

Basis for a One Health Approach—Inventory of Routine Data Collections on Zoonotic Diseases in Lower Saxony, Germany

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Concept of the Study and Collaborating Partners
2.2. Identification and Selection of Data Collections and Pathogens
2.3. Collection of Metadata on Data Collections and Pathogens
3. Results
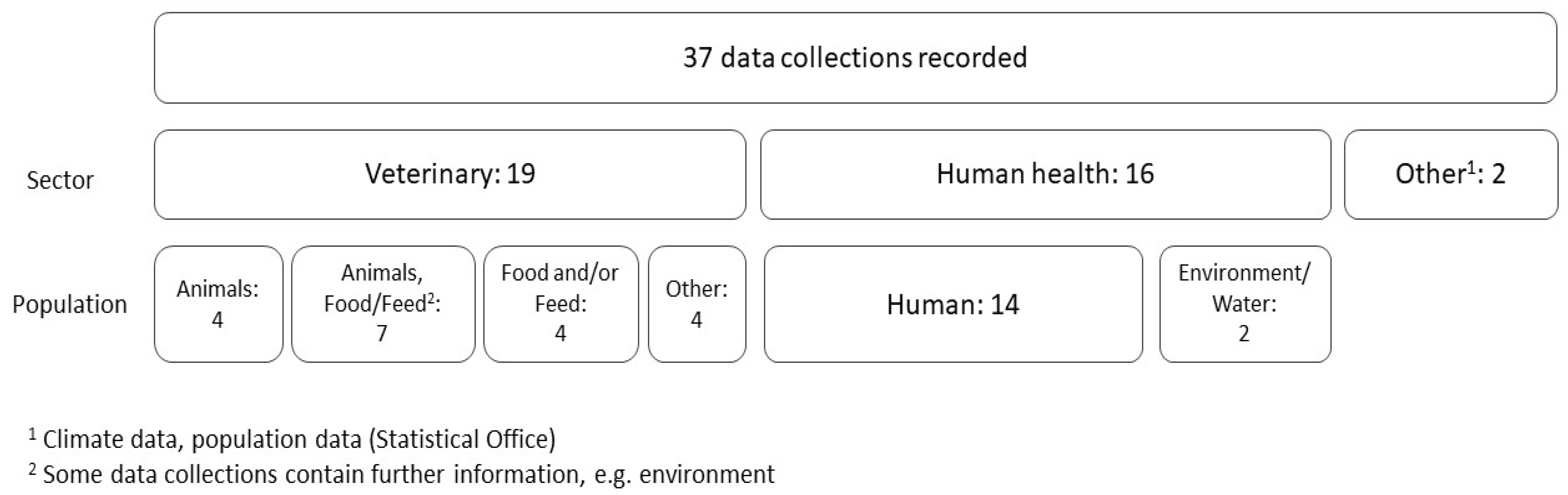
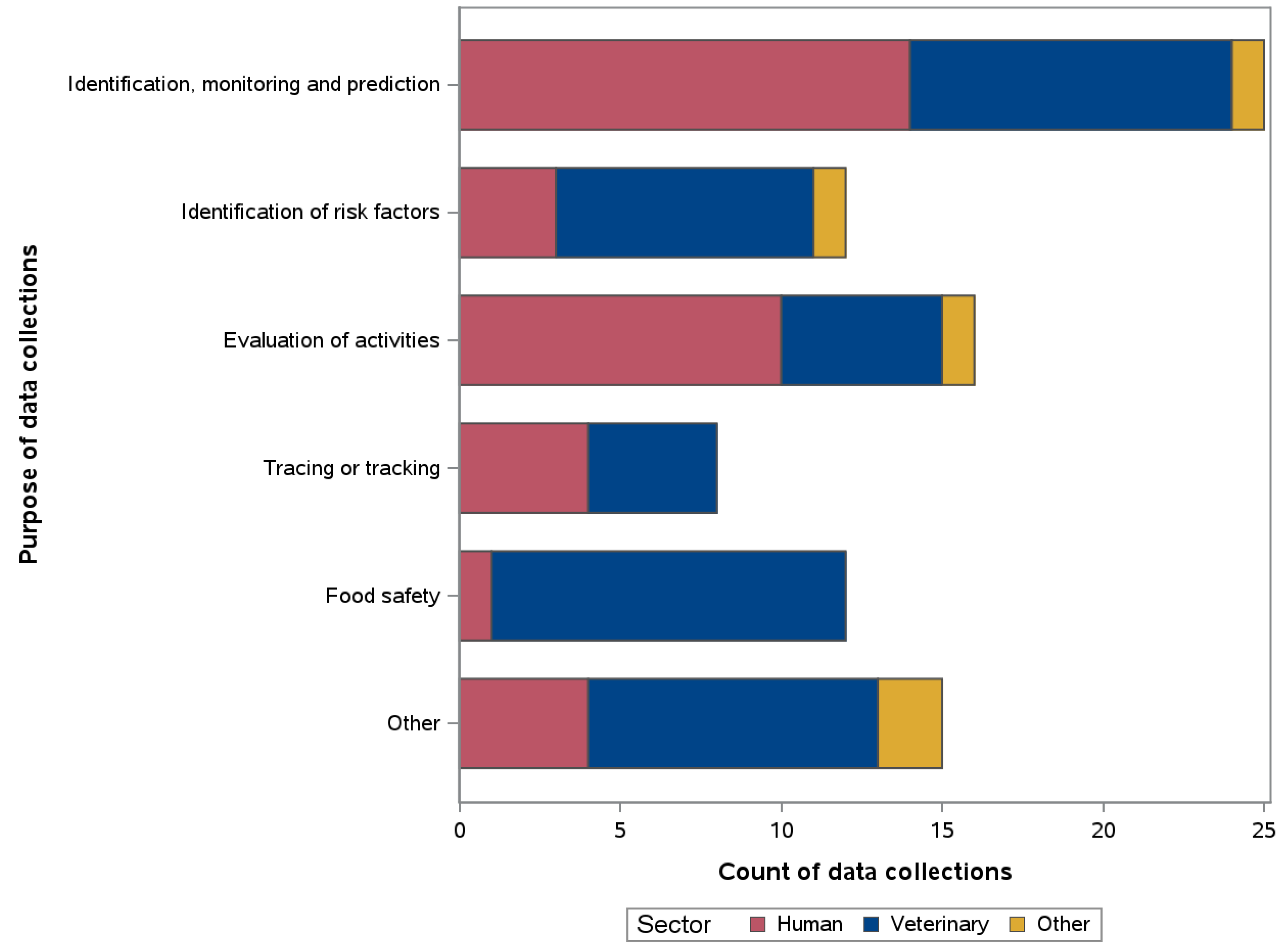
3.1. Metadata of Data Collections
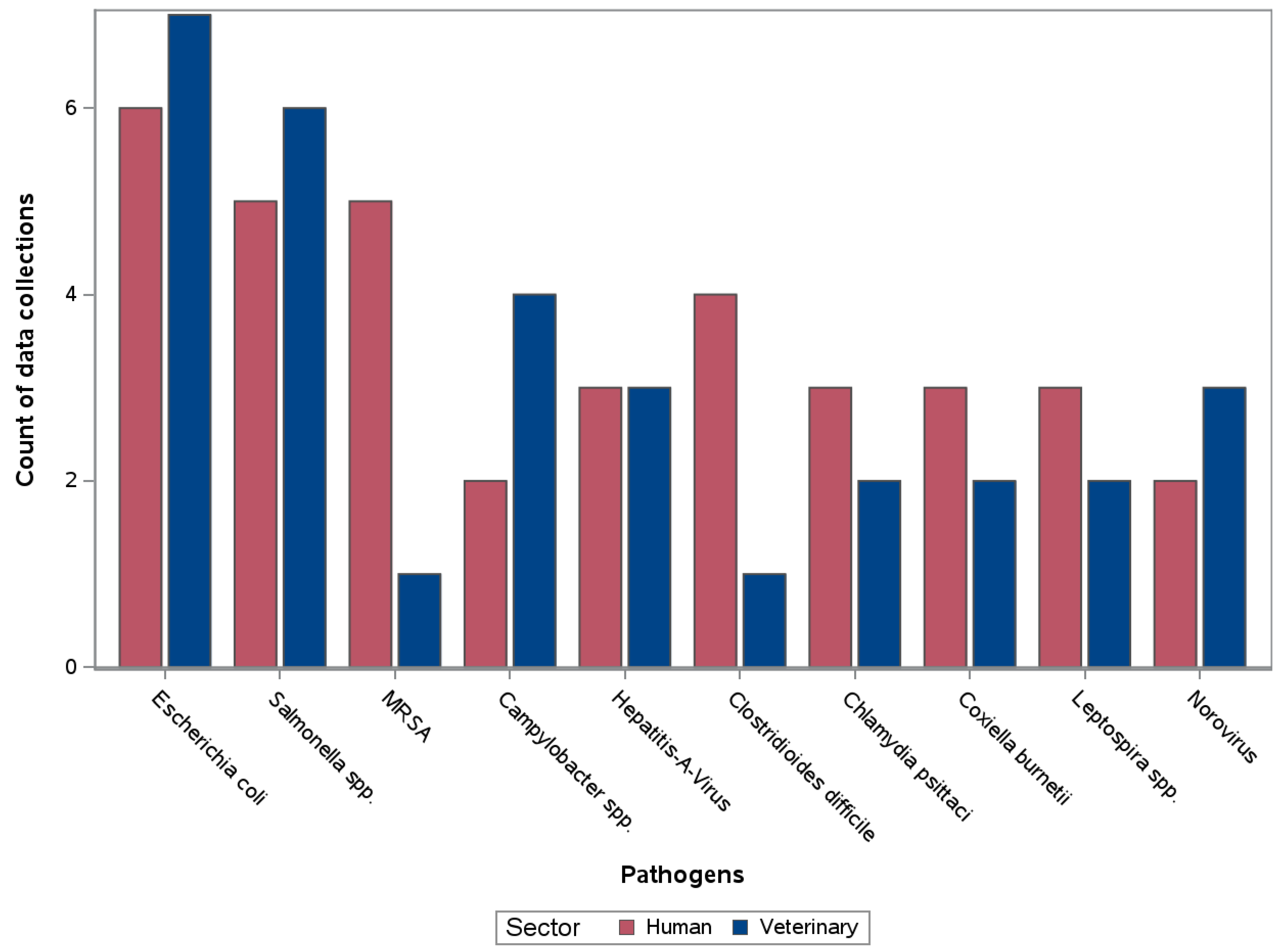
3.2. Metadata of Pathogens
4. Discussion
4.1. Strategies for a One Health MOSS and Inventory of the Existing Routine Data Collections
4.2. International One Health MOSS
4.3. Considerations for Cross-Sector One Health Data Curation
- Data-related
- Data structure and level of aggregation: i.e., the level of spatial and temporal aggregation has to be harmonised;
- Nomenclature and formats: i.e., catalogues and definitions have to be harmonised with easy to follow rules;
