1. Introduction
Healthcare-associated infections (HAI) are a serious public health problem [
1]. The impact of HAI implies high costs for patients and their families, health institutions and society [
1,
2]. Hand hygiene is a quality indicator for healthcare safety [
2].
Hospitalized children require the provision of nursing care and are therefore particularly vulnerable and at high risk of contracting a HAI. Professionals must ensure a strict practice of hand hygiene to guarantee health care safety. However, low adherence to the practice of hand hygiene is an identified reality [
3,
4].
The WHO ’my five moments for hand hygiene‘ [
2] includes: Moment 1 (before touching a patient), Moment 2 (before a clean or aseptic procedure), Moment 3 (after body fluid exposure risk), Moment 4 (after touching a patient), and Moment 5 (after touching the patient’s surroundings). The WHO guideline also includes hand hygiene technique and the duration of the entire procedure: 20 to 30 seconds for hand hygiene with alcohol-based formulation and 40 to 60 seconds for hand hygiene with soap and water.
The aim of this study is to evaluate the practice of hand hygiene by nurses working in a paediatric ward, during different times in the provision of nursing care.
2. Materials and Methods
We conducted a descriptive cross-sectional study, with a convenience sample consisting of 28 nurses working at a paediatric ward in a hospital located in the continental Portugal territory.
A single auditor trained for the task performed observations of the practice of hand hygiene that took place in October 2021, and used a model form aligned with the recommendations of the WHO [
2] and the Directorate-General for Health of Portugal [
5].
We conducted observations during daytime hours, and assigned a code to the observation forms, ensuring the anonymity of the person performing the procedure. We used the IBM Statistical Package for the Social Sciences (SPSS), version 28.0, (Armonk, NY, USA), to analyse the data. We safeguarded the ethical principles inherent to the research process and requested authorization from the institution’s Ethics Committee.
3. Results and Discussion
The global implementation of the WHO multimodal hand hygiene strategy has strongly contributed to the success of behaviour change worldwide and the consequent reduction of HAI [
6].
We used direct observation by a trained auditor [
2], which is considered the standard gold method for monitoring hand hygiene compliance [
7]. Moreover, observation of the professionals during their work shifts can also contribute to improving their practice [
8].
We observed 224 opportunities for the practice of hand hygiene and, on average, observed each nurse eight times. The analysis of the results highlights that the overall percentage of adherence to the practice of hand hygiene was 91.1%. This result may be associated with the Hawthorne effect, referenced in several studies, since the practice of hand hygiene compliance is higher when the participants are aware of the presence of the observer [
6].
Comparing the current results with another study conducted in 2019 within the same context [
9], we found improvements in what concerns adherence to the practice of hand hygiene by nurses. We conducted the first study before the COVID-19 pandemic; and therefore, we can relate this improvement to behavioural changes imposed during the pandemic and the consequent attention professionals pay to healthcare safety.
