
Persistence of Second and Third-Line Biologics in Inflammatory Bowel Disease: A Multi-Centre Cohort Study

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
Statistical Analysis
3. Results
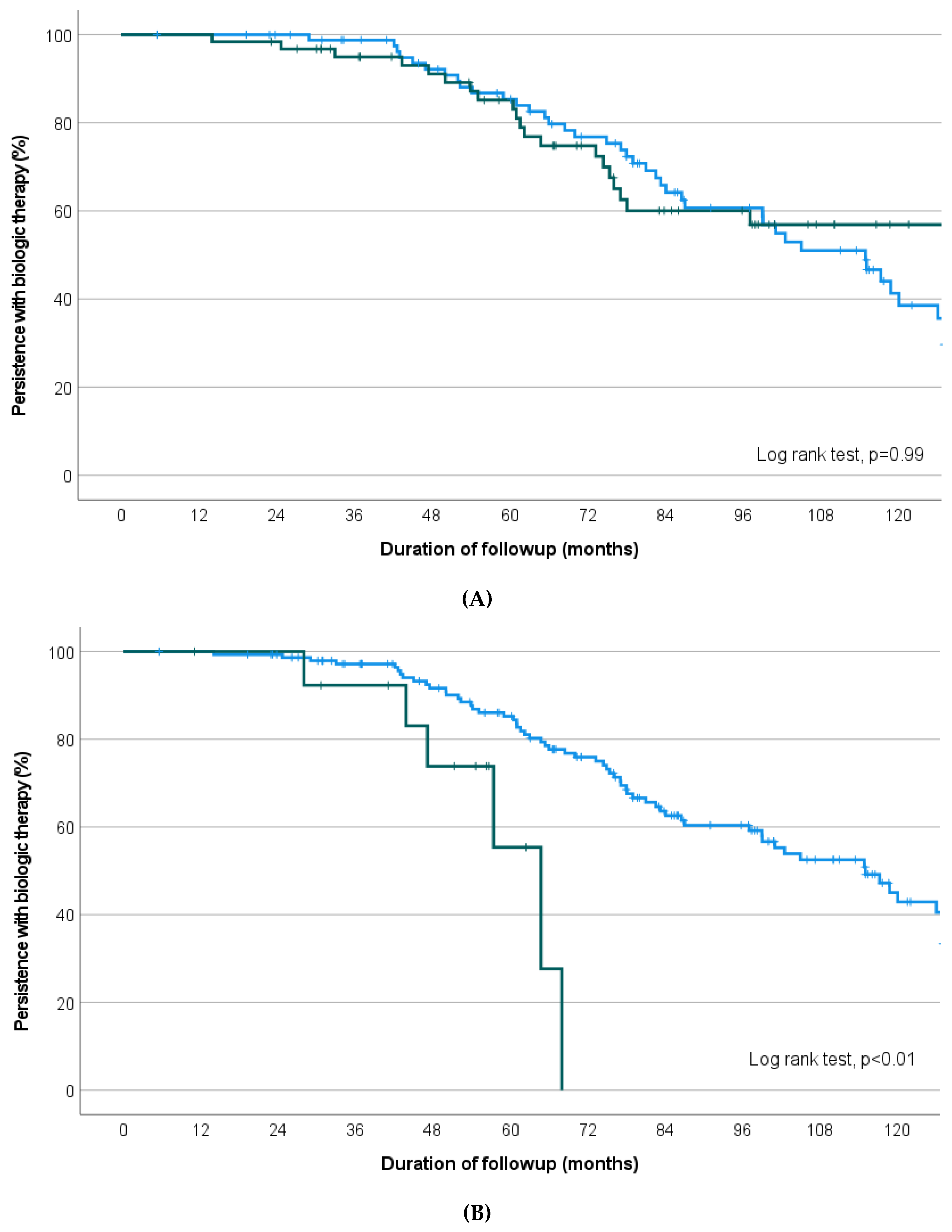
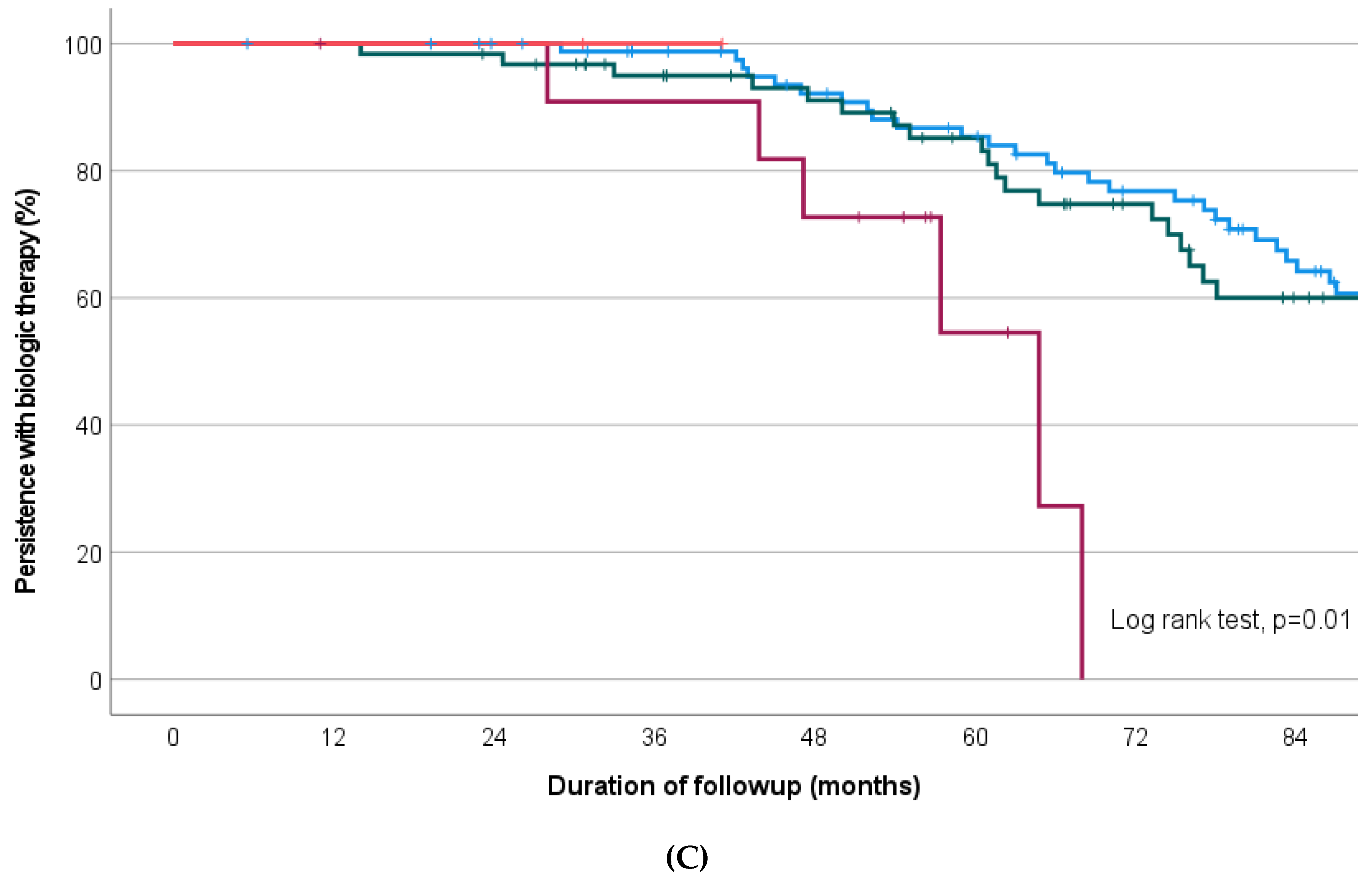
3.1. Choice of Biologic Order on Overall Therapy Persistence
3.2. Factors Associated with Treatment Persistence
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ungaro, R.; Colombel, J.-F.; Lissoos, T.; Peyrin-Biroulet, L. A Treat-to-Target Update in Ulcerative Colitis: A Systematic Review. Am. J. Gastroenterol. 2019, 114, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.-F.; D’haens, G.; Lee, W.-J.; Petersson, J.; Panaccione, R. Outcomes and Strategies to Support a Treat-to-target Approach in Inflammatory Bowel Disease: A Systematic Review. J. Crohn’s Colitis 2019, 14, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Roda, G.; Jharap, B.; Neeraj, N.; Colombel, J.-F. Loss of Response to Anti-TNFs: Definition, Epidemiology, and Management. Clin. Transl. Gastroen. 2016, 7, e135. [Google Scholar] [CrossRef] [PubMed]
- Mitrev, N.; Casteele, N.V.; Seow, C.H.; Andrews, J.M.; Connor, S.J.; Moore, G.T.; Barclay, M.; Begun, J.; Bryant, R.; Chan, W.; et al. Review article: Consensus statements on therapeutic drug monitoring of anti-tumour necrosis factor therapy in inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2017, 46, 1037–1053. [Google Scholar] [CrossRef] [PubMed]
- Privitera, G.; Pugliese, D.; Lopetuso, L.R.; Scaldaferri, F.; Neri, M.; Guidi, L.; Gasbarrini, A.; Armuzzi, A. Novel trends with biologics in inflammatory bowel disease: Sequential and combined approaches. Ther. Adv. Gastroenter. 2021, 14, 17562848211006668. [Google Scholar] [CrossRef]
