Abstract
Acute Respiratory Distress Syndrome is a familiar and destructive clinical condition characterized by progressive, swift and impaired pulmonary state. It leads to mortality if not managed in a timely manner. Recently the role of imbalanced macrophage polarization has been reported in ARDS. Macrophages are known for their heterogeneity and plasticity. Under different microenvironmental stimuli, they (M0) can switch between classically activated macrophage (M1) and alternatively activated (M2) states. This switch is regulated by several signaling pathways and epigenetic changes. In this review, the importance of macrophage M1 and M2 has been discussed in the arena of ARDS citing the phase-wise impact of macrophage polarization. This will provide a further understanding of the molecular mechanism involved in ARDS and will help in developing novel therapeutic targets. Various biomarkers that are currently used concerning this pathophysiological feature have also been summarized.
1. Introduction
Acute respiratory distress syndrome (ARDS) is characterized by the acute onset of pulmonary oedema of non-cardiogenic origin, along with bilateral pulmonary infiltration and subsequent failure of the respiratory system. Refractive hypoxemia and stiff lung are the clinical hallmarks of ARDS. Since its first description, ARDS has been redefined several times to ameliorate the accuracy of clinical diagnosis [1]. The first known description of the syndrome dates back to 1821 when Laennec described fatal “idiopathic pulmonary oedema”. Later, the first and the second World wars provided evidence that several traumatic insults could result in the eventual development of an edematous lung injury, so that and the term “shock lung” were developed to describe such a condition. In 1967, Ashbaugh et al. published a case series of 12 patients who had developed respiratory failure after a variety of insults [2], providing the first systematic description of this condition (Table 1).

Table 1.
The various definitions adapted for ALI/ARDS.
At a microscopic level, ARDS is associated with capillary endothelial injury and diffusive alveolar damage, due to which it is also known as diffuse alveolar damage (DAD) disorder. When ARDS progresses, the subject undergoes different extents of pulmonary artery vasoconstriction that later develops into pulmonary hypertension. ARDS is associated with high mortality and there are few therapeutic options to combat this condition.
2. Etiology
Although numerous medical and surgical ailments lead to ARDS, the syndrome mainly develops in pneumonia and sepsis (>80%). Environmental triggers progressing ALI can be broadly divided into two categories, direct and indirect lung injury, also known as pulmonary and extra-pulmonary injury (See Table 2). Those with predisposing medical disorders including metabolic acidosis, pancreatitis, older age and chronic alcohol abuse are at risk of developing ARDS. Trauma cases with APACHE II score >16 have a 2.5 times higher chance of developing this syndrome [6].
Table 2.
Direct and Indirect triggers for ALI.
3. Pathophysiology
The natural course of ARDS encompasses three phases: exudative phase (day 0–7), proliferative phase (day 7–21) and proliferative phase (>day 21) (Figure 1). In ARDS, also known as hyaline membrane disease, the injury at the endothelial and epithelial lining compromises the integrity of the alveolar–capillary membrane. There has been much evidence suggesting that ARDS arises from an inflammatory reaction initiated by a variety of pro-inflammatory cytokines. During the initial 30 min after an acute insult, there is increased synthesis of interleukin 8 (IL-8), a potent neutrophil chemotactic and activating agent, by pulmonary macrophages. Release of IL-8 along with other factors, such as IL-1 and tumor necrosis factor (TNFα), leads to endothelial activation and sequestration and activation of neutrophils in pulmonary capillaries. Activated neutrophils release a variety of products (e.g., reactive oxygen species, reactive nitric oxide species, and proteases) that damage the alveolar epithelium and endothelium membrane. The assault on the endothelium and epithelium causes vascular leakiness and loss of surfactant that dampens the alveolar unit in order to expand. Of note, the destructive forces unleashed by neutrophils can be counteracted by an array of endogenous anti-proteases and anti-oxidants that are up-regulated by proinflammatory cytokines. In the end, it is the balance between the destructive and protective factors that determines the degree of tissue injury and clinical severity of the ALI/ARDS [7].A detailed pathophysiological change has been discussed in the context of the macrophage at various phases, the “role of the macrophage in acute lung injury”, discussing the effect of the above-mentioned cytokines, factors and the various signaling pathways involved.
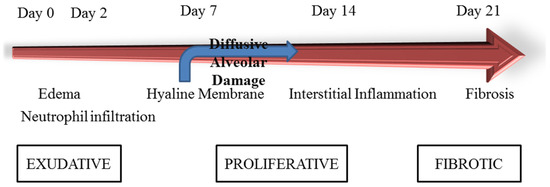
Figure 1.
Illustration showing time course for development and resolution of ARDS. Reprinted with permission from Ref. [6].