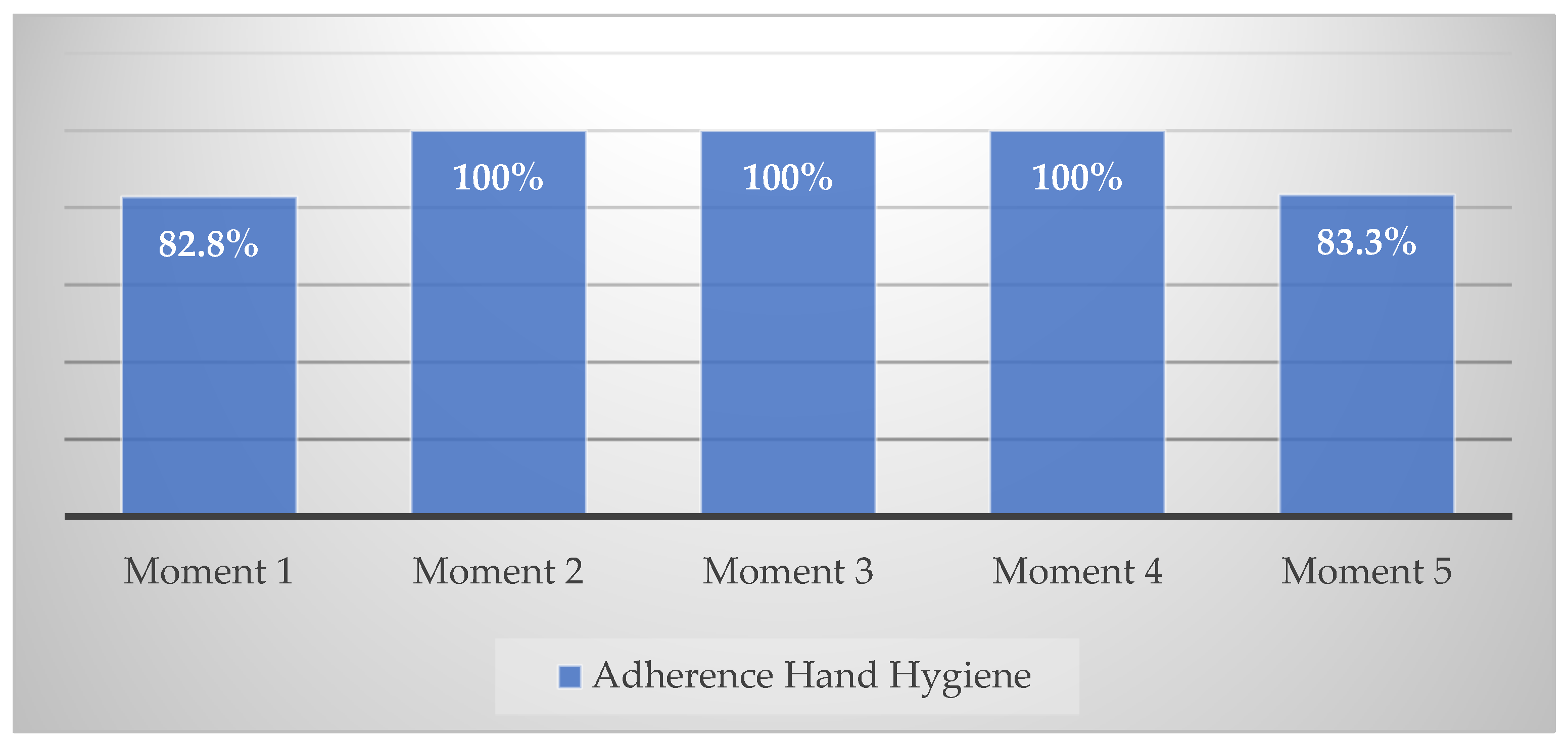
As can be seen in
Figure 1 below, the analysis of the results demonstrates that moment 1 (before touching a patient) registered the lowest adherence (82.8%), followed by moment 5 (after touching the patient surroundings), which registered 83.3%; the other moments registered 100% adherence. Other studies reported lower adherence to the practice of hand hygiene at moment 1 [
4,
10].
Nurses preferred using alcohol-based formulation (72.1%) and a smaller percentage chose to wash their hands with plain soap and water (27.9%). Alcohol-based hand rub is, indeed, the gold standard of hand hygiene [
6].
