
Adaptation of the One Health Zoonotic Disease Prioritization Tool for Government and Privately Owned Companion Animal Zoonotic Disease Surveillance


Abstract
:Simple Summary
Abstract
1. Introduction
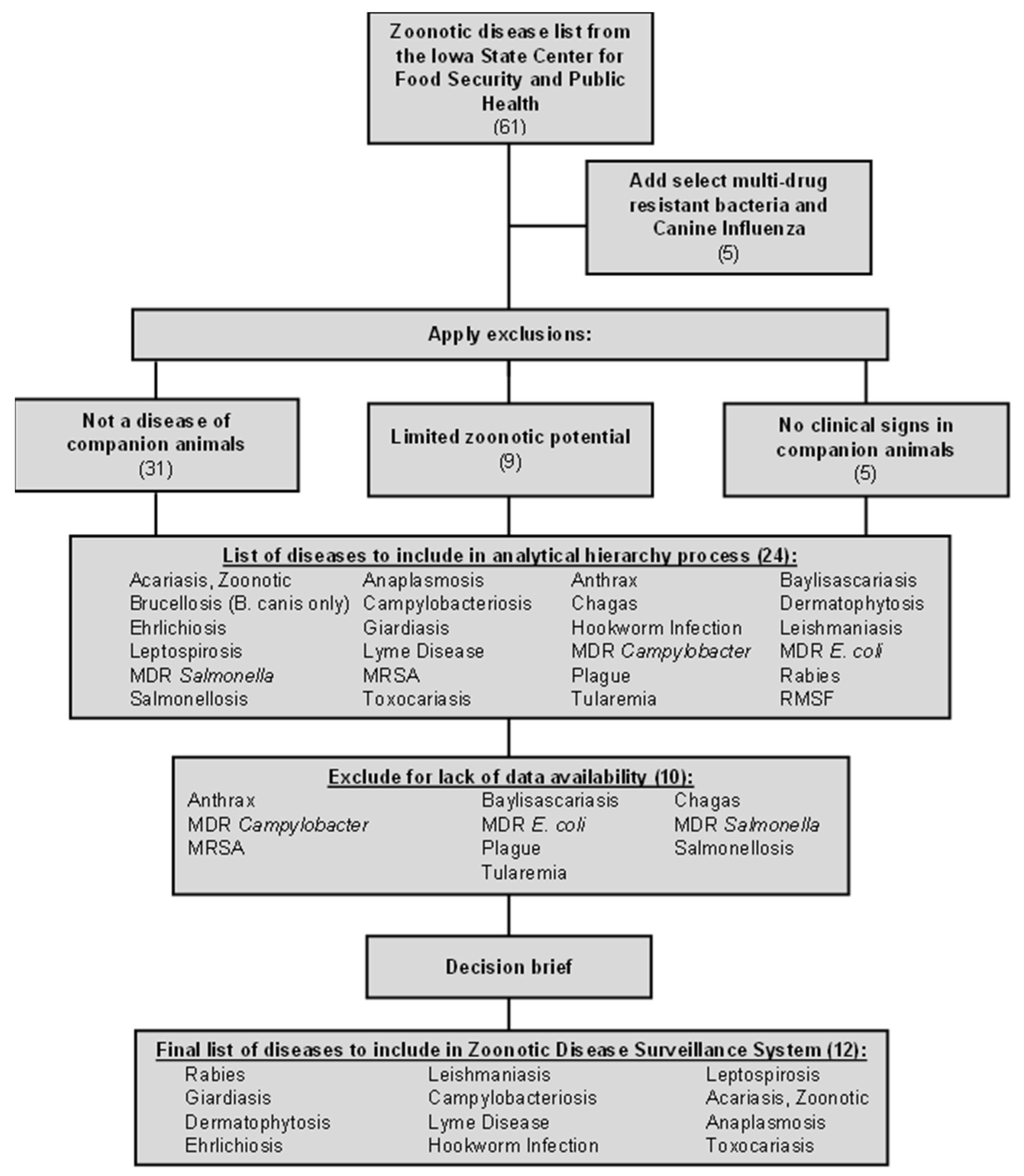
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- American Pet Products Association. Available online: https://www.americanpetproducts.org/press_industrytrends.asp (accessed on 21 October 2022).