- Ding, N.S.; Hart, A.; Cruz, P.D. Systematic review: Predicting and optimising response to anti-TNF therapy in Crohn’s disease—Algorithm for practical management. Aliment. Pharmacol. Ther. 2016, 43, 30–51. [Google Scholar] [CrossRef]
- Singh, S.; George, J.; Boland, B.S.; Casteele, N.V.; Sandborn, W.J. Primary Non-Response to Tumor Necrosis Factor Antagonists is Associated with Inferior Response to Second-line Biologics in Patients with Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. J. Crohn’s Colitis 2018, 12, 635–643. [Google Scholar] [CrossRef]
- Yanai, H.; Hanauer, S.B. Assessing Response and Loss of Response to Biological Therapies in IBD. Am. J. Gastroenterol. 2011, 106, 685–698. [Google Scholar] [CrossRef]
- Ben-Horin, S.; Chowers, Y. Review article: Loss of response to anti-TNF treatments in Crohn’s disease. Aliment. Pharmacol. Ther. 2011, 33, 987–995. [Google Scholar] [CrossRef]
- Singh, S.; Fumery, M.; Sandborn, W.J.; Murad, M.H. Systematic review and network meta-analysis: First- and second-line biologic therapies for moderate-severe Crohn’s disease. Aliment. Pharmacol. Ther. 2018, 48, 394–409. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Marín, A.C.; McNicholl, A.G.; Chaparro, M. Systematic review with meta-analysis: The efficacy of a second anti-TNF in patients with inflammatory bowel disease whose previous anti-TNF treatment has failed. Aliment. Pharmacol. Ther. 2015, 41, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Fasanmade, A.A.; Adedokun, O.J.; Olson, A.; Strauss, R.; Davis, H.M. Serum albumin concentration: A predictive factor of infliximab pharmacokinetics and clinical response in patients with ulcerative colitis. Int. J. Clin. Pharmacol. Ther. 2010, 48, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Fasanmade, A.A.; Adedokun, O.J.; Ford, J.; Hernandez, D.; Johanns, J.; Hu, C.; Davis, H.M.; Zhou, H. Population pharmacokinetic analysis of infliximab in patients with ulcerative colitis. Eur. J. Clin. Pharmacol. 2009, 65, 1211–1228. [Google Scholar] [CrossRef] [PubMed]