The heterogeneous nature of the syndrome itself, presence of additional comorbidities, potentially incomplete gene penetrance and complex gene–environment interactions lead to difficulty in assessing the underlying mechanism of ARDS. At present the research is channelized into the role of genetic factors and their contribution to ARDS susceptibility, thus providing targets for research in treatment development. This review is intended to understand the role of macrophage polarization in ARDS and to identify key targets for the resolution of this damaging respiratory syndrome.
ARDS is characterized by an excessive and uncontrolled systemic inflammatory response in which different subsets of macrophages are involved. This includes resident alveolar macrophages (AMs) and recruited macrophages from the blood which function differently under microenvironmental stimuli, playing a causal role in the pathogenesis and resolution of ARDS.
As a part of the innate immune system, macrophages serve as the first barrier of defense against extrinsic invaders and airborne particles, especially in the lung. They help in clearing cellular debris and ensuing resolution in a post-injury state. This is governed by switching between two polarized states of macrophage depending upon the extracellular environment. This includes the classically activated phenotype (M1) and the alternatively activated phenotype (M2). M1 macrophages partake in pro-inflammatory conditions and have cytotoxic capabilities, whereas M2 mainly function as anti-inflammatory cells and have a tissue remodeling role and matrix deposition in post-injury conditions [8].
4. Biomarkers
There are various established biomarkers for ARDS concerning different phases of pathogenesis. Here, since abnormal macrophage polarization is considered a key orchestrator of ARDS, identifying these could serve an important function in developing therapeutic agents. Some of the routinely used biomarkers are described in Table 3. CD68 and CD11b are total markers of macrophages. M1 and M2 macrophages have specific markers.
Table 3.
Some of the biomarkers associated with M1 and M2.
Macrophages are a type of monocyte (mononuclear phagocyte system) universally present as a part of the innate immune system belonging to both invertebrates and vertebrates. They were recognized first time by Metchnikoff in 1882 in the larvae of starfish upon insertion of thorns of the tangerine tree, and later in Daphnia Magna or the common water flea infected with fungal spores, as cells responsible for the process of phagocytosis of foreign particles [14]. Macrophages stem from a very early phase of embryogenesis known as primitive hematopoiesis occurring at embryonic day 6, from precursor cells present in the extraembryonic yolk sac. The process of hematopoiesis progresses towards the fetal liver at the beginning and finally to the bone marrow in the adult animal, including humans [15]. Macrophages can be classified based on anatomical regions and polarization state.
5. Based on Anatomical Regions
In normal physiological conditions, monocytes circulate in the bloodstream while macrophages remain in different tissues serving specific purposes, such as intestinal macrophages in the gut, Kupffer cells in the liver, microglial cells in the brain, and osteoclasts in bone, and many more (See Table 4).
Table 4.
Depending on the site of action, macrophages can be classified into the following-.
6. Division Depending on Polarization
The polarization of macrophages has a diverse heterogenic function and phenotypes, depending on their activation in respect to the duration of stimulation and spatial localization. According to the activation state and functions of macrophages, they can be divided into
- (A) M1-type (classically activated macrophages (CAMs) or pro-inflammatory).
- (B) M2-type (alternatively activated macrophages (AAMs) or anti-inflammatory).
- (C) Regulatory Macrophages (Mreg).
Some of the recognized states in different pathological conditions are stated below (Figure 2); however, this is not a clear cut demarcation of the subtypes involved as switching occurs continuously in a disease state.
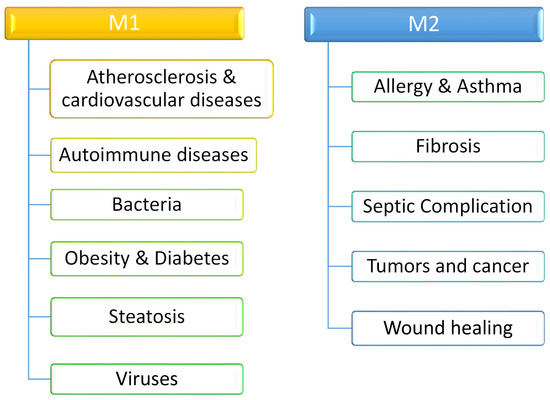
Figure 2.
Difference in physiological significance of polarized macrophage.
Apart from the above stated broad classification, there are several subtypes of activated macrophages which include M2a, M2b, M2c and M2d, responsible for anti-inflammatory and wound healing, immunomodulation, efferocytosis and angiogenesis, respectively [16].
