
Monkeypox: Re-Emerging Zoonotic Threat


Abstract
1. Introduction
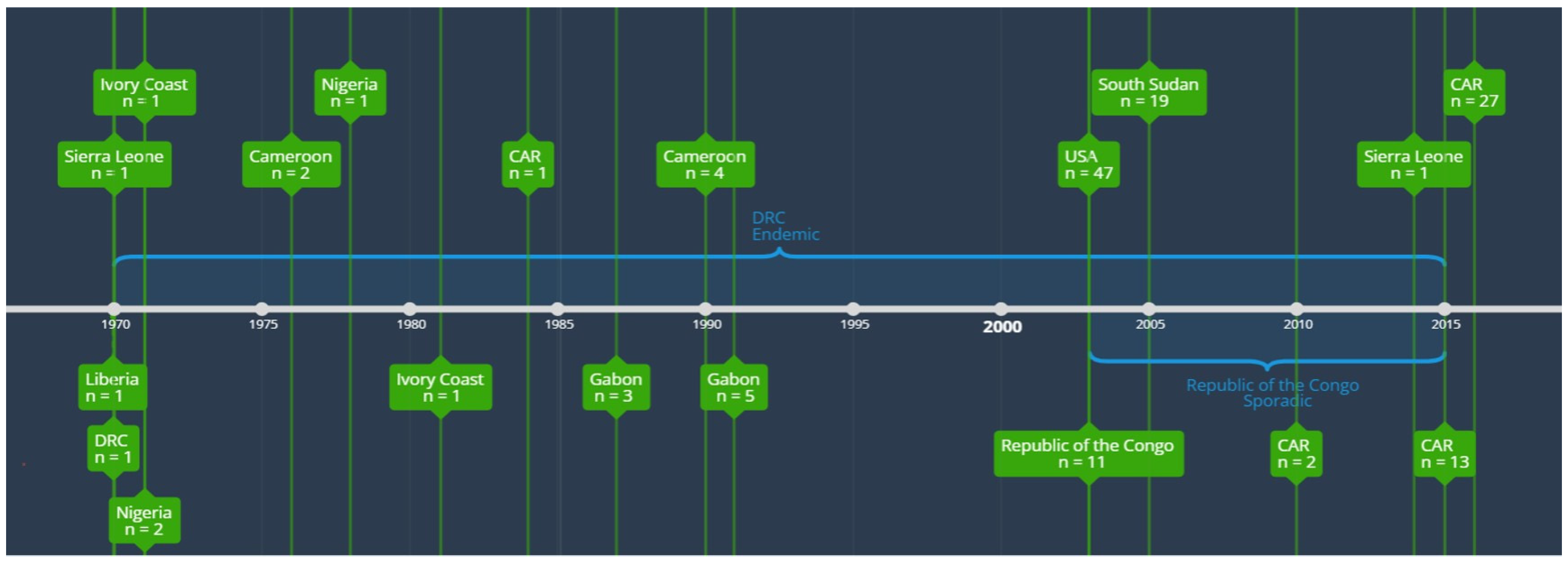
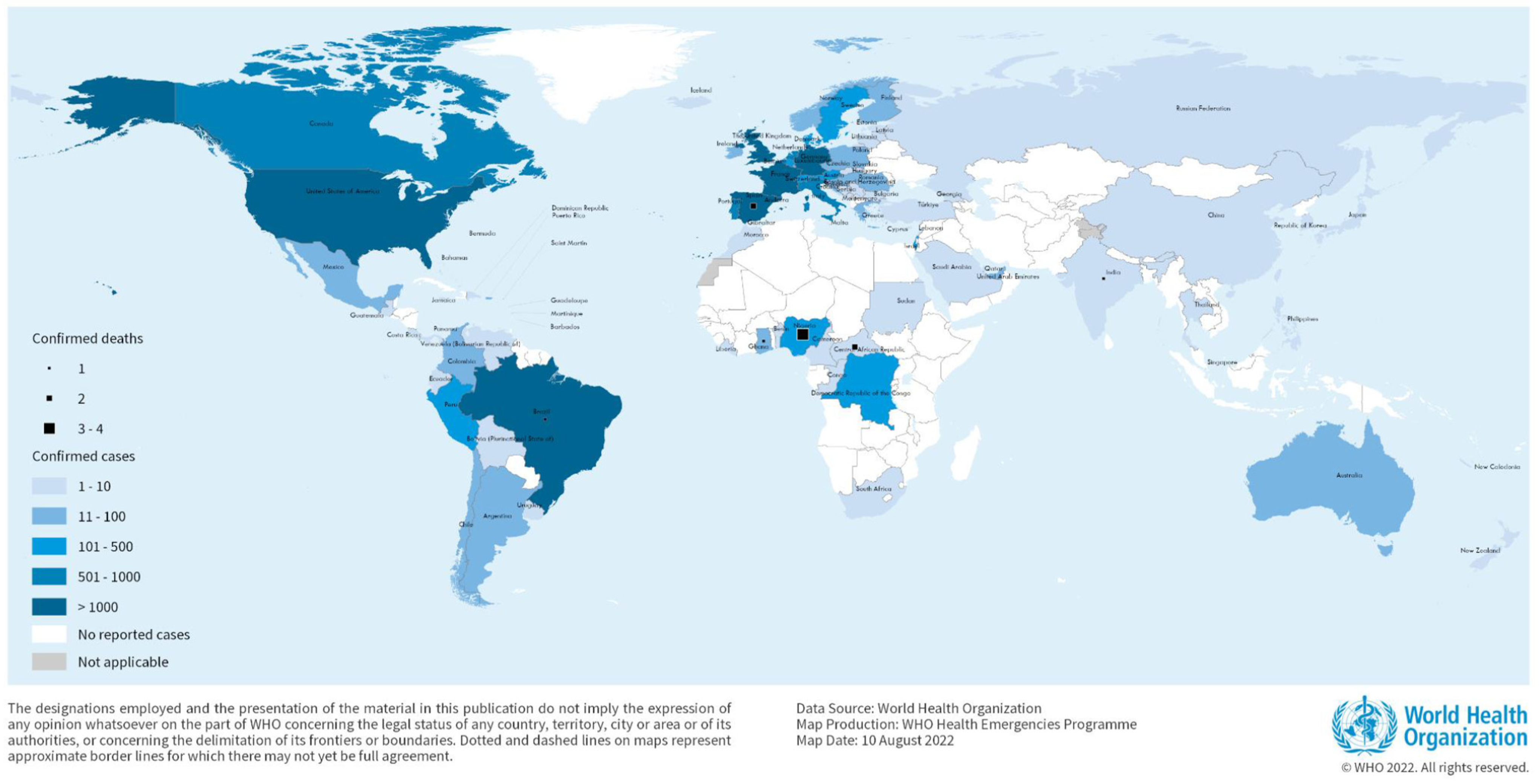
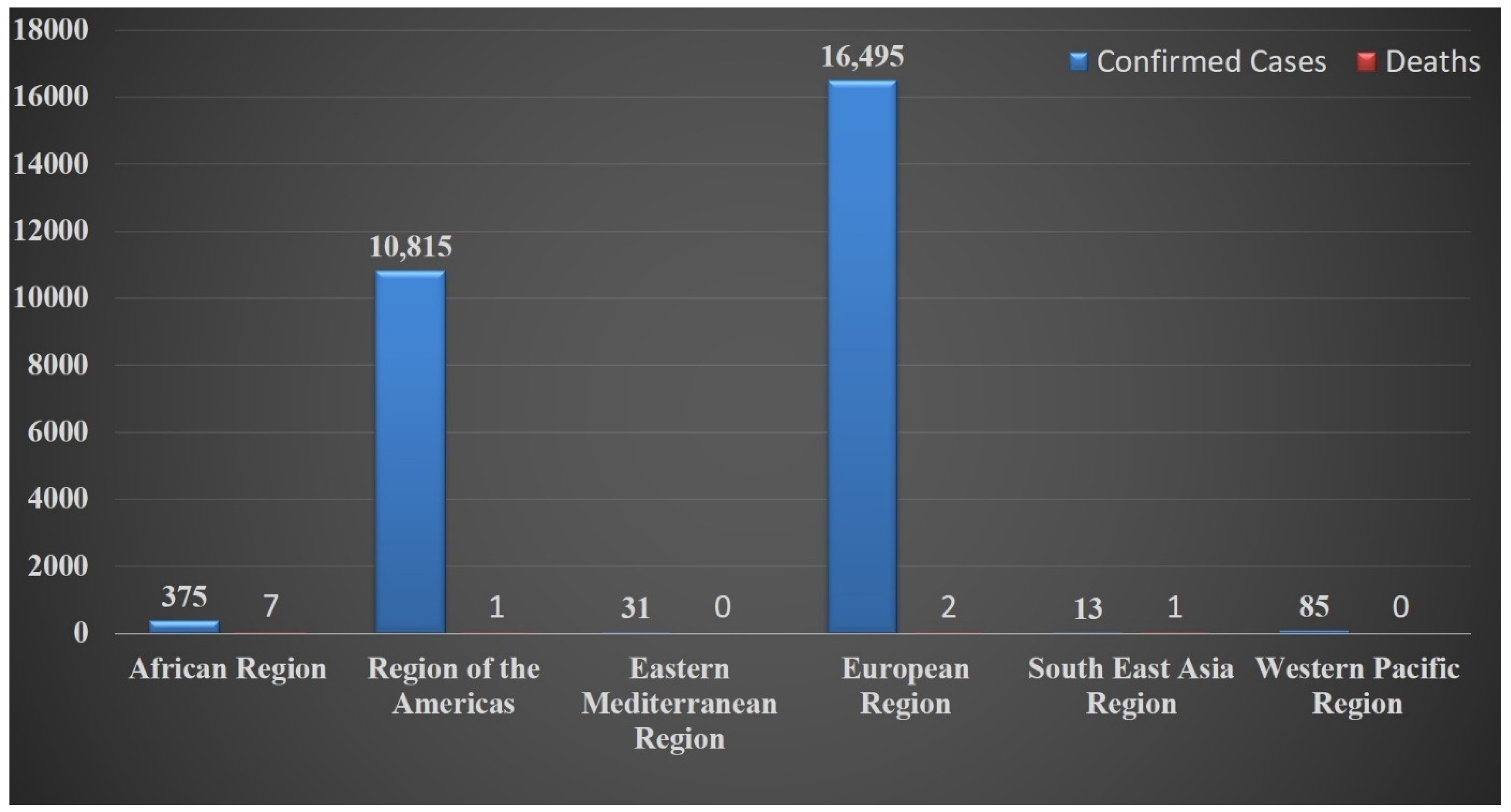
2. Epidemiology and Its History
3. Etiology, Host, and Reservoir
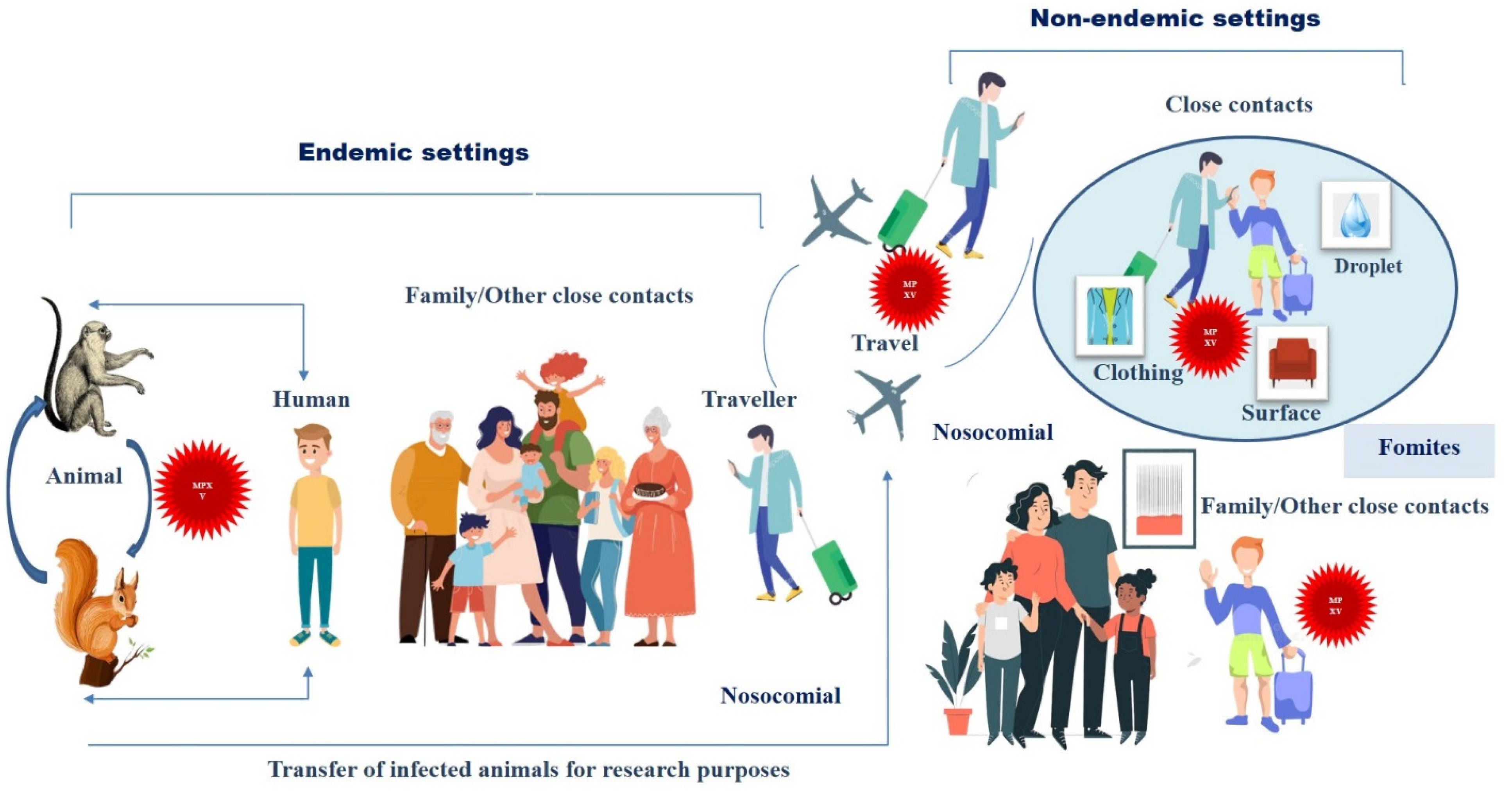
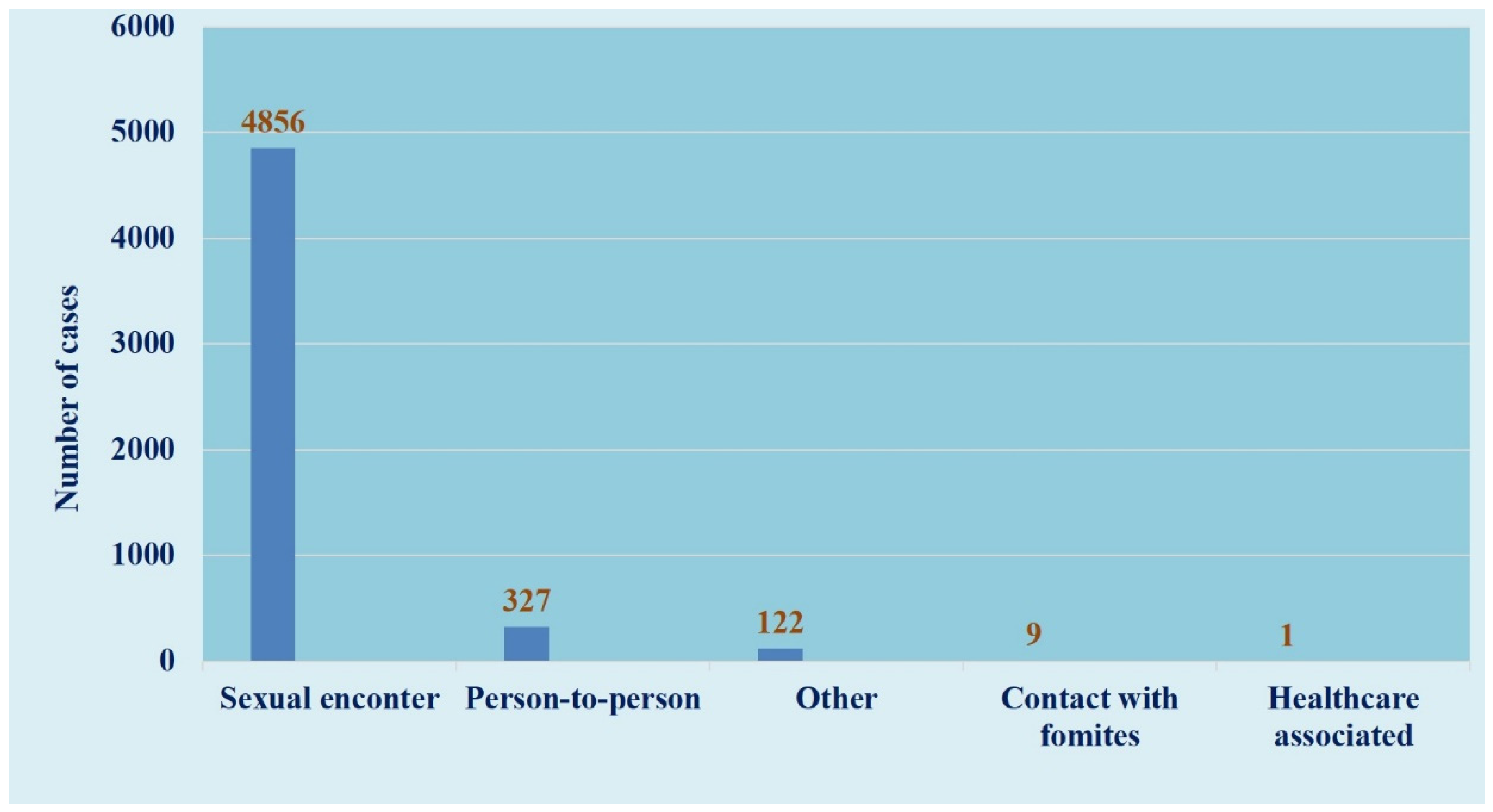
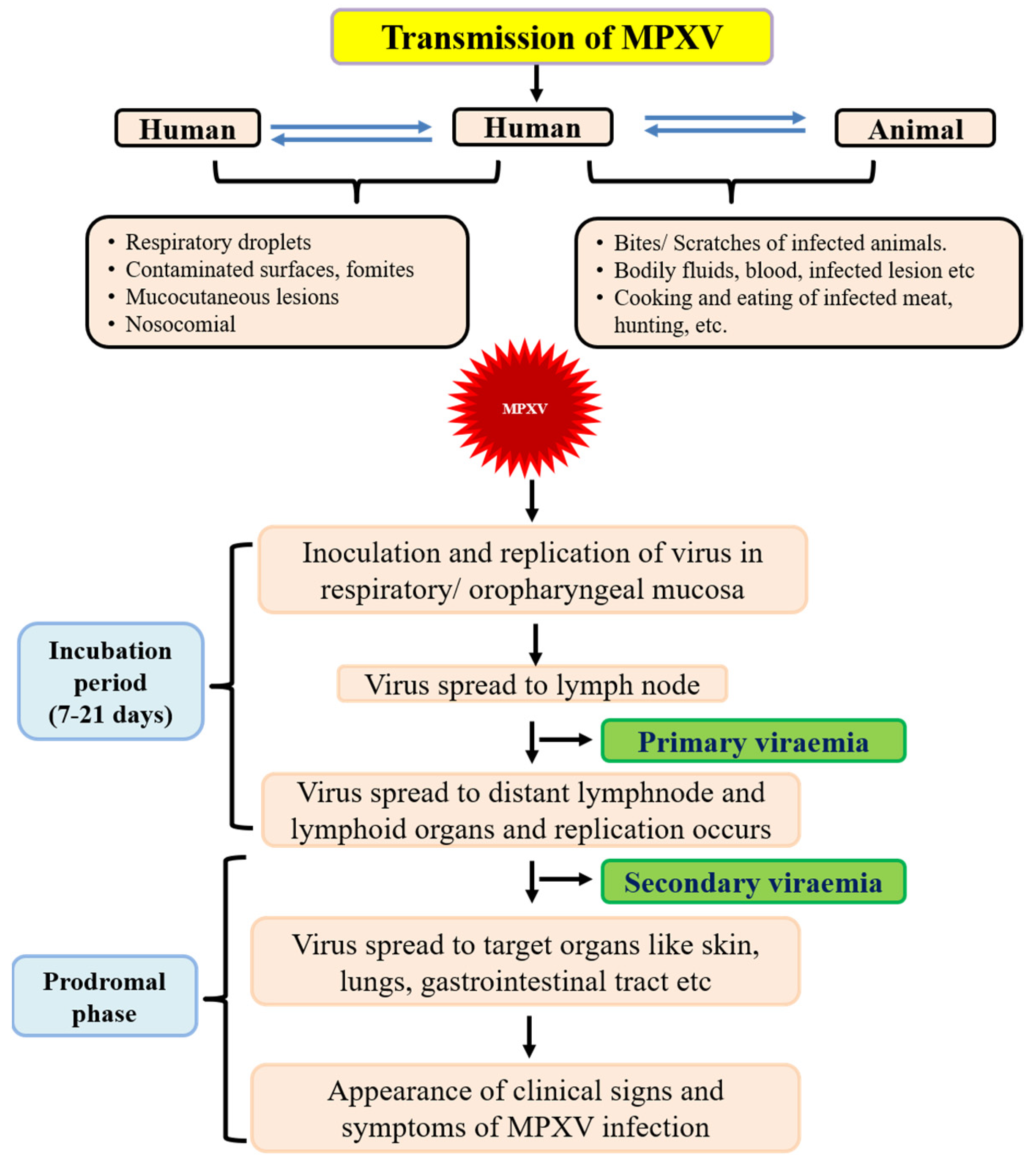
4. Mode of Transmission
5. Infectious Dose, Incubation Period and Communicability Period
6. Pathology and Pathophysiology
7. Diagnosis