- Completeness and data quality: i.e., according to the use cases addressed, variables under study have to be selected, the number of missing values has to be calculated and data quality rules have to be addressed;
- Level of differentiation of pathogens: i.e., the available/needed level, e.g., genus, species, subspecies, genes, needs to be considered/harmonised.
- Content-related
- Purpose of data collection: e.g., to improve knowledge and monitoring purposes, food safety;
- Type of data collection sampling: e.g., monitoring, surveillance, active or passive systems.
- Data privacy-related
- Re-Identification: i.e., individual plants or people must not be identifiable. Therefore, access to the highest possible spatial resolution may be denied.
- Purpose of data use: i.e., for legal data protection assessments, the purpose of data use must be precisely defined.
- Technical-related
- Implementation of data exchange: e.g., via individual exports, data-interfaces or a data warehouse. Most data collections are stand-alone solutions, which were developed for a specific purpose and have grown historically. This makes it difficult to use these systems for other purposes.
- Development of analysis procedures: e.g., control charts/Shewart charts, time series analysis and expected values derived therefrom.
- Personal-related
- Experts for the original data: i.e., due to the variety of data and types of documentation, experts in each data collection are needed to explain and interpret the data.
- Statistical-, data management-, and IT-experts: i.e., to develop analysis procedures and to implement data transfer and management.
- Personal contacts between the sectors and other stakeholders: i.e., intersectoral exchange is essential to build a One Heath MOSS, e.g., via regular meetings or joint workshops.
