
Accuracy in the Plaster Model of Total Prosthetic Plates in Three Different Manufacturing Methods: In Vitro Study


 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Creation of the Model
- First impression: The impression of the upper arch is taken using alginate (irreversible hydrocolloid) and a commercial impression tray.
- First plaster model: From the alginate impression, a hard plaster model is obtained (the plaster we use is HydrocalKerrTM) on which to build the individual resin impression tray (impression tray resin LC—Henry Schein®).
- Second impression: The second impression is taken using Permlastic™ condensation polysulfide and the individual impression tray built on the previously obtained plaster model.
- Second plaster model: From the second impression, the definitive model is obtained using Class IV extra-hard plaster in order to have high resistance characteristics and smooth surfaces (Suprastone ultra-hard chalkTM) (Figure 1).
2.2. Construction of the Plates with the Three Methods
2.2.1. Traditional Method
- Waxing of the model: The plate is created on the plaster model with a sheet of wax (the teeth have been mounted in our model).
- Putting into the muffle: The plaster model with the waxing is inserted into the muffle (mold and counter-mold), and everything is placed in a kettle to melt the wax. Once the muffle has been opened and the mold and counter-mold have been washed with hot water to eliminate wax residues, we proceed to carry out the retentions in the teeth.
- Resin packing: The resin we have chosen is Promolux, a hot polymerizing resin with color stability based on methyl methacrylate. Once the powder is mixed with the liquid and the initial plasticity consistency is obtained, it is inserted into the muffle.
- Polymerization: The closed muffle is inserted into the kettle at a programmed temperature of 70 degrees for 30–60 min, and then the kettle brings the temperature to 100 degrees for 30 min.
- Finishing: After polymerization, the flask is opened, the resin prosthesis is removed, and it is finished with suitable cutters and rubbers (Figure 2).
2.2.2. CAD/CAM Method for Milling
- Model scanning: The plaster model inserted into the scanner is scanned to obtain a three-dimensional digital model using software.
- Design: The digital model obtained from the scan is imported into CAD software (Exocad®), where the digital model of the prosthetic plate is created
- Milling: Once the design of the prosthesis in the CAD software is completed, a CAM file is generated which is sent to a software that manages the milling machine (HyperDent®) that contains the information necessary for milling. A micro-filled disk in PMMA (Smile Cam®) is milled until the previously designed plate is obtained
- Verification and adaptation: The prosthetic plate is then tried on the model to verify the adaptation (Figure 3).
2.2.3. CAD/CAM Method for Addition
- Model scanning: The plaster model inserted into the scanner is scanned to obtain a three-dimensional digital model using software.
- Design: The digital model obtained from the scan is imported into Exocad® CAD software, where the digital model of the prosthetic plate is created.
- Printing of the plate: The digital model is prepared for printing, correctly positioning the prosthesis on the virtual support plate. The CAD file is sent to the Phrozen® 3D printer, where the printing parameters are set via a software that manages the 3D printer (Chitubox®), and the plaque is formed layer-by-layer. A Raydent® composite resin was used.
- Finishing: After printing, the plate is removed from the support plate and subjected to finishing and testing on the model to check the fit (Figure 4).
2.3. Creation of the Silicone Models to Be Examined
- a—Creation of the silicone with the prosthetic plate n° 1:Figure 6. (a) Base paste and catalyst mixture; (b) Fit Checker applied to the plate; (c) plate inserted into the model and application of controlled pressure; (d) silicone obtained from plate n°1.Figure 6. (a) Base paste and catalyst mixture; (b) Fit Checker applied to the plate; (c) plate inserted into the model and application of controlled pressure; (d) silicone obtained from plate n°1.
![Prosthesis 07 00042 g006a]()
![Prosthesis 07 00042 g006b]()
- b—Creation of the silicone with the prosthetic plate n. 2:Figure 7. (a) Base paste and catalyst paste; (b) mixture applied in the base obtained by milling; (c) Fit Checker applied to the plate; (d) silicone obtained from plate n° 2.Figure 7. (a) Base paste and catalyst paste; (b) mixture applied in the base obtained by milling; (c) Fit Checker applied to the plate; (d) silicone obtained from plate n° 2.
