Measuring Foot Progression Angle during Walking Using Force-Plate Data




Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Material and Experimental Protocol
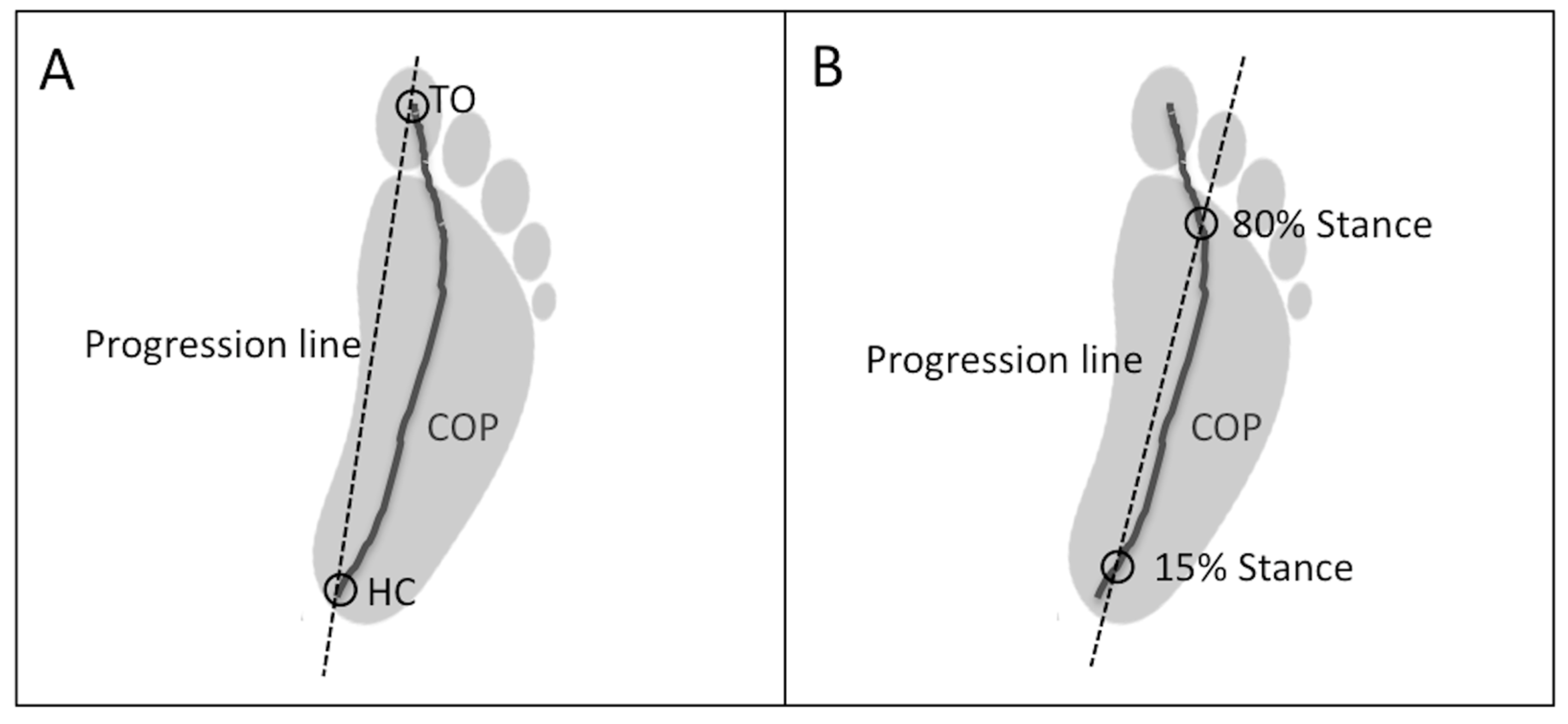
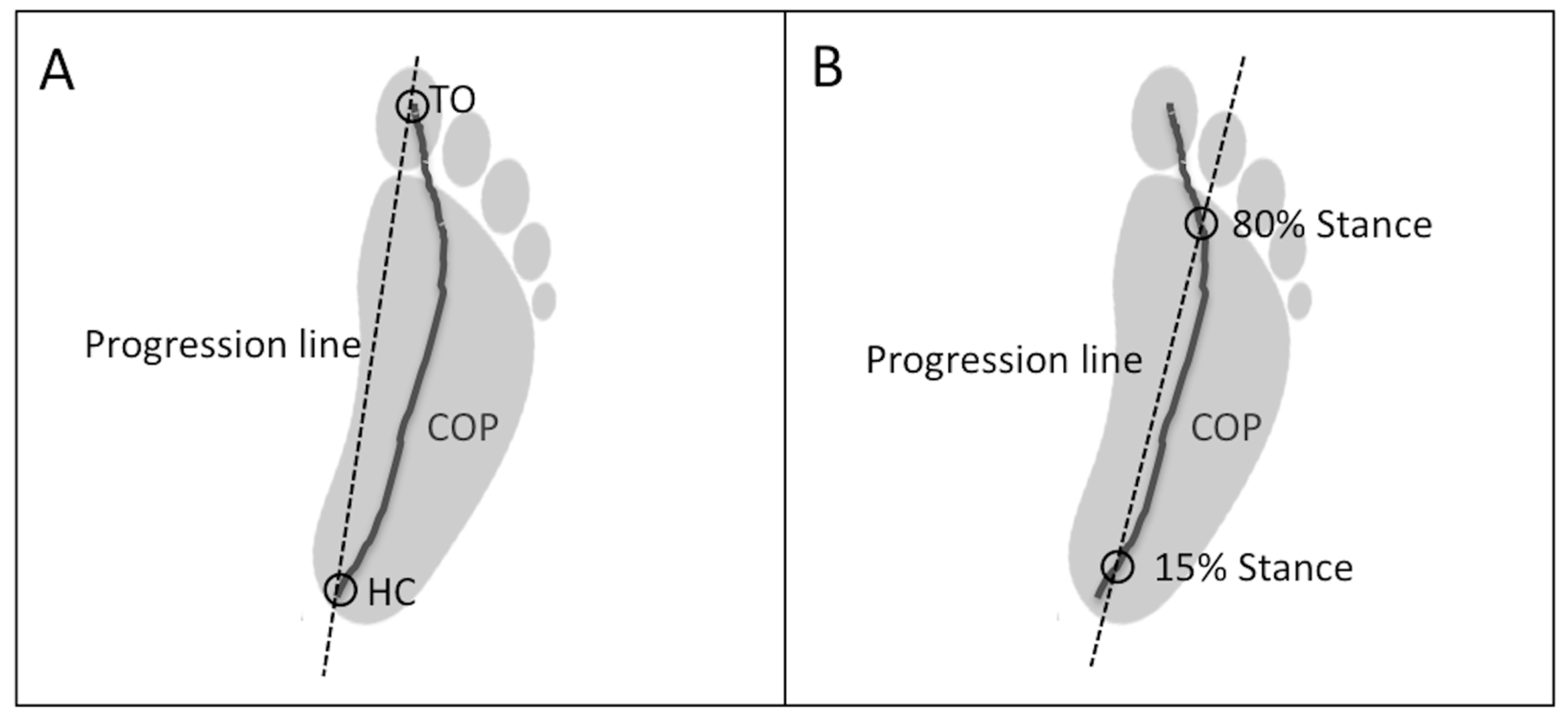
2.3. Data Analysis
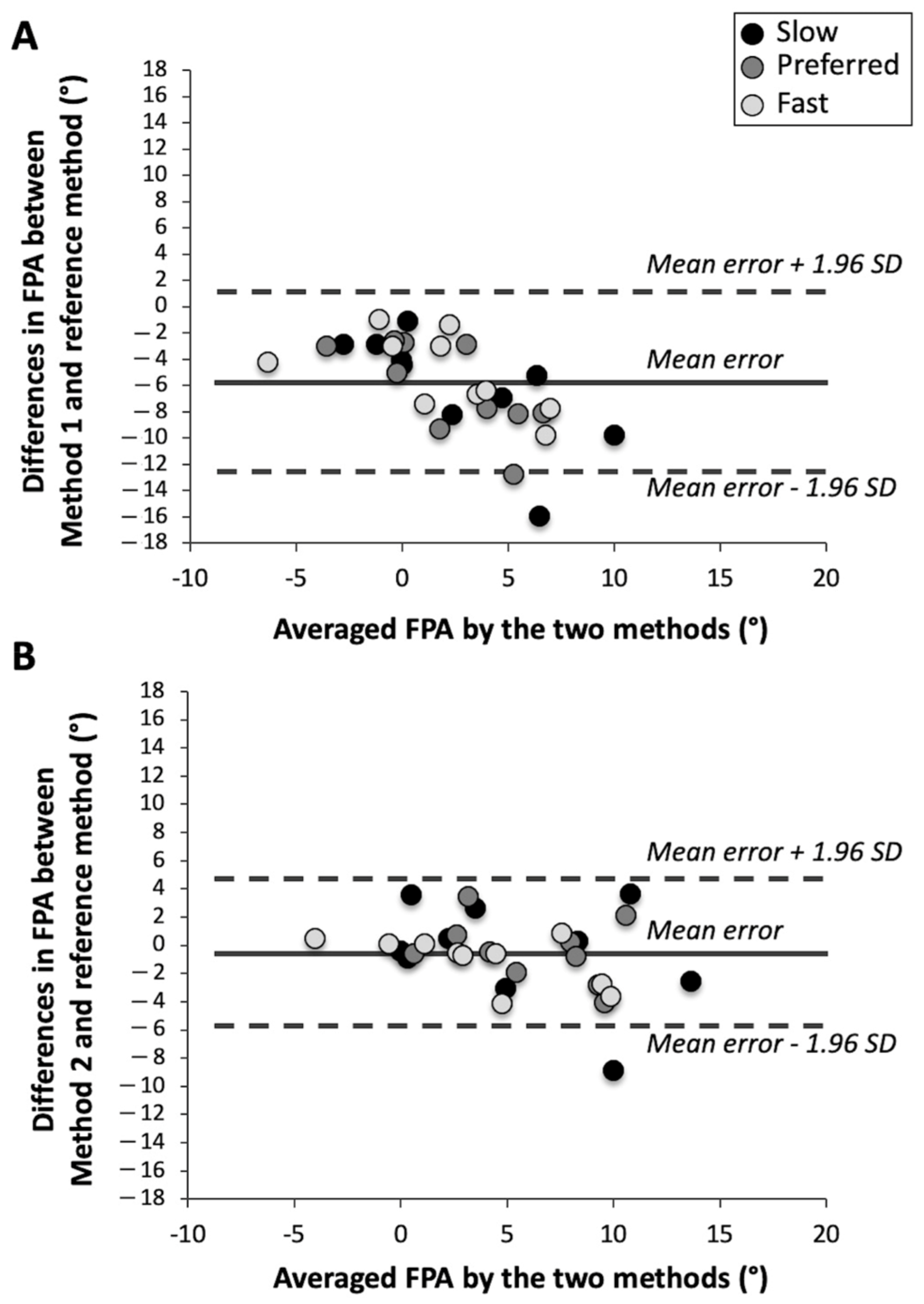
2.4. Statistical Analysis
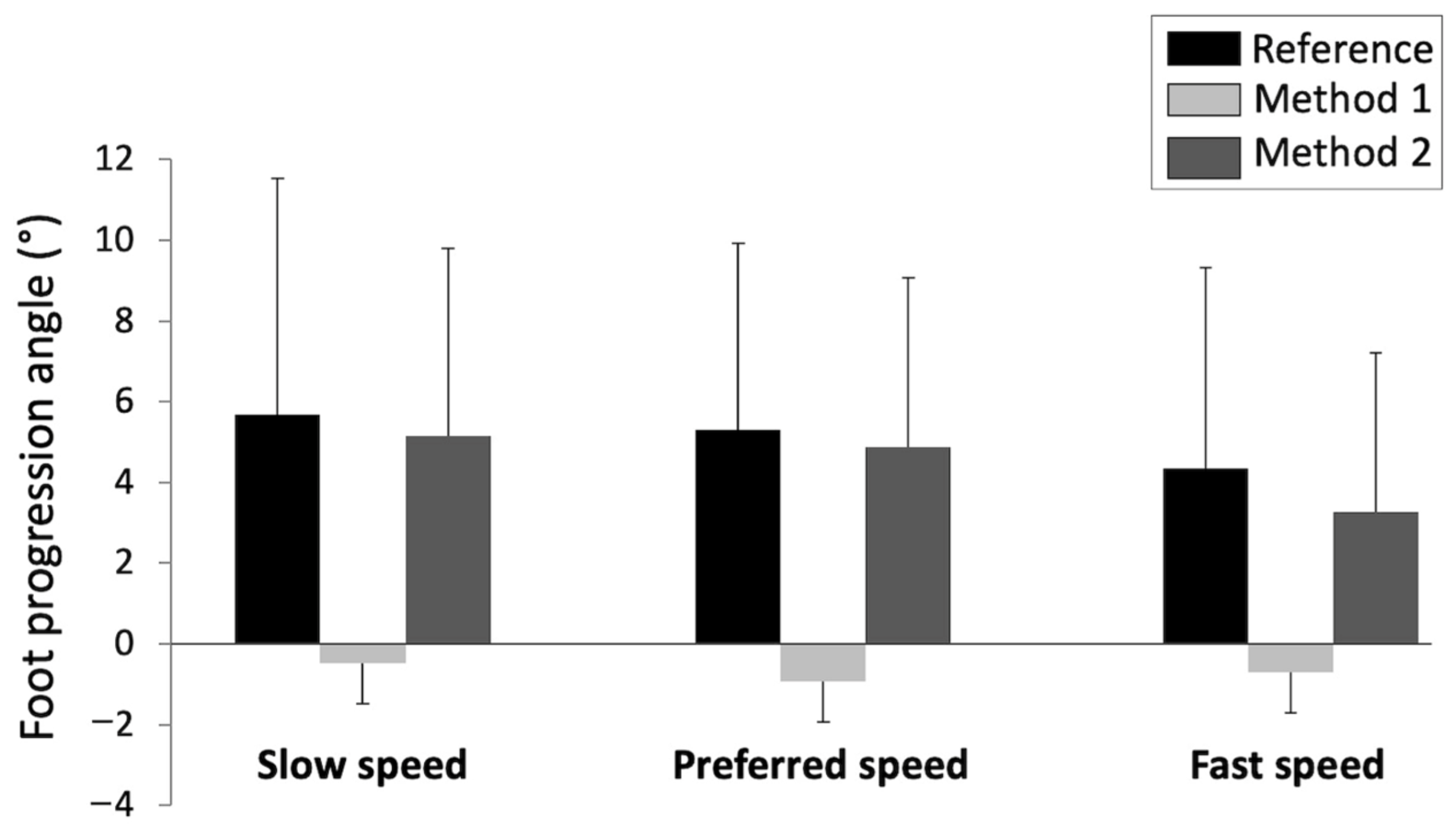
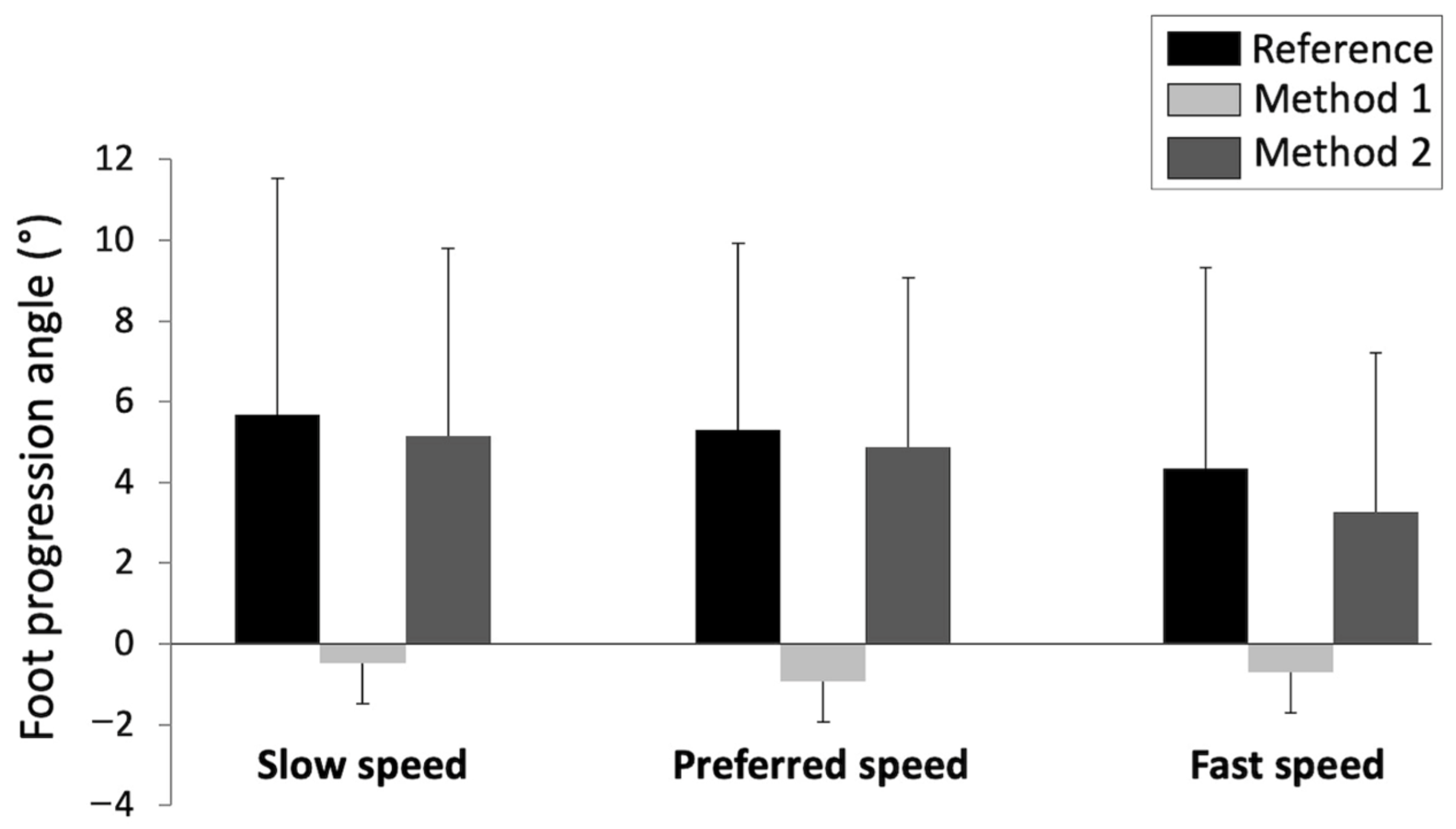
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cibulka, M.T.; Winters, K.; Kampwerth, T.; McAfee, B.; Payne, L.; Roeckenhaus, T.; Ross, S.A. Predicting Foot Progression Angle during Gait Using Two Clinical Measures in Healthy Adults, a Preliminary Study. Int. J. Sports Phys. Ther. 2016, 11, 400–408. [Google Scholar] [PubMed]
- Hudson, D. The rotational profile: A study of lower limb axial torsion, hip rotation, and the foot progression angle in healthy adults. Gait Posture 2016, 49, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, D.J.; Hubley-Kozey, C.L.; Deluzio, K.J.; Stanish, W.D.; Dunbar, M. Foot progression angle and the knee adduction moment: A cross-sectional investigation in knee osteoarthritis. Osteoarthr. Cartil. 