5. Conclusions and Outlook
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Connect OHD: | Connect One Health Data |
| LAVES: | Lower Saxony State Office for Consumer Protection and Food Safety, Germany (Niedersächsisches Landesamt für Verbraucherschutz und Lebensmittelsicherheit) |
| LIMS: | Laboratory information management system |
| MOSS: | Monitoring and surveillance system |
| NLGA: | Public Health Agency of Lower Saxony, Germany (Niedersächsisches Landesgesundheitsamt) |
| REDCap: | Research Electronic Data Capture |
| TiHo: | University for Veterinary Medicine Hannover, Foundation (Stiftung Tierärztliche Hochschule Hannover) |
References
- Palmer, S.R.; Soulsby, L.; Torgerson, P.; Brown, D.W.G. The global challenge of zoonoses control. In Oxford Textbook of Zoonoses: Biology, Clinical Practice, and Public Health Control; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Tissot-Dupont, H.; Raoult, D. Clinical Aspects, Diagnosis and Treatment of Q Fever: Rickettsial Diseases; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Robert Koch-Institut. Campylobacter-Enteritis; RKI-Ratgeber. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Merkblaetter/Ratgeber_Campylobacter.html;jsessionid=72441A0798DDA71F0BE17C306AB559F3.internet092#doc2374558bodyText2 (accessed on 21 November 2022).
- Leal Filho, W.; Ternova, L.; Parasnis, S.A.; Kovaleva, M.; Nagy, G.J. Climate Change and Zoonoses: A Review of Concepts, Definitions, and Bibliometrics. Int. J. Environ. Res. Public Health 2022, 19, 893. [Google Scholar] [CrossRef] [PubMed]
- Slingenbergh, J.; Gilbert, M.; de Balogh, K.I.; Wint, W. Ecological sources of zoonotic diseases. Rev. Sci. Tech. Off. Int. Épizooties 2004, 23, 467–484. [Google Scholar] [CrossRef] [PubMed]
- Mishra, J.; Mishra, P.; Arora, N.K. Linkages between environmental issues and zoonotic diseases: With reference to COVID-19 pandemic. Environ. Sustain. 2021, 4, 455–467. [Google Scholar] [CrossRef]
- Wendt, A.; Kreienbrock, L.; Campe, A. Zoonotic Disease Surveillance—Inventory of Systems Integrating Human and Animal Disease Information. Zoonoses Public Health 2015, 62, 61–74. [Google Scholar] [CrossRef]
- Wendt, A.; Kreienbrock, L.; Campe, A. Joint use of Disparate Data for the Surveillance of Zoonoses: A Feasibility Study for a One Health Approach in Germany. Zoonoses Public Health 2016, 63, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Friedrich-Loeffler-Institut. OHEJP Knowledge Base: Inventory on Surveillance Systems. Available online: https://shiny.fli.de/ife-apps/EJPOrion_WP2Epi/ (accessed on 13 July 2022).
- European Union EU. Directive 2003/99/EC of the European Parliament and of the Council of 17 November 2003 on the Monitoring of Zoonoses and Zoonotic Agents, Amending Council Decision 90/424/EEC and Repealing Council Directive 92/117/EEC; European Union: Brussels, Belgium, 2003. [Google Scholar]
- Narrod, C.; Zinsstag, J.; Tiongco, M. A one health framework for estimating the economic costs of zoonotic diseases on society. Ecohealth 2012, 9, 150–162. [Google Scholar] [CrossRef]
- Zinsstag, J.; Schelling, E.; Crump, L.; Whittaker, M.; Tanner, M.; Stephen, C. One Health: The Theory and Practice of Integrated Health Approaches, 2nd ed.; CAB International: Wallingford, UK, 2021. [Google Scholar]
- Landesamt für Statistik Niedersachsen. Bevölkerung und Katasterfläche in Niedersachsen (Gebietsstand: 1.11.2021); Tabelle A100001G; Landesamt für Statistik Niedersachsen: Hannover, Germany, 2022. (In German) [Google Scholar]
- Landesamt für Statistik Niedersachsen. Landwirtschaftliche Betriebe mit Viehhaltung und Viehbestand am 1. März in Niedersachsen; Tabelle Z6080020; Landesamt für Statistik Niedersachsen: Hannover, Germany, 2021. (In German) [Google Scholar]