8. Treatment
9. Prevention and Control
10. Immunization and Prophylaxis
11. Biosafety and Biosecurity Measures
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacNeil, A.; Reynolds, M.; Braden, Z.; Carroll, D.S.; Bostik, V.; Karem, K.; Smith, S.K.; Davidson, W.; Li, Y.; Moundeli, A.; et al. Transmission of atypical varicella-zoster virus infections involving palm and sole manifestations in an area with monkeypox endemicity. Clin. Infect. Dis. 2009, 48, e6–e8. [Google Scholar] [CrossRef] [PubMed]
- Radonić, A.; Metzger, S.; Dabrowski, P.W.; Couacy-Hymann, E.; Schuenadel, L.; Kurth, A.; Mätz-Rensing, K.; Boesch, C.; Leendertz, F.H.; Nitsche, A. Fatal monkeypox in wild-living sooty mangabey, Cote d’Ivoire, 2012. Emerg. Infect. Dis. 2014, 20, 1009–1011. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.; Nuara, A.; Buller, R.M.L.; Schultz, D.A. Human monkeypox: An emerging zoonotic disease. Future. Microbiol. 2007, 2, 17–34. [Google Scholar] [CrossRef]
- Heymann, D.L. Control of Communicable Diseases Manual, 19th ed.; American Public Health Association: Washington, DC, USA, 2008. [Google Scholar]
- Weber, D.J.; Rutala, W.A. Risks and prevention of nosocomial transmission of rare zoonotic diseases. Clin. Infect. Dis. 2001, 32, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Multi-Country Outbreak of Monkeypox, External Situation Report #3—10 August 2022. Available online: https://www.who.int/publications/m/item/multi-country-outbreak-of-monkeypox--external-situation-report--3---10-august-2022 (accessed on 13 August 2022).
