
Prevalence and Risk Factors of Human Taenia solium Cysticercosis in Mbulu District, Northern Tanzania


 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Area
2.2. Study Design
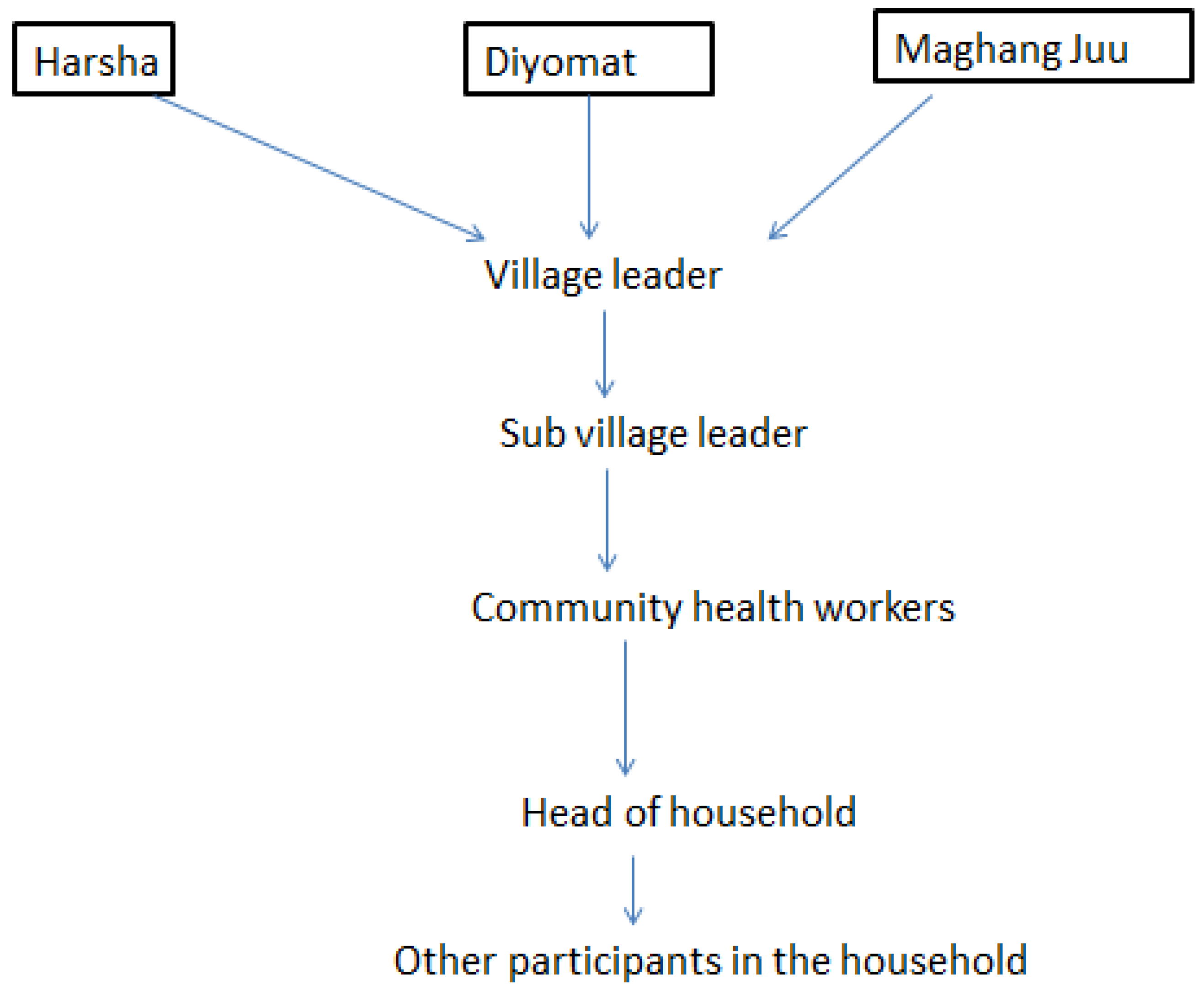
2.3. Household and Participant Selection
2.4. Data Collection
2.4.1. Questionnaire and Observational Check List
2.4.2. Sample Collection
2.4.3. ELISA Method
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
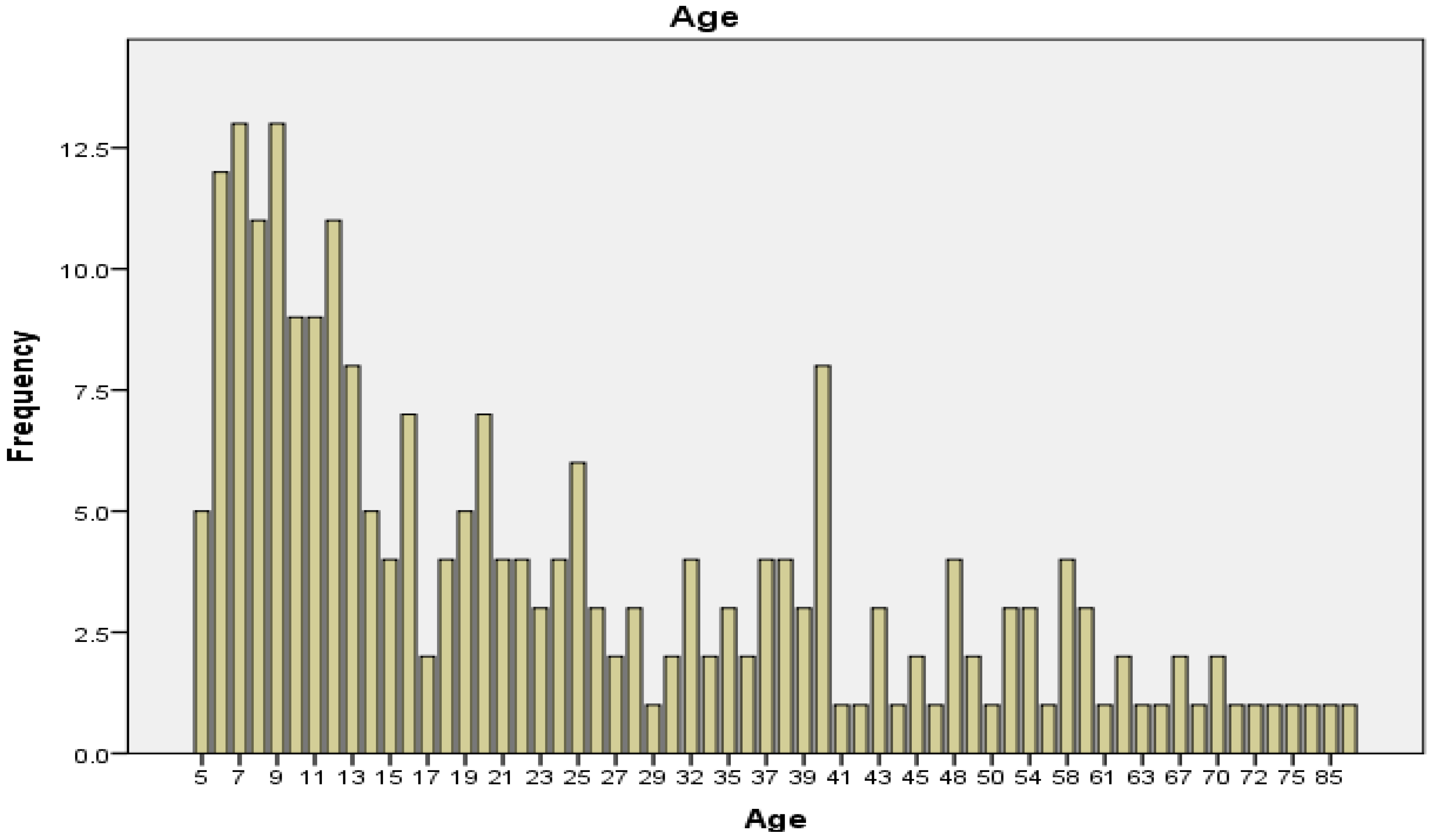
3.1. Demographic Characteristics
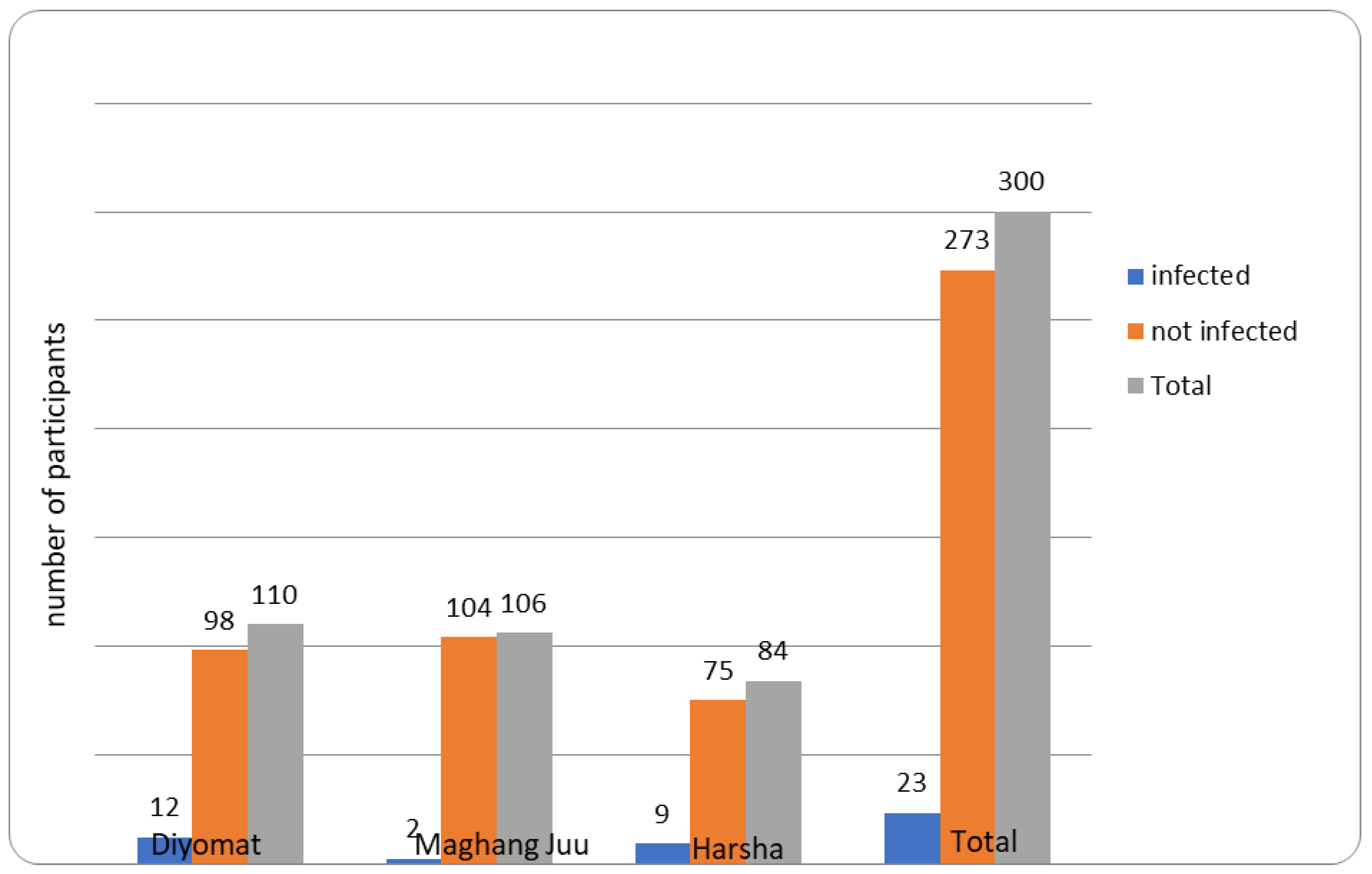
3.2. Prevalence of Cysticercosis
3.3. Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ELISA | Enzyme-linked Immunosorbent Assay |
| NCC | Neurocysticercosis |
| NIMR | National Institute for Medical Research |
| OD | Optical density |
| SPSS | Statistical Package for Social Sciences |
| WHO | World Health Organisation |
References
- Ito, A.; Wandra, T.; Li, T.; Dekumyoy, P.; Nkouawa, A.; Okamoto, M.; Budke, C. The Present Situation of Human Taeniases and Cysticercosis in Asia. Recent Pat. Anti-Infect. Drug Discov. 2015, 9, 173–185. [Google Scholar] [CrossRef]
- Mata, D.E.; Craig, S.; Mencos, F. Epidemiology of Taenia solium taeniosis and in two rural Guatemalan communities. Am. J. Trop. Med. Hyg. 1996, 55, 282–289. [Google Scholar]
- Galán-Puchades, M.T. Taeniosis vs cysticercosis infection routes. Asian Pac. J. Trop. Med. 2016, 9, 619–620. [Google Scholar] [CrossRef]