- Landesamt für Statistik Niedersachsen. Landwirtschaftliche Betriebe mit Haltung von Sonstigem Geflügel und Bestand an Sonstigem Geflügel am 1. März in Niedersachsen; Tabelle Z6080026; Landesamt für Statistik Niedersachsen: Hannover, Germany, 2021. (In German) [Google Scholar]
- Landesamt für Statistik Niedersachsen. Landwirtschaftliche Betriebe mit Hühnerhaltung und Hühnerbestand am 1. März in Niedersachsen; Tabelle Z6080025; Landesamt für Statistik Niedersachsen: Hannover, Germany, 2021. (In German) [Google Scholar]
- Wendt, A. One Health Surveillance; Tierärztliche Hochschule: Hannover, Germany, 2016. (In German) [Google Scholar]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, R.L.; Anderson, W.; Anelich, L.; Cordier, J.L.; Dewanti-Hariyadi, R.; Ross, T.; Zwietering, M.H. Microorganisms in Foods 7: Microbiological Testing in Food Safety Management; Springer: Cham, Switzerland, 2018; p. 5. [Google Scholar]
- Ellis-Iversen, J.; Petersen, C.; Helwigh, B. One Health Integration in Surveillance—Inspiration and Ideas; Technical University of Denmark: Kongens Lyngby, Denmark, 2019; p. 17. [Google Scholar]
- Kreienbrock, L.; Pigeot, I.; Ahrens, W. Epidemiologische Methoden, 5th ed.; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Intemann, T.; Kaulke, K.; Kipker, D.-K.; Lettieri, V.; Stallmann, C.; Schmidt, C.O.; Geidel, L.; Bialke, M.; Hampf, C.; Stahl, D.; et al. White Paper—Verbesserung des Record Linkage für die Gesundheitsforschung in Deutschland. Fachrepositorium Leb. 2023, 1, 125. (In German) [Google Scholar] [CrossRef]
- Fluck, J.; Golebiewski, M.; Darms, J. Data Publication for Personalised Health Data: A New Publication Standard Introduced by NFDI4Health. In Proceedings of the Conference on Research Data Infrastructure, Karlsruhe, Germany, 12–14 September 2023. [Google Scholar]
- TMF. Technologie- und Methodenplattform für die Vernetzte Medizinische Forschung e.V. Deutsches Forschungsdatenportal für Gesundheit (FDPG). Available online: https://forschen-fuer-gesundheit.de/ (accessed on 1 December 2023).
- Wieler, L.; Antao, E.-M.; Semmler, T. Research on zoonoses: Central element of the “One Health” initiative. BMTW 2009, 122, 412–416. [Google Scholar]
- Rudolph, B.; Davis, R. Administrative Data and Disease Surveillance: An Integration Toolkit; National Association of Health Data Organizations: Provo, UT, USA, 2011. [Google Scholar]
- Förster, C.; Nordhoff, K.; Fritzemeier, J.; Breuer, J.; Kreienbrock, L. A Framework for Study Planning in Food Safety Investigations. Berl. Münchener Tierärztliche Wochenschr. 2022, 135, 1–10. [Google Scholar]
- El Idrissi, A.H.; Larfaoui, F.; Dhingra, M.; Johnson, A.; Pinto, J.; Sumption, K. Digital technologies and implications for Veterinary Services. Rev. Sci. Tech. 2021, 40, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Ganslandt, T. Perspektive Interoperabilität. In Proceedings of the TMF Jahreskongress 2023 Köln—Session 4: Panel Standardisierung & Datenqualität, Köln, Germany, 18–19 April 2023. (In German). [Google Scholar]
- Häsler, B.; Gilbert, W.; Jones, B.A.; Pfeiffer, D.U.; Rushton, J.; Otte, M.J. The Economic Value of One Health in Relation to the Mitigation of Zoonotic Disease Risks; Springer: Berlin/Heidelberg, Germany, 2013; Volume 365, pp. 127–151. [Google Scholar]
- Häsler, B.; Cornelsen, L.; Bennani, H.; Rushton, J. A review of the metrics for One Health benefits. Rev. Sci. Tech. 2014, 33, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Bordier, M.; Uea-Anuwong, T.; Binot, A.; Hendrikx, P.; Goutard, F.L. Characteristics of One Health surveillance systems: A systematic literature review. Prev. Vet. Med. 2020, 181, 104560. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Public Health and the Environment (RIVM). Dutch Signalling Forum Zoonoses. Available online: https://www.rivm.nl/en/one-health/dutch-signalling-forum-zoonoses (accessed on 12 May 2023).