2008, 16, 883–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shull, P.B.; Shultz, R.; Silder, A.; Dragoo, J.L.; Besier, T.F.; Cutkosky, M.R.; Delp, S.L. Toe-in gait reduces the first peak knee adduction moment in patients with medial compartment knee osteoarthritis. J. Biomech. 2013, 46, 122–128. [Google Scholar] [CrossRef]
- Ho, C.S.; Lin, C.J.; Chou, Y.L.; Su, F.C.; Lin, S.C. Foot progression angle and ankle joint complex in preschool children. Clin. Biomech. 2000, 15, 271–277. [Google Scholar] [CrossRef]
- Bowsher, K.A.; Vaughan, C.L. Effect of foot-progression angle on hip joint moments during gait. J. Biomech. 1995, 28, 759–762. [Google Scholar] [CrossRef]
- Rosenbaum, D. Foot loading patterns can be changed by deliberately walking with in-toeing or out-toeing gait modifications. Gait Posture 2013, 38, 1067–1069. [Google Scholar] [CrossRef]
- Shull, P.B.; Silder, A.; Shultz, R.; Dragoo, J.L.; Besier, T.F.; Delp, S.L.; Cutkosky, M.R. Six-week gait retraining program reduces knee adduction moment, reduces pain, and improves function for individuals with medial compartment knee osteoarthritis. J. Orthop. Res. 2013, 31, 1020–1025. [Google Scholar] [CrossRef]
- Chang, A.; Hurwitz, D.; Dunlop, D.; Song, J.; Cahue, S.; Hayes, K.; Sharma, L. The relationship between toe-out angle during gait and progression of medial tibiofemoral osteoarthritis. Ann. Rheum Dis. 2007, 66, 1271–1275. [Google Scholar] [CrossRef]
- Simic, M.; Wrigley, T.V.; Hinman, R.S.; Hunt, M.A.; Bennell, K.L. Altering foot progression angle in people with medial knee osteoarthritis: The effects of varying toe-in and toe-out angles are mediated by pain and malalignment. Osteoarthr. Cartil. 2013, 21, 1272–1280. [Google Scholar] [CrossRef] [Green Version]
- Xia, H.; Xu, J.; Wang, J.; Hunt, M.A.; Shull, P.B. Validation of a smart shoe for estimating foot progression angle during walking gait. J. Biomech. 