- Okello, A.L.; Thomas, L.F. Human taeniosis: Current insights into prevention and management strategies in endemic countries. Risk Manag. Healthc. Policy 2017, 10, 107–116. [Google Scholar] [CrossRef]
- Mahanty, S.; Garcia, H.H. Cysticercosis and neurocysticercosis as pathogens affecting the nervous system. Prog. Neurobiol. 2010, 91, 172–184. [Google Scholar] [CrossRef]
- Yancey, L.S.; Diaz-Marchan, P.J.; White, A.C. Cysticercosis: Recent advances in diagnosis and management of neurocysticercosis. Curr. Infect. Dis. Rep. 2005, 7, 39–47. [Google Scholar] [CrossRef]
- Del Brutto, O.H. Neurocysticercosis. Handb. Clin. Neurol. 2014, 121, 1445–1459. [Google Scholar] [CrossRef]
- Montano, S.M.; Villaran, M.V.; Ylquimiche, L.; Figueroa, J.J.; Rodriguez, S.; Bautista, C.T.; Gonzalez, A.E.; Tsang, V.C.W.; Gilman, R.H.; Garcia, H.H. Neurocysticercosis: Association between seizures, serology, and brain CT in rural Peru. Neurology 2005, 65, 229–234. [Google Scholar] [CrossRef]
- Shukla, N.; Husain, N.; Venkatesh, V.; Masood, J.; Husain, M. Seroprevalence of cysticercosis in North Indian population. Asian Pac. J. Trop. Med. 2010, 3, 589–593. [Google Scholar] [CrossRef]
- Rojas, R.G.; Patiño, F.; Pérez, J.; Medina, C.; Lares, M.; Méndez, C.; Aular, J.; Parkhouse RM, E.; Cortéz, M.M. Transmission of porcine cysticercosis in the Portuguesa state of Venezuela. Trop. Anim. Health Prod. 2019, 51, 165–169. [Google Scholar] [CrossRef]