- Taylor, L.H.; Latham, S.M.; Woolhouse, M.E. Risk factors for human disease emergence. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2001, 356, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Woolhouse, M.E.J.; Gowtage-Sequeria, S. Host range and emerging and reemerging pathogens. Emerg. Infect. Dis. 2005, 11, 1842–1847. [Google Scholar] [CrossRef] [PubMed]
- Broadbelt, D.; Middleton, S.; Summers, J.; Church, D. Companion Animal Practice Based Disease Surveillance in the UK. Epidemiol. Et Sante Anim. 2011, 59–60, 38–40. [Google Scholar]
- Balabanova, Y.; Gilsdorf, A.; Buda, S.; Burger, R.; Eckmanns, T.; Gärtner, B.; Groß, U.; Haas, W.; Hamouda, O.; Hübner, J.; et al. Communicable diseases prioritized for surveillance and epidemiological research: Results of a standardized prioritization procedure in Germany. PLoS ONE 2011, 6, e25691. [Google Scholar] [CrossRef] [PubMed]
- Cito, F.; Rijks, J.; Rantsios, A.T.; Cunningham, A.A.; Baneth, G.; Guardabassi, L.; Kuiken, T.; Giovannini, A. Prioritization of Companion Animal Transmissible Diseases for Policy Intervention in Europe. J. Comp. Pathol. 2016, 155 (Suppl. 1), S18–S26. [Google Scholar] [CrossRef] [PubMed]
- Stebler, N.; Schuepbach-Regula, G.; Braam, P.; Falzon, L.C. Use of a modified Delphi panel to identify and weight criteria for prioritization of zoonotic diseases in Switzerland. Prev. Vet. Med. 2015, 121, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.B.; Hautala, J.A. Meeting Report: Panel on the Potential Utility and Strategies for Design and Implementation of a National Companion Animal Infectious Disease Surveillance System. Zoonoses Public Health 2008, 55, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Krause, G. How can infectious diseases be prioritized in public health? A standardized prioritization scheme for discussion. EMBO Rep. 2008, 9 (Suppl. 1), S22–S27. [Google Scholar] [CrossRef]
- O’Brien, E.C.; Taft, R.; Geary, K.; Ciotti, M.; Suk, J.E. Best practices in ranking communicable disease threats: A literature review, 2015. Eurosurveillance 2016, 21, 30212. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.; Sargeant, J.M. A quantitative approach to the prioritization of zoonotic diseases in North America: A health professionals’ perspective. PLoS ONE 2013, 8, e72172. [Google Scholar] [CrossRef] [PubMed]
- Burnette, W.N.; Hoke, C.H.; Scovill, J.; Clark, K.; Abrams, J.; Kitchen, L.W.; Hanson, K.; Palys, T.J.; Vaughn, D.W. Infectious Diseases Investment Decision Evaluation Algorithm—A Quantitative Algorithm for Prioritization of Naturally Occurring Infectious Disease Threats to the U.S. Military. Mil. Med. 2008, 173, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Rist, C.L.; Arriola, C.S.; Rubin, C. Prioritizing zoonoses: A proposed one health tool for collaborative decision-making. PLoS ONE 2014, 9, e109986. [Google Scholar] [CrossRef]
- Department of Defense Directive 6400.04E. DoD Veterinary Public Health and Animal Health Services. 2017. Available online: https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodd/640004Ep.pdf?ver=2019-04-08-104448-270 (accessed on 21 October 2022).
- The Center for Food Security and Public Health. Available online: https://www.cfsph.iastate.edu/diseaseinfo/?transmission%5B%5D=006&lang=en (accessed on 21 October 2022).
- Sun, H.; Blackmon, S.; Yang, G.; Waters, K.; Li, T.; Tangwangvivat, R.; Xu, Y.; Shyu, D.; Wen, F.; Cooley, J.; et al. Zoonotic Risk, Pathogenesis, and Transmission of Avian-Origin H3N2 Canine Influenza Virus. J. Virol. 2017, 91, e00637-17. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Setting Priorities in Communicable Disease Surveillance; World Health Organization: Lyon, France, 2006. [Google Scholar]
- Saaty, T.L. Decision making with the analytic hierarchy process. Int. J. Serv. Sci. 2008, 1, 83–98. [Google Scholar] [CrossRef]
- Mu, E.; Pereyra-Rojas, M. Understanding the Analytic Hierarchy Process. In Practical Decision Making; SpringerBriefs in Operations Research; Springer: Berlin/Heidelberg, Germany, 2017; Chapter 2; pp. 7–22. [Google Scholar]
- Dolan, J.G. Shared decision-making—Transferring research into practice: The Analytic Hierarchy Process (AHP). Patient Educ. Couns. 2008, 73, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Pauer, F.; Schmidt, K.; Babac, A.; Damm, K.; Frank, M.; von der Schulenburg, J.M.G. Comparison of different approaches applied in Analytic Hierarchy Process—An example of information needs of patients with rare diseases. BMC Med. Inform. Decis. Mak. 2016, 16, 117. [Google Scholar] [CrossRef] [PubMed]
- Wedley, W.C. Consistency prediction for incomplete AHP matrices. Math. Comput. Model. 1993, 17, 151–161. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/lyme/index.html#:~:text=Lyme%20disease%20is%20the%20most,bite%20of%20infected%20blacklegged%20ticks (accessed on 21 October 2022).