7. Functional Role of Macrophages in Human Physiology
Macrophages are similar to neutrophils as they have various types of pattern recognition receptors (PRRs), are an influential mechanism of phagocytosis, can alarm other immune about the infection, and use oxidative molecules as their defense protocol. Cytokines secreted by activated TH cells along with other inflammatory factors can upgrade the macrophage inflammatory response. Activated macrophages are more powerful for eliminating pathogens. They exhibit greater phagocytic activity, increased secretion of inflammatory factors, and higher expression levels of MHC class II molecules, which can present antigens to TH cells. Thus, macrophages and TH cells work in a symbiotic fashion. Macrophages not only eliminate pathogens directly but also act as antigen-presenting cells (APC) for a stronger immune response.
Macrophages are present in all vertebrate tissues, from mid-gestation throughout life, constituting a widely dispersed organ system. They regulate various physiological functions by responding to internal and external changes within the body acting as a dispersed homeostatic organ, not only as phagocytes in defense against microbes and clearance of dead and senescent cells, but also through trophic, regulatory and repair functions. Some of the noted physiological functions are given below (Figure 3):
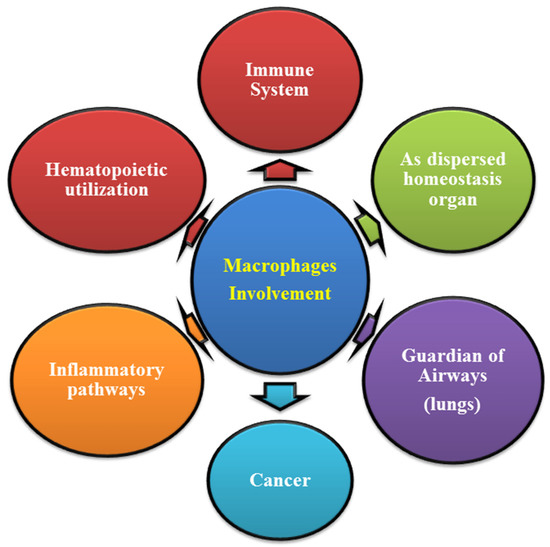
Figure 3.
Utilization of macrophage as a multipurpose system.
8. Molecular Mechanism of Macrophage in ARDS
The lung primarily contains alveolar macrophages either of embryonic origin or bone marrow-derived hematopoietic stem cells (HSCs) [17], whose turnover is independent, and production and maturation depend on various transcription factors. In addition, the airway contains the antigen-responsive bronchial dendritic cell and interstitial macrophages. Monocytes are recruited later in adult life to restock alveolar macrophages and during the inflammatory response. Alveolar macrophages play a key role in the clearance of particles, microbes, dust and pollutants and the regulation of surfactant proteolipid turnover through local secretion of Granulocyte-Macrophage-Colony Stimulating Factors (GM-CSF), otherwise the surfactant protein accumulate in the alveoli hampering the lung function. Alveolar macrophages are rounded, loosely adherent cells and display a distinctive phenotype from other lung or tissue macrophages. The oxygen-rich environment may generate ligands for these scavenger receptors.
Lung macrophages are durable cells with wide differentiation potential, which reside in the lung interstitium and alveoli or are organ-recruited upon inflammatory stimuli. The role of resident and recruited macrophages in initiating and maintaining pulmonary inflammation in lung infection or injury has been convincingly demonstrated. More recent reports suggest that lung macrophages are the main orchestrators of the termination and resolution of inflammation. They are also initiators of parenchymal repair processes that are essential for return to homeostasis with normal gas exchange.
To understand the pivotal role of macrophages in the pulmonary region, we will consider it in a stepwise manner relating to the changes occurring in the exudative phase, rehabilitation phase and fibrotic phase of ALI/ARDS (Figure 4). The function of the macrophage is divided here into resident alveolar macrophages (M1) and recruited macrophages (M2) from the blood, concerning the pathogenesis of ALI/ARDS.
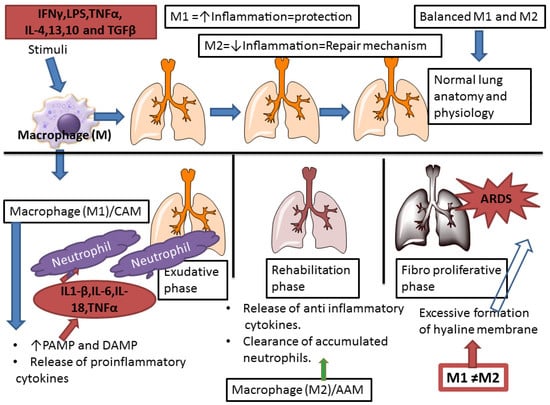
Figure 4.