2017, 61, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Caderby, T.; Yiou, E.; Peyrot, N.; Bonazzi, B.; Dalleau, G. Detection of swing heel-off event in gait initiation using force-plate data. Gait Posture 2013, 37, 463–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods towards Developing a Markerless System. Sports Med. Open 2018, 4, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Jirattigalachote, W.; Cutkosky, M.R.; Zhu, X.; Shull, P.B. Novel Foot Progression Angle Algorithm Estimation via Foot-Worn, Magneto-Inertial Sensing. IEEE Trans. Biomed. Eng. 2016, 63, 2278–2285. [Google Scholar] [CrossRef]
- Karatsidis, A.; Richards, R.E.; Konrath, J.M.; van den Noort, J.C.; Schepers, H.M.; Bellusci, G.; Harlaar, J.; Veltink, P.H. Validation of wearable visual feedback for retraining foot progression angle using inertial sensors and an augmented reality headset. J. Neuroeng. Rehabil. 2018, 15, 78. [Google Scholar] [CrossRef]
- Wouda, F.J.; Jaspar, S.; Harlaar, J.; van Beijnum, B.F.; Veltink, P.H. Foot progression angle estimation using a single foot-worn inertial sensor. J. Neuroeng. Rehabil. 2021, 18, 37. [Google Scholar] [CrossRef]
