Real-World Treatment Patterns, Clinical Outcomes, and Healthcare Resource Utilization in Early-Stage Non-Small-Cell Lung Cancer

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Baseline Patient and Disease Characteristics
2.3. Treatment Patterns
2.4. Survival Outcomes
2.5. Healthcare Resource Utilization
3. Results
3.1. Baseline Patient and Disease Characteristics
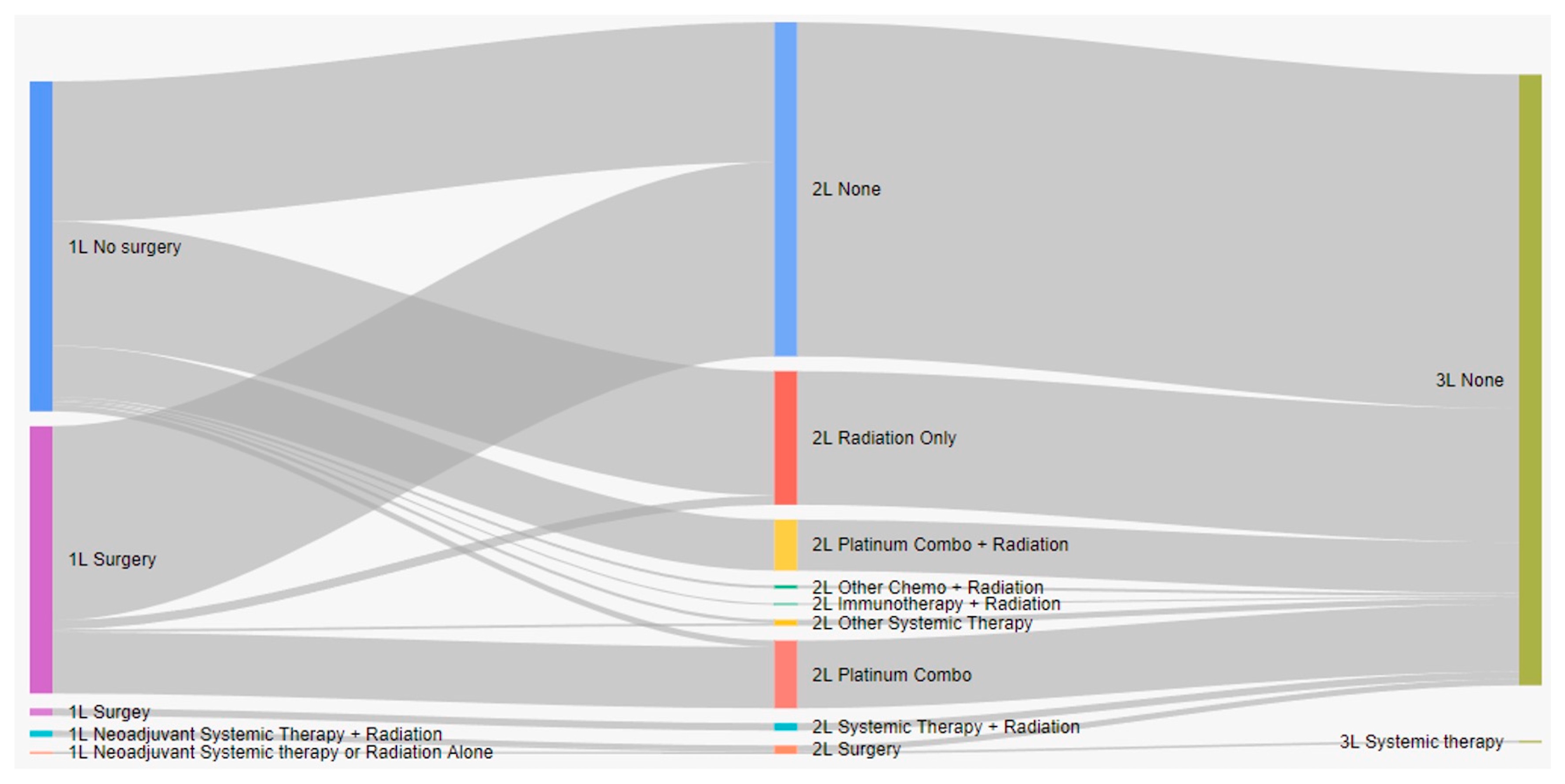