- Nalca, A.; Rimoin, A.W.; Bavari, S.; Whitehouse, C.A. Re-emergence of monkeypox: Prevalence, diagnostics, and countermeasures. Clin. Infect. Dis. 2005, 41, 1765–1771. [Google Scholar] [CrossRef]
- Petersen, E.; Kantele, A.; Koopmans, M.; Asogun, D.; Yinka-Ogunleye, A.; Ihekweazu, C.; Zumla, A. Human monkeypox: Epidemiologic and clinical characteristics, diagnosis, and prevention. Infect. Dis. Clin. N. Am. 2019, 33, 1027–1043. [Google Scholar] [CrossRef]
- Von Magnus, P.; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A pox-like disease in cynomolgus monkeys. Acta Pathol. Microbiol. Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar]
- Sklenovska, N.; Van Ranst, M. Emergence of monkeypox as the most important orthopoxvirus infection in humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef]
- Heymann, D.L.; Simpson, K. The evolving epidemiology of human monkeypox: Questions still to be answered. J. Infect. Dis. 2021, 223, 1839–1841. [Google Scholar] [CrossRef]
- Sejvar, J.J.; Chowdary, Y.; Schomogyi, M.; Stevens, J.; Patel, J.; Karem, K.; Fischer, M.; Kuehnert, M.J.; Zaki, S.R.; Paddock, C.D.; et al. Human monkeypox infection: A family cluster in the midwestern United States. J. Infect. Dis. 2004, 190, 1833–1840. [Google Scholar] [CrossRef] [PubMed]
- Erez, N.; Achdout, H.; Milrot, E.; Schwartz, Y.; Wiener-Well, Y.; Paran, N.; Politi, B.; Tamir, H.; Israely, T.; Weiss, S.; et al. Diagnosis of imported monkeypox, Israel, 2018. Emerg. Infect. Dis. 2019, 25, 980–983. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, A.; Aarons, E.; Astbury, J.; Brooks, T.; Chand, M.; Flegg, P.; Hardman, A.; Harper, N.; Jarvis, R.; Mawdsley, S.; et al. Human-to-human transmission of monkeypox virus, United Kingdom, October 2018. Emerg. Infect. Dis. 2020, 26, 782–785. [Google Scholar] [CrossRef]
- Yong, S.E.F.; Ng, O.T.; Ho, Z.J.M.; Mak, T.M.; Marimuthu, K.; Vasoo, S.; Yeo, T.W.; Ng, Y.K.; Cui, L.; Ferdous, Z.; et al. Imported monkeypox, Singapore. Emerg. Infect. Dis. 2020, 26, 1826–1830. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.K.; Schulte, J.; Chen, T.-H.; Hughes, C.M.; Davidson, W.; Neff, J.M.; Markarian, M.; Delea, K.C.; Wada, S.; Liddell, A.; et al. Monkeypox in a traveler returning from Nigeria—Dallas, Texas, July 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 509–516. [Google Scholar] [CrossRef]
- Khodakevich, C.; Jezek, Z.; Messinger, D. Monkeypox virus: Ecology and public health significance. Bull. World Health Organ. 1988, 66, 742–752. [Google Scholar]
- Acha, P.N.; Szyfres, B. Zoonoses and Communicable Diseases Common to Man and Animals, 3rd ed.; Pan American Health Organization: Washington, DC, USA, 2003; ISBN 9275119910. Available online: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=2237:2010-zoonoses-communicable-diseases-common-man-animals-3rd-edition-three-volumes&Itemid=1894&lang=en#gsc.tab=0 (accessed on 25 September 2022).
- Foster, S.O.; Brink, E.W.; Hutchins, D.L.; Pifer, J.M.; Lourie, B.; Moser, C.R.; Cummings, E.C.; Kuteyi, O.E.; Eke, R.E.; Titus, J.B.; et al. Human monkeypox. Bull. World. Health. Organ. 1972, 46, 569–576. [Google Scholar]
- Pattyn, S.R. Monkeypoxvirus Infections; Revue Scientifique et Technique Office International des Epizooties: 2000. Available online: https://research.itg.be/en/publications/monkeypoxvirus-infections (accessed on 25 September 2022).
- Hutin, Y.J.; Williams, R.J.; Malfait, P.; Pebody, R.; Loparev, V.N.; Ropp, S.L.; Rodriguez, M.; Knight, J.C.; Tshioko, F.K.; Khan, A.S.; et al. Outbreak of human monkeypox, Democratic Republic of Congo, 1996 to 1997. Emerg. Infect. Dis. 2001, 7, 434–438. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Davidson, W.B.; Curns, A.T.; Conover, C.S.; Huhn, G.; Davis, J.P.; Wegner, M.; Croft, D.R.; Newman, A.; Obiesie, N.N.; et al. Spectrum of infection and risk factors for human monkeypox, United States, 2003. Emerg. Infect. Dis. 2007, 13, 1332–1339. [Google Scholar] [CrossRef]
- Croft, D.R.; Sotir, M.J.; Williams, C.J.; Kazmierczak, J.J.; Wegner, M.V.; Rausch, D.; Graham, M.B.; Foldy, S.L.; Wolters, M.; Damon, I.K.; et al. Occupational risks during a monkeypox outbreak, Wisconsin, 2003. Emerg. Infect. Dis. 2007, 13, 1150–1157. [Google Scholar] [CrossRef]
- Update: Multistate outbreak of monkeypox—Illinois, Indiana, Kansas, Missouri, Ohio, and Wisconsin, 2003. Morb. Mortal. Wkly. Rep. 2003, 52, 642–646.
- Centers for Disease Control and Prevention. Available online: http://www.cdc.gov/poxvirus/monkeypox/index.html (accessed on 13 May 2016).
- Formenty, P.; Muntasir, M.O.; Damon, I.; Chowdhary, V.; Opoka, M.L.; Monimart, C.; Mutasim, E.M.; Manuguerra, J.-C.; Davidson, W.B.; Karem, K.L.; et al. Human monkeypox outbreak caused by novel virus belonging to Congo Basin clade, Sudan, 2005. Emerg. Infect. Dis. 2010, 16, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Learned, L.A.; Bolanda, J.D.; Li, Y.; Reynolds, M.; Moudzeo, H.; Wassa, D.W.; Libama, F.; Harvey, J.M.; Likos, A.; Formenty, P.; et al. Extended interhuman transmission of monkeypox in a hospital community in the Republic of the Congo, 2003. Am. J. Trop. Med. Hyg. 2005, 73, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Damon, I.K.; Roth, C.E.; Chowdhary, V. Discovery of monkeypox in Sudan. N. Engl. J. Med. 2006, 355, 962–963. [Google Scholar] [CrossRef] [PubMed]
- International Federation of Red Cross and Red Crescent Societies. Emergency Plan of Action (EPoA) CAR Monkey-Pox Epidemic Outbreak. Available online: http://reliefweb.int/sites/reliefweb.int/files/resources/MDRCF020.pdf (accessed on 20 May 2016).
