1. Introduction
Oral health is a critical component of overall health and well-being, yet it remains largely overlooked in many low- to middle-income countries due to a confluence of factors including limited resources, inadequate dental infrastructure, and a general lack of awareness about its significance. Such disparities in access to dental care can have a profound impact on community health, necessitating innovative approaches to bridge these gaps. International dental outreach camps have emerged as a vital intervention in this regard, providing essential dental services to underserved communities and offering a platform for dental volunteers to enhance their skills and understanding of global dental health challenges [
1,
2].
Zanzibar, with its rich historical and cultural ties to the Sultanate of Oman, was chosen as the location for these dental outreach initiatives by a dental institution based in Oman, to which the authors of this paper are affiliated. This partnership was inspired by a shared history and a mutual recognition of Zanzibar’s unmet dental care needs, mirroring the broader challenges faced by low- to middle-income areas. The region’s struggle with limited dental care access provides a poignant backdrop for such initiatives, with both entities committed to addressing this gap [
3,
4].
The oral health situation in Zanzibar, similar to the broader Tanzanian context, is characterized by a low prevalence of dental care programs, limited availability of free dental care, and a lack of preventive programs [
4]. Recent reports by the World Health Organization (WHO) and additional assessments across African regions have consistently highlighted a relatively low incidence of dental caries in Tanzania. Intriguingly, residents in urban areas exhibit a significantly reduced likelihood of experiencing dental caries compared to their rural counterparts [
3]. This marks a notable shift from the situation 25 years ago [
4], underscoring the current focus of dental care initiatives predominantly in urban locales. This trend has inadvertently widened the gap in dental care access for rural areas, including Zanzibar, leading to elevated levels of untreated dental caries. Particularly, the prevalence of dental caries in primary teeth remains alarmingly high [
4]. A substantial majority of these are decayed teeth, far outnumbering those that are filled or missing, thereby spotlighting a significant deficiency in available dental treatment.
In response, the dental outreach camps organized in 2019 and 2023 were designed to provide immediate dental care to the Zanzibar community and enrich the practical experience of volunteering students from the Oman-based institution. These initiatives encompassed a broad spectrum of services and educational activities, meticulously crafted to elevate oral health standards in the region. Through these dedicated efforts, the outreach aimed to forge a lasting positive change within Zanzibar’s oral health scenario and simultaneously enhance the educational voyage of its participants.
To plan for effective clinical prevention and management of dental issues, as well as to recognize the strides made in oral health, comprehensive reports on dental health problems and their distribution within determinative populations, such as that of Zanzibar, are indispensable. Therefore, this study aimed to scrutinize the oral health outcomes stemming from the international dental outreach endeavors in Zanzibar, Tanzania over two periods: 2019 and 2023. By delving into the effects of these programs on the community’s dental health, this research seeks to highlight observable trends and shifts across a four-year span. The analysis of these developments is essential, providing insight into the dynamic landscape of dental health issues and the effectiveness of implemented interventions. This study lays the groundwork for developing future outreach models and health policies, designed to address the evolving dental health needs of the community.
2. Materials and Methods
This observational study involved a cross-sectional analysis of oral health data collected from dental outreach camps on the island of Unguja, part of Zanzibar, Tanzania. The first camp was held in July 2019 and the second in July 2023.
Participants included 224 pupils in 2019 and 354 pupils in 2023, from local schools in the region. These pupils were within the age groups of preschool and school-aged children (3–10 years) and adolescents and teens (11–17 years). The inclusion criteria encompassed all pupils present during the dental camps that were willing to participate. The dental examinations were carried out by a team of qualified dental professionals and students from a dental school, where the authors of this paper are affiliated.
Prior to the outreach, the team underwent a calibration process to ensure uniformity and accuracy in their diagnostic and treatment methods. The dental examinations utilized mobile dental chairs equipped with light sources, allowing for comprehensive assessments. Each examination was facilitated using a complete set of dental examination kits, inclusive of all necessary instruments. To maintain the highest standards of hygiene and patient safety, all instruments were sterilized using autoclaving before their use on each patient. In addition to this, strict cross-infection control protocols were followed, with team members donning new disposable gloves, gowns, and masks for each patient examination to prevent any potential cross-contamination. This meticulous approach ensured the delivery of effective, safe, and high-quality dental care to the community members.