- Brandse, J.F.; van den Brink, G.R.; Wildenberg, M.E.; van der Kleij, D.; Rispens, T.; Jansen, J.M.; Mathôt, R.A.; Ponsioen, C.Y.; Löwenberg, M.; D’Haens, G.R.A.M. Loss of Infliximab Into Feces Is Associated With Lack of Response to Therapy in Patients With Severe Ulcerative Colitis. Gastroenterology 2015, 149, 350–355.e2. [Google Scholar] [CrossRef] [PubMed]
- Choy, M.C.; Seah, D.; Gorelik, A.; An, Y.; Chen, C.; Macrae, F.A.; Sparrow, M.P.; Connell, W.R.; Moore, G.T.; Radford-Smith, G.; et al. Predicting response after infliximab salvage in acute severe ulcerative colitis. J. Gastroenterol. Hepatol. 2018, 33, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Choy, M.C.; Seah, D.; Faleck, D.M.; Shah, S.C.; Chao, C.-Y.; An, Y.-K.; Radford-Smith, G.; Bessissow, T.; Dubinsky, M.C.; Ford, A.C. Systematic Review and Meta-analysis: Optimal Salvage Therapy in Acute Severe Ulcerative Colitis. Inflamm. Bowel Dis. 2019, 25, 1169–1186. [Google Scholar] [CrossRef] [PubMed]
- Gibson, D.J.; Heetun, Z.S.; Redmond, C.E.; Nanda, K.S.; Keegan, D.; Byrne, K.; Mulcahy, H.E.; Cullen, G.; Doherty, G.A. An Accelerated Infliximab Induction Regimen Reduces the Need for Early Colectomy in Patients With Acute Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2015, 13, 330–335.e1. [Google Scholar] [CrossRef]
- An, Y.; Chen, C.; White, L.; Howlett, M.; Lord, A.; Radford-Smith, G. Accelerated dosing of infliximab induction and endoscopic mucosal healing in patients with acute severe ulcerative colitis. J. Gastroenterol. Hepatol. 2017, 32, 121–154. [Google Scholar] [CrossRef]
- Louis, E.; Ghoul, Z.E.; Vermeire, S.; Dall’Ozzo, S.; Rutgeerts, P.; Paintaud, G.; Belaiche, J.; de Vos, M.; van Gossum, A.; Colombel, J.-F.; et al. Association between polymorphism in IgG Fc receptor IIIa coding gene and biological response to infliximab in Crohn’s disease. Aliment. Pharmacol. Ther. 2004, 19, 511–519. [Google Scholar] [CrossRef]