- Human pathogens and toxins act. S.C. 24, Second Session, Fortieth Parliament, 57–58 Elizabeth II, 2009. Available online: https://laws.justice.gc.ca/eng/acts/H-5.67/20090623/P1TT3xt3.html (accessed on 25 September 2022).
- Dubois, M.E.; Slifka, M.K. Retrospective analysis of monkeypox infection. Emerg. Infect. Dis. 2008, 14, 592–599. [Google Scholar] [CrossRef] [PubMed]
- McFadden, G. Poxvirus tropism. Nat. Rev. Microbiol. 2005, 3, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, G.P.; Rodrigues, R.A.L.; Lima, M.T.; Drumond, B.P.; Abrahao, J.S. Poxvirus host range genes and virus-host spectrum: A critical review. Viruses 2017, 9, 331. [Google Scholar] [CrossRef]
- Hughes, A.L.; Irausquin, S.; Friedman, R. The evolutionary biology of poxviruses. Infect. Genet. Evol. 2010, 10, 50–59. [Google Scholar] [CrossRef]
- Esposito, J.J.; Obijeski, J.F.; Nakano, J.H. The virion and soluble antigen proteins of variola, monkeypox, and vaccinia viruses. J. Med. Virol. 1977, 1, 95–110. [Google Scholar] [CrossRef]
- Baxby, D. Identification and interrelationships of the variola/ vaccinia subgroup of poxviruses. Prog. Virol. Med. 1975, 19, 215–246. [Google Scholar]
- Yinka-Ogunleye, A.; Aruna, O.; Dalhat, M.; Ogoina, D.; McCollum, A.; Disu, Y.; Mamadu, I.; Akinpelu, A.; Ahmad, A.; Burga, J.; et al. Outbreak of human monkeypox in Nigeria in 2017–18: A clinical and epidemiological report. Lancet. Infect. Dis. 2019, 19, 872–879. [Google Scholar] [CrossRef]
- Likos, A.M.; Sammons, S.A.; Olson, V.A.; Frace, A.M.; Li, Y.; Olsen-Rasmussen, M.; Davidson, W.; Galloway, R.; Khristova, M.L.; Reynolds, M.G.; et al. A tale of two clades: Monkeypox viruses. J. Gen. Virol. 2005, 86, 2661–2672. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.G.; Damon, I.K. Outbreaks of human monkeypox after cessation of smallpox vaccination. Trends Microbiol. 2012, 20, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- McCollum, A.M.; Damon, I.K. Human monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef]
- Mukinda, V.B.; Mwema, G.; Kilundu, M.; Heymann, D.L.; Khan, A.S.; Esposito, J.J. Re-emergence of human monkeypox in Zaire in 1996. Lancet 1997, 349, 1449–1450. [Google Scholar] [CrossRef]
- Doty, J.B.; Malekani, J.M.; Kalemba, L.N.; Stanley, W.T.; Monroe, B.P.; Nakazawa, Y.U.; Mauldin, M.R.; Bakambana, T.L.; Liyandja, T.L.D.; Braden, Z.H.; et al. Assessing monkeypox virus prevalence in small mammals at the human-animal interface in the Democratic Republic of the Congo. Viruses 2017, 9, 283. [Google Scholar] [CrossRef]
- Silva, N.I.O.; de Oliveira, J.S.; Kroon, E.G.; Trindade, G.S.; Drumond, B.P. Here, there, and everywhere: The wide host range and geographic distribution of zoonotic Orthopoxviruses. Viruses 2021, 13, 43. [Google Scholar] [CrossRef]
- Diaz, J.H. The Disease Ecology, Epidemiology, Clinical Manifestations, Management, Prevention, and Control of Increasing Human Infections with Animal Orthopoxviruses. Wilderness Environl. Med. 2021, 32, 528–536. [Google Scholar] [CrossRef]
- Patrono, L.V.; Pléh, K.; Samuni, L.; Ulrich, M.; Röthemeier, C.; Sachse, A.; Muschter, S.; Nitsche, A.; Couacy-Hymann, E.; Boesch, C.; et al. Monkeypox virus emergence in wild chimpanzees reveals distinct clinical outcomes and viral diversity. Nat. Microbiol. 2020, 5, 955–965. [Google Scholar] [CrossRef]
- Thomassen, H.A.; Fuller, T.; Asefi-Najafabady, S.; Shiplacoff, J.A.G.; Mulembakani, P.M.; Blumberg, S.; Johnston, S.C.; Kisalu, N.K.; Kinkela, T.L.; Fair, J.N.; et al. Pathogen-host associations and predicted range shifts of human monkeypox in response to climate change in central Africa. PLoS ONE 2013, 8, e66071. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Biosafety in Microbiological and Biomedical Laboratories (BMBL), 5th ed.; Richmond, J.Y., McKinney, R.W., Eds.; Centers for Disease Control and Prevention: Washingtion, DC, USA, 2007.