- Mwape, K.E.; Phiri, I.K.; Praet, N.; Speybroeck, N.; Muma, J.B.; Dorny, P.; Gabriël, S. The Incidence of Human Cysticercosis in a Rural Community of Eastern Zambia. PLoS Neglected Trop. Dis. 2013, 7, e0002142. [Google Scholar] [CrossRef] [PubMed]
- Torgerson, P.R.; Devleesschauwer, B.; Praet, N.; Speybroeck, N.; Willingham, A.L.; Kasuga, F.; Rokni, M.B.; Zhou, X.N.; Fèvre, E.M.; Sripa, B.; et al. World Health Organization Estimates of the Global and Regional Disease Burden of 11 Foodborne Parasitic Diseases, 2010: A Data Synthesis. PLoS Med. 2015, 12, e1001920. [Google Scholar] [CrossRef] [PubMed]
- Torgerson, P.R.; Macpherson, C.N.L. Veterinary Parasitology The socioeconomic burden of parasitic zoonoses: Global trends. Vet. Parasitol. 2011, 182, 79–95. [Google Scholar] [CrossRef] [PubMed]
- Gulelat, Y.; Eguale, T.; Kebede, N.; Aleme, H.; Fèvre, E.M. Epidemiology of Porcine Cysticercosis in Eastern and Southern Africa: Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 836177. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, C.; Devleesschauwer, B.; Schmidt, V.; Winkler, A.S.; Harrison, W.; Johansen, M.V. The societal cost of Taenia solium cysticercosis in Tanzania. Acta Trop. 2017, 165, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Braae, U.C.; Saarnak, C.F.L.; Mukaratirwa, S.; Devleesschauwer, B.; Magnussen, P.; Johansen, M.V. Taenia solium taeniosis/cysticercosis and the co-distribution with schistosomiasis in Africa. Parasites Vectors 2015, 8, 323. [Google Scholar] [CrossRef]
