]
- Sillesen, M.; Hansen, C.P.; Burgdorf, S.K.; Dencker, E.E.; Krohn, P.S.; Gisela Kollbeck, S.L.; Stender, M.T.; Storkholm, J.H. Impact of para aortic lymph node removal on survival following resection for pancreatic adenocarcinoma. BMC Surg. 2023, 23, 214. [Google Scholar] [CrossRef]
- Van Wijk, L.; De Klein, G.W.; Kanters, M.A.; Patijn, G.A.; Klaase, J.M. The ultimate preoperative C-reactive protein-to-albumin ratio is a prognostic factor for survival after pancreatic cancer resection. Eur. J. Med. Res. 2020, 25, 46. [Google Scholar] [CrossRef]
- Eskander, M.F.; de Geus, S.W.L.; Kasumova, G.G.; Ng, S.C.; Al-Refaie, W.; Ayata, G.; Tseng, J.F. Evolution and impact of lymph node dissection during pancreaticoduodenectomy for pancreatic cancer. Surgery 2017, 161, 968–976. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.J.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Endo, Y.; Kitago, M.; Kitagawa, Y. Evidence and Future Perspectives for Neoadjuvant Therapy for Resectable and Borderline Resectable Pancreatic Cancer: A Scoping Review. Cancers 2024, 16, 1632. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wu, T.; Lu, D.; Zhen, J.; Zhang, L. CD44 overexpression related to lymph node metastasis and poor prognosis of pancreatic cancer. Int. J. Biol. Markers 2018, 33, 308–313. [Google Scholar] [CrossRef]
- Maeda, S.; Shinchi, H.; Kurahara, H.; Mataki, Y.; Maemura, K.; Sato, M.; Natsugoe, S.; Aikou, T.; Takao, S. CD133 expression is correlated with lymph node metastasis and vascular endothelial growth factor-C expression in pancreatic cancer. Br. J. Cancer 2008, 98, 1389–1397. [Google Scholar] [CrossRef]
- Meng, F.; Hua, S.; Chen, X.; Meng, N.; Lan, T. Lymph node metastasis related gene BICC1 promotes tumor progression by promoting EMT and immune infiltration in pancreatic cancer. BMC Med. Genom. 2023, 16, 263. [Google Scholar] [CrossRef] [PubMed]
- Izumi, S.; Nakamura, S.; Mano, S.; Akaki, S. Well differentiation and intact Smad4 expression are specific features of groove pancreatic ductal adenocarcinomas. Pancreas 2015, 44, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Fukasawa, M.; Korc, M. Vascular endothelial growth factor-trap suppresses tumorigenicity of multiple pancreatic cancer cell lines. Clin. Cancer Res. 2004, 10, 3327–3332. [Google Scholar] [CrossRef] [PubMed]
- Kurahara, H.; Takao, S.; Maemura, K.; Mataki, Y.; Kuwahata, T.; Maeda, K.; Sakoda, M.; Iino, S.; Ishigami, S.; Ueno, S.; et al. M2-polarized tumor-associated macrophage infiltration of regional lymph nodes is associated with nodal lymphangiogenesis and occult nodal involvement in pN0 pancreatic cancer. Pancreas 2013, 42, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Asaoka, T.; Miyamoto, A.; Maeda, S.; Hama, N.; Tsujie, M.; Ikeda, M.; Sekimoto, M.; Nakamori, S. CA19-9 level determines therapeutic modality in pancreatic cancer patients with para-aortic lymph node metastasis. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 75–80. [Google Scholar] [CrossRef]
- Søreide, K.; Ismail, W.; Roalsø, M.; Ghotbi, J.; Zaharia, C. Early Diagnosis of Pancreatic Cancer: Clinical Premonitions, Timely Precursor Detection and Increased Curative-Intent Surgery. Cancer Control J. Moffitt Cancer Cent. 2023, 30. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).