End-of-Life Care Preferences of Patients with Advanced Urological Malignancies: An Explorative Survey Study at a Tertiary Referral Center

 , , , and
, , , and 
Abstract
1. Introduction
2. Methods
- -
- Demographic data;
- -
- Preferences regarding the preferred place of death;
- -
- Existence of a living will and/or health care proxy;
- -
- Level of knowledge about their disease;
- -
- Communication about wishes for the last stage of life.
3. Results
3.1. Demographics and Symptoms
3.2. Preferred Place of Death
3.3. Communication about Place of Death
3.4. Living Will/Health Care Proxy
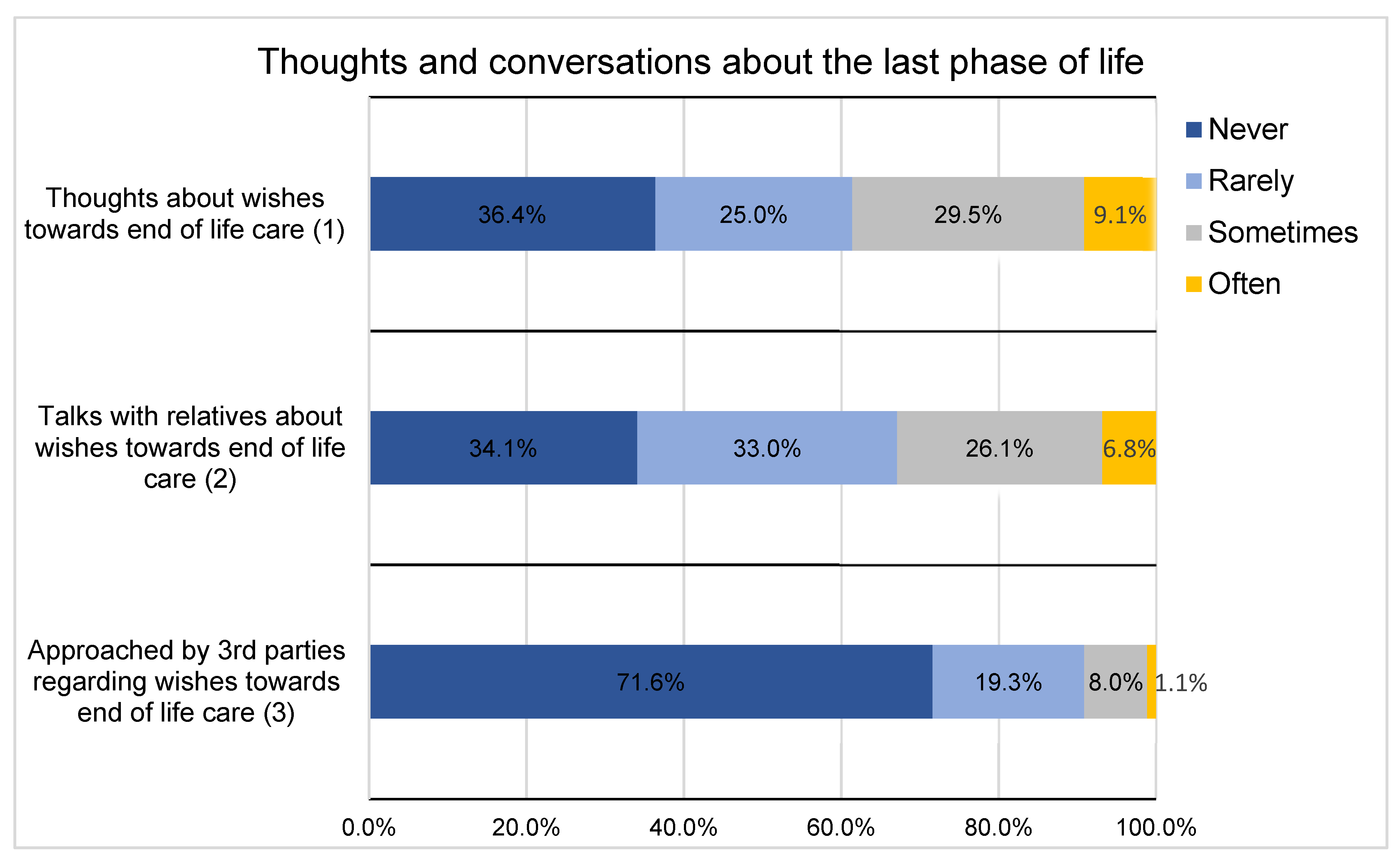
3.5. Discussions about Care Options
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robert-Koch-Institut. Krebs in Deutschland für 2017/2018; Robert-Koch-Institut: Berlin, Germany, 2021; p. 172.