- Winkler, A.S. Neurocysticercosis in sub-Saharan Africa: A review of prevalence, clinical characteristics, diagnosis, and management. Pathog. Glob. Health 2012, 106, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Mwang’onde, B.; Nkwengulila, G.; Chacha, M. The Serological Survey for Human Cysticercosis Prevalence in Mbulu District, Tanzania. Adv. Infect. Dis. 2012, 2, 62–66. [Google Scholar] [CrossRef]
- Mwanjali, G.; Kihamia, C.; Kakoko DV, C.; Lekule, F.; Ngowi, H.; Johansen, M.V.; Thamsborg, S.M.; Willingham, A.L. Prevalence and Risk Factors Associated with Human Taenia solium Infections in Mbozi District, Mbeya Region, Tanzania. PLoS Neglected Trop. Dis. 2013, 7, e0002102. [Google Scholar] [CrossRef] [PubMed]
- Mwita, C.J.; Yohana, C.; Nkwengulila, G. The Prevalence of Porcine Cysticercosis and Risk Factors for Taeniosis in Iringa Rural District. Int. J. Anim. Vet. Adv. 2013, 5, 251–255. [Google Scholar]
- Kabululu, M.L.; Ngowi, H.A.; Mlangwa, J.E.D.; Mkupasi, E.M.; Braae, U.C.; Trevisan, C.; Colston, A.; Cordel, C.; Johansen, M.V. Endemicity of Taenia solium cysticercosis in pigs from Mbeya Rural and Mbozi districts, Tanzania. BMC Vet. Res. 2020, 16, 325. [Google Scholar] [CrossRef] [PubMed]