- Ziagkas, E.; Loukovitis, A.; Zekakos, D.X.; Chau, T.D.; Petrelis, A.; Grouios, G.A. Novel Tool for Gait Analysis: Validation Study of the Smart Insole PODOSmart®. Sensors 2021, 21, 5972. [Google Scholar] [CrossRef]
- Young, J.; Simic, M.; Simic, M. A Novel Foot Progression Angle Detection Method. In Computer Vision in Control Systems-4; Favorskaya, M., Jain, L., Eds.; Springer: Cham, Switzerland, 2018; Volume 136, pp. 299–317. [Google Scholar]
- Ledoux, W.R.; Hillstrom, H.J. The distributed plantar vertical force of neutrally aligned and pes planus feet. Gait Posture 2002, 15, 1–9. [Google Scholar] [CrossRef]
- Jameson, E.G.; Davids, J.R.; Anderson, J.P.; Davis, R.B.; Blackhurst, D.W.; Christopher, L.M. Dynamic pedobarography for children: Use of the center of pressure progression. J. Pediatr. Orthop. 2008, 28, 254–258. [Google Scholar] [CrossRef]
- Hagins, M.; Pappas, E. Biomechanics of the foot and ankle. In Biomechanics of the Foot and Ankle; Nordin, M., Frankel, V.H., Eds.; LWW: Philadelphia, PA, USA, 2012; pp. 206–253. [Google Scholar]