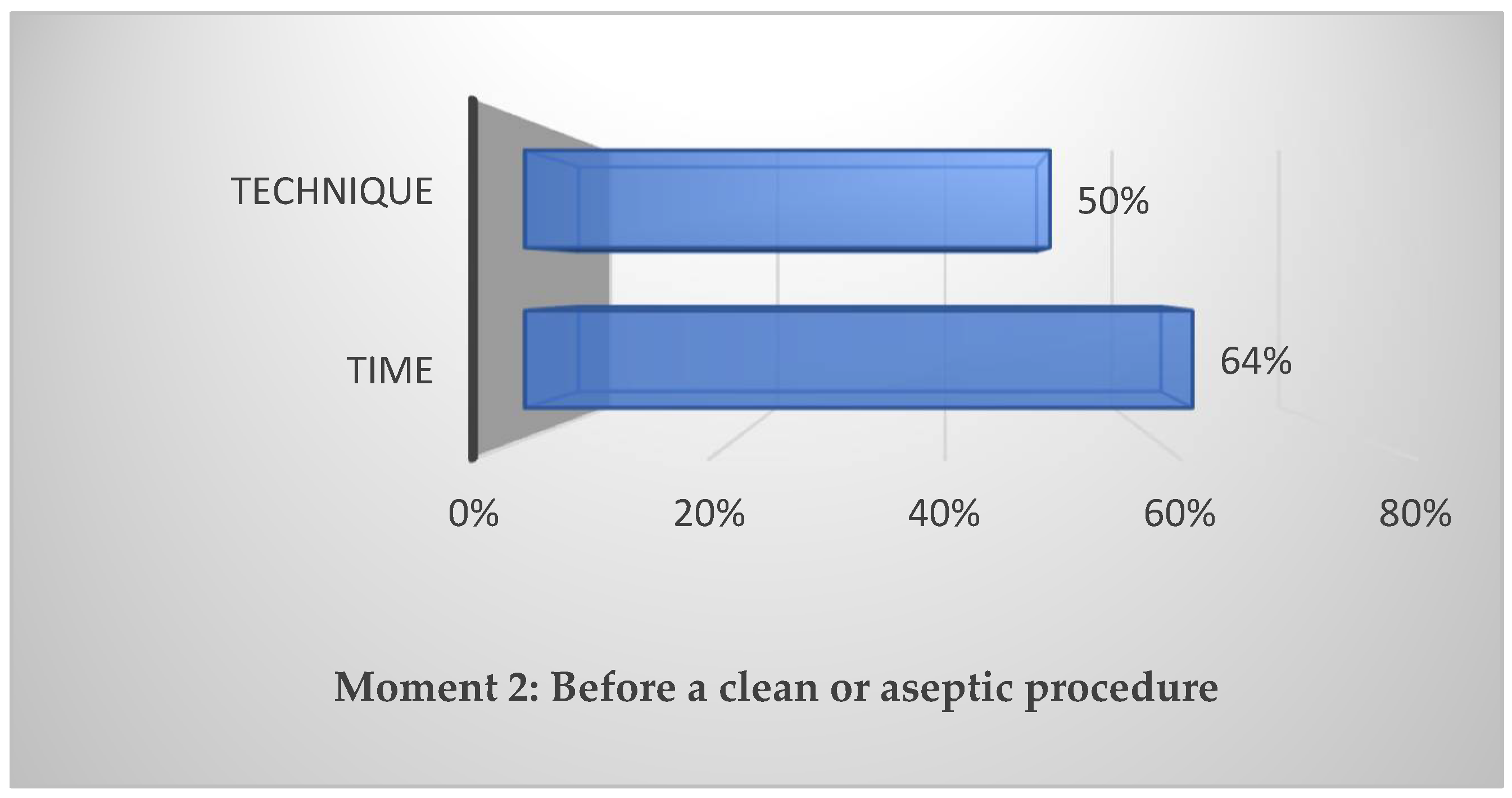
Regarding the hygiene technique and its duration, compliance was low. In 37.3% of the observations, the nurses complied with the hygiene technique recommended by the WHO and the duration of the entire procedure only registered 24% of the observations.
Although the results outperform other studies, for example, a longitudinal study conducted in intensive care units over 3 years [
8], the recommendations suggested by the WHO on the practice of hand hygiene fall short [
2]; particularly noteworthy were non-compliance with time (64%) and hygiene technique before performing aseptic procedures (50%), as shown in
Figure 2. In this situation, the likelihood of transmitting infectious agents is dangerously increased, hence it puts the children’s safety at risk.
The results reveal the need to implement a multimodal strategy to improve and sustain hand hygiene compliance rates among nurses, as recommended in other studies [
3,
4,
7]. In the context under study, we particularly focused the intervention on the hand hygiene technique and its duration.