Key factors behind macrophage polarization in ARDS. In the pathological state, the excess release of pro-inflammatory cytokines leads to an imbalance between the two polarized states. Due to the persistent influence of the M2 polarized state, the hyaline membrane is formed leading to late stage complication of ARDS.
During the inflammatory response preceding injury in the lung, Macrophages play a tricky role. They are generally pro-inflammatory in the initial stage followed by an anti-inflammatory response in the later stages. This occurs due to the phenotypic transformation of macrophage from M1 to M2 via various signaling pathways including Toll-like receptor, NOD-like receptor, JAK/STAT pathway, intracellular helicases such as retinoic acid-inducible gene I (RIG-I), along with various pattern recognition receptors such as Pathogen Associated Molecular Pattern (PAMP) and Danger Associated Molecular Pattern (DAMP), which integrate into the shaping of pulmonary macrophages’ phenotyping and programming.
Recently, Liang et al. demonstrated the role of JAK/STAT3 phosphorylation in alveolar macrophage in LPS induced acute lung injury. They reported a decrease in the expression of Kruppel-like factor 2 (KLF2) in the alveolar macrophage which inhibited the phosphorylation of STAT3 and reduced levels of STAT3 target genes, including matrix metalloproteinase (MMP)-2/9 (MMP-2/9), which exacerbated pulmonary inflammation in ALI [18].
Another study performed by Chai et al. demonstrated the role of curcumin in down-regulation of M1 and up-regulation of M2 in the lungs of CLP-induced mouse ALI model. They raised an interesting fact regarding the anti-inflammatory effect of IL-10, which is mediated by metabolic reprogramming of macrophages, including inhibition of mTOR signaling and inflammasome activations, citing the importance of the macrophage in the inflammatory response. Macrophages are either M1 or M2, and these cells play different roles in ARDS. The classically activated phenotype (M1) releases various potent proinflammatory mediators aggravating ALI, while the M2 phenotype eliminates apoptotic cells and participates in lung tissue repair, alleviating ALI [19].
These pathways on activation release early response cytokines such as type I IFN, TNF-α, and IL-1β in an IRF- or NF-κB-dependent way [20]. These stimulate the adjacent alveolar epithelial cells and tissue-resident macrophages (M2) in an auto- and paracrine manner to fabricate various chemokines which in turn regulate the recruitment of neutrophils along the lining, and afterwards exudate macrophages (M1) and lymphocytes to the site of infection, ultimately resulting in clearance of pathogens in a stepwise manner. A study performed by William et al. assessed the balance of cytokines such as TNFα, IL-1β, IL-6 and IL-10 in 23 patients with risk of ARDS and 46 patients with established ARDS, in which they found that a high concentration of anti-inflammatory cytokine during early onset produce a low molar ratio of pro-inflammatory to anti-inflammatory mediators in the lung, thereby dampening the over enhanced inflammation in the airspace, and emphasized that there is a requirement of measuring both pro- and anti-inflammatory cytokines for the correct assessment of ARDS [21].
Clearance of the pathogen along with downregulation of the initial inflammatory signals upon its recognition, or other stimuli, does not completely stop the lung inflammatory process. A well-coordinated system comprising of granulocyte emigration from blood vessels, restoration of normal vascular permeability and removal of extravasated fluids, termination of monocyte emigration and induction of their maturation into resident alveolar macrophages, removal of apoptotic neutrophils, and finally, restoration of functional endothelial and epithelial monolayers, helps in the full-fledged confrontation with the lung inflammation. Here, the macrophage plays an important role, apart from classical phagocytosis, as they are endowed with functional flexibility to either play their card as pro- or anti-inflammatory, along with the tissue reparation, depending upon the signals they receive and decode from the surrounding cell or from the pathogen itself. The proficiency of these macrophages, either lung resident or recruited to terminate and resolve alveolar inflammation in the later phase of ALI/ARDS, serving as the repair mechanism, is essential for homeostasis [22].
Based on the phases of ALI, starting with Phase I, also known as the exudative phase, when compared with normal lung it has been observed that there is an increased expression of PAMP and DAMP upon infection or exposure to endotoxin, leading to injury, with a shift of tissue-resident macrophage M2 to M1. This alveolar polarization serves as the first line of defense against the invading pathogen or the expressed stimuli. This M1 macrophage releases various pro-inflammatory chemokines such as Il-1beta, IL-6 and IL-18 which interjects the neutrophil from surrounding intravascular space to the epithelial and endothelial lining of the alveolus from where they enter into the lungs and alveolar space, thereby promoting the ALI/ARDS. However on another note, a protective aspect of M1 has been observed, where they produce an increased level of amphiregulin, which act as a ligand for epithelial growth factor receptor thereby protecting the epithelial barrier.
