

Impingement During Dislocation-Prone Activities: Geometric Modeling Analysis of an Uncemented Standard Versus Modular Dual Mobility Acetabular Cups

 , , , and
, , , and
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
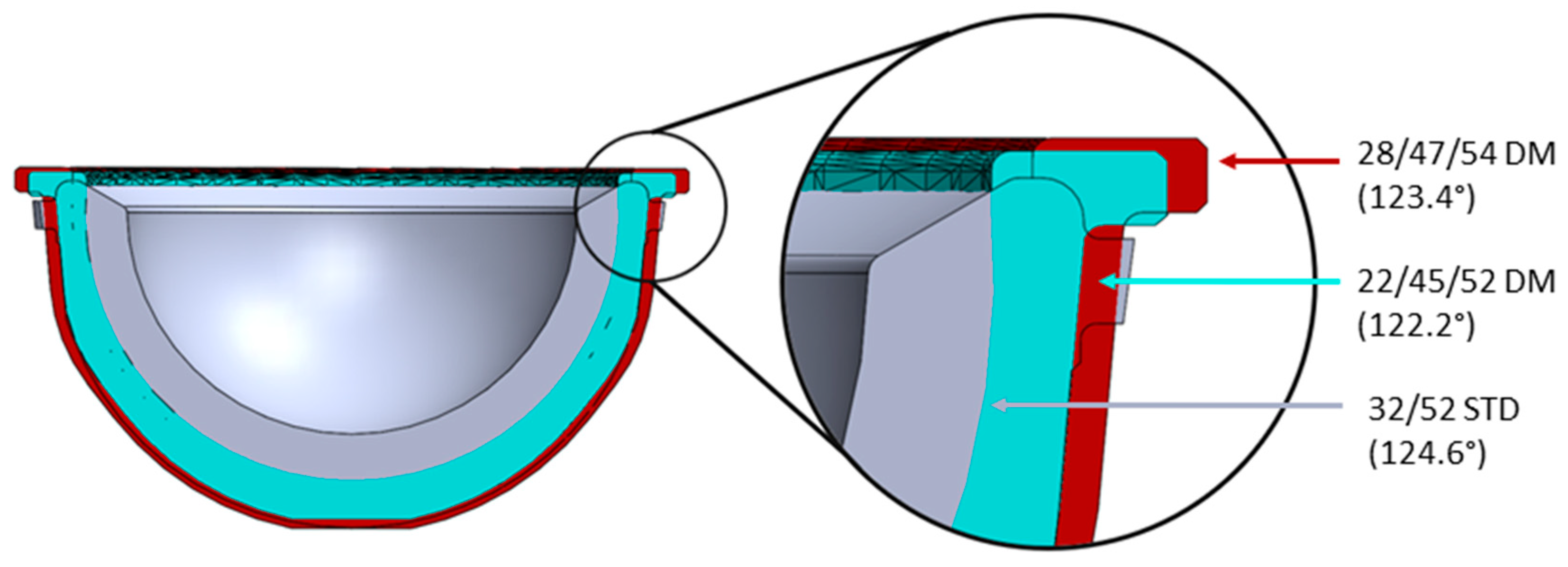
2.1. Components
2.2. Geometric Modeling
3. Results
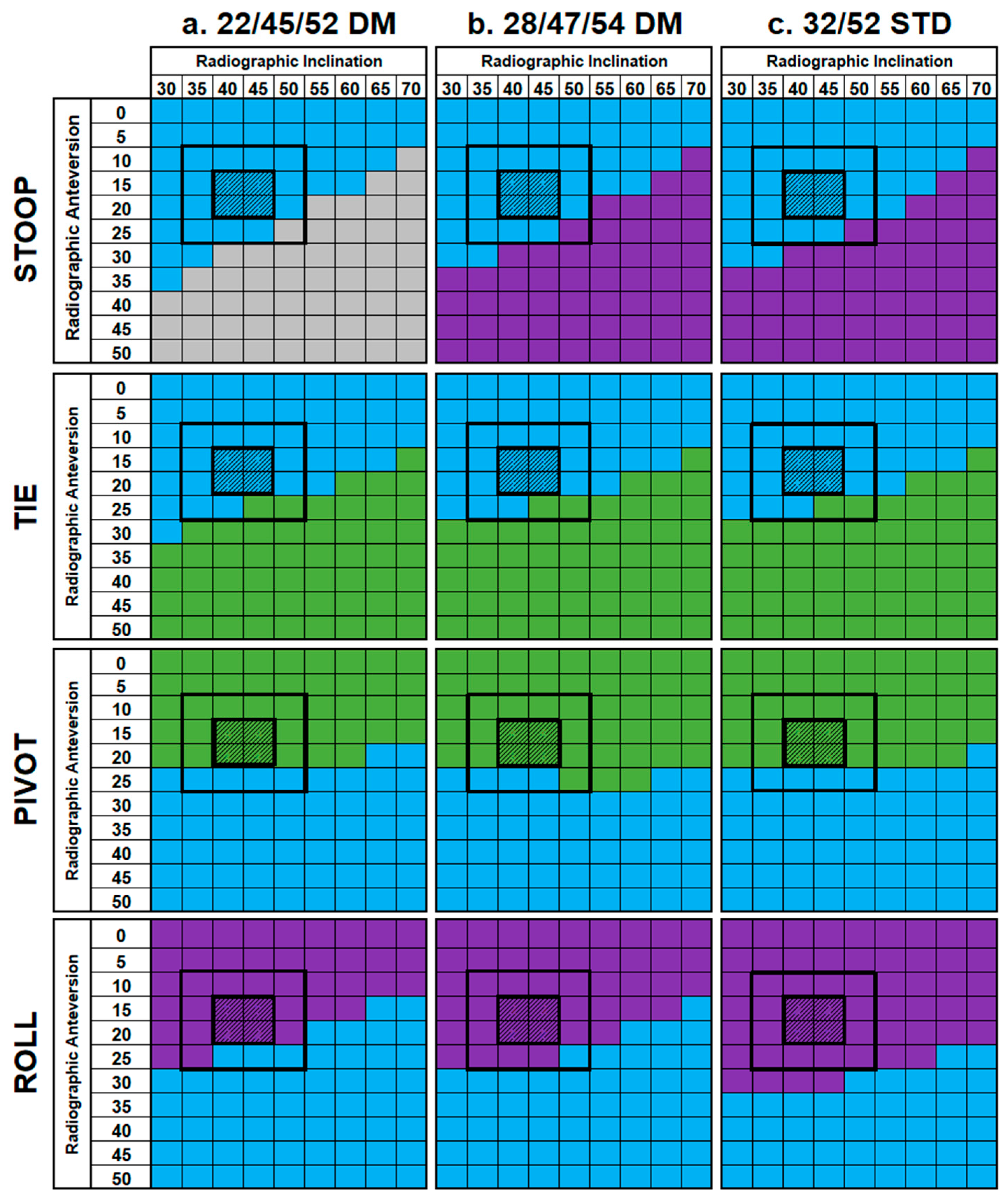
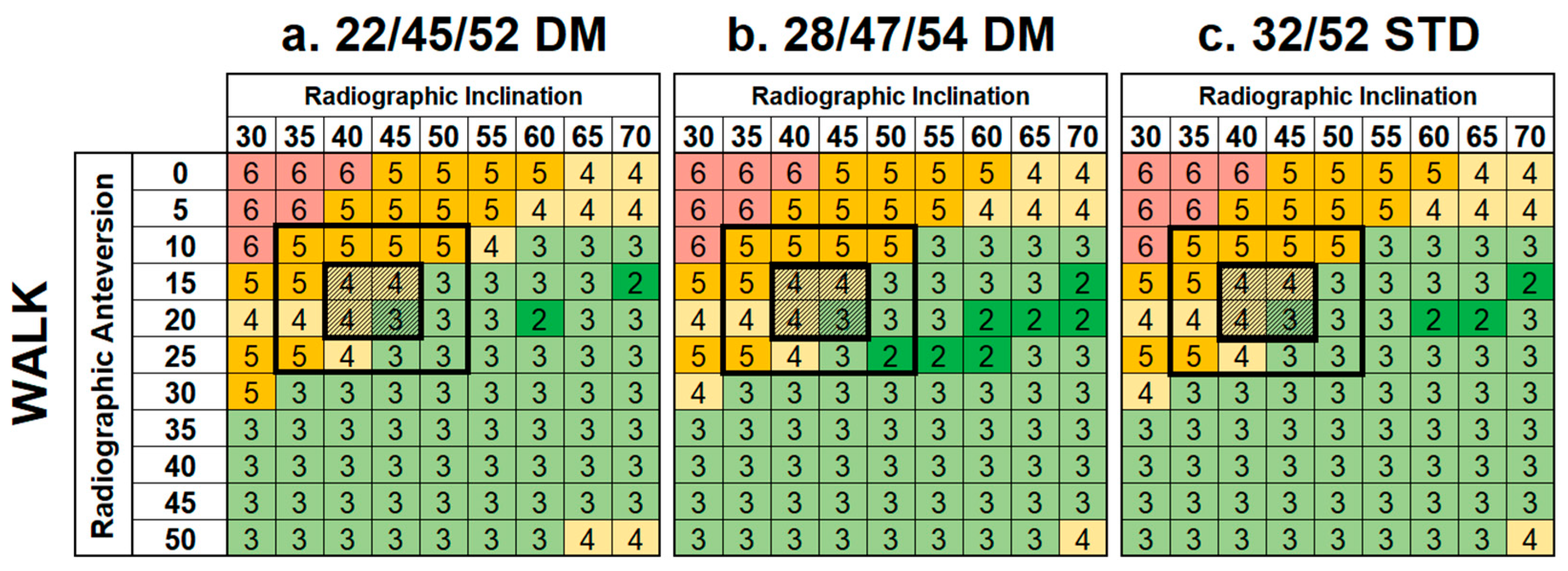
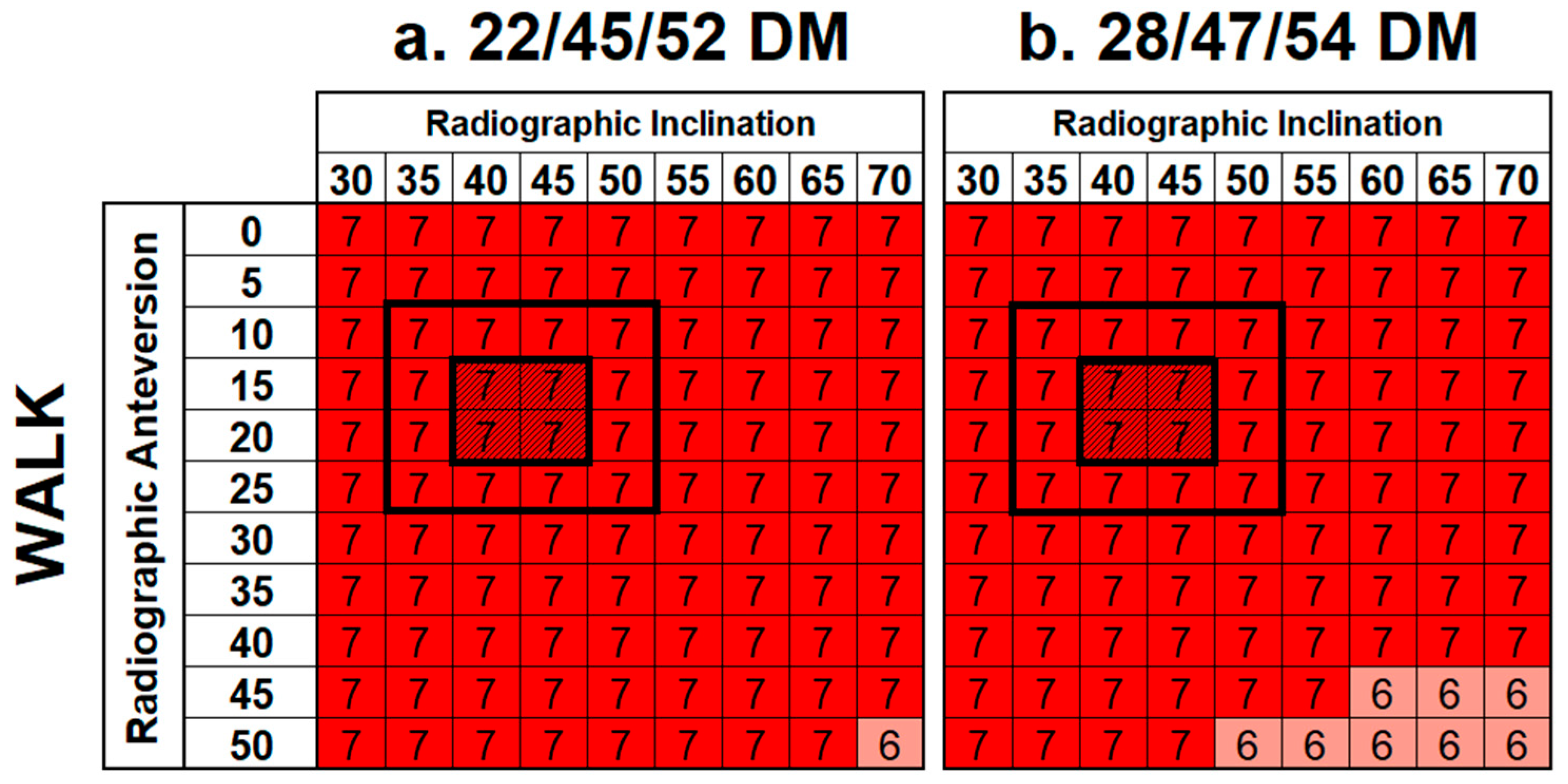