- Gefen, A.; Megido-Ravid, M.; Itzchak, Y.; Arcan, M. Biomechanical analysis of the three-dimensional foot structure during gait: A basic tool for clinical applications. J. Biomech. Eng. 2000, 122, 630–639. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Malatesta, D.; Canepa, M.; Menendez Fernandez, A. The effect of treadmill and overground walking on preferred walking speed and gait kinematics in healthy, physically active older adults. Eur. J. Appl. Physiol. 2017, 117, 1833–1843. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Biomechanics and Motor Control of Human Movement, 2nd ed.; Wiley: New York, NY, USA, 1990. [Google Scholar]
- Ghoussayni, S.; Stevens, C.; Durham, S.; Ewins, D. Assessment and validation of a simple automated method for the detection of gait events and intervals. Gait Posture 2004, 20, 266–272. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Slow Speed | Preferred Speed | Fast Speed | Effects | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Method 1 | Method 2 | Method 1 | Method 2 | Method 1 | Method 2 | Method | Speed | Interaction | |
| RE(°) | −6.1 ± 4.3 | −0.5 ± 3.7 | −6.2 ± 3.5 | −0.4 ± 2.2 | −5.1 ± 3.0 | −1.1 ± 1.8 | p < 0.01 | NS | NS |
| AE (°) | 6.2 ± 4.2 | 3.3 ± 2.1 | 6.2 ± 3.5 | 2.0 ± 1.2 | 5.1 ± 2.9 | 2.0 ± 1.2 | p < 0.01 | NS | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caderby, T.; Begue, J.; Dalleau, G.; Peyrot, N. Measuring Foot Progression Angle during Walking Using Force-Plate Data. Appl. Mech. 2022, 3, 174-181. https://doi.org/10.3390/applmech3010013
Caderby T, Begue J, Dalleau G, Peyrot N. Measuring Foot Progression Angle during Walking Using Force-Plate Data. Applied Mechanics. 2022; 3(1):174-181. https://doi.org/10.3390/applmech3010013
Chicago/Turabian StyleCaderby, Teddy, Jérémie Begue, Georges Dalleau, and Nicolas Peyrot. 2022. "Measuring Foot Progression Angle during Walking Using Force-Plate Data" Applied Mechanics 3, no. 1: 174-181. https://doi.org/10.3390/applmech3010013
APA StyleCaderby, T., Begue, J., Dalleau, G., & Peyrot, N. (2022). Measuring Foot Progression Angle during Walking Using Force-Plate Data. Applied Mechanics, 3(1), 174-181. https://doi.org/10.3390/applmech3010013