- Kaler, J.; Hussain, A.; Flores, G.; Kheiri, S.; Desrosiers, D. Monkeypox: A Comprehensive Review of Transmission, Pathogenesis, and Manifestation. Cureus 2022, 14, e26531. [Google Scholar] [CrossRef] [PubMed]
- Mutombo, M.W.; Jezek, Z.; Arita, I.; Jezek, Z. Human monkeypox transmitted by a chimpanzee in a tropical rain-forest area of Zaire. Lancet 1983, 1, 735–737. [Google Scholar] [CrossRef]
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.; Buller, R.M. A review of experimental and natural infections of animals with monkeypox virus between 1958 and 2012. Futur. Virol. 2013, 8, 129–157. [Google Scholar] [CrossRef]
- Nolen, L.D.; Tamfum, J.-J.M.; Kabamba, J.; Likofata, J.; Katomba, J.; McCollum, A.M.; Monroe, B.; Kalemba, L.; Mukadi, D.; Bomponda, P.L.; et al. Introduction of monkeypox into a community and household: Risk factors and zoonotic reservoirs in the Democratic Republic of the Congo. Am. J. Trop. Med. Hyg. 2015, 93, 410–415. [Google Scholar] [CrossRef]
- Ellis, C.K.; Carroll, D.S.; Lash, R.R.; Peterson, A.T.; Damon, I.K.; Malekani, J.; Formenty, P. Ecology and geography of human monkeypox case occurrences across Africa. J. Wildl. Dis. 2012, 48, 335–347. [Google Scholar] [CrossRef]
- Yinka-Ogunleye, A.; Aruna, O.; Ogoina, D.; Aworabhi, N.; Eteng, W.; Badaru, S.; Mohammed, A.; Agenyi, J.; Etebu, E.; Numbere, T.-W.; et al. Reemergence of human monkeypox in Nigeria, 2017. Emerg. Infect. Dis. 2018, 24, 1149–1151. [Google Scholar] [CrossRef]
- Ihekweazu, C.; Yinka-Ogunleye, A.; Lule, S.; Ibrahim, A. Importance of epidemiological research of monkeypox: Is incidence increasing? Expert Rev. Anti-Infect. Ther. 2020, 18, 389–392. [Google Scholar] [CrossRef]
- Hussain, A.; Kaler, J.; Tabrez, E.; Tabrez, S.; Tabrez, S.S. Novel COVID-19: A comprehensive review of transmission, manifestation, and pathogenesis. Cureus 2020, 12, e8184. [Google Scholar] [CrossRef]
- Titanji, B.K.; Tegomoh, B.; Nematollahi, S.; Konomos, M.; Kulkarni, P.A. Monkeypox: A Contemporary Review for Healthcare Professionals. Open Forum Infect. Dis. 2022, 9, ofac310. [Google Scholar] [CrossRef] [PubMed]
- Jezek, Z.; Grab, B.; Szczeniowski, M.V.; Paluku, K.M.; Mutombo, M. Human monkeypox: Secondary attack rates. Bull. World Health Organ. 1988, 66, 465–470. [Google Scholar] [PubMed]
- Di Giulio, D.B.; Eckburg, P.B. Human monkeypox: An emerging zoonosis. Lancet Infect. Dis. 2004, 4, 15–25. [Google Scholar] [CrossRef]
- Antinori, A.; Mazzotta, V.; Vita, S.; Carletti, F.; Tacconi, D.; Lapini, L.E.; D’Abramo, A.; Cicalini, S.; Lapa, D.; Pittalis, S.; et al. Epidemiological, clinical and virological characteristics of four cases of monkeypox support transmission through sexual contact, Italy, May 2022. Eurosurveillance 2022, 27, 2200421. [Google Scholar] [CrossRef]
- Heskin, J.; Belfield, A.; Milne, C.; Brown, N.; Walters, Y.; Scott, C.; Bracchi, M.; Moore, L.S.; Mughal, N.; Rampling, T.; et al. Transmission of monkeypox virus through sexual contact—A novel route of infection. J. Infect. 2022, 85, 334–363. [Google Scholar] [CrossRef]
- Rimoin, A.W.; Mulembakani, P.M.; Johnston, S.C.; Smith, J.O.L.; Kisalu, N.K.; Kinkela, T.L.; Blumberg, S.; Thomassen, H.A.; Pike, B.L.; Fair, J.N.; et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc. Natl. Acad. Sci. USA 2010, 107, 16262–16267. [Google Scholar] [CrossRef]
- Nolen, L.D.; Osadebe, L.; Katomba, J.; Likofata, J.; Mukadi, D.; Monroe, B.; Doty, J.; Hughes, C.M.; Kabamba, J.; Malekani, J.; et al. Extended human-to-human transmission during a monkeypox outbreak in the Democratic Republic of the Congo. Emerg. Infect. Dis. 2016, 22, 1014–1021. [Google Scholar] [CrossRef]
- Meyer, H.; Perrichot, M.; Stemmler, M.; Emmerich, P.; Schmitz, H.; Varaine, F.; Shungu, R.; Tshioko, F.; Formenty, P. Outbreaks of disease suspected of being due to human monkeypox virus infection in the Democratic Republic of Congo in 2001. J. Clin. Microbiol. 2002, 40, 2919–2921. [Google Scholar] [CrossRef]
- Nakouné, E.; Kazanji, M. Monkeypox detection in maculopapular lesions in two young Pygmies in the Central African Republic. Int. J. Infect. Dis. 2012, 16, e266–e267. [Google Scholar] [CrossRef]
- Moore, M.; Zahra, F. Monkeypox; Stat Pearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Okyay, R.A.; Bayrak, E.; Kaya, E.; Sahin, A.R.; Kocyigit, B.F.; Tasdogan, A.M.; Avci, A.; Sumbul, H.E. Another epidemic in the shadow of Covid 19 pandemic: A review of monkeypox. EJMO 2022, 6, 95–99. [Google Scholar] [CrossRef]
- Reynolds, M.G.; McCollum, A.M.; Nguete, B.; Lushima, R.S.; Petersen, B.W. Improving the care and treatment of monkeypox patients in low-resource settings: Applying evidence from contemporary biomedical and smallpox biodefense research. Viruses 2017, 9, 380. [Google Scholar] [CrossRef] [PubMed]
- Stagles, M.; Watson, A.; Boyd, J.; More, I.; McSeveney, D. The histopathology and electron microscopy of a human monkeypox lesion. Trans. R. Soc. Trop. Med. Hyg. 1985, 79, 192–202. [Google Scholar] [CrossRef]
- Afshar, Z.M.; Rostami, H.N.; Hosseinzadeh, R.; Janbakhsh, A.; Pirzaman, A.T.; Babazadeh, A.; Aryanian, Z.; Sio, T.T.; Barary, M.; Ebrahimpour, S. The reemergence of monkeypox as a new potential health challenge: A critical review. Authorea 2022. [Google Scholar] [CrossRef]
- Chen, N.; Li, G.; Liszewski, M.K.; Atkinson, J.P.; Jahrling, P.B.; Feng, Z.; Schriewer, J.; Buck, C.; Wang, C.; Lefkowitz, E.J.; et al. Virulence differences between monkeypox virus isolates from West Africa and the Congo Basin. Virology 2005, 340, 46–63. [Google Scholar] [CrossRef]
- Rubins, K.H.; Hensley, L.E.; Relman, D.A.; Brown, P.O. Stunned silence: Gene expression programs in human cells infected with monkeypox or vaccinia virus. PLoS ONE 2011, 6, e15615. [Google Scholar] [CrossRef] [PubMed]
- Multi-Country Outbreak of Monkeypox, External Situation Report #2—25 July 2022. Available online: https://www.who.int/publications/m/item/multi-country-outbreak-of-monkeypox--external-situation-report--2---25-july-2022 (accessed on 25 July 2022).