- Alves, F.; Artursson, K.; Bloch, J.; Brisabois, A.; Imberechts, H.; Jokelainen, P.; La Ragione, R.; Lindblad, M.; Forss, R.L.; Marston, D.A.; et al. A multi-country One Health foodborne outbreak simulation exercise: Cross-sectoral cooperation, data sharing and communication. Front. Public Health 2023, 11, 1121522. [Google Scholar] [CrossRef] [PubMed]
- National Research Council (US) Committee on Achieving Sustainable Global Capacity for Surveillance and Response to Emerging Diseases of Zoonotic Origin. Sustaining Global Surveillance and Response to Emerging Zoonotic Diseases; Keusch, G.T., Pappaioanou, M., Gonzalez, M.C., Scott, K.A., Tsai, P., Eds.; Making the Case for Zoonotic Disease Surveillance; National Academies Press: Washington, DC, USA, 2009; Volume 2. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Data Collection | Population of Interest | Competent Authority | Number of Zoonotic Pathogens Recorded |
|---|---|---|---|
| Human | |||
| Causes of death | Human | Federal Statistical Office of Germany | 36 |
| Causes of death, Lower Saxony | Human | State Office for Statistics of Lower Saxony | 4 |
| Haemovigilance blood donations (Hämovigilanz Blutspenden) | Human | Paul-Ehrlich-Institut (PEI) | 0 |
| Hospital diagnoses—Full inpatients discharged from hospital (Krankenhausdiagnosen—Aus dem Krankenhaus entlassene vollstationäre Patientinnen und Patienten) | Human | Federal Statistical Office of Germany | 31 |
| Hospital diagnoses—Quality reports of the hospitals (Krankenhausdiagnosen—Qualitätsberichte der Krankenhäuser) | Human | Federal Joint Committee | 0 |
| Krankenhaus-Infektions-Surveillance-System—Surveillance of nosocomial infections in intensive care units (Krankenhaus-Infektions-Surveillance-System (KISS)—Surveillance nosokomialer Infektionen auf Intensivstationen (ITS-KISS Infektionen) | Human | National Reference Center for Surveillance of Nosocomial Infections (NRZ) | 3 |
| Meningitis and Encephalitis Register in Lower Saxony (Meningitis- u. Enzephalitis Register in Niedersachsen (MERIN)) | Human | Public Health Agency of Lower Saxony (NLGA) | 2 |
| Surveillance for influenza and other acute respiratory illnesses in Lower Saxony—Module virological surveillance (Surveillance für Influenza und andere akute respiratorische Erkrankungen (ARE) in Niedersachsen—Modul virologische Surveillance (ARE-Labor)) | Human | Public Health Agency of Lower Saxony (NLGA) | 3 |
| Surveillance for influenza and other acute respiratory illnesses in Lower Saxony—Module sickness rate (Surveillance für Influenza und andere akute respiratorische Erkrankungen (ARE) in Niedersachsen—Modul Krankenstand (ARE-Krankenstand)) | Human | Public Health Agency of Lower Saxony (NLGA) | Not pathogen-based |
| Surveillance of Clostridium difficile-associated diarrhoea in hospitals (Surveillance von Clostridium difficile assoziierter Diarrhoe in Krankenhäusern (CDAD-KISS) | Human | National Reference Center for Surveillance of Nosocomial Infections (NRZ) | 1 |
| Surveillance of device-associated nosocomial infections in normal care units/non-intensive care units (Surveillance Device-assoziierter nosokomialer Infektionen auf Normalpflegestationen/Nicht-Intensivstationen (Stations-KISS Infektionen)) | Human | National Reference Center for Surveillance of Nosocomial Infections (NRZ) | 1 |
| Surveillance of Methicillin-Resistant Staphylococcus aureus in Hospitals (Surveillance von Methicillin-Resistentem Staphylococcus aureus in Krankenhäusern (MRSA-KISS)) | Human | National Reference Center for Surveillance of Nosocomial Infections (NRZ) | 1 |
| Surveillance of patients with multidrug-resistant pathogens and/or Clostridium difficile-associated diarrhoea in intensive care units and normal care units (Surveillance von Patienten mit multiresistenten Erregern (MRE) und/oder Clostridium difficile assoziierter Diarrhö (CDAD) auf Intensivstationen und Normalpflegestationen (KISS Erreger ITS u.a. Stationen)) | Human | National Reference Center for Surveillance of Nosocomial Infections (NRZ) | 2 |
| SurvNet@RKI | Human | Robert Koch Institute (RKI) | 65 |