![Prosthesis 07 00042 g007]()
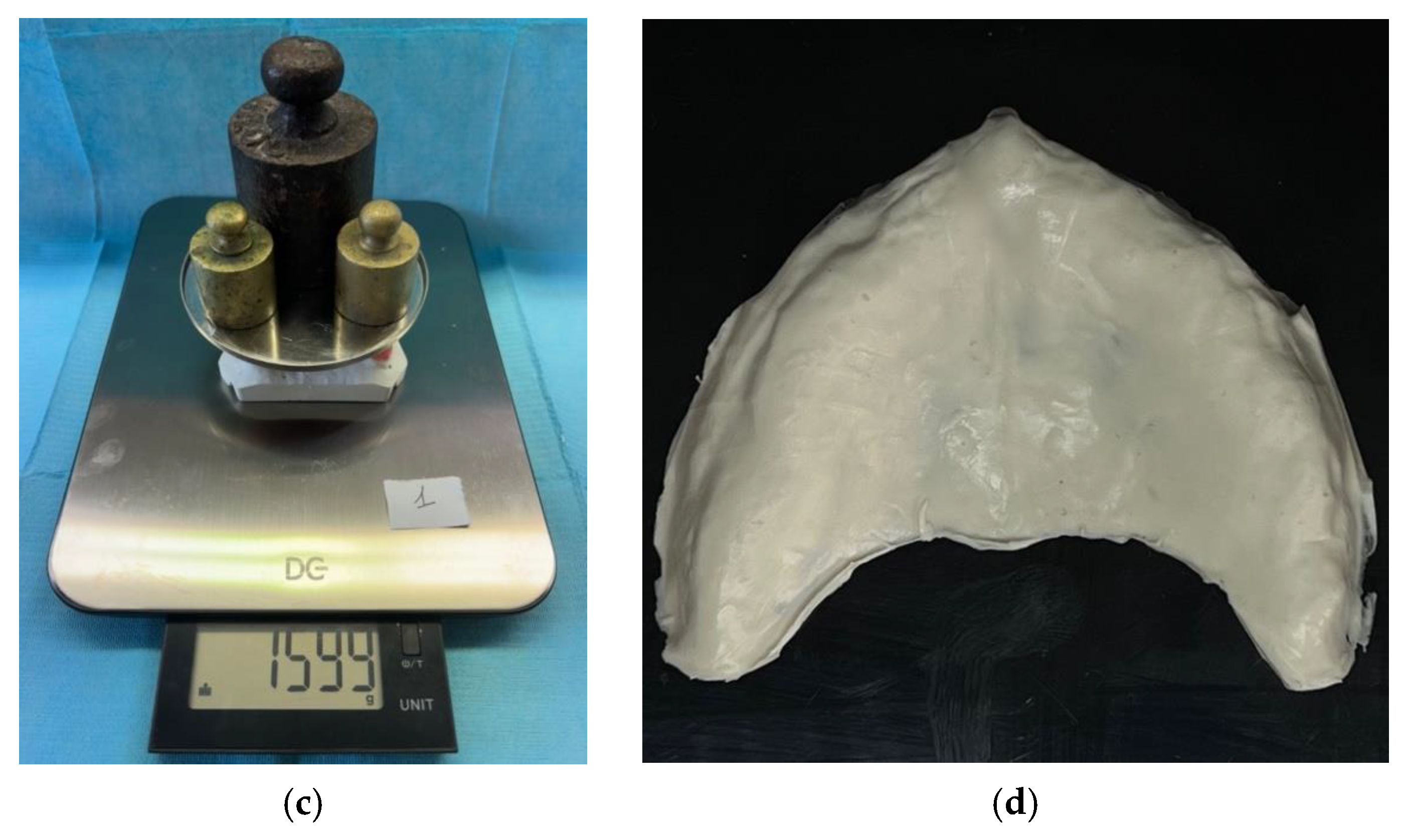
- c—Creation of the silicone with the prosthetic plate n° 3:Figure 8. (a) Base paste and catalyst paste; (b) mixture applied in the base obtained by milling; (c) load applied on the model; (d) silicone obtained from plate n° 3.Figure 8. (a) Base paste and catalyst paste; (b) mixture applied in the base obtained by milling; (c) load applied on the model; (d) silicone obtained from plate n° 3.