- Ngowi, H.; Kassuku, A.; Maeda, G.E.; Boa, M.; Carabin, H.; Willingham, A. Risk factors for the prevalence of porcine cysticercosis in Mbulu District, Tanzania. Vet. Parasitol. 2004, 120, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Pondja, A.; Neves, L.; Mlangwa, J.; Afonso, S.; Fafetine, J.; Willingham, A.L.; Thamsborg, S.M.; Johansen, M.V. Prevalence and risk factors of porcine cysticercosis in Angónia District, Mozambique. PLoS Neglected Trop. Dis. 2010, 4, e0000594. [Google Scholar] [CrossRef] [PubMed]
- Kabululu, M.L.; Johansen, M.V.; Lightowlers, M.; Trevisan, C.; Braae, U.C.; Ngowi, H.A. Aggregation of Taenia solium cysticerci in pigs: Implications for transmission and control. Parasite Epidemiol. Control 2023, 22, e00307. [Google Scholar] [CrossRef] [PubMed]
- Guideline for Preventive Chemotherapy for the Control of Taenia solium Taeniosis; Pan American Health Organization: Washington, DC, USA, 2021. [CrossRef]
- World Bank. Guidelines for School-Based Deworming Programs: Information for Policy-Makers and Planners on Conducting Deworming as Part of an Integrated School Health Program; Partnership for Child Development: London, UK, 2018. [Google Scholar]
- CDC. One Health Zoonotic Disease Prioritization for Multi-Sectoral Engagement in Tanzania; CDC: Atlanta, GA, USA, 2017; pp. 1–24. Available online: https://www.cdc.gov/onehealth/pdfs/uganda-one-health-zoonotic-disease-prioritization-report-508.pdf (accessed on 6 December 2019).