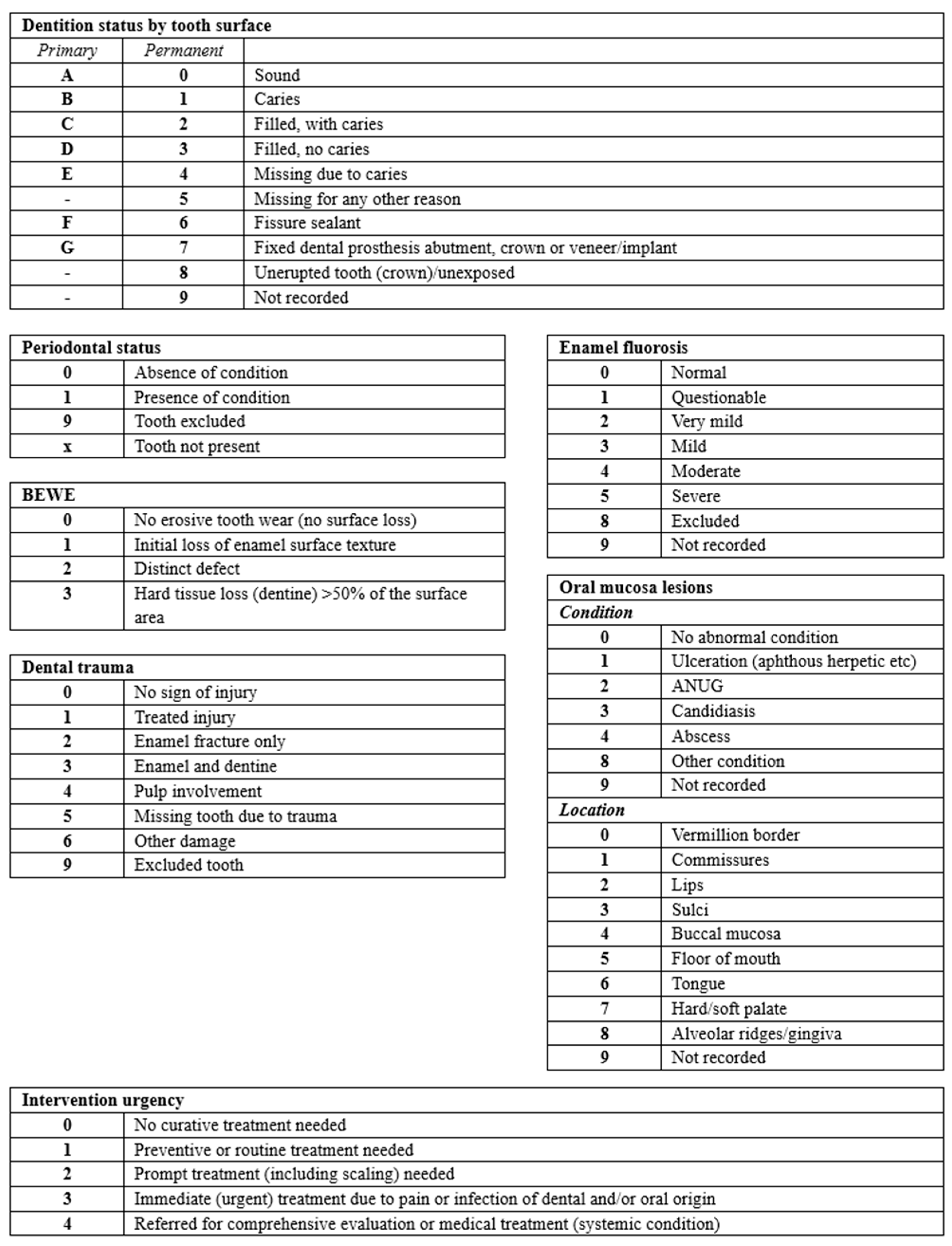
The dental health assessment encompassed a range of parameters, including the prevalence of dental caries, the number of teeth missing due to caries, the number of filled teeth, the DMFT (Decayed, Missing, and Filled Teeth) and dmft (decayed, missing, and filled teeth in primary dentition) indices, enamel fluorosis, dental trauma, oral mucosa lesions, and non-carious tooth surface loss (measured using the Basic Erosive Wear Examination, or BEWE, index). The examinations also recorded the urgency of required dental interventions.