- Louis, E.J.; Watier, H.E.; Schreiber, S.; Hampe, J.; Taillard, F.; Olson, A.; Thorne, N.; Zhang, H.; Colombel, J.-F. Polymorphism in IgG Fc receptor gene FCGR3A and response to infliximab in Crohn’s disease: a subanalysis of the ACCENT I study. Pharmacogenet. Genom. 2006, 16, 911–914. [Google Scholar] [CrossRef]
- Louis, E.; Ribbens, C.; Godon, A.; Franchimont, D.; Groote, D.D.; Hardy, N.; Boniver, J.; Belaiche, J.; Malaise, M. Increased production of matrix metalloproteinase-3 and tissue inhibitor of metalloproteinase-1 by inflamed mucosa in inflammatory bowel disease. Clin. Exp. Immunol. 2000, 120, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Cleynen, I.; Vermeire, S. Paradoxical inflammation induced by anti-TNF agents in patients with IBD. Nat. Rev. Gastroenterol. 2012, 9, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Zator, Z.A.; Silva P de Nguyen, D.D.; Korzenik, J.; Yajnik, V.; Ananthakrishnan, A.N. Older age is associated with higher rate of discontinuation of anti-TNF therapy in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2012, 19, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Lobatón, T.; Ferrante, M.; Rutgeerts, P.; Ballet, V.; Assche, G.V.; Vermeire, S. Efficacy and safety of anti-TNF therapy in elderly patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2015, 42, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Roblin, X. Letter: Immunogenicity of anti-TNF in elderly IBD patients. Aliment. Pharmacol. Ther. 2019, 50, 336. [Google Scholar] [CrossRef]
- Pawelec, G. Age and immunity: What is “immunosenescence”? Exp. Gerontol. 2018, 105, 4–9. [Google Scholar] [CrossRef]
- Grimm, I.S.; Friedman, L.S. Inflammatory bowel disease in the elderly. Gastroenterol. Clin. N. Am. 1990, 19, 361–389. [Google Scholar] [CrossRef]