- Salyer, S.J.; Silver, R.; Simone, K.; Behravesh, C.B. Prioritizing Zoonoses for Global Health Capacity Building—Themes from One Health Zoonotic Disease Workshops in 7 Countries, 2014–2016. Emerg. Infect. Dis. J. 2017, 23 (Suppl. 1), S55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Criteria | Definition | Weight |
|---|---|---|
| Epidemic/pandemic potential in humans | Is the zoonotic disease capable of sustained human-to-human transmission? | 6 |
| Data availability | Can data for the zoonotic disease be accurately and consistently captured in the current system of record, (i.e., electronic animal health record)? | 5 |
| Bioterrorism potential | Is the zoonotic-disease-causing pathogen listed as a select agent? | 4 |
| Severity of Illness in humans | Is the case fatality in humans greater than 10% or does the pathogen cause long-term disability? | 3 |
| Ability to prevent/control | Is there an effective vaccine for the zoonotic disease in the companion animal reservoir? | 2 |
| Severity of illness in animal | Is the case fatality in animals greater than 10% or does the pathogen cause long-term disability? | 1 |
| Disease | Normalized Score | Rank |
|---|---|---|
| Leptospirosis | 1.000 | 1 |
| Plague * | 0.824 | 2 |
| Anthrax * | 0.765 | 3 |
| Acariasis, Zoonotic | 0.647 | 4 |
| Campylobacteriosis | 0.647 | 4 |
| Dermatophytosis | 0.647 | 4 |
| Giardiasis | 0.647 | 4 |
| Rabies | 0.647 | 4 |
| Leishmaniasis | 0.529 | 5 |
| MRSA * | 0.529 | 5 |
| Tularemia * | 0.471 | 6 |
| Lyme Disease | 0.412 | 7 |
| MDR Campylobacter * | 0.353 | 8 |
| MDR E. coli * | 0.353 | 8 |
| MDR Salmonella * | 0.353 | 8 |
| RMSF | 0.353 | 8 |
| Salmonellosis * | 0.353 | 8 |
| Anaplasmosis | 0.294 | 9 |
| Brucellosis (B. canis only) | 0.294 | 9 |
| Ehrlichiosis | 0.294 | 9 |
| Hookworm Infection | 0.294 | 9 |
| Toxocariasis | 0.294 | 9 |
| Chagas * | 0.235 | 10 |
| Baylisascariasis * | 0.176 | 11 |
| Final Zoonotic Disease List |
|---|
| Rabies |
| Leishmaniasis |
| Leptospirosis |
| Giardiasis |
| Campylobacteriosis |
| Acariasis, Zoonotic |
| Dermatophytosis |
| Lyme Disease |
| Anaplasmosis |
| Ehrlichiosis |
| Hookworm Infection |
| Toxocariasis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayko, H.; Watkins, S.; Waugh, S.; Moore, G.; Mullaney, S.B. Adaptation of the One Health Zoonotic Disease Prioritization Tool for Government and Privately Owned Companion Animal Zoonotic Disease Surveillance. Zoonotic Dis. 2023, 3, 243-250. https://doi.org/10.3390/zoonoticdis3030020
Bayko H, Watkins S, Waugh S, Moore G, Mullaney SB. Adaptation of the One Health Zoonotic Disease Prioritization Tool for Government and Privately Owned Companion Animal Zoonotic Disease Surveillance. Zoonotic Diseases. 2023; 3(3):243-250. https://doi.org/10.3390/zoonoticdis3030020
Chicago/Turabian StyleBayko, Heather, Sarah Watkins, Sheldon Waugh, Gerald Moore, and Sara B. Mullaney. 2023. "Adaptation of the One Health Zoonotic Disease Prioritization Tool for Government and Privately Owned Companion Animal Zoonotic Disease Surveillance" Zoonotic Diseases 3, no. 3: 243-250. https://doi.org/10.3390/zoonoticdis3030020
APA StyleBayko, H., Watkins, S., Waugh, S., Moore, G., & Mullaney, S. B. (2023). Adaptation of the One Health Zoonotic Disease Prioritization Tool for Government and Privately Owned Companion Animal Zoonotic Disease Surveillance. Zoonotic Diseases, 3(3), 243-250. https://doi.org/10.3390/zoonoticdis3030020