
Hip Replacement Following Intertrochanteric Osteosynthesis Failure: Is It Possible to Restore Normal Hip Biomechanics?

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanis, J.A.; Oden, A.; McCloskey, E.V.; Johansson, H.; Wahl, D.A.; Cooper, C.; IOF Working Group on Epidemiology and Quality of Life. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos. Int. 2012, 23, 2239–2256. [Google Scholar] [CrossRef] [PubMed]
- Mattisson, L.; Bojan, A.; Enocson, A. Epidemiology, treatment and mortality of trochanteric and subtrochanteric hip fractures: Data from the Swedish fracture register. BMC Musculoskelet. Disord. 2018, 19, 369. [Google Scholar] [CrossRef] [PubMed]
- Innocenti, M.; Civinini, R.; Carulli, C.; Matassi, F. Proximal femoral fractures: Epidemiology. Clin. Cases Miner. Bone Metab. 2009, 6, 117–119. [Google Scholar] [PubMed]
- Sambrook, P.; Cooper, C. Osteoporosis. Lancet 2006, 367, 2010–2018, Erratum in Lancet 2006, 368, 28. [Google Scholar] [CrossRef] [PubMed]
- Piazzolla, A.; Bizzoca, D.; Solarino, G.; Moretti, L.; Moretti, B. Vertebral fragility fractures: Clinical and radiological results of augmentation and fixation—A systematic review of randomized controlled clinical trials. Aging Clin. Exp. Res. 2020, 32, 1219–1232. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Maggi, S. Epidemiology and social costs of hip fracture. Injury 2018, 49, 1458–1460. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.M.; Magaziner, J.; Hebel, J.R.; Kenzora, J.E.; Kashner, T.M. Intertrochanteric versus femoral neck hip fractures: Differential characteristics, treatment, and sequelae. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 1999, 54, M635–M640. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Zhang, S.; Yang, J.; Dong, W.; Wang, S.; Cheng, Y.; Al-Qwbani, M.; Wang, Q.; Yu, B. Proximal femoral nail vs. dynamic hip screw in treatment of intertrochanteric fractures: A meta-analysis. Med. Sci. Monit. 2014, 20, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- Tawari, A.A.; Kempegowda, H.; Suk, M.; Horwitz, D.S. What made an intertrochanteric fracture unstable in 2015? Does the lateral wall play a role in the decision matrix? J. Orthop. Trauma 2015, 29 (Suppl. 4), S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Uppal, H.S. Hip Fractures: Relevant Anatomy, Classification, and Biomechanics of Fracture and Fixation. Geriatr. Orthop. Surg. Rehabil. 2019, 10, 2151459319859139. [Google Scholar] [CrossRef] [PubMed]