- Damon, I.K. Status of human monkeypox: Clinical disease, epidemiology and research. Vaccine 2011, 29, D54–D59. [Google Scholar] [CrossRef]
- Jezek, Z.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Human monkeypox: Clinical features of 282 patients. J. Infect. Dis. 1987, 156, 293–298. [Google Scholar] [CrossRef]
- Breman, J.G. Monkeypox: An emerging infection for humans? In Emerging Infections 4; American Society of Microbiology: Washington, DC, USA, 2000; pp. 45–67. [Google Scholar]
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.G.; Kuehnert, M.J. Clinical characteristics of human monkeypox, and risk factors for severe disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef]
- Roess, A.A.; Monroe, B.P.; Kinzoni, E.A.; Gallagher, S.; Ibata, S.R.; Badinga, N.; Molouania, T.M.; Mabola, F.S.; Mombouli, J.V.; Carroll, D.S.; et al. Assessing the effectiveness of a community intervention for monkeypox prevention in the Congo basin. PLoS Negl. Trop. Dis. 2011, 5, e1356. [Google Scholar] [CrossRef]
- Quarleri, J.; Delpino, M.V.; Galvan, V. Monkeypox: Considerations for the understanding and containment of the current outbreak in non-endemic countries. Geroscience 2022, 20, 1–9. [Google Scholar] [CrossRef]
- De Clercq, E. Cidofovir in the treatment of poxvirus infections. Antivir. Res. 2002, 55, 1–13. [Google Scholar] [CrossRef]
- Butcher, W.; Ulaeto, D. Contact inactivation of Orthopoxviruses by household disinfectants. J. Appl. Microbiol. 2005, 99, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.E.; Jezek, Z.; Grab, B.; Dixon, H. The transmission potential of monkeypox virus in human populations. Int. J. Epidemiol. 1988, 17, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Canadian Biosafety Standard (CBS); Government of Canada: Ottawa, ON, Canada, 2015.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sub-Families | Genus | Species (Members)—Virus | |
|---|---|---|---|
| 1. Chorodopoxvirinae | 1. Avipoxvirus | ||
| 2. Capripoxvirus | |||
| 3. Centapoxvirus | |||
| 4. Cervidpoxvirus | |||
| 5. Crocodylidpoxvirus |  | Akhmeta virus | |
| 6. Leporipoxvirus | Abatino macacapox virus | ||
| 7. Macropopoxvirus | Camelpox virus | ||
| 8. Molluscipoxvirus | cowpox virus | ||
| 9. Muselpoxvirus | Ectromelia virus | ||
| 10. Oryzopoxvirus | Monkeypox virus | ||
| 11. Orthopoxvirus | Raccoonpox virus | ||
| 12. Parapoxvirus | Skunkpox virus | ||
| 13. Pteropopoxvirus | Taerapox virus | ||
| 14. Salmonpoxvirus | Vaccinia virus | ||
| 15. Sciuripoxvirus | Variola virus | ||
| 16. Suipoxvirus | Volepox virus | ||
| 17. Vespertilionpoxvirus | |||
| 18. Yatapoxvirus | |||
| 2. Entomopoxvirinae | 1. Alphaentomopoxvirus | ||
| 2. Betaentomopoxvirus | |||
| 3. Deltaentomopoxvirus | |||
| 4. Gammaentomopoxvirus | |||
| Sr. No. | Transmission | Reports |
|---|---|---|
| 1 | Animal-to-human transmission through a bite or direct contact with the infected animal’s blood, body fluids, or lesions (1° Transmission) | Mutombo et al., 1983 [51]; Nalca et al., 2005 [7]; Croft et al., 2007 [24]; Reynolds et al., 2007 [23]; Brown and Leggat, 2016 [52]; Petersen et al., 2019 [8]; Diaz, 2021 [46] |
| 2 | Human-to-human via the respiratory tract, by direct contact with body fluids of an infected person, respiratory droplets, or with virus-contaminated objects (fomites) (2° Transmission) | Weber and Rutala, 2001 [5]; Nalca et al., 2005 [7]; Centers for Disease Control and Prevention, 2007 [49]; Croft et al., 2007 [24]; Formenty et al., 2010 [27]; Parker & Buller, 2013 [53]; Nolen et al., 2015 [54] |
| 3 | Consuming raw/infected meats | Parker & Buller, 2013 [53] Thomassen et al., 2013 [48] |
| 4 | Nosocomial | Ellis et al., 2012 [55]; Nolen et al., 2015 [54]; Yinka-Ogunleye et al., 2018 [56]; Ihekweazu et al., 2020 [57] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranjan, R.; Biswal, J.K. Monkeypox: Re-Emerging Zoonotic Threat. Zoonotic Dis. 2022, 2, 234-246. https://doi.org/10.3390/zoonoticdis2040019
Ranjan R, Biswal JK. Monkeypox: Re-Emerging Zoonotic Threat. Zoonotic Diseases. 2022; 2(4):234-246. https://doi.org/10.3390/zoonoticdis2040019
Chicago/Turabian StyleRanjan, Rajeev, and Jitendra Kumar Biswal. 2022. "Monkeypox: Re-Emerging Zoonotic Threat" Zoonotic Diseases 2, no. 4: 234-246. https://doi.org/10.3390/zoonoticdis2040019
APA StyleRanjan, R., & Biswal, J. K. (2022). Monkeypox: Re-Emerging Zoonotic Threat. Zoonotic Diseases, 2(4), 234-246. https://doi.org/10.3390/zoonoticdis2040019