- Dasch, B.; Blum, K.; Gude, P.; Bausewein, C. Place of death: Trends over the course of a decade—A population based study of death certificates from the years 2001 and 2011. Dtsch. Aerzteblatt Online 2015, 112, 496. [Google Scholar] [CrossRef]
- Sauer, S.; Müller, R.; Rothgang, H. Institutionalisiertes Sterben in Deutschland: Trends in der Sterbeortverteilung: Zu Hause, Krankenhaus und Pflegeheim. Z. Gerontol. Geriatr. 2015, 48, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Escobar Pinzón, L.C.; Weber, M.; Claus, M.; Fischbeck, S.; Unrath, M.; Martini, T.; Münster, E. Factors Influencing Place of Death in Germany. J. Pain Symptom Manag. 2011, 41, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Papke, J.; Koch, R. Places of Death from Cancer in a Rural Location. Oncol. Res. Treat. 2007, 30, 105–108. [Google Scholar] [CrossRef]
- Dasch, B.; Zahn, P.K. Place of death trends and utilization of outpatient palliative care at the end of life—Analysis of death certificates (2001, 2011, 2017) and pseudonymized data from selected palliative medicine consultation services (2017) in Westphalia, Germany. Dtsch. Aerzteblatt Online 2021, 118, 331. [Google Scholar] [CrossRef]
- Haun, M.W.; Estel, S.; Rücker, G.; Friederich, H.-C.; Villalobos, M.; Thomas, M.; Hartmann, M. Early palliative care for adults with advanced cancer. Cochrane Database Syst. Rev. 2017, 6, CD011129. [Google Scholar] [CrossRef]
- Bausewein, C.; Fegg, M.; Roller, S.; Voltz, R. Patientenbedürfnisse. In Leitfaden Palliative Care; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1–16. ISBN 978-3-437-23315-9. [Google Scholar]
- Seifart, C.; Nagelschmidt, K.; von Blanckenburg, P. Barrieren für Gespräche über Tod und Sterben in der Medizin. AINS Anästhesiol. Intensivmed. Notfallmedizin Schmerzther. 2020, 55, 334–339. [Google Scholar] [CrossRef]
- Ellershaw, J.; Dewar, S.; Murphy, D. Achieving a good death for all. BMJ 2010, 341, c4861. [Google Scholar] [CrossRef]
- Deutscher Hospiz- und Palliativverband. Wissen und Einstellungen der Menschen in Deutschland zum Sterben—Ergebnisse einer Repräsentativen Bevölkerungsbefragung im Auftrag des DHPV. 2017. Available online: https://www.dhpv.de/files/public/aktuelles/Forschung/Forschung_2017_Ergebnisse_DHPVBevoelkerungsbefragung.pdf (accessed on 11 November 2021).
- Gomes, B.; Higginson, I.J.; Calanzani, N.; Cohen, J.; Deliens, L.; Daveson, B.A.; Bechinger-English, D.; Bausewein, C.; Ferreira, P.L.; Toscani, F.; et al. Preferences for place of death if faced with advanced cancer: A population survey in England, Flanders, Germany, Italy, the Netherlands, Portugal and Spain. Ann. Oncol. 2012, 23, 2006–2015. [Google Scholar] [CrossRef]
- Escobar Pinzon, L.C.; Claus, M.; Zepf, K.I.; Letzel, S.; Fischbeck, S.; Weber, M. Preference for Place of Death in Germany. J. Palliat. Med. 2011, 14, 1097–1103. [Google Scholar] [CrossRef]
- Fereidouni, A.; Rassouli, M.; Salesi, M.; Ashrafizadeh, H.; Vahedian-Azimi, A.; Barasteh, S. Preferred Place of Death in Adult Cancer Patients: A Systematic Review and Meta-Analysis. Front. Psychol. 2021, 12, 704590. [Google Scholar] [CrossRef]
- Statistisches Bundesamt (Destatis). Krankenhausstatistik: Eckdaten der Krankenhauspatientinnen und -Patienten. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Krankenhaeuser/Tabellen/entlassene-patienten-eckdaten.html (accessed on 12 November 2021).