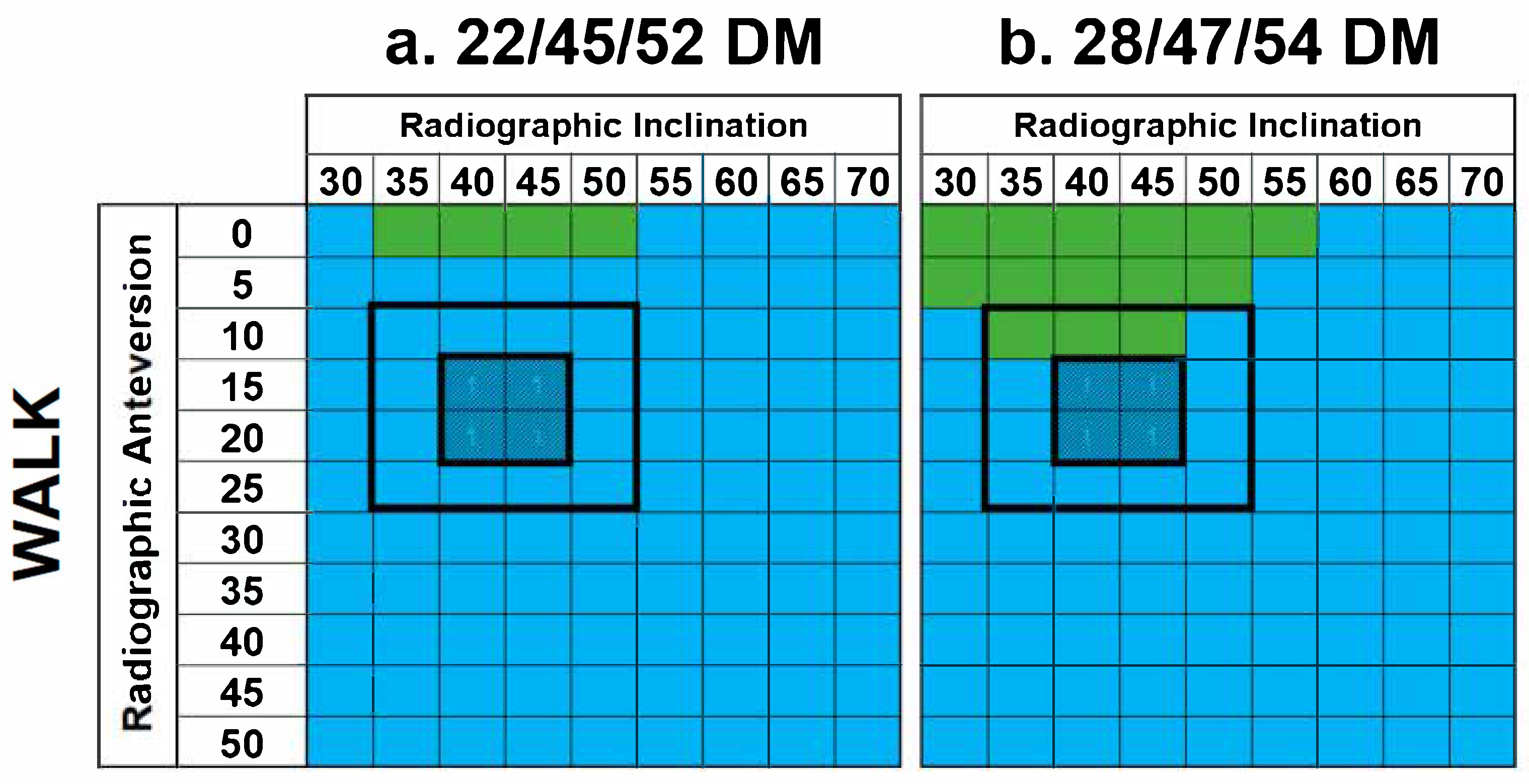
3.1. Incidence of Impingement in Constructs
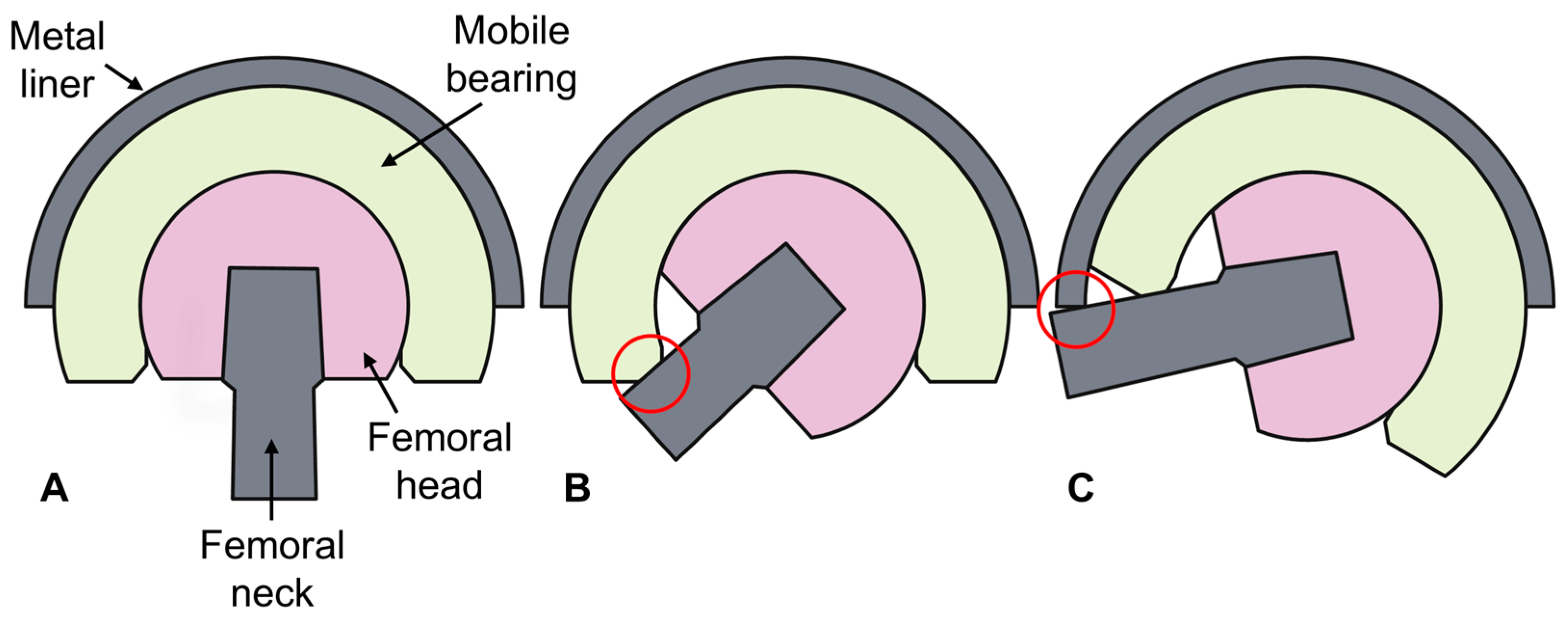
3.2. Incidence of Femoral Neck–Mobile Bearing Contact in DM Cups
3.3. Range of Motion of Constructs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| THA | Total hip arthroplasty |
| DM | Dual mobility |
| CAD | Computer-aided design |
| OD | Outer diameter |
| ID | Inner diameter |
| ADL | Activity of daily living |
| ROM | Range of motion |
References
- National Joint Registry. 21st Annual Report 2024. 2024. Available online: www.njrcentre.org.uk (accessed on 11 March 2025).