This polarization shift occurs due to the JAK/STAT pathway as mentioned above. The circulating pro-inflammatory cytokines, specifically IFN-1gamma, binds to the cell surface receptor, activating Janus kinase 1, 2 and activating STAT1. Suppressor of Cytokine Signaling 1/3 inversely regulates STAT1, inhibiting the macrophage polarization by phosphorylating tyrosine residue on JAK. Another underlying pathway in polarization is regulated via transcription factor IRF-5. This factor significantly decreases in the presence of SOCS 3. To sum up STAT 1, SOCS 1, SOCS 3 and IRF-5 regulate polarization of macrophage M1 in injured conditions [18,23].
Phase II, better known as the rehabilitation phase, sum ups the recovery response after the pathogen exposure is counteracted by pro-inflammatory chemokine in phase I. The first step in this area is to reduce the level of cytokines that are promoting inflammation and inducing phenotypic alteration from M1 to M2 via various signaling pathways including STAT6, SOCS1/SOCS3 [23], and IRF4. Apart from the stated pathways, M2 itself differentiates into four subtypes (M2a, M2b, M2c, M2d) depending upon the activation signal. M2 macrophage plays a key role in tissue repair around the lungs by decreasing the level of chemokine in Phase I and helps in the production of anti-inflammatory chemokines such as IL-10 and IL-1 receptor antagonist in response to type 2 helper T cell (Th2). Balancing the level of pro- and anti-inflammatory cytokines does not alleviate inflammation and the clearance of neutrophils in phase I also serves as the main contributing factor. Neutrophils, upon recognizing the pathogen, exhibit apoptosis and apoptotic cells are accumulated. Macrophage 2, with the help of “find me” and “eat me” signals, helps in the clearance of apoptotic cells and debris by G-protein coupled macrophage chemotaxis receptor G2A [24], and CD31 or CD47/SIRP-α signals, respectively. Efferocytosis by M2 also increases the level of IL-10 and TGF-β1 which controls the inflammation, reducing the level of inducible nitric oxide synthase level and stimulating the expression of arginase 1 which reduces reactive nitric oxide species.
An observational study performed in 2015, where 79 patients were enrolled fulfilling Acute Physiologic and Chronic Health Evaluation (APACHE) II score, Sequential Organ Failure Assessment (SOFA) score, and Lung Injury Score, to assess the significance of level between CD4 + CD25 + Foxp3 + regulatory T (Treg) cells and T helper (Th)17 with ARDS, concluded that The Th17/Treg imbalance favoring a Th17 shift exemplifies a potential therapeutic target to improve lung injury in patients with ARDS [25].
The last Phase III, also termed as the fibro proliferative phase, is paradoxically a late-stage complication of persistent ALI/ARDS. In order to maintain lung homeostasis, a well-defined remodeling of the tissue after the injury is required, ensuring minimum fibrosis or scar deposition, which serves as a complication in later stages. Here M2 macrophage has a significant role in terms of fibroblast proliferation by enhanced expression of TGF-β, fibronectin, proline, arginase 1 and tissue inhibitor of metalloproteinase (TIMP). Sustained release of IL-13 and IL-4 in phase II on the alveolar surface promotes M2 mediated fibrosis via TGF-β and arginase-1 pathway. M1 macrophages, on the other hand, are anti-fibrotic by enhanced expression of CXCL10 and matrix metalloproteinase, thereby resolving excessive scarring, fibroblast deposition and maintaining membrane integrity. (Figure 4) [26].
9. Discussion
This paper has provided an overview of ARDS including definition, aetiology and pathogenesis. It also summarises macrophage, their different subtypes, regulation of macrophage polarisation by signalling pathways and lastly the role of macrophage polarisation in ARDS. Through this, we have tried to bring attention to the impact of macrophage functioning in ARDS and, while developing novel therapies, the plasticity of macrophages should be a deciding factor.
Various reports have suggested the importance of M1 in the early stage of ARDS, but contradicting reports also exist. Therefore, a biomarker-based approach that could clearly distinguish between the polarised states is the need of the hour. This can be reached by studying the signalling pathway involved in M1/M2 polarization. This would lead to formulating treatment strategies that would concentrate on neutralising the overexpression of M1 polarization; in the later stages, the expression of M2 polarization should be pondered.
While numerous studies have demonstrated the role of macrophages M1 and M2 in the pathogenesis of ARDS [19,27,28,29], there are still many paths to be explored regarding the underlying signalling pathways and cell to cell communication. Some important points which need to be considered are as follows:
- How do these macrophages decide the level of inflammatory cytokine and neutrophil production?