- Riegler, G.; Tartaglione, M.T.; Carratú, R.; D’incá, R.; Valpiani, D.; Russo, M.I.; Papi, C.; Fiorentini, M.T.; Ingrosso, M.; Andreoli, A.; et al. Age-Related Clinical Severity at Diagnosis in 1705 Patients with Ulcerative Colitis. Dig. Dis. Sci. 2000, 45, 462–465. [Google Scholar] [CrossRef]
- Del Val, J.H. Old-age inflammatory bowel disease onset: A different problem? World J. Gastroenterol. 2011, 17, 2734–2739. [Google Scholar] [CrossRef]
- Heresbach, D.; Alexandre, J.-L.; Bretagne, J.-F.; Cruchant, E.; Dabadie, A.; Dartois-Hoguin, M.; Girardot, P.-M.; Jouanolle, H.; Kerneis, J.; Le Verger, J.-C.; et al. Crohn’s disease in the over-60 age group. Eur. J. Gastroenterol. Hepat. 2004, 16, 657–664. [Google Scholar] [CrossRef]
- Freeman, H.J. Age-Dependent Phenotypic Clinical Expression of Crohn’s Disease. J. Clin. Gastroenterol. 2005, 39, 774–777. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Stitt, L.W.; Zou, G.; Khanna, R.; Dulai, P.S.; Sandborn, W.J.; Feagan, B.G.; Jairath, V. Early combined immunosuppression may be effective and safe in older patients with Crohn’s disease: Post hoc analysis of REACT. Aliment. Pharmacol. Ther. 2019, 49, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Scott, F.I.; Lichtenstein, G.R. Therapeutic Drug Monitoring of Anti-TNF Therapy in Inflammatory Bowel Disease. Curr. Treat. Options Gastroenterol. 2014, 12, 59–75. [Google Scholar] [CrossRef] [PubMed]
- Reinhold, I.; Blümel, S.; Schreiner, J.; Boyman, O.; Bögeholz, J.; Cheetham, M.; Rogler, G.; Biedermann, L.; Scharl, M. Clinical Relevance of Anti-TNF Antibody Trough Levels and Anti-Drug Antibodies in Treating Inflammatory Bowel Disease Patients. Inflamm. Intest. Dis. 2021, 6, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Adedokun, O.J.; Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Xu, Z.; Marano, C.W.; Johanns, J.; Zhou, H.; Davis, H.M.; Cornillie, F.; et al. Association between Serum Concentration of Infliximab and Efficacy in Adult Patients with Ulcerative Colitis. Gastroenterology 2014, 147, 1296–1307.e5. [Google Scholar] [CrossRef]