![Prosthesis 07 00042 g008]()



2.4. Statistics of the Data Collected
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davidowitz, G.; Kotick, P.G. The use of CAD/CAM in dentistry. Dent. Clin. N. Am. 2011, 55, 559–570, ix. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Maihemaiti, M.; Ren, L.; Maimaiti, M.; Yang, N.; Wang, Y.; Wang, M.; Wang, X.; Fu, Y.; Wang, Z. A comparative study of the use of digital technology in the anterior smile experience. BMC Oral Health 2024, 24, 492. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ceraulo, S. Aesthetics in Removable Partial Dentures: Modification of the Proximal Plate and Retentive Lamellae in Kennedy Class II Scenarios. Prosthesis 2024, 6, 107–118. [Google Scholar] [CrossRef]
- Alghazzawi, T.F. Advancements in CAD/CAM technology: Options for practical implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Arslan, M.; Murat, S.; Alp, G.; Zaimoglu, A. Evaluation of flexural strength and surface properties of prepolymerized CAD/CAM PMMA-based polymers used for digital 3D complete dentures. Int. J. Comput. Dent. 2018, 21, 31–40. [Google Scholar] [PubMed]
- Abualsaud, R.; Gad, M.M. Flexural Strength of CAD/CAM Denture Base Materials: Systematic Review and Meta-analysis of In-vitro Studies. J. Int. Soc. Prev. Community Dent. 2022, 12, 160–170. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prpić, V.; Schauperl, Z.; Ćatić, A.; Dulčić, N.; Čimić, S. Comparison of Mechanical Properties of 3D-Printed, CAD/CAM, and Conventional Denture Base Materials. J. Prosthodont. 2020, 29, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Mert, D.; Kamnoedboon, P.; Al-Haj Husain, N.; Özcan, M.; Srinivasan, M. CAD-CAM complete denture resins: Effect of relining on the shear bond strength. J. Dent. 2023, 131, 104438. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Jordan, D.; Methani, M.M.; Piedra-Cascón, W.; Özcan, M.; Zandinejad, A. Influence of printing angulation on the surface roughness of additive manufactured clear silicone indices: An in vitro study. J. Prosthet. Dent. 2021, 125, 462–468. [Google Scholar] [CrossRef] [PubMed]
- AlHelal, A.; AlRumaih, H.S.; Kattadiyil, M.T.; Baba, N.Z.; Goodacre, C.J. Comparison of retention between maxillary milled and conventional denture bases: A clinical study. J. Prosthet. Dent. 2017, 117, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Shi, Y.F.; Xie, P.J.; Wu, J.H. Accuracy of digital complete dentures: A systematic review of in vitro studies. J. Prosthet. Dent. 2021, 125, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Masri, G.; Mortada, R.; Ounsi, H.; Alharbi, N.; Boulos, P.; Salameh, Z. Adaptation of Complete Denture Base Fabricated by Conventional, Milling, and 3-D Printing Techniques: An In Vitro Study. J. Contemp. Dent. Pract. 2020, 21, 367–371. [Google Scholar] [PubMed]
- Fiorillo, L.; D’Amico, C.; Ronsivalle, V.; Cicciù, M.; Cervino, G. Restauro di un singolo impianto dentale: Cementato o avvitato? Una revisione sistematica di studi clinici randomizzati multifattoriali. Prosthesis 2024, 6, 871–886. [Google Scholar] [CrossRef]
- Gupta, R.; Brizuela, M. Dental Impression Materials. 2023 Mar 19. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Marino, G.; Canton, A.; Marino, A. Moderno Trattato di Protesi Mobile Completa; Edizioni Martina, s.r.l.: Bologna, Italy, 2014; ISBN 978-88-7572-118-3. [Google Scholar]
- Villias, A.; Karkazis, H.; Yannikakis, S.; Artopoulou, I.I.; Polyzois, G. Il numero di appuntamenti per la fabbricazione di protesi dentarie complete è ridotto con CAD-CAM? Una revisione della letteratura. Prosthesis 2022, 4, 91–101. [Google Scholar] [CrossRef]
- Alotaibi, H.N. Patient Satisfaction with CAD/CAM 3D-Printed Complete Dentures: A Systematic Analysis of the Clinical Studies. Healthcare 2025, 13, 388. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zadrożny, Ł.; Czajkowska, M.; Tallarico, M.; Wagner, L.; Markowski, J.; Mijiritsky, E.; Cicciù, M. Modelli chirurgici protesici e preparazione del sito dell’impianto dentale: Uno studio in vitro. Protesi 2022, 4, 25–37. [Google Scholar] [CrossRef]