In both the 2019 and 2023 dental camps, we employed a standardized data collection method using a validated dental chart, informed by the WHO Oral Health Assessment Form for Children. This tool facilitated a uniform and precise recording of clinical findings, which is essential for the consistent assessment of dental health and comparison across the two campaigns [
3]. For an in-depth view of the dental chart employed in this study, see
Appendix A. Initial assessments that included height, weight, and waist measurements were part of a comprehensive health evaluation. However, these anthropometric data were not analyzed or included in the study’s results, which concentrated exclusively on dental health outcomes.
For both the 2019 and 2023 data, the collected information was recorded and analyzed. This involved classifying and quantifying instances of dental caries, trauma, fluorosis, and non-carious tooth surface loss, along with calculating the DMFT and dmft indices. Statistical analysis was meticulously performed using GraphPad Prism version 9. The analysis aimed to identify patterns, trends, and changes in dental health over the four-year period. In our analysis, the Chi-square test was used to determine statistical significance across various dental health categories. A p-value of less than 0.05 was considered indicative of a statistically significant difference.
The study was conducted with full ethical clearance, provided by the involved dental school and the Ministry of Health in the region where the outreach activities took place. This ensured adherence to the highest ethical standards and compliance with both institutional and national research guidelines. All procedures involving human participants were in line with the ethical standards of the research committee and conformed to the principles of the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study, ensuring their voluntary participation and understanding of the research. Parental or guardian consent was secured for all minor participants, in addition to assent from the minors themselves. The consent forms, signed by the minors’ guardians or parents, affirmed their informed agreement to partake in the study.
3. Results
In the comparison of dental health data from outreach camps in 2019 and 2023, several notable trends and statistical significances were observed across various categories (
Table 1). The gender ratio was skewed towards females, with a distribution of 57.6% females and 42.4% males, a flip from the slight male predominance observed in 2019. In the 2023 outreach visit, the exploration into oral health disparities across different age demographics sheds light on a pivotal transition in dental health patterns.
A remarkable decrease in dental caries was observed among adolescents and teens, dropping from 62.5% to 35.59% (p < 0.0001). This significant reduction indicates a positive change in oral health among this age group. In contrast, the decrease in caries among preschool and school-aged children was more modest, from 51.78% to 48.59% (p > 0.05), suggesting a slower rate of improvement in this younger demographic.
Both adolescents and teens (p < 0.0001) and preschool/school-aged children (p = 0.004) showed substantial decreases in missing teeth due to caries, with the current rates standing at 9.04% and 11.86%, a marked decline from the 40.2% and 25.89% recorded in the prior survey, indicating improvements in dental health and possibly the effectiveness of preventive measures.
The dmft index, which focuses on primary teeth, showed a slight decrease from 3.80 in 2019 to 3.76 in 2023. This minor change indicates a relatively stable condition of dental health in younger children, with only a slight improvement over the four-year period. On the other hand, the DMFT index, which assesses permanent teeth, exhibited a more notable decrease, dropping from 3.05 in 2019 to 1.95 in 2023. This reduction in the DMFT score suggests improvements in the oral health of the older population, indicating fewer decayed, missing, and filled permanent teeth. These changes in the DMFT and dmft indices highlight the varying degrees of progress in dental health across different age groups within the community, underscoring the effectiveness of dental health interventions and the need for continued focus on both preventive and curative dental care.
Non-carious tooth surface loss presented an area of concern, with significant increases in BEWE = 2 cases from 1.8% to 6.8% (p > 0.05) and BEWE = 1 cases from 48.2% to 61% (p = 0.044). Conversely, cases with no signs of non-carious tooth loss decreased from 48.2% to 33.3% (p = 0.016), underscoring an escalation in non-carious tooth surface loss over the years.