- Paul, S.; Moreau, A.C.; Tedesco, E.D.; Rinaudo, M.; Phelip, J.-M.; Genin, C.; Peyrin-Biroulet, L.; Roblin, X. Pharmacokinetics of Adalimumab in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2014, 20, 1288–1295. [Google Scholar] [CrossRef]
- D’Arcangelo, G.; Imondi, C.; Terrin, G.; Catassi, G.; Aloi, M. Is Fecal Calprotectin a Useful Marker for Small Bowel Crohn’s Disease? J. Pediatr. Gastroenterol. Nutr. 2021, 73, 242–246. [Google Scholar] [CrossRef]
- Ye, L.; Cheng, W.; Chen, B.; Lan, X.; Wang, S.; Wu, X.; Huang, W.; Wang, F.-Y. Levels of Faecal Calprotectin and Magnetic Resonance Enterocolonography Correlate with Severity of Small Bowel Crohn’s Disease: A Retrospective Cohort Study. Sci. Rep. 2017, 7, 1970. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. 3), s1–s106. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N = (%) 1 |
|---|---|
| Age at diagnosis (median (range) (y)) | 26.19 (3.6, 83.7) |
| Male sex | 92 (51%) |
| Crohn’s disease as diagnosis | 134 (75%) |
| Duration since diagnosis at first biologic commencement (median [range] (y)) | 4.9 (0, 37.4) |
| Current smoker at first biologic commenced | 44 (35%) |
| Prior IBD related surgical intervention(s) | 58 (40%) |
| Serum CRP at baseline (mg/L, median, (range) (y)) | 5.4 (1, 180) |
| Serum albumin at first biologic (g/L, median, range (y)) | 36 (18, 47) |
| Faecal calprotectin >200 (µg/mL) at baseline | 28 (64%) |
| Variable | Biologic 1 n = 179 (%) | Biologic 2 n = 162 (%) | Biologic 3 n = 53 (%) | p Value |
|---|---|---|---|---|
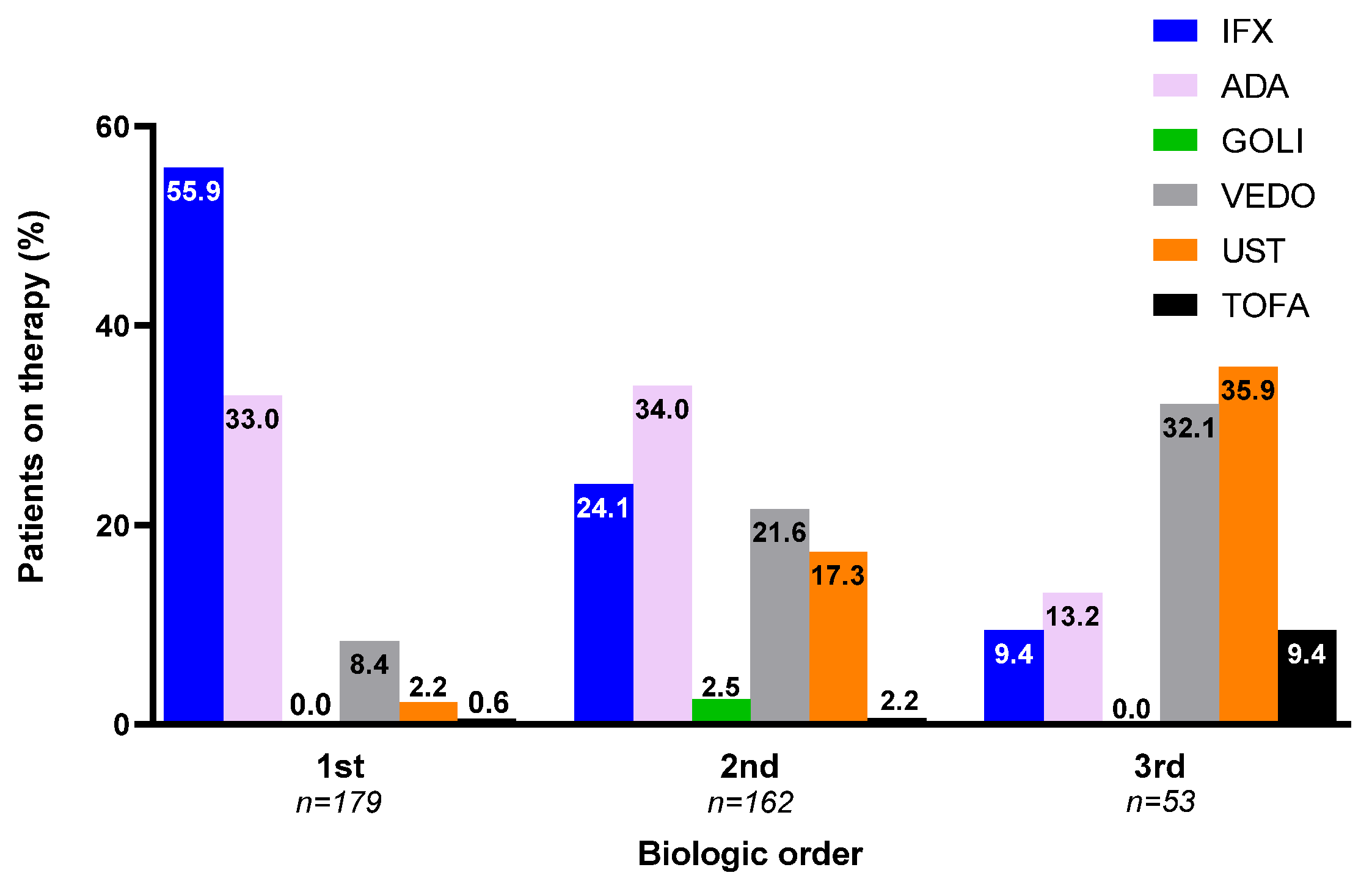