- How do they interact with localised endothelial cells from airway epithelial progenitors during the regeneration process?
The most important question still to be answered is: how does polarization occur in an organ-specific inflammatory environment and how can this polarization be utilised more specifically in M1 and M2 to enhance the outcome in acute lung injury therapy. The respiratory tract is in direct contact with the outer environment and is especially vulnerable to the harsh effects of the pathogen and the other allergens. Understanding this macrophage and its host immune defence against these outer based pathogens or allergens which cause insult to the lungs is vital, as understanding of the regulating pathway of macrophage activation and the mediators involved in it by (direct or indirect) release could make way for more effectual approaches for the treatment of lung disease.
When an organ is attacked by an infection or a disease, the proinflammatory M1 phenotype of macrophages can trigger tissue damage. The anti-inflammatory M2 phenotype can suppress the inflammation and promote tissue remodeling. Therefore, to treat inflammatory disorders including ARDS researchers aim to reverse the polarization of macrophage populations. Although the concept of epigenetic modifiers has only been around for a couple of years, their potential has been widely explored. The combination of 5-Aza 2-deoxycytidine (Aza) and Trichostatin A (TSA) decreased the expression of the M1 phenotype while augmenting the expression of the M2 phenotype in LPS-induced macrophages [28,29]. These studies can help researchers to explore new strategies to improve the outcome in ARDS [30].
Understanding the pathogenesis of lung injury and its resolution will help develop new drugs that can improve the survival rate and minimize the toxicity of these devastating diseases. MSCs are known to secrete various effector molecules that can reverse the major changes in lung injury.
In an experimental model, the presence of MSCs isolated from the alveolar wall restored the normal production and barrier properties of the alveolar protein [31].
Human mesenchymal stem cells have potential therapeutic properties for patients with ARDS. Studies show that these cells can augment the function of human macrophages and alter their phenotypes. Human MSCs were tested ex vivo by exposing them to an isolated lung perfusion system. The results showed that the media did not affect the lung wet-to-dry ratio and alveolar fluid clearance [27].
With declining mortality, new drugs will need to be studied to select the patients with the highest expected mortality. Currently, clinical trials are focused on assessing the effects of statin therapy on various inflammatory diseases. In humans, aspirin is effective in preventing the development of acid-induced lung injury (ALI) in animals. A prospective study is planned to test the safety and effectiveness of aspirin in high-risk patients [32,33,34].
Further research into the factors that influence the long-term functional status of patients following recovery from acute respiratory distress syndrome (ARDS) and ALI is expected to stimulate new approaches to prevent these conditions [35,36]. The idea that macrophages can respond to the environment’s signals has been gaining increasing support due to the large amount of data that supports this hypothesis [37]. This has profound implications for the development of new drugs that target the polarization of the macrophages’ function. The exact molecular factors that contribute to the dynamic transition of a macrophage phenotype are still not known. Further studies are needed to elucidate these factors and examine the mechanisms of their interaction.
To develop potential treatment strategies against ARDS, the underlying cellular and molecular mechanism need to be identified. Recently Zhang et al. identified a novel regulator of M1 polarization IFIH1. They found a strong correlation of this gene with ARDS. This could lead to a search for novel targets [35].
Recently gene-editing tools have been employed to further strengthen the molecular mechanism behind a disease and disorder. In this direction, Crisper/Cas9 complex provides a new tool for the reprogramming of the M1/M2 macrophage by utilizing the knockout technique. The specific knockout of the ubiquitin-specific proteinase, for example USP 18, which is involved in the IFN signaling in macrophages could regulate the polarization [36]. This will be a more robust and effective method, by targeting genes involved in the pro and anti-inflammation process. For example, there is a two target gene with differential expression in the pro- and anti-inflammatory macrophages, i.e., 7-dehydrocholesterolreductase (DHCR7) and cytochrome B 245 [37].