- Statistisches Bundesamt (Destatis). Todesursachenstatistik 2016 bis 2020: Deutschland, Jahre, Todesursachen. Available online: https://www-genesis.destatis.de/genesis/online?operation=ergebnistabelleQualitaetSeparatAUS&levelindex=3&levelid=1636627342709&downloadname=23211-0001#abreadcrumb (accessed on 11 November 2021).
- Dasch, B.; Blum, K.; Vogelsang, H.; Bausewein, C. Epidemiologische Untersuchung zum Sterbeort von Tumorpatienten. DMW Dtsch. Med. Wochenschr. 2016, 141, e158–e165. [Google Scholar] [CrossRef]
- Volberg, C.; Schrade, S.; Heers, H.; Carrasco, A.J.P.; Morin, A.; Gschnell, M. End-of-life wishes and care planning for patients with advanced skin cancer. J. Dtsch. Dermatol. Ges. 2023, 21, 1148–1155. [Google Scholar] [CrossRef]
- Gomes, B.; Calanzani, N.; Gysels, M.; Hall, S.; Higginson, I.J. Heterogeneity and changes in preferences for dying at home: A systematic review. BMC Palliat. Care 2013, 12, 7. [Google Scholar] [CrossRef]
- Wilson, D.M.; Cohen, J.; Deliens, L.; Hewitt, J.A.; Houttekier, D. The Preferred Place of Last Days: Results of a Representative Population-Based Public Survey. J. Palliat. Med. 2013, 16, 502–508. [Google Scholar] [CrossRef]
- Hunt, K.J.; Shlomo, N.; Addington-Hall, J. End-of-life care and achieving preferences for place of death in England: Results of a population-based survey using the VOICES-SF questionnaire. Palliat. Med. 2014, 28, 412–421. [Google Scholar] [CrossRef]
- Austad, S.N. Why women live longer than men: Sex differences in longevity. Gend. Med. 2006, 3, 79–92. [Google Scholar] [CrossRef]
- Crimmins, E.M.; Shim, H.; Zhang, Y.S.; Kim, J.K. Differences between Men and Women in Mortality and the Health Dimensions of the Morbidity Process. Clin. Chem. 2019, 65, 135–145. [Google Scholar] [CrossRef]
- Volberg, C.; Corzilius, J.; Maul, J.; Morin, A.; Gschnell, M. Schmerztherapie in der deutschen spezialisierten ambulanten Palliativversorgung: Eine Querschnittsstudie zur Darstellung der aktuellen schmerzmedizinischen Versorgung von palliativen Patienten im häuslichen Umfeld. Schmerz 2023, 23, e30. [Google Scholar] [CrossRef] [PubMed]
- van Doorne, I.; van Rijn, M.; Dofferhoff, S.M.; Willems, D.L.; Buurman, B.M. Patients’ preferred place of death: Patients are willing to consider their preferences, but someone has to ask them. Age Ageing 2021, 50, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, W.C. Wirkungen einer Patientenverfügung. In Zimmermann Vorsorgevollmacht-Betreuungsverfügung-Patientenverfügung; Erich Schmidt Verlag GmbH & Co: Berlin, Germany, 2017. [Google Scholar]
- Wright, A.A.; Zhang, B.; Ray, A.; Mack, J.W.; Trice, E.; Balboni, T.; Mitchell, S.L.; Jackson, V.A.; Block, S.D.; Maciejewski, P.K.; et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008, 300, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Ilan, R.; Jiang, X.; You, J.J.; Dodek, P. The prevalence of medical error related to end-of-life communication in Canadian hospitals: Results of a multicentre observational study. BMJ Qual. Saf. 2016, 25, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Nagelschmidt, K.; Leppin, N.; Seifart, C.; Rief, W.; von Blanckenburg, P. Systematic mixed-method review of barriers to end-of-life communication in the family context. BMJ Support. Palliat. Care 2021, 11, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Brighton, L.J.; Bristowe, K. Communication in palliative care: Talking about the end of life, before the end of life. Postgrad. Med. J. 2016, 92, 466–470. [Google Scholar] [CrossRef]