| Anti-TNF biologic Infliximab Adalimumab Golimumab | 159 (88.8) 100 (55.9) 59 (33.0) 0 (0.0) | 98 (60.5) 39 (24.1) 55 (34.0) 4 (2.5) | 12 (22.6) 5 (9.4) 7(13.2) 0 (0.0) | * * ns ns |
| Non-anti-TNF biologic/agent Vedolizumab Ustekinumab Tofacitinib | 20 (12.2) 15 (8.4) 4 (2.2) 1 (0.6) | 64 (39.5) 35 (21.6) 28 (17.3) 1 (0.6) | 41 (77.4) 17 (32.1) 19 (35.9) 5 (9.4) | * * * ns |
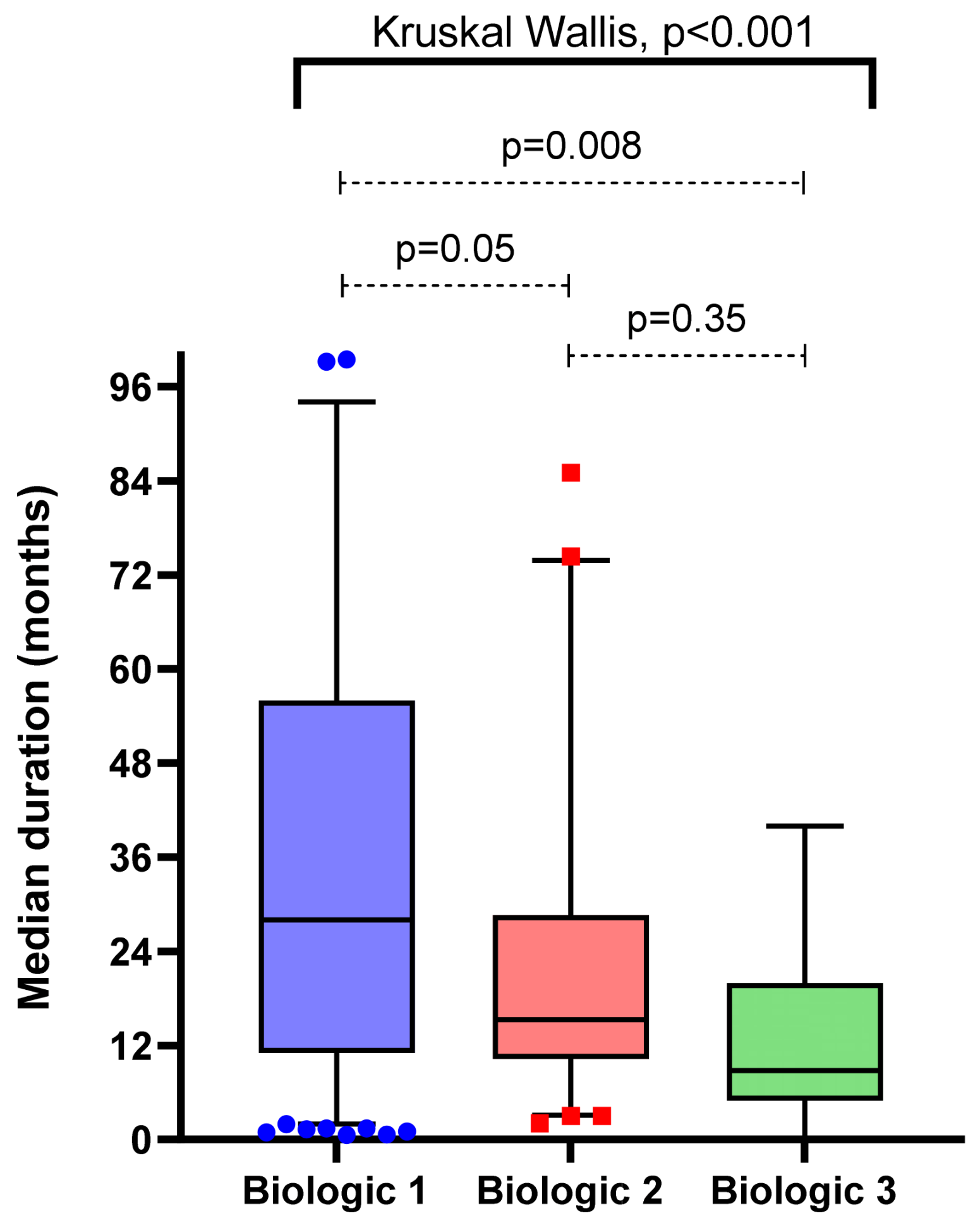
| Median duration of therapy (range, months) Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 26.1 (0.6, 152.7) 28.0 (0.6, 152.7) 19.4 (8.0, 44.4) | 29.1 (2.0, 193.1) 36.7 (2.0, 193.1) 24.7 (5.5, 70.5) | 20.0 (0.1, 71.9) 30.0 (8.0, 58.8) 16.1 (0.1, 71.9) | ns ns ns |
| Cessation due to primary non-response Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 44 (24.6) 38 (23.9) 6 (30.0) | 15 (8.4) 7 (7.1) 8 (12.5) | 2 (1.1) 0 (0.0) 2 (4.9) | * * * |
| Cessation due to non-disease related reasons Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 49 (27.4) 48 (33.3) 1 (7.7) | 12 (20.3) 9 (23.1) 3 (15.0) | 2 (4.3) 1 (10.0) 1 (2.8) | * * ns |
| Therapeutic drug level achieved during therapy Anti-TNF biologic only | 41 (56.9) | 20 (54.1) | 2 (50.0) | ns |
| Objectively demonstrated biologic failure Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 97 (54.2) 88 (55.3) 9 (45.0) | 120 (67.0) 83 (84.7) 37 (57.8) | 60 (33.5) 8 (66.7) 20 (48.8) | ns ns ns |
| Pharmacodynamic failure Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 73 (40.8) 67 (42.1) 6 (30.0) | 37 (20.7) 27 (27.6) 10 (15.6) | 5 (2.8) 3 (25.0) 2 (4.9) | * ns * |
| Endoscopic remission achieved during therapy Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 38 (34.5) 34 (36.6) 4 (23.5) | 68 (45.6) 49 (53.8) 19 (32.8) | 45 (42.5) 5 (62.5) 12 (38.7) | ns * ns |
| Surgical resection during therapy Overall Anti-TNF biologic Non-anti-TNF biologic/agent | 5 (4.6) 5 (5.6) 0 (0.0) | 8 (8.5) 6 (12.0) 2 (4.5) | 7 (36.8) 1 (14.3) 5 (35.7) | * ns * |