10. Conclusions
Although limited, this review suggests that regulating the pro-inflammatory response in the early exudative phase and fibroblast proliferation in the repair phase by reprogramming the macrophage polarization might be a new target for the treatment of ARDS. Identification of gene-specific biomarkers related to the polarized state might contribute to the early diagnosis of ARDS and provide sufficient time windows to the physicians for managing it. However, there is an urgent need for translation of such specific work, including stem cell therapies to identify therapeutic agents for ARDS.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Ashbaugh, D.G.; Boyd Bigelow, D.; Petty, T.L.; Levine, B.E.; Bigelow, D.B.; Petty, T.L. Acute respiratory distress in adults. Lancet 1967, 290, 319–323. [Google Scholar] [CrossRef]
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. Acute respiratory distress in adults. The Lancet, Saturday 12 August 1967. Crit. Care Resusc. 2005, 7, 60–61. [Google Scholar]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R.; et al. Report of the American-European consensus conference on ARDS: Definitions, mechanisms, relevant outcomes and clinical trial coordination. Intensive Care Med. 1994, 20, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin definition. JAMA J. Am. Med. Assoc. 2012, 307, 2526–2533. [Google Scholar]
- Rebecca, M.B.; Bruce, D.L. Harrison’s Principles of Internal Medicine; McGraw Hill: New York, NY, USA, 2018. [Google Scholar]
- Bhatia, M.; Moochhala, S. Role of inflammatory mediators in the pathophysiology of acute respiratory distress syndrome. J. Pathol. 2004, 202, 145–156. [Google Scholar] [CrossRef]
- Atri, C.; Guerfali, F.Z.; Laouini, D. Role of Human Macrophage Polarization in Inflammation during Infectious Diseases. Int. J. Mol. Sci. 2018, 19, 1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Two Types of Macrophages: M1 and M2 Macrophages. Cusabio. Available online: https://www.cusabio.com/c-20938.html (accessed on 18 October 2021).
- Hesketh, M.; Sahin, K.B.; West, Z.E.; Murray, R.Z. Macrophage Phenotypes Regulate Scar Formation and Chronic Wound Healing. Int. J. Mol. Sci. 2017, 18, 1545. [Google Scholar] [CrossRef] [Green Version]
- Martinez, F.O.; Helming, L.; Gordon, S. Alternative Activation of Macrophages: An Immunologic Functional Perspective. Annu. Rev. Immunol. 2009, 27, 451–483. [Google Scholar] [CrossRef] [Green Version]
- Kubota, T.; Inoue, M.; Kubota, N.; Takamoto, I.; Mineyama, T.; Iwayama, K.; Tokuyama, K.; Moroi, M.; Ueki, K.; Yamauchi, T.; et al. Downregulation of macrophage Irs2 by hyperinsulinemia impairs IL-4-indeuced M2a-subtype macrophage activation in obesity. Nat. Commun. 2018, 9, 4863. [Google Scholar] [CrossRef]
- Rőszer, T. Understanding the Mysterious M2 Macrophage through Activation Markers and Effector Mechanisms. Mediat. Inflamm. 2015, 2015, 816460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A thorn of a tangerine tree. British Society for Immunology. Available online: https://www.immunology.org/thorn-tangerine-tree-1882 (accessed on 27 March 2020).
- Wynn, T.A.; Chawla, A.; Pollard, J.W. Macrophage biology in development, homeostasis and disease. Nature 2013, 496, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, M.H.; Abdelwahab, S.F.; Wan, J.; Cai, W.; Huixuan, W.; Jianjun, C.; Kumar, K.D.; Vasudevan, A.; Sadek, A.; Su, Z.; et al. Alternatively activated macrophages; a double-edged sword in allergic asthma. J. Transl. Med. 2020, 18, 1–12. [Google Scholar] [CrossRef]
- Epelman, S.; LaVine, K.J.; Randolph, G.J. Origin and Functions of Tissue Macrophages. Immunity 2014, 41, 21–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Luo, J.; Yang, N.; Wang, S.; Ye, M.; Pan, G. Activation of the IL-1β/KLF2/HSPH1 pathway promotes STAT3 phosphorylation in alveolar macrophages during LPS-induced acute lung injury. Biosci. Rep. 2020, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, Y.-S.; Chen, Y.-Q.; Lin, S.-H.; Xie, K.; Wang, C.-J.; Yang, Y.-Z.; Xu, F. Curcumin regulates the differentiation of naïve CD4+T cells and activates IL-10 immune modulation against acute lung injury in mice. Biomed. Pharmacother. 2020, 125, 109946. [Google Scholar] [CrossRef]
- Martin, T.R. Cytokines and the acute respiratory distress syndrome (ARDS): A question of balance. Nat. Med. 1997, 3, 272–273. [Google Scholar] [CrossRef]