- Marsillo, E.; Pintore, A.; Asparago, G.; Oliva, F.; Maffulli, N. Cephalomedullary nailing for reverse oblique intertrochanteric fractures 31A3 (AO/OTA). Orthop. Rev. 2022, 14, 38560. [Google Scholar] [CrossRef] [PubMed]
- Queally, J.M.; Harris, E.; Handoll, H.H.; Parker, M.J. Intramedullary nails for extracapsular hip fractures in adults. Cochrane Database Syst. Rev. 2014, 9, CD004961. [Google Scholar] [CrossRef] [PubMed]
- Bizzoca, D.; Bortone, I.; Vicenti, G.; Caringella, N.; Rifino, F.; Moretti, B. Gait analysis in the postoperative assessment of intertrochanteric femur fractures. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 3), 345–351. [Google Scholar] [PubMed]
- Méndez-Ojeda, M.M.; Herrera-Rodríguez, A.; Álvarez-Benito, N.; González-Pacheco, H.; García-Bello, M.A.; Álvarez-de la Cruz, J.; Pais-Brito, J.L. Treatment of Trochanteric Hip Fractures with Cephalomedullary Nails: Single Head Screw vs. Dual Integrated Compression Screw Systems. J. Clin. Med. 2023, 12, 3411. [Google Scholar] [CrossRef]
- Zeelenberg, M.L.; Nugteren, L.H.T.; Plaisier, A.C.; Loggers, S.A.I.; Joosse, P.; Den Hartog, D.; Verhofstad, M.H.J.; van Lieshout, E.M.M.; STABLE-HIP Study Group. Extramedullary versus intramedullary fixation of stable trochanteric femoral fractures: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2023, 143, 5065–5083. [Google Scholar] [CrossRef] [PubMed]
- Haidukewych, G.J.; Berry, D.J. Hip arthroplasty for salvage of failed treatment of intertrochanteric hip fractures. J. Bone Jt. Surg. Am. 2003, 85, 899–904. [Google Scholar] [CrossRef]
- Solarino, G.; Bizzoca, D.; Dramisino, P.; Vicenti, G.; Moretti, L.; Moretti, B.; Piazzolla, A. Total hip arthroplasty following the failure of intertrochanteric nailing: First implant or salvage surgery? World J. Orthop. 2023, 14, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Hardinge, K. The direct lateral approach to the hip. J. Bone Jt. Surg. Br. 1982, 64, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Zhan, K.; Zhang, L.; Zeng, D.; Yu, W.; Zhang, X.; Zhao, M. Conversion to total hip arthroplasty after failed proximal femoral nail antirotations or dynamic hip screw fixations for stable intertrochanteric femur fractures: A retrospective study with a minimum follow-up of 3 years. BMC Musculoskelet. Disord. 2017, 18, 38. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Han, X.; Chen, W.; Mao, S.; Zhao, M.; Zhang, X.; Han, G.; Ye, J.; Chen, M.; Zhuang, J. Conversion from a failed proximal femoral nail anti-rotation to a cemented or uncemented total hip arthroplasty device: A retrospective review of 198 hips with previous intertrochanteric femur fractures. BMC Musculoskelet. Disord. 2020, 21, 791. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patients (n = 31) | |