| Animal | |||
| “Import Screening for the Anticipating of Food Risks”-Tool (ISAR-Tool) | Animal, food or feed | Bavarian Health and Food Safety Authority (LGL) | Not pathogen-based |
| Animal Disease Reporting System— Public part of the Animal Disease Information System (Tierseuchennachrichtensystem (TSN)-TierSeuchenInformationsSystem (TSIS)) | Animal | Friedrich-Loeffler-Institut (FLI) | 0 (see TSN-online) |
| Animal Disease Reporting System— Crisis module (Tierseuchennachrichtensystem (TSN)–Krisenfallverwaltungsprogramm) | Animal | Friedrich-Loeffler-Institut (FLI) | 0 (see TSN-online) |
| Animal Disease Reporting System—Central animal disease database (Tierseuchennachrichtensystem (TSN)-Zentrale Tierseuchendatenbank (TSN-Online)) | Animal | Friedrich-Loeffler-Institut (FLI) | 26 |
| Approval control data for food establishments (Zulassungskontrolldaten für Lebensmittelbetriebe) | Food or feed | Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Not pathogen-based |
| BALVI iP | Animal, food or feed, environment or water | BALVI GmbH various authorities | Not pathogen-based |
| BALVI iP—Animal feed safety | Feed | Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Not pathogen-based |
| Federal surveillance plan (Bundesweiter Überwachungsplan (BÜP)) | Food | Federal Office of Consumer Protection and Food Safety (BVL) | Not pathogen-based |
| Laboratory information management system (LIMS) of the Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Animal, food or feed, environment or water | Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | 31 |
| Monitoring according §§ 50–52 German Food and Feed Code | Food | National: Federal Office of Consumer Protection and Food Safety Lower Saxony: Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Not pathogen-based |
| Monitoring of zoonoses and zoonotic agents (Zoonosen-Monitoring (ZooMo)) | Animal, food or feed | National: Federal Office of Consumer Protection and Food Safety Lower Saxony: Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | 0 (see LIMS LAVES) |
| National Residue Control Plan (Nationaler Rückstandskontrollplan, NRKP) | Animal, food or feed | Federal Office of Consumer Protection and Food Safety Lower Saxony: Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Not pathogen-based |
| Nationwide system for collecting data on food involved in foodborne outbreaks (Bundesweites System zur Erfassung von Daten zu Lebensmitteln, die an lebensmittelbedingten Krankheitsausbrüchen beteiligt sind (BELA)) | Other | Federal Office of Consumer Protection and Food Safety (BVL) | 7 |
| Rapid Alert System for Food and Feed (RASFF) | Food or feed, other | European commission, Directorate-General for Health and Food Safety (GD SANTE) | 15 |
| Salmonella control programme (Salmonellen-Bekämpfungsprogramm) | Animal | German Federal Institute for Risk Assessment (BfR) | 1 |
| Organizational tool for sampling (Probenbörse) | Other | Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Not pathogen-based |
| Trade Control and Expert System New Technology (TRACES NT) | Animal, food or feed | European Commission-DG Health and Food Safety | Not pathogen-based |
| Whistleblower system/Anonymous reporting system (Anonyme Meldestelle) | Overarching | Lower Saxony State Office for Consumer Protection and Food Safety (LAVES) | Not pathogen-based |
| Zoonoses Trend Reports (Zoonosen-Trendbericht) | Overarching | National: Federal Office of Consumer Protection and Food Safety (BVL) | 0 (see LIMS LAVES) |
| Environment | |||
| Bathing Water Report of Lower Saxony for the European Union (EU-Badegewässer-Berichterstattung für Niedersachsen (BBE)) | Environment or water | Public Health Agency of Lower Saxony (NLGA) | 2 |
| Climate Data Center (CDC) | Environment | Deutscher Wetterdienst | Not pathogen-centred |
| Drinking Water Database of Lower Saxony (Niedersächsische Trinkwasserdatenbank (NiWaDaB)) | Environment, other | Public Health Agency of Lower Saxony (NLGA) | 5 |
| Others | |||
| LSN-Online-Database | Humans, Animal, environment | Statistical Office of Lower Saxony | Not pathogen-centred |