- WHO-World Bank. School Deworming. 2003. Available online: https://www.who.int/publications/i/item/School-deworming-at-a-glance-2003 (accessed on 10 October 2019).
- National Bureau of Statistics; Office of Chief Government Statistician. 2012 Population and Housing Survey. Population Distribution by Administrative Areas—United Republic of Tanzania. 2013. Available online: https://www.nbs.go.tz/index.php/en/census-surveys/population-and-housing-census/162-2012-phcpopulation-distribution-by-administrative-areas (accessed on 6 December 2019).
- DPLO. Mbulu District Council Strategic Plan; 2015; Volume 3, pp. 1–6. Available online: https://mbuludc.go.tz/storage/app/uploads/public/59a/7f0/862/59a7f086212e0202562801.pdf (accessed on 5 May 2018).
- Mwang’onde, B.J.; Chacha, M.J.; Nkwengulila, G. The status and health burden of neurocysticercosis in Mbulu district, northern Tanzania. BMC Res. Notes 2018, 11, 890. [Google Scholar] [CrossRef] [PubMed]
- Rotondi, M.; Donner, A. Sample size estimation in cluster randomized trials: An evidence-based perspective. Comput. Stat. Data Anal. 2012, 56, 1174–1187. [Google Scholar] [CrossRef]
- ApDia. In Vitro Diagnostic Kit Cysticercosis Ag ELISA. 2004. Available online: https://apdiagroup.com/wp-content/uploads/2020/03/650501-IFU-Cysticercosis-Ag-ELISA-96T-vs10-2018.pdf (accessed on 6 December 2019).
- Segala, F.V.; De Vita, E.; Amone, J.; Ongaro, D.; Nassali, R.; Oceng, B.; Okori, S.; Putoto, G.; Lochoro, P.; Ictho, J.; et al. Neurocysticercosis in Low-and Middle-Income Countries, a Diagnostic Challenge from Oyam District, Uganda. Infect. Dis. Rep. 2022, 14, 505–508. [Google Scholar]
- Hossain, M.S.; Shabir, S.; Toye, P.; Thomas, L.F.; Falcone, F.H. Insights into the diagnosis, vaccines, and control of Taenia solium, a zoonotic, neglected parasite. Parasites Vectors 2023, 16, 380. [Google Scholar] [CrossRef] [PubMed]
- García-Díez, J.; Saraiva, S.; Moura, D.; Grispoldi, L.; Cenci-Goga, B.T.; Saraiva, C. The Importance of the Slaughterhouse in Surveilling Animal and Public Health: A Systematic Review. Vet. Sci. 2023, 10, 1–42. [Google Scholar]
- Kabululu, M.L.; Ogunro, B.N.; Ngowi, H.A. Spatial and Temporal Changes in Taenia solium Cysticercosis Seroprevalence among Pigs in the Southern Highlands of Tanzania. Vet. Med. Int. 2024, 2024, 7261324. [Google Scholar] [CrossRef]
- Carabin, H.; Millogo, A.; Ngowi, H.A.; Bauer, C.; Dermauw, V.; Koné, A.C.; Sahlu, I.; Salvator, A.L.; Preux, P.M.; Somé, T.; et al. Effectiveness of a community-based educational programme in reducing the cumulative incidence and prevalence of human Taenia solium cysticercosis in Burkina Faso in 2011–14 (EFECAB): A cluster-randomised controlled trial. Lancet Glob. Health 2018, 6, e411–e425. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.M.; Mohan, V.R.; Muliyil, J.; Dorny, P.; Rajshekhar, V. Changes in knowledge and practices related to taeniosis/cysticercosis after health education in a south Indian community. Int. Health 2012, 4, 164–169. [Google Scholar] [CrossRef] [PubMed]
- World Bank. National Education Profile: Tanzania 2018 Update; Education Policy and Data Center: Washington, DC, USA, 2018; Available online: https://www.epdc.org/sites/default/files/documents/EPDC_NEP_2018_Tanzania.pdf (accessed on 8 February 2024).