|---|---|
| Age | |
| Mean ± SD | 76.2 ± 6.84 |
| Gender | |
| Female, n (%) | 21 (67.74%) |
| BMI (kg/m2) | |
| Mean ± SD | 27.8 ± 4.76 |
| Side | |
| Right, n (%) | 16 (51.61%) |
| Timing from nailing to THA (mean ± SD, months) | 11.86 ± 10.3 |
| Mean operating time (mean ± SD, minutes) | 101 ± 48.73 |
| Patients undergoing ≥3 blood transfusions, n (%) | 17 (54.84%) |
| VAS (mean ± SD, at the final follow-up) | 2.3 ± 3.45 |
| Healthy Hip | Affected Hip | ∆ | p | |
|---|---|---|---|---|
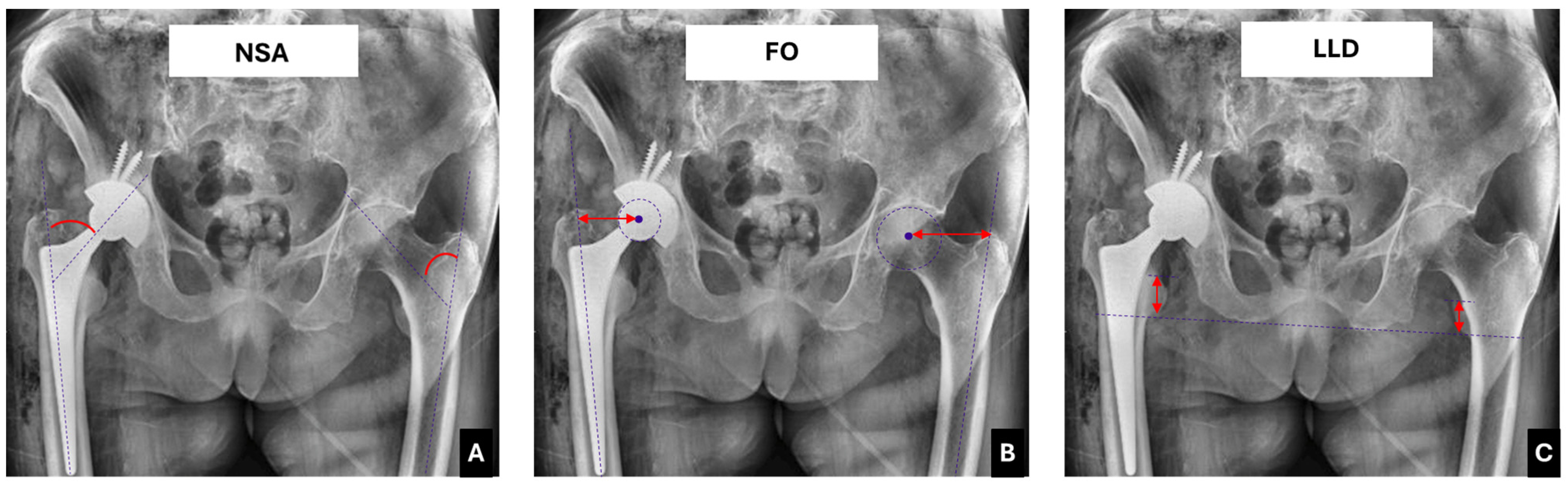
| Neck shaft angle (NSA) | 127.7 ± 5.6° | 135.1 ± 2.4° | 7.4 ± 2.6° | <0.001 * |
| Femoral offset (FO) | 42.4 ± 2.7 mm | 51.4 ± 7.42 mm | 9 ± 3.2 mm | <0.001 * |
| Limb length discrepancy (LLD) | - | - | 8.35 ± 2.25 mm | - |
| HHS | VAS | |||
|---|---|---|---|---|
| R | p | R | p | |
| ∆NSA | −0.61 | 0.01 * | 0.41 | 0.095 |
| ∆FO | −0.56 | 0.03 * | 0.24 | 0.176 |
| ∆LLD | −0.21 | 0.112 | 0.13 | 0.223 |
| Patients (n = 31) | ||
|---|---|---|
| N | Percentage | |
| Periprosthetic fractures | 3 | 9.6% |
| Implant instability | 1 | 3.23% |
| THA dislocation | 1 | 3.23% |
| Periprosthetic Joint Infections | 2 | 6.45% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bizzoca, D.; Giannini, G.; Cannito, F.D.; Colasuonno, G.; De Giosa, G.; Solarino, G. Hip Replacement Following Intertrochanteric Osteosynthesis Failure: Is It Possible to Restore Normal Hip Biomechanics? Prosthesis 2025, 7, 50. https://doi.org/10.3390/prosthesis7030050
Bizzoca D, Giannini G, Cannito FD, Colasuonno G, De Giosa G, Solarino G. Hip Replacement Following Intertrochanteric Osteosynthesis Failure: Is It Possible to Restore Normal Hip Biomechanics? Prosthesis. 2025; 7(3):50. https://doi.org/10.3390/prosthesis7030050
Chicago/Turabian StyleBizzoca, Davide, Giorgio Giannini, Francesco Domenico Cannito, Giulia Colasuonno, Giuseppe De Giosa, and Giuseppe Solarino. 2025. "Hip Replacement Following Intertrochanteric Osteosynthesis Failure: Is It Possible to Restore Normal Hip Biomechanics?" Prosthesis 7, no. 3: 50. https://doi.org/10.3390/prosthesis7030050
APA StyleBizzoca, D., Giannini, G., Cannito, F. D., Colasuonno, G., De Giosa, G., & Solarino, G. (2025). Hip Replacement Following Intertrochanteric Osteosynthesis Failure: Is It Possible to Restore Normal Hip Biomechanics? Prosthesis, 7(3), 50. https://doi.org/10.3390/prosthesis7030050