The shift in intervention urgency was notable, with no cases in 2023 requiring ‘Curative Treatment’ as opposed to 15.2% in 2019 (p < 0.0001). There was also a marked increase in cases needing ‘Preventive or Routine Treatment’ from 29.5% to an overwhelming majority, 77% (p > 0.05), alongside a decrease in ‘Prompt Treatment’ from 35.7% to 23% (p = 0.008).
In the realms of enamel fluorosis, dental trauma, and oral mucosa lesions, the data did not show significant statistical differences across the years. In enamel fluorosis, the presence of ‘No Signs’, ‘Mild Fluorosis’, and ‘Moderate Fluorosis’ remained relatively unchanged (p > 0.05). Similarly, for dental trauma, no significant changes were observed in the absence of signs, enamel fractures, and treated injuries. In the case of oral mucosa lesions, while changes in the buccal mucosa and alveolar ridge/gum were not significant (p > 0.05), a notable difference was observed in tongue lesions (p = 0.029).
A chi-square test was conducted to see if there is a significant association between gender and the presence of dental problems. However, there was no statistically significant difference (
p > 0.05).
Table 1 presents a detailed overview of the changes in various dental health indicators, including gender distribution, dental caries prevalence in different age groups, missing teeth due to caries, DMFT and dmft indices, non-carious tooth surface loss (BEWE scores), intervention urgency, and conditions such as enamel fluorosis, dental trauma, and oral mucosa lesions.
4. Discussion
The findings of our study illuminate the evolving dental health landscape in Zanzibar, with notable trends that mirror broader national patterns as well as highlight the unique challenges faced by this rural community. Our analysis revealed a significant decline in dental caries among adolescents and teens, from 62.5% in 2019 to 35.59% in 2023, suggesting a positive shift towards improved oral health in these age groups. This decrease is particularly encouraging as it indicates the potential effectiveness of preventive and educational outreach efforts aimed at younger populations. Furthermore, the reduction in the number of teeth missing due to caries reinforces the importance of early intervention and regular dental care in preventing severe dental problems.
However, the increasing incidence of non-carious tooth surface loss underscores emerging oral health challenges that may not have been previously prioritized. This trend prompts a reassessment of current dental health strategies to address the multifaceted nature of oral health issues, including those beyond caries and tooth loss.
The comparison of 2023 dental outreach data with that of 2019 also highlights a distinct constancy in specific aspects of oral health in Zanzibar over the four-year interval. Particularly in the categories of enamel fluorosis, dental trauma, and oral mucosa lesions, a close alignment between the data of the two years is evident. The steady figures in enamel fluorosis underscore a sustained, unchanged impact over the years, with no significant rise or fall in the individuals reporting no signs of fluorosis, and a comparable distribution in mild and moderate cases. This trend is mirrored in the data for dental trauma, where the incidences of enamel fractures and treated injuries show minimal fluctuation from the 2019 statistics, indicating a consistent pattern over the years. The assessment of oral mucosa lesions in 2023 further echoes this narrative of stability, reflecting similar proportions to the 2019 findings with a marginal rise in specific lesions. In these particular oral health categories, the comparable data from both years emphasize the enduring and unchanged nature of these health issues within the community, underscoring the persistent need for concentrated and continued oral health interventions in Zanzibar.
A review of the clinical data provides several valuable insights into the oral health landscape of the community served by the dental outreach camps. The high prevalence of dental caries underscores the significant oral health challenges faced by this community [
4]. This aligns with the broader global trend, particularly in low- and middle-income countries, where access to preventive dental care is limited and dental diseases, especially dental caries, are prevalent [
5,
6,
7,
8].
Our study identified a caries prevalence of 48.6% among preschool and school-aged children (3–10 years) in Zanzibar, closely paralleling the national survey’s finding of 43.2% in a comparable age group. Notably, both studies demonstrate a trend of reduced caries prevalence in older children. In our study, the prevalence among adolescents and teens (11–17 years) was 35.6%, showing a marked reduction from the younger age group. This trend resonates with the 2023 survey, where a similar decrease in caries prevalence was noted among older children, albeit in slightly different age brackets (12 and 15 years compared to 5 years) [
3].