- Shonyela, S.M.; Mkupasi, E.M.; Sikalizyo, S.C.; Kabemba, E.M.; Ngowi, H.A.; Phiri, I. An epidemiological survey of porcine cysticercosis in Nyasa District, Ruvuma Region, Tanzania. Parasite Epidemiol. Control 2017, 2, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Cysticercosis Ag ELISA REF 650505. Available online: https://apdiagroup.com/we-sell/elisa/elisa-apdia/cysticercosis-antigen (accessed on 14 March 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Village | |||||
|---|---|---|---|---|---|
| Variable | Total N (%) | Harsha A (%) | Maghang Juu B (%) | Diyomat C (%) | |
| Sex | Male | 155 (51.7) | 43 (51.1) | 66 (62.2) | 46 (41.8) |
| Female | 145 (48.3) | 41 (48.8) | 40 (37.7) | 64 (58.1) | |
| 5–15 | 104 (34.7) | 32 (30.7) | 36 (36.6) | 36 (36.6) | |
| Age | 16–25 | 51 (17.0) | 11 (21.5) | 14 (27.4) | 26 (50.9) |
| 26–35 | 51 (17.0) | 8 (15.7) | 18 (35.3) | 25 (49.0) | |
| 36–45 | 43 (14.3) | 14 (32.5) | 15 (34.9) | 13 (30.2) | |
| >45 | 51 (17.0) | 19 (37.2) | 22 (43.1) | 10 (2.1) | |
| Primary | 261 (87.0) | 107 (41.5) | 79 (30.6) | 75 (29.1) | |
| Education | Secondary | 12 (4.0) | 2 (2.4) | 9 (10.9) | 1 (1.2) |
| Tertiary | 5 (1.7) | 1 (20) | 4 (80) | 0 (0) | |
| None | 22 (7.3) | 0 (0) | 14 (63.6) | 8 (36.3) | |
| Occupation | Students | 96 (32.0) | 30 (31.2) | 34 (35.4) | 32 (33.3) |
| Farmer | 204 (68.0) | 54 (26.5) | 72 (35.3) | 78 (38.2) | |
| Total | 300 (100) | 84 (28) | 106 (35.3) | 110 (36.7) | |
| Variable | Total (n) | Positive p (%) | Negative N (%) | OR (95% CI) | p Value | |
|---|---|---|---|---|---|---|
| Sex | Male | 145 | 12 (8.27) | 133 (91.72) | 1.18 (0.50–2.77) | 0.702 |
| Female | 155 | 11 (7.09) | 144 (92.90) | Ref | ||
| Age | 5–15 | 104 | 5 (4.80) | 99 (95.19) | Ref | |
| 16–25 | 51 | 2 (3.92) | 49 (96.07) | 0.81 (0.15–4.32 | 0.803 | |
| 26–35 | 51 | 6 (11.76) | 45 (88.23) | 2.64 (0.77–9.11) | 0.124 | |
| 36–45 | 43 | 4 (9.30) | 39 (90.69) | 2.03 (0.52–7.96) | 0.309 | |
| 46 and above | 51 | 6 (11.76) | 45 (88.23) | 2.64 (0.77–9.11) | 0.124 | |
| Education level | Primary | 261 | 23 (8.8) | 238 (91.1) | 4.43 (0.2675.46) | 0.303 |
| Secondary | 12 | 0 (0) | 12 (100) | 1.8 (0.03–96.37) | 0.772 | |
| Tertiary | 5 | 0 (0) | 5 (100) | 4.09 (0.07–230) | 0.493 | |