- Betker, L.; Nagelschmidt, K.; Leppin, N.; Knorrenschild, J.R.; Volberg, C.; Berthold, D.; Sibelius, U.; Rief, W.; Barke, A.; Von Blanckenburg, P.; et al. The Difficulties in End-of-Life Discussions—Family Inventory (DEOLD-FI): Development and Initial Validation of a Self-Report Questionnaire in a Sample of Terminal Cancer Patients. J. Pain Symptom Manag. 2021, 62, e130–e138. [Google Scholar] [CrossRef]
- Sullivan, D.R.; Chan, B.; Lapidus, J.A.; Ganzini, L.; Hansen, L.; Carney, P.A.; Fromme, E.K.; Marino, M.; Golden, S.E.; Vranas, K.C.; et al. Association of Early Palliative Care Use With Survival and Place of Death Among Patients With Advanced Lung Cancer Receiving Care in the Veterans Health Administration. JAMA Oncol. 2019, 5, 1702. [Google Scholar] [CrossRef]
- van Lummel, E.V.; Ietswaard, L.; Zuithoff, N.P.; Tjan, D.H.; van Delden, J.J. The utility of the surprise question: A useful tool for identifying patients nearing the last phase of life? A systematic review and meta-analysis. Palliat. Med. 2022, 36, 1023–1046. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, J.; Bernacki, R.; Paladino, J. Shifting to Serious Illness Communication. JAMA 2022, 327, 321. [Google Scholar] [CrossRef]
- Bernacki, R.; Paladino, J.; Neville, B.A.; Hutchings, M.; Kavanagh, J.; Geerse, O.P.; Lakin, J.; Sanders, J.J.; Miller, K.; Lipsitz, S.; et al. Effect of the Serious Illness Care Program in Outpatient Oncology: A Cluster Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 751. [Google Scholar] [CrossRef]


{kind=link}
| n | % | ||
|---|---|---|---|
| Gender | Male | 76 | |
| Prostate cancer | 41 | 54 | |
| Renal cell carcinoma | 26 | 34 | |
| Urothelial carcinoma | 9 | 12 | |
| Female | 12 | ||
| Renal cell carcinoma | 9 | 75 | |
| Urothelial carcinoma | 3 | 25 | |
| Age | <70 | 42 | 48 |
| ≥70 | 46 | 52 | |
| Time since tumor diagnosis | <5 years | 62 | 70 |
| Prostate cancer | 29 | 33 | |
| Renal cell carcinoma | 21 | 24 | |
| Urothelial carcinoma | 12 | 14 | |
| ≥5 years | 26 | 30 | |
| Prostate cancer | 12 | 14 | |
| Renal cell carcinoma | 14 | 16 | |
| Urothelial carcinoma | 0 | 0 | |
| Tumor entity | Prostate cancer | 41 | 47 |
| Renal cell carcinoma | 35 | 40 | |
| Urothelial carcinoma | 12 | 14 | |
| Symptoms | Symptoms | 70 | 80 |
| No symptoms | 18 | 20 | |
| Number of symptoms | <5 | 72 | 82 |
| ≥5 | 16 | 18 | |
| Symptom burden | Affected | 51 | 58 |
| Not affected | 37 | 42 | |
| Marital status | In a stable relationship or married/registered partnership | 66 | 75 |
| Single/widowed | 22 | 25 | |
| Need for care | Care requirements | 33 | 38 |
| No need for care | 55 | 63 | |