This consistent observation across both studies suggests a general trend of decreasing caries prevalence with increasing age in Tanzanian children. Additionally, the higher caries prevalence in the Zanzibar region, as observed in our study, aligns with the survey’s findings that rural areas often exhibit a higher prevalence compared to urban and cosmopolitan regions in Tanzania. This highlights the particular oral health challenges faced in rural settings like Zanzibar and underscores the importance of targeted dental health interventions in these areas.
The number of teeth extracted due to caries is another significant finding. This could suggest a potential lack of early dental intervention in this community leading to advanced dental issues that necessitate extraction. The ratio of fillings to extractions could serve as a potential indicator of the state of oral health in the community, reflecting both the prevalence of dental disease and the availability (or lack thereof) of early, preventive dental care.
The relatively high proportion of preventive procedures such as fluoride application and scaling is an encouraging finding, reflecting the outreach camp’s focus on treating existing issues and preventing future ones. This preventive approach is crucial in communities where regular access to dental care is limited [
9].
The extensive treatment provided in a short period signifies the pressing need for continuous and accessible dental care in this community. It also showcases the substantial impact that such dental outreach camps can have, both in terms of immediate relief and longer-term preventive care [
7].
The findings of this study align with the commonly posited inverse relationship between non-carious tooth loss and caries [
10]. This inverse correlation is attributable to the natural cleansing action of abrasive diets which combined with the accelerated degradation of tooth structure through repeated erosive episodes, aids in the removal of newly formed carious lesions. This phenomenon is particularly pronounced when there is a high frequency of erosive/abrasive cycles and erosive attacks, underlining a complex interplay between dietary habits and dental health.
The observed increase in non-carious tooth surface loss cases in 2023, compared to pre-COVID-19 pandemic values in 2019, presents a compelling point for discussion. A possible explanation for this trend could be rooted in the unique public health responses and cultural practices that emerged during the COVID-19 pandemic in Tanzania [
11,
12]. In May 2020, the Tanzanian government, diverging from global trends, focused on alternative, herbal-based remedies for COVID-19. One such remedy was COVID-Organics, a herbal tea derived primarily from sweet wormwood (
Artemisia annua), supplemented with other herbs. Additionally, the Tanzanian President’s emphasis on using medicinal herbs for steaming and oral consumption as an alternative treatment for COVID-19 further fueled these practices [
12,
13,
14].
Commonly used medicinal herbs included citron (
Citrus medica), lemon (
Citrus limon L.), and lime (
Citrus aurantiifolia) [
11,
14]. These citrus-based herbs, known for their acidic nature, become even more erosive when heated and consumed in a boiled form [
15,
16], as per the instructions given by the government [
13]. The widespread consumption of these herbal mixtures, particularly during the pandemic’s peak, likely contributed to the increased incidence of non-carious tooth surface loss observed in the population. The acidic nature of these herbal concoctions, especially when ingested regularly and in heated forms, could have led to an accelerated rate of dental erosion, exacerbating the wear on tooth surfaces.
Another common local practice was chewing guava tree (
Psidium guajava) barks [
13]. This habit might have exacerbated the erosive potential of the boiled citrusy drinks by adding an abrasive component to the formula, making the situation even worse if consumed and chewed concomitantly [
17].
Thus, the spike in non-carious tooth surface loss cases in 2023 might be attributed to these culturally ingrained and government-promoted practices during the COVID-19 pandemic. This correlation between increased herbal remedy consumption, particularly of an acidic nature, and the rise in non-carious tooth surface loss cases offers a critical perspective on the unforeseen dental health consequences of alternative medical practices during a global health crisis.