- American Joint Replacement Registry. The Eleventh Annual Report of the AJRR on Hip and Knee Arthroplasty. 2024. Available online: https://www.aaos.org/registries/publications/ajrr-annual-report/ (accessed on 11 March 2025).
- Masaoka, T.; Yamamoto, K.; Shishido, T.; Katori, Y.; Mizoue, T.; Shirasu, H.; Nunoda, D. Study of hip joint dislocation after total hip arthroplasty. Int. Orthop. 2006, 30, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Woolson, S.T.; Rahimtoola, Z.O. Risk Factors for Dislocation During the First 3 Months After Primary Total Hip Replacement. J. Arthroplast. 1999, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Galvain, T.; Mantel, J.; Kakade, O.; Board, T.N. Treatment patterns and clinical and economic burden of hip dislocation following primary total hip arthroplasty in England. Bone Joint J. 2022, 104, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Laura, A.D.; Hothi, H.; Battisti, C.; Cerquiglini, A.; Henckel, J.; Skinner, J.; Hart, A. Wear of dual-mobility cups: A review article. Int. Orthop. 2017, 41, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.P.; Weitzler, L.; Salvatore, A.; Wright, T.M.; Westrich, G.H. A Retrieval Analysis of Impingement in Dual-Mobility Liners. J. Arthroplast. 2018, 33, 2660–2665. [Google Scholar] [CrossRef] [PubMed]
- W-Dahl, A.; Kärrholm, J.; Rogmark, C.; Nauclér, E.; Nåtman, J.; Bülow, E.; Arani, P.I.; Mohaddes, M.; Rolfson, O. The Swedish Arthroplasty Register Annual Report 2023; Swedish Arthroplasty Register: Gothenburg, Sweden, 2023; Available online: https://sar.registercentrum.se/ (accessed on 11 March 2025).
- Darrith, B.; Courtney, P.M.; Della Valle, C.J. Outcomes of dual mobility components in total hip arthroplasty: A systematic review of the literature. Bone Joint J. 2018, 100, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Reina, N.; Pareek, A.; Krych, A.J.; Pagnano, M.W.; Berry, D.J.; Abdel, M.P. Dual-Mobility Constructs in Primary and Revision Total Hip Arthroplasty: A Systematic Review of Comparative Studies. J. Arthroplast. 2019, 34, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Khatod, M.; Chan, P.H.; Prentice, H.A.; Fasig, B.H.; Paxton, E.W.; Reddy, N.C.; Kelly, M.P. Can Dual Mobility Cups Reduce Revision and Dislocation Risks? An Analysis of 107,528 Primary Total Hip Arthroplasties in the United States. J. Arthroplast. 2024, 39, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, W.; Bingham, R.; Dyer, C.; Rainbird, S.; Graves, S.E. A Comparison of Revision Rates for Dislocation and Aseptic Causes Between Dual Mobility and Large Femoral Head Bearings in Primary Total Hip Arthroplasty With Subanalysis by Acetabular Component Size: An Analysis of 106,163 Primary Total Hip Arthroplasties. J. Arthroplast. 2021, 36, 3233–3240. [Google Scholar] [CrossRef] [PubMed]
- Pryce, G.M.; Sabu, B.; Al-Hajjar, M.; Wilcox, R.K.; Thompson, J.; Isaac, G.H.; Board, T.; Williams, S. Impingement in total hip arthroplasty: A geometric model. Proc. Inst. Mech. Eng. H 2022, 236, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Nadzadi, M.E.; Pedersen, D.R.; Yack, H.J.; Callaghan, J.J.; Brown, T.D. Kinematics, kinetics, and finite element analysis of commonplace maneuvers at risk for total hip dislocation. J. Biomech. 2003, 36, 577–591. [Google Scholar] [CrossRef] [PubMed]
- BS ISO 14242-1:2014+A1:2018; Implants for Surgery—Wear of Total Hip-Joint Prostheses (Part 1: Loading and Displacement Parameters for Wear-Testing Machines and Corresponding Environmental Conditions for Test). International Organization for Standardization: Geneva, Switzerland, 2018.