In the short term, we expect to implement a comprehensive multimodal intervention program, which not only includes the practice of hand hygiene, but also other items of basic precautions that have been the aim of this study.
4. Conclusions
Hand hygiene is still a concern of healthcare institutions and the results of this study highlight the need for intervention in order to increase adherence to the ’five moments‘, and improve hand hygiene techniques and the recommended time for its performance. Hand hygiene improvements contribute to stopping the cross-transmission of potentially infectious microorganisms and hence contribute to preventing HAI. In the near future, we intend to implement a multimodal intervention within the context of healthcare under study, which includes the specificity of hand hygiene, in addition to other items of standard precautions.
Author Contributions
Conceptualization, J.N., C.B. and P.C.; methodology, J.N. and C.B.; software, J.N. and C.B.; validation, C.B.; formal analysis, C.B.; investigation, P.C. and F.M.; writing—original draft preparation, J.N. and P.C.; writing—review and editing, C.B. and J.N.; project administration, C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received external funding by National Funds through FCT—Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020).
Institutional Review Board Statement
The study was carried out in accordance with the Declaration of Helsinki and obtained assent from the Ethics Committee of the host institution (protocol code 265-21 on 30 September 2021).
Informed Consent Statement
We obtained informed consent from all subjects involved in the study.
Data Availability Statement
No special permission is required to reuse all, or part of article published by MDPI, including figures and tables.
Acknowledgments
This article was supported by National Funds through FCT—Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020).
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide; World Health Organization Press: Genève, Switzerland, 2011; Available online: https://www.who.int/publications/i/item/report-on-the-burden-of-endemic-health-care-associated-infection-worldwide (accessed on 30 May 2022).
- World Health Organization. WHO Guidelines on Hand Hygiene in Health Care; World Health Organization Press: Genève, Switzerland, 2009; Available online: https://www.who.int/publications/i/item/9789241597906 (accessed on 30 May 2022).
- Corrêa, I.; Nunes, I. Higienización de las manos: el cotidiano del profisional de la salud en una unidad de internación pediátrica. Invest. Educ. Enferm. 2011, 29, 54–60. [Google Scholar]
- Abed, N.T.; Eldesouky, R.S. Infection Control: Hand Hygiene Practices among Nurses in the Neonatal Intensive Care Unit at Benha University Hospital. Egypt. J. Hosp. Med. 2020, 80, 619–626. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde. Norma 7/2019 Higiene das mãos nas unidades de saúde. Direção Geral da Saúde, 2019. Available online: https://normas.dgs.min-saude.pt/wp-content/uploads/2019/10/higiene-das-maos-nas-unidades-de-saude.pdf (accessed on 30 May 2022).
- Lotfinejad, N.; Peters, A.; Tartari, E.; Fankhauser-Rodriguez, C.; Pires, D.; Pittet, D. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect. Dis. 2021, 21, e209–e221. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M. Electronic monitoring in combination with direct observation as a means to significantly improve hand hygiene compliance. Am. J. Infect. Control 2017, 45, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Gur, R.; Bharara, T.; Duggal, S.; Chugh, V. Evaluation of hand hygiene compliance over the years, in an intensive care unit of a north Delhi hospital preparing for accreditation: A 3-year study. J. Fam. Med. Prim. Care 2020, 9, 1939–1943. [Google Scholar] [CrossRef] [PubMed]
- Campos, P. Higiene das Mãos na Segurança da Criança Hospitalizada. Master’s Thesis, Escola Superior de Enfermagem do Porto, Porto, Portugal, 2020. Unpublished. [Google Scholar]
- Suzuki, Y.; Morino, M.; Morita, I.; Yamamoto, S. The effect of a 5-year hand hygiene initiative based on the WHO multimodal hand hygiene improvement strategy: An interrupted time-series study. Antimicrob. Resist. Infect. Control 2020, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
{kind=link}