The observed trends in dental caries, particularly the notable reduction among adolescents and teens, alongside the decline in the number of missing teeth due to caries, are indicative of the positive impact of continuous dental outreach programs, including the one conducted in 2019 by the authors of this paper. This reduction in dental caries observed in 2023, as compared to 2019, could be attributed in part to the strategic initiatives outlined in Tanzania’s Strategic Oral Health Plan (2012–2017) [
18]. Despite initial challenges in implementation, the involvement of non-dentally trained health workers in providing emergency dental services in rural areas with limited oral health services has been a crucial step towards meeting oral health needs in Tanzania.
The partnership between dental training charities (e.g., the UK-based Bridge2Aid) and the Tanzanian government has also played a pivotal role in advancing the primary goals of the plan, significantly contributing to the reduction in caries prevalence [
19,
20,
21]. This highlights the importance of government policy and collaborative efforts in improving oral health outcomes in underserved communities. Additionally, the dental outreach conducted in 2019 by the authors of this paper, which included a substantial focus on preventive dental treatment, likely also played a key role in this reduction. By providing preventive care and education, the outreach program addressed immediate dental needs and set the foundation for long-term improvements in oral health within the community. This comprehensive approach, combining policy initiatives with practical outreach efforts, underscores the multifaceted strategy needed to effectively tackle dental health challenges in regions like Zanzibar.
It is important to note that while dental outreach camps like this one can provide much-needed immediate care and relief, they are not a substitute for accessible, regular dental care. The recurring and preventable nature of dental diseases requires continuous care and preventive measures, ideally provided by a regular, locally accessible dental service [
22].
The study focused exclusively on school-going children in Zanzibar, which may not represent the entire pediatric population of the region. The findings might not accurately reflect the oral health status of children who are out of school, potentially leading to an underestimation or overestimation of dental health issues. As the study was conducted in a specific geographic and cultural setting, the findings might not be generalizable to other regions or populations. Despite the calibration of the dental team, variations in clinical assessments could introduce observer bias. Different practitioners may have slightly different thresholds for diagnosing conditions like dental caries or erosion.
While the calibration process for data collectors aimed to ensure consistent and accurate assessments, we acknowledge that the study did not include formal intra-observer and inter-observer reliability testing. Future endeavors will benefit from incorporating such measures to quantitatively validate the consistency of data collection across different observers. Additionally, in determining the cause of missing teeth, our study primarily relied on patient recall, which could introduce recall bias. Without corroborative dental records, the precision of our findings on teeth missing due to caries may be affected.
In light of our study’s findings, we advocate for a multifaceted strategy to elevate oral health within the examined groups. Key to this approach is the extension and diversification of preventive dental health programs, especially those capable of tackling both the enduring challenge of dental caries and the emerging concern of non-carious tooth surface loss. The significance of comprehensive oral health education cannot be overstated, and initiatives targeting all age groups must be developed and implemented with a curriculum that spans the full spectrum of oral health challenges. Continuous monitoring forms the backbone of any effective health intervention, enabling stakeholders to identify emerging trends and adapt strategies accordingly. Furthermore, fostering a deeper engagement with the community will ensure that interventions are both well-received and specifically tailored to meet the unique needs of the population. By adopting such an integrated approach, predicated on ongoing assessment and community involvement, we can build on the positive impacts observed from previous outreach efforts. This would set a precedent for a sustainable improvement in oral health outcomes aligning with global health objectives and ensuring the resilience of rural communities against dental health challenges.
5. Conclusions
The study illuminates the critical role of continuous dental outreach programs in enhancing oral health in rural Tanzania, with a particular focus on the Zanzibar region. Notably, we observed a significant reduction in the prevalence of dental caries among adolescents and teens between the years 2019 and 2023, underscoring the effectiveness of such initiatives. Concurrently, the increase in non-carious tooth surface loss during the same period emerged as a new area requiring immediate attention.
Our analysis underscores the dynamic nature of dental health challenges within rural communities and the imperative for adaptive, comprehensive oral health strategies. The tangible improvements observed over the four-year span highlight the importance of sustained outreach efforts. However, the emergence of non-carious tooth surface loss as a growing concern calls for an integrated approach to oral health that encompasses both treatment and extensive preventive education. Future outreach must continue to evolve in response to these findings, ensuring a holistic approach to improving oral health outcomes for all age groups in Zanzibar and similar contexts.