- Smeeton, M.; Williams, S.; Anderson, J.; Wilcox, R.; Board, T.; Williams, S.; Isaac, G. A Geometric Model of Impingement During Dislocation Prone Activities in Dual Mobility, Lipped Liner and Standard Acetabular Cups; [Dataset]; University of Leeds: Leeds, UK, 2024. [Google Scholar] [CrossRef]
- Rittmeister, M.; Callitsis, C. Factors influencing cup orientation in 500 consecutive total hip replacements. Clin. Orthop. Relat. Res. 2006, 445, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Danoff, J.R.; Bobman, J.T.; Cunn, G.; Murtaugh, T.; Gorroochurn, P.; Geller, J.A.; Macaulay, W. Redefining the Acetabular Component Safe Zone for Posterior Approach Total Hip Arthroplasty. J. Arthroplast. 2016, 31, 506–511. [Google Scholar] [CrossRef]
- McCollum, D.E.; Gray, W.J. Dislocation after total hip arthroplasty. Causes and prevention. Clin. Orthop. Relat. Res. 1990, 261, 159–170. [Google Scholar] [CrossRef]
- Brown, T.D.; Callaghan, J.J. Impingement in total hip replacement: Mechanisms and consequences. Curr. Orthop. 2008, 22, 376–391. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Li, J.; Jin, Z.; Fisher, J. The contact mechanics and occurrence of edge loading in modular metal-on-polyethylene total hip replacement during daily activities. Med. Eng. Phys. 2016, 38, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Spece, H.; MacDonald, D.W.; Mont, M.A.; Lee, G.-C.; Kurtz, S.M. Fretting Corrosion and Polyethylene Damage Mechanisms in Modular Dual Mobility Total Hip Arthroplasty. In Beyond the Implant: Retrieval Analysis Methods for Implant Surveillance; ASTM International: West Conshoshocken, PA, USA, 2018; pp. 106–117. [Google Scholar] [CrossRef]
- Di Laura, A.; Hothi, H.S.; Henckel, J.; Cerquiglini, A.; Liow, M.H.L.; Kwon, Y.M.; Skinner, J.A.; Hart, A.J. Retrieval evidence of impingement at the third articulation in contemporary dual mobility cups for total hip arthroplasty. Int. Orthop. 2017, 41, 2495–2501. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smeeton, M.; Williams, S.P.; Anderson, J.; Wilcox, R.; Board, T.; Williams, S.; Isaac, G. Impingement During Dislocation-Prone Activities: Geometric Modeling Analysis of an Uncemented Standard Versus Modular Dual Mobility Acetabular Cups. Prosthesis 2025, 7, 59. https://doi.org/10.3390/prosthesis7030059
Smeeton M, Williams SP, Anderson J, Wilcox R, Board T, Williams S, Isaac G. Impingement During Dislocation-Prone Activities: Geometric Modeling Analysis of an Uncemented Standard Versus Modular Dual Mobility Acetabular Cups. Prosthesis. 2025; 7(3):59. https://doi.org/10.3390/prosthesis7030059
Chicago/Turabian StyleSmeeton, Mackenzie, Simon P. Williams, James Anderson, Ruth Wilcox, Tim Board, Sophie Williams, and Graham Isaac. 2025. "Impingement During Dislocation-Prone Activities: Geometric Modeling Analysis of an Uncemented Standard Versus Modular Dual Mobility Acetabular Cups" Prosthesis 7, no. 3: 59. https://doi.org/10.3390/prosthesis7030059
APA StyleSmeeton, M., Williams, S. P., Anderson, J., Wilcox, R., Board, T., Williams, S., & Isaac, G. (2025). Impingement During Dislocation-Prone Activities: Geometric Modeling Analysis of an Uncemented Standard Versus Modular Dual Mobility Acetabular Cups. Prosthesis, 7(3), 59. https://doi.org/10.3390/prosthesis7030059