| Education | (Technical) university degree | 12 | 14 |
| Vocational training | 69 | 78 | |
| No professional training | 7 | 8 |
| Tumor Entity | |||||
|---|---|---|---|---|---|
| Symptoms | Prostate Cancer | Renal Cell Carcinoma | Urothelial Carcinoma | Total | % of Cases |
| Pain | 21 | 17 | 5 | 43 | 61.4 |
| Shortness of breath | 2 | 10 | 3 | 15 | 21.4 |
| Urinary tract infection | 2 | 1 | 2 | 5 | 7.1 |
| Visible hematuria | 1 | 0 | 2 | 3 | 4.3 |
| Sexual problems/ reduced libido | 15 | 5 | 2 | 22 | 31.4 |
| Nausea | 4 | 11 | 2 | 17 | 24.3 |
| Diarrhea/constipation | 10 | 14 | 6 | 30 | 42.9 |
| Sleep disorders | 15 | 13 | 7 | 35 | 50.0 |
| Pronounced daytime tiredness (fatigue) | 4 | 8 | 2 | 14 | 20.0 |
| Open wounds | 1 | 5 | 0 | 6 | 8.6 |
| Fear | 6 | 4 | 4 | 14 | 20.0 |
| Other symptoms | 8 | 12 | 2 | 22 | 31.4 |
| Civil Partnership | Number of Symptoms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Single, Widowed | % of Life Partnership | % of Death Place Request | Stable Relationship, Married/Registered Civil Partnership | % of Life Partnership | % of Death Place Request | <5 Symptoms | % from < 5 Symptoms | ≥5 Symptoms | % from ≥ 5 Symptoms | ||
| Preferred place of death | At home | 11 | 50.0 | 17.2 | 53 | 80.3 | 82.8 | 56 | 77.8 | 8 | 50.0 |
| Nursing home | 1 | 4.5 | 100.0 | 0 | 0.0 | 9.1 | 1 | 1.4 | 0 | 0.0 | |
| Hospital | 0 | 0.0 | 0.0 | 2 | 3.0 | 100.0 | 1 | 1.4 | 1 | 6.3 | |
| Hospice | 7 | 31.8 | 77.8 | 2 | 3.0 | 22.2 | 4 | 5.6 | 5 | 31.3 | |
| Other place | 1 | 4.5 | 100.0 | 0 | 0.0 | 0.0 | 1 | 1.4 | 0 | 0.0 | |
| Not important | 2 | 9.1 | 18.2 | 9 | 13.6 | 81.8 | 9 | 12.5 | 2 | 12.5 | |
| Total | 22 | 100 | 25 | 66 | 100 | 75 | 72 | 100 | 16 | 100 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volberg, C.; Urhahn, F.; Pedrosa Carrasco, A.J.; Morin, A.; Gschnell, M.; Huber, J.; Flegar, L.; Heers, H. End-of-Life Care Preferences of Patients with Advanced Urological Malignancies: An Explorative Survey Study at a Tertiary Referral Center. Curr. Oncol. 2024, 31, 462-471. https://doi.org/10.3390/curroncol31010031
Volberg C, Urhahn F, Pedrosa Carrasco AJ, Morin A, Gschnell M, Huber J, Flegar L, Heers H. End-of-Life Care Preferences of Patients with Advanced Urological Malignancies: An Explorative Survey Study at a Tertiary Referral Center. Current Oncology. 2024; 31(1):462-471. https://doi.org/10.3390/curroncol31010031
Chicago/Turabian StyleVolberg, Christian, Fabian Urhahn, Anna J. Pedrosa Carrasco, Astrid Morin, Martin Gschnell, Johannes Huber, Luka Flegar, and Hendrik Heers. 2024. "End-of-Life Care Preferences of Patients with Advanced Urological Malignancies: An Explorative Survey Study at a Tertiary Referral Center" Current Oncology 31, no. 1: 462-471. https://doi.org/10.3390/curroncol31010031
APA StyleVolberg, C., Urhahn, F., Pedrosa Carrasco, A. J., Morin, A., Gschnell, M., Huber, J., Flegar, L., & Heers, H. (2024). End-of-Life Care Preferences of Patients with Advanced Urological Malignancies: An Explorative Survey Study at a Tertiary Referral Center. Current Oncology, 31(1), 462-471. https://doi.org/10.3390/curroncol31010031