- Park, W.Y.; Goodman, R.B.; Steinberg, K.P.; Ruzinski, J.T.; Radella, F.; Park, D.R.; Pugin, J.; Skerrett, S.J.; Hudson, L.D.; Martin, T.R. Cytokine Balance in the Lungs of Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2001, 164, 1896–1903. [Google Scholar] [CrossRef]
- Ariel, A.; Maridonneau-Parini, I.; Rovere-Querini, P.; Levine, J.S.; Mühl, H. Macrophages in inflammation and its resolution. Front. Immunol. 2012, 3, 324. [Google Scholar] [CrossRef] [Green Version]
- Song, Z.; Zhao, X.; Gao, Y.; Liu, M.; Hou, M.; Jin, H.; Cui, Y. Recombinant human brain natriuretic peptide ameliorates trauma-induced acute lung injury via inhibiting JAK/STAT signaling pathway in rats. J. Trauma Acute Care Surg. 2015, 78, 980–987. [Google Scholar] [CrossRef]
- Kern, K.; Schäfer, S.M.G.; Cohnen, J.; Pierre, S.; Osthues, T.; Tarighi, N.; Hohmann, S.; Ferreiros, N.; Brüne, B.; Weigert, A.; et al. The G2A Receptor Controls Polarization of Macrophage by Determining Their Localization Within the Inflamed Tissue. Front. Immunol. 2018, 9, 2261. [Google Scholar] [CrossRef]
- Yu, Z.-X.; Ji, M.-S.; Yan, J.; Cai, Y.; Liu, J.; Yang, H.-F.; Li, Y.; Jin, Z.-C.; Zheng, J.-X. The ratio of Th17/Treg cells as a risk indicator in early acute respiratory distress syndrome. Crit. Care 2015, 19, 82. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.-Y.; Chen, C.-S.; Yiang, G.-T.; Cheng, Y.-L.; Yong, S.-B.; Wu, M.-Y.; Li, C.-J. New Insights into the Immune Molecular Regulation of the Pathogenesis of Acute Respiratory Distress Syndrome. Int. J. Mol. Sci. 2018, 19, 588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aggarwal, N.R.; King, L.S.; D’Alessio, F.R. Diverse macrophage populations mediate acute lung inflammation and resolution. Am. J. Physiol. Cell. Mol. Physiol. 2014, 306, L709–L725. [Google Scholar] [CrossRef] [PubMed]
- Samanta, S.; Zhou, Z.; Rajasingh, S.; Panda, A.; Sampath, V.; Rajasingh, J. DNMT and HDAC inhibitors together abrogate endotoxemia mediated macrophage death by STAT3-JMJD3 signaling. Int. J. Biochem. Cell Biol. 2018, 102, 117–127. [Google Scholar] [CrossRef]
- Thangavel, J.; Samanta, S.; Rajasingh, S.; Barani, B.; Xuan, Y.-T.; Dawn, B.; Rajasingh, J. Epigenetic modifiers reduce inflammation and modulate macrophage phenotype during endotoxemia-induced acute lung injury. J. Cell Sci. 2015, 128, 3094–3105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, U.; Rajasingh, S.; Samanta, S.; Cao, T.; Dawn, B.; Rajasingh, J. Macrophage polarization in response to epigenetic modifiers during infection and inflammation. Drug Discov. Today 2017, 22, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.N.; Das, S.R.; Emin, M.T.; Wei, M.; Sun, L.; Westphalen, K.; Rowlands, D.J.; Quadri, S.K.; Bhattacharya, S.; Bhattacharya, J. Mitochondrial transfer from bone-marrow–derived stromal cells to pulmonary alveoli protects against acute lung injury. Nat. Med. 2012, 18, 759–765. [Google Scholar] [CrossRef] [Green Version]
- Looney, M.R.; Nguyen, J.X.; Hu, Y.; Van Ziffle, J.A.; Lowell, C.A.; Matthay, M.A. Platelet depletion and aspirin treatment protect mice in a two-event model of transfusion-related acute lung injury. J. Clin. Investig. 2009, 119, 3450–3461. [Google Scholar] [CrossRef] [Green Version]
- Brodie, D.; Bacchetta, M. Extracorporeal Membrane Oxygenation for ARDS in Adults. New Engl. J. Med. 2011, 365, 1905–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viola, A.; Munari, F.; Sánchez-Rodríguez, R.; Scolaro, T.; Castegna, A. The Metabolic Signature of Macrophage Responses. Front. Immunol. 2019, 10, 1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Chu, C.; Wu, Z.; Liu, F.; Xie, J.; Yang, Y.; Qiu, H. IFIH1 Contributes to M1 Macrophage Polarization in ARDS. Front. Immunol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.P.; Cash, M.N.; Santostefano, K.E.; Nakanishi, M.; Terada, N.; Wallet, M.A. CRISPR/Cas9 knockout of USP18 enhances type I IFN responsiveness and restricts HIV-1 infection in macrophages. J. Leukoc. Biol. 2018, 103, 1225–1240. [Google Scholar] [CrossRef] [PubMed]
- Gerrick, K.Y.; Gerrick, E.R.; Gupta, A.; Wheelan, S.J.; Yegnasubramanian, S.; Jaffee, E.M. Transcriptional profiling identifies novel regulators of macrophage polarization. PLoS ONE 2018, 13, e0208602. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).