- Jeong, M.; Radomski, K.; Lopez, D.; Liu, J.T.; Lee, J.D.; Lee, S.J. Materials and Applications of 3D Printing Technology in Dentistry: An Overview. Dent. J. 2023, 12, 1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zahel, A.; Roehler, A.; Kaucher-Fernandez, P.; Spintzyk, S.; Rupp, F.; Engel, E. Conventionally and digitally fabricated removable complete dentures: Manufacturing accuracy, fracture resistance and repairability. Dent. Mater. 2024, 40, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Kamal, M.N.M. Comparison between relining of ill-fitted maxillary complete denture versus CAD/CAM milling of new one regarding patient satisfaction, denture retention and adaptation. BMC Oral. Health 2025, 25, 18. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- García, E.; Jaramillo, S. Miglioramento della ritenzione delle protesi dentarie complete digitali mandibolari mediante scanner intraorale: Un caso clinico. Prosthesis 2025, 7, 29. [Google Scholar] [CrossRef]
- Souza Curinga, M.R.; Claudino Ribeiro, A.K.; de Moraes, S.L.D.; do Egito Vasconcelos, B.C.; da Fonte Porto Carreiro, A.; Pellizzer, E.P. Mechanical properties and accuracy of removable partial denture frameworks fabricated by digital and conventional techniques: A systematic review. J. Prosthet. Dent. 2025, 133, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z.; Kattadiyil, M.T. Comparison of denture base adaptation between CAD-CAM and conventional fabrication techniques. J. Prosthet. Dent. 2016, 116, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.N.; Oh, K.C.; Lee, S.J.; Han, J.S.; Yoon, H.I. Tissue surface adaptation of CAD-CAM maxillary and mandibular complete denture bases manufactured by digital light processing: A clinical study. J. Prosthet. Dent. 2020, 124, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, S.; Asper, L.; Long, J.; Lee, A.; Harrison, K.; Golebiowski, B. Ocular and visual discomfort associated with smartphones, tablets and computers: What we do and do not know. Clin. Exp. Optom. 2019, 102, 463–477. [Google Scholar] [CrossRef] [PubMed]
- Zandinejad, A.; Floriani, F.; Lin, W.S.; Naimi-Akbar, A. Clinical outcomes of milled, 3D-printed, and conventional complete dentures in edentulous patients: A systematic review and meta-analysis. J. Prosthodont. 2024, 33, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.; Zhou, M.L.; Min, M.; Zhang, X.F.; Qian, W.H. Evaluation of the trueness and tissue surface adaptation of digital and traditional complete denture bases. Shanghai Kou Qiang Yi Xue 2024, 33, 471–475. (In Chinese) [Google Scholar] [PubMed]
- Bessadet, M.; Drancourt, N.; El Osta, N. Time efficiency and cost analysis between digital and conventional workflows for the fabrication of fixed dental prostheses: A systematic review. J. Prosthet. Dent. 2025, 133, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Avelino, M.E.L.; Costa, R.T.F.; Vila-Nova, T.E.L.; Vasconcelos, B.C.D.E.; Pellizzer, E.P.; Moraes, S.L.D. Clinical performance and patient-related outcome measures of digitally fabricated complete dentures: A systematic review and meta-analysis. J. Prosthet. Dent. 2024, 132, e1–e748. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, B.J.; Goodacre, C.J. Additive Manufacturing for Complete Denture Fabrication: A Narrative Review. J. Prosthodont. 2022, 31, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Yin, Y.; Wu, J.; Wang, X.; Zhong, Z. Curvature-based interaction potential between a micro/nano curved surface body and a particle on the surface of the body. J. Biol. Phys. 2016, 42, 33–51. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Allegra, G.; Raos, G. Sliding friction between polymer surfaces: A molecular interpretation. J. Chem. Phys. 2006, 124, 144713. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters that can Influence the Construction Method |
| operator experience |
| alteration of polymerization times |
| type of resin used |
| Parameters that can influence the CAD design method |
| software used |
| operator experience for design |
| thickness and contour of the plaque |
| properties of the material used |
| accuracy of scanning and virtual model |