| Variable | Odds Ratio [95% CI] | p Value |
|---|---|---|
| Age at IBD diagnosis (per y increase) | 0.97 [0.94, 0.998] | 0.04 |
| Crohn’s disease as diagnosis | 7.1 [2.3, 21.7] | <0.01 |
| Primary non-response to first biologic therapy | 0.3 [0.1, 0.7] | <0.01 |
| Endoscopic remission achieved with first biologic therapy | 10.4 [1.3, 79.9] | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanrahan, T.P.; Chan, R.; Tassone, D.; Ding, N.S.; Basnayake, C.; Schulberg, J.; Vasudevan, A.; Kamm, M.; De Gregorio, M.; van Langenberg, D.R.; et al. Persistence of Second and Third-Line Biologics in Inflammatory Bowel Disease: A Multi-Centre Cohort Study. Future Pharmacol. 2022, 2, 669-680. https://doi.org/10.3390/futurepharmacol2040041
Hanrahan TP, Chan R, Tassone D, Ding NS, Basnayake C, Schulberg J, Vasudevan A, Kamm M, De Gregorio M, van Langenberg DR, et al. Persistence of Second and Third-Line Biologics in Inflammatory Bowel Disease: A Multi-Centre Cohort Study. Future Pharmacology. 2022; 2(4):669-680. https://doi.org/10.3390/futurepharmacol2040041
Chicago/Turabian StyleHanrahan, Timothy P., Robbie Chan, Daniel Tassone, Nik S. Ding, Chamara Basnayake, Julien Schulberg, Abhinav Vasudevan, Michael Kamm, Michael De Gregorio, Daniel R. van Langenberg, and et al. 2022. "Persistence of Second and Third-Line Biologics in Inflammatory Bowel Disease: A Multi-Centre Cohort Study" Future Pharmacology 2, no. 4: 669-680. https://doi.org/10.3390/futurepharmacol2040041
APA StyleHanrahan, T. P., Chan, R., Tassone, D., Ding, N. S., Basnayake, C., Schulberg, J., Vasudevan, A., Kamm, M., De Gregorio, M., van Langenberg, D. R., & Niewiadomski, O. (2022). Persistence of Second and Third-Line Biologics in Inflammatory Bowel Disease: A Multi-Centre Cohort Study. Future Pharmacology, 2(4), 669-680. https://doi.org/10.3390/futurepharmacol2040041