| None | 22 | 0 (0) | 22 (100) | Ref | ||
| Village | Harsha | 84 | 9 (10.71) | 75 (89.28) | Ref | |
| Diyomat | 110 | 12 (10.90) | 98 (89.09) | 1.02 (0.41–2.55) | 0.965 | |
| Maghang Juu | 106 | 2 (1.88) | 104 (98.11) | 0.16(0.03–0.76) | 0.021 | |
| Occupation | Student | 96 | 5 (5.20) | 91 (94.79) | Ref | |
| Farmer | 204 | 18 (8.82) | 186 (91.17) | 1.76 (0.63–4.89) | 0.278 | |
| Total | 300 | 23 (7.67) | 277 (92.33) | |||
| Community | Household | Community Prevalence p (%) | Household and Community Risks for Cysticercosis | |||||
|---|---|---|---|---|---|---|---|---|
| Tap Water T (%) | Pond Water p (%) | River Water R (%) | Latrine L (%) | Keeping Pig K (%) | Odds Ratio (95%CI) | |||
| Diyomat | 34 | 12/110 (10.9) | 29 (85.3) | 3 (8.8) | 2 (5.9) | 24 (70.6) | 26 (76.5) | Reference |
| Maghang Juu | 22 | 2/106 (1.88) | 12 (54.5) | 0 (0) | 10 (45.5) | 11 (50.0) | 17 (77.3) | 3.8824 (0.7916–19.0407 |
| Harsha | 33 | 9/84 (10.71) | 0 (0) | 0 (0) | 33 (100) | 8 (24.3) | 26 (78.8) | 0.8889 (0.3209–2.4622) |
| Total | 89 | 23/300 (7.67) | 41/89 (46.1) | 3/89 (3.3) | 45/89 (50.6) | 43/89 (48.3) | 69/89 (77.5) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandi, V.; Ngowi, B.; Mpolya, E.; Kilale, A.M.; Vianney, J.-M. Prevalence and Risk Factors of Human Taenia solium Cysticercosis in Mbulu District, Northern Tanzania. Zoonotic Dis. 2024, 4, 135-145. https://doi.org/10.3390/zoonoticdis4020013
Bandi V, Ngowi B, Mpolya E, Kilale AM, Vianney J-M. Prevalence and Risk Factors of Human Taenia solium Cysticercosis in Mbulu District, Northern Tanzania. Zoonotic Diseases. 2024; 4(2):135-145. https://doi.org/10.3390/zoonoticdis4020013
Chicago/Turabian StyleBandi, Vedasto, Bernard Ngowi, Emmanuel Mpolya, Andrew Martin Kilale, and John-Mary Vianney. 2024. "Prevalence and Risk Factors of Human Taenia solium Cysticercosis in Mbulu District, Northern Tanzania" Zoonotic Diseases 4, no. 2: 135-145. https://doi.org/10.3390/zoonoticdis4020013
APA StyleBandi, V., Ngowi, B., Mpolya, E., Kilale, A. M., & Vianney, J.-M. (2024). Prevalence and Risk Factors of Human Taenia solium Cysticercosis in Mbulu District, Northern Tanzania. Zoonotic Diseases, 4(2), 135-145. https://doi.org/10.3390/zoonoticdis4020013