| resolution of the virtual model |
| Parameters that can influence CAM milling |
| feed rate and tool rotation speed |
| type of cutter or tip to determine accuracy and surface finish |
| milling machine parameters and machine accuracy |
| milling machine calibration and cooling system |
| type of material to be milled and shape and size of the plate |
| Parameters that can influence the CAD design method |
| software used |
| operator experience for design |
| thickness and contour of the plaque |
| properties of the material used |
| accuracy of scanning and virtual model |
| resolution of the virtual model |
| Parameters that can influence CAM by addition |
| type of printer |
| feed rate and set speed |
| Printer parameters |
| calibration and cooling system |
| type of material and shape and size of the plate |
| Silicone 1 | Silicone 2 | Silicone 3 | ||||||
|---|---|---|---|---|---|---|---|---|
| Sample | Sex | Age | Area A | Area B | Area A | Area B | Area A | Area B |
| Dentist 1 | M | 38 | 1 | 2 | 3 | 1 | 2 | 2 |
| Dentist 2 | M | 46 | 1 | 1 | 2 | 2 | 3 | 2 |
| Dentist 3 | M | 42 | 1 | 1 | 2 | 3 | 1 | 2 |
| Dentist 4 | M | 39 | 1 | 1 | 3 | 2 | 2 | 3 |
| Dentist 5 | F | 50 | 1 | 1 | 2 | 2 | 3 | 2 |
| Dentist 6 | F | 41 | 2 | 2 | 1 | 1 | 3 | 3 |
| Dentist 7 | M | 38 | 1 | 1 | 2 | 3 | 2 | 2 |
| Dentist 8 | F | 46 | 1 | 1 | 2 | 3 | 1 | 1 |
| Dentist 9 | M | 46 | 1 | 2 | 3 | 1 | 2 | 3 |
| Dentist 10 | M | 44 | 2 | 1 | 1 | 3 | 2 | 2 |
| Dentist 11 | M | 60 | 2 | 1 | 1 | 1 | 3 | 3 |
| Dentist 12 | F | 41 | 1 | 2 | 3 | 1 | 2 | 2 |
| Dentist 13 | M | 42 | 1 | 2 | 2 | 1 | 3 | 3 |
| Dentist 14 | M | 44 | 1 | 1 | 2 | 3 | 2 | 3 |
| Dentist 15 | M | 53 | 1 | 2 | 2 | 1 | 2 | 3 |
| Total | 18 | 21 | 31 | 28 | 33 | 36 | ||
| Silicone | Average Area A | Average Area B | Variance A | Variance B | Deviance A | Deviance B |
|---|---|---|---|---|---|---|
| Silicone 1 | 1.2 | 1.4 | 0.16 | 0.28 | 0.4 | 0.52 |
| Silicone 2 | 2.06 | 1.86 | 0.31 | 0.78 | 0.55 | 0.88 |
| Silicone 3 | 2.2 | 2.4 | 0.42 | 0.37 | 0.64 | 0.60 |
| µtotale | 1.8533 |
|---|---|
| SST | 1.095 |
| SSB | 1.095 |
| SSW | 32.48 |
| dfb | 5 |
| dfw | 84 |
| MSB | 0.219 |
| MSW | 0.386 |
| F-value | 0.568 |
| p-value | 0.735 |
| Campione/Area | 1 | 2 | 3 |
|---|---|---|---|
| SILICONE 1/Area A | 12 | 3 | 0 |
| SILICONE 1/Area B | 9 | 6 | 0 |
| SILICONE 2/Area A | 3 | 8 | 4 |
| SILICONE 2/Area B | 7 | 3 | 5 |
| SILICONE 3/Area A | 2 | 8 | 5 |
| SILICONE 3/Area B | 1 | 7 | 7 |
| Research Gap |
|---|
| Reduced number of prosthetic plates |
| Small sample of dentists involved in the evaluation |
| The adaptability assessment was carried out by visual examination which is a subjective examination |
| Future Research Ideas |
| Experimental studies with the aim of establishing objective parameters with larger samples of plates and observers to allow for the identification of the most subtle differences between the different construction methods with precise and comparable data |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceraulo, S.; Barbarisi, A.; Selvaggio, L.; Caccianiga, G.; Lauritano, D. Accuracy in the Plaster Model of Total Prosthetic Plates in Three Different Manufacturing Methods: In Vitro Study. Prosthesis 2025, 7, 42. https://doi.org/10.3390/prosthesis7020042
Ceraulo S, Barbarisi A, Selvaggio L, Caccianiga G, Lauritano D. Accuracy in the Plaster Model of Total Prosthetic Plates in Three Different Manufacturing Methods: In Vitro Study. Prosthesis. 2025; 7(2):42. https://doi.org/10.3390/prosthesis7020042
Chicago/Turabian StyleCeraulo, Saverio, Antonio Barbarisi, Leonardo Selvaggio, Gianluigi Caccianiga, and Dorina Lauritano. 2025. "Accuracy in the Plaster Model of Total Prosthetic Plates in Three Different Manufacturing Methods: In Vitro Study" Prosthesis 7, no. 2: 42. https://doi.org/10.3390/prosthesis7020042
APA StyleCeraulo, S., Barbarisi, A., Selvaggio, L., Caccianiga, G., & Lauritano, D. (2025). Accuracy in the Plaster Model of Total Prosthetic Plates in Three Different Manufacturing Methods: In Vitro Study. Prosthesis, 7(2), 42. https://doi.org/10.3390/prosthesis7020042