| Data Collection | Population and, if Applicable, Matrix of Interest | Average Findings per Year * | Publication of Data | Access to Original Data | Source Data Type | Export Data Type | Editing of the Original Data | Updating |
|---|---|---|---|---|---|---|---|---|
| Campylobacter spp. | ||||||||
| Rapid Alert System for Food and Feed (RASFF) | Food | 2 | Yes | Reading and/or export publicly | Database | Excel, CSV | Re-selection and reduction | Daily |
| Nationwide system for collecting data on food involved in foodborne outbreaks (BELA) | Food | 20 | Yes | Access denied | No | Annually | ||
| Animal Disease Reporting System (TSN) | Animal | 30 | Yes | Access denied | Database | Excel, CSV, KMZ/KML | Re-selection and reduction | Daily |
| Laboratory information management system LAVES | Animal, food or feed, environment or water: divers matrices | 460 | No | Access denied | Database | Excel, CSV, XML | Anonymisation, re-selection and reduction | Daily |
| SurvNet@RKI | Human: blood/serum, tissue sample, other | 6000 | Yes | Reading and/or export on request | Database | CSV | Anonymisation | Daily |
| Causes of death | Human | 5 | Yes | Reading and/or export publicly | Database | Excel, PDF | Anonymisation, aggregation of detailed data into larger units | Annually |
| Listeria spp. | ||||||||
| Hospital diagnoses—full inpatients discharged from hospital | Human | 30 | Yes | Reading and/or export publicly | Database | Excel, CSV, XML, FLAT | Anonymisation, aggregation of detailed data into larger units, re-selection and reduction | Annually |
| Rapid Alert System for Food and Feed | Food | 30 | Yes | Reading and/or export publicly | Database | Excel, CSV, | Re-selection and reduction | Daily |
| Animal Disease Reporting System (TSN) | Animals | 5 | Yes | Access denied | Database | Excel, CSV, KMZ/KML | Re-selection and reduction | Daily |
| Laboratory information management system LAVES | Population and matrix both divers | 250 | No | Access denied | Database | Excel, CSV, XML | Anonymisation, re-selection and reduction | Daily |
| SurvNet@RKI | Human: blood/ serum, tissue sample, Other | 60 | Yes | Reading and/or export on request | Database | CSV | No | Daily |
| Causes of death | Human | 20 | Yes | Reading and/or export publicly | Database | Excel, PFD | Anonymisation, aggregation of detailed data into larger units | Annually |
| Francisella tularensis | ||||||||
| Laboratory information management system LAVES | Population and matrix both divers | 50 | No | Access denied | Database | Excel, CSV, XML | Anonymisation, re-selection and reduction | Daily |
| SurvNet@RKI | Human: blood/ serum, tissue sample, other | 2 | Yes | Reading and/or export on request | Database | CSV | No | Daily |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnepf, A.; Hille, K.; van Mark, G.; Winkelmann, T.; Remm, K.; Kunze, K.; Velleuer, R.; Kreienbrock, L. Basis for a One Health Approach—Inventory of Routine Data Collections on Zoonotic Diseases in Lower Saxony, Germany. Zoonotic Dis. 2024, 4, 57-73. https://doi.org/10.3390/zoonoticdis4010007
Schnepf A, Hille K, van Mark G, Winkelmann T, Remm K, Kunze K, Velleuer R, Kreienbrock L. Basis for a One Health Approach—Inventory of Routine Data Collections on Zoonotic Diseases in Lower Saxony, Germany. Zoonotic Diseases. 2024; 4(1):57-73. https://doi.org/10.3390/zoonoticdis4010007
Chicago/Turabian StyleSchnepf, Anne, Katja Hille, Gesine van Mark, Tristan Winkelmann, Karen Remm, Katrin Kunze, Reinhard Velleuer, and Lothar Kreienbrock. 2024. "Basis for a One Health Approach—Inventory of Routine Data Collections on Zoonotic Diseases in Lower Saxony, Germany" Zoonotic Diseases 4, no. 1: 57-73. https://doi.org/10.3390/zoonoticdis4010007
APA StyleSchnepf, A., Hille, K., van Mark, G., Winkelmann, T., Remm, K., Kunze, K., Velleuer, R., & Kreienbrock, L. (2024). Basis for a One Health Approach—Inventory of Routine Data Collections on Zoonotic Diseases in Lower Saxony, Germany. Zoonotic Diseases, 4(1), 57-73. https://doi.org/10.3390/zoonoticdis4010007