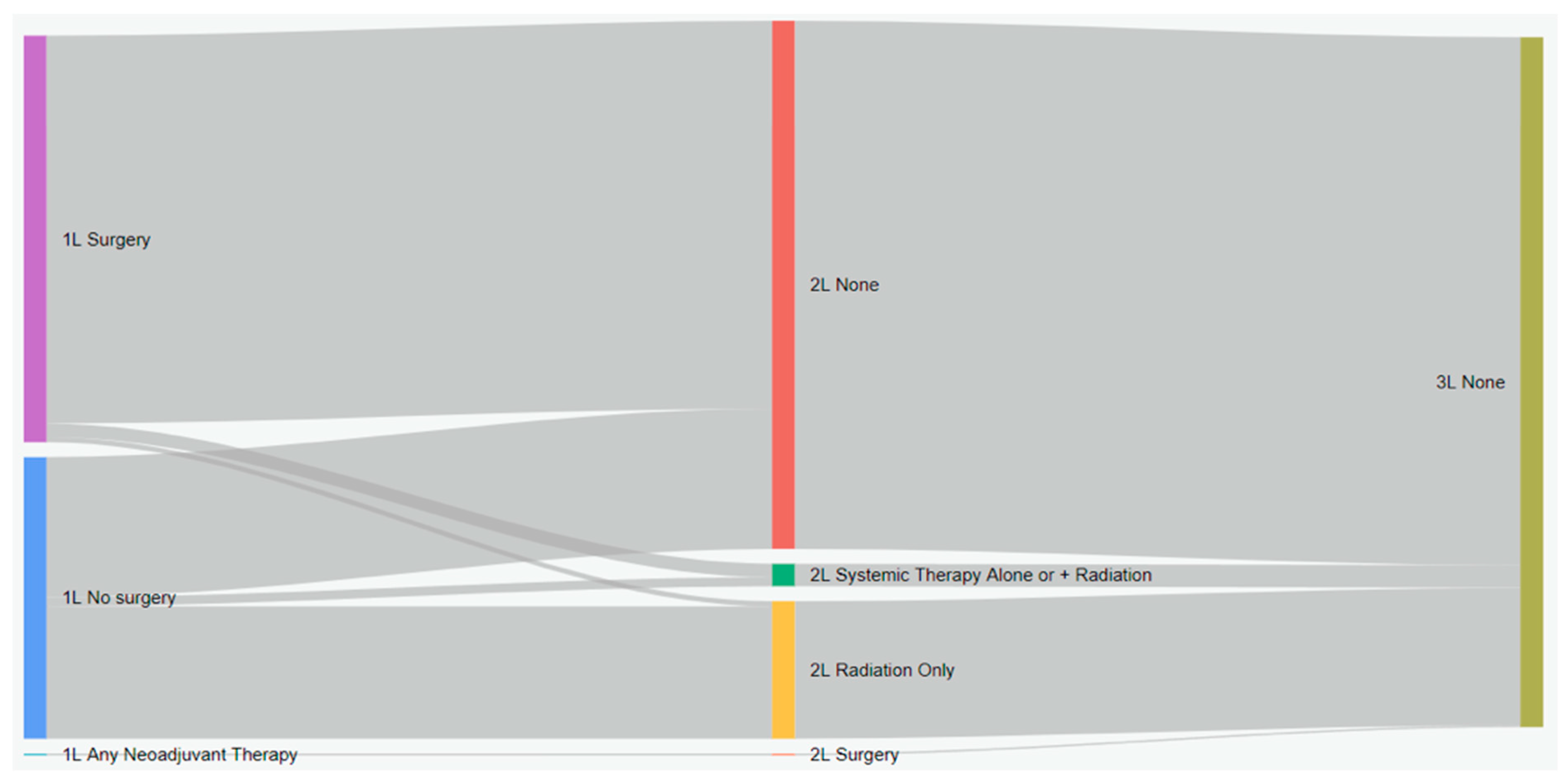
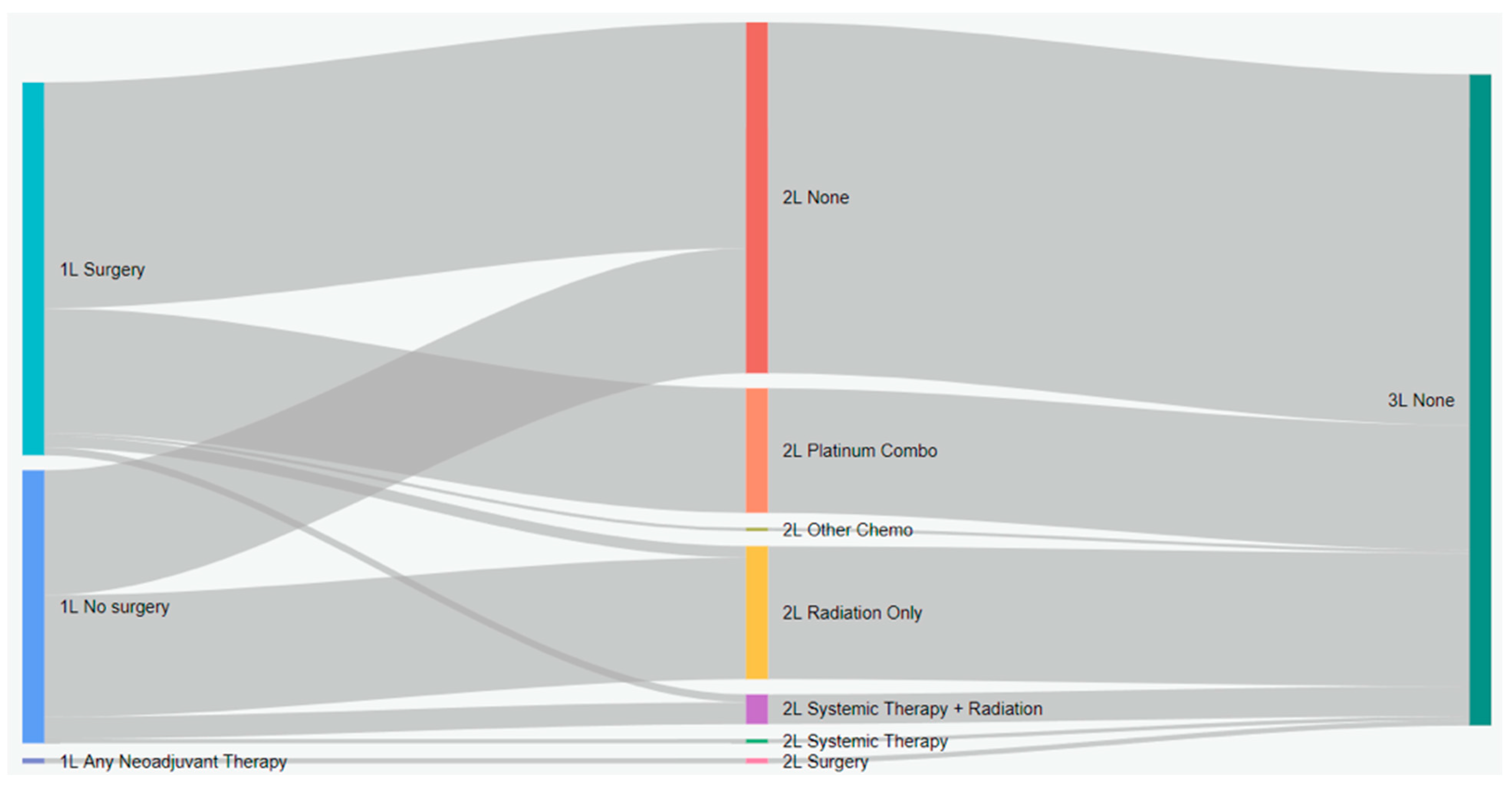
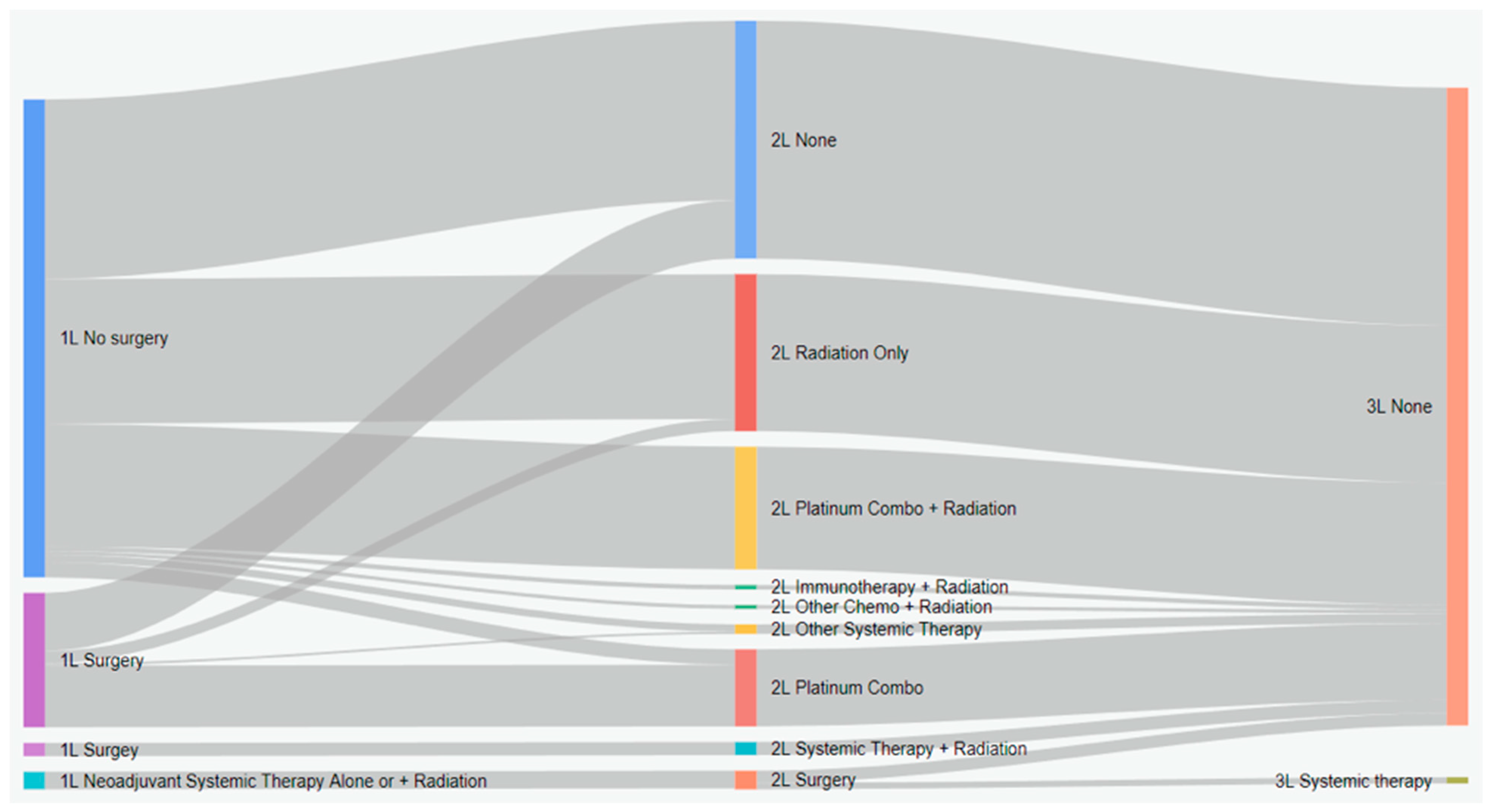
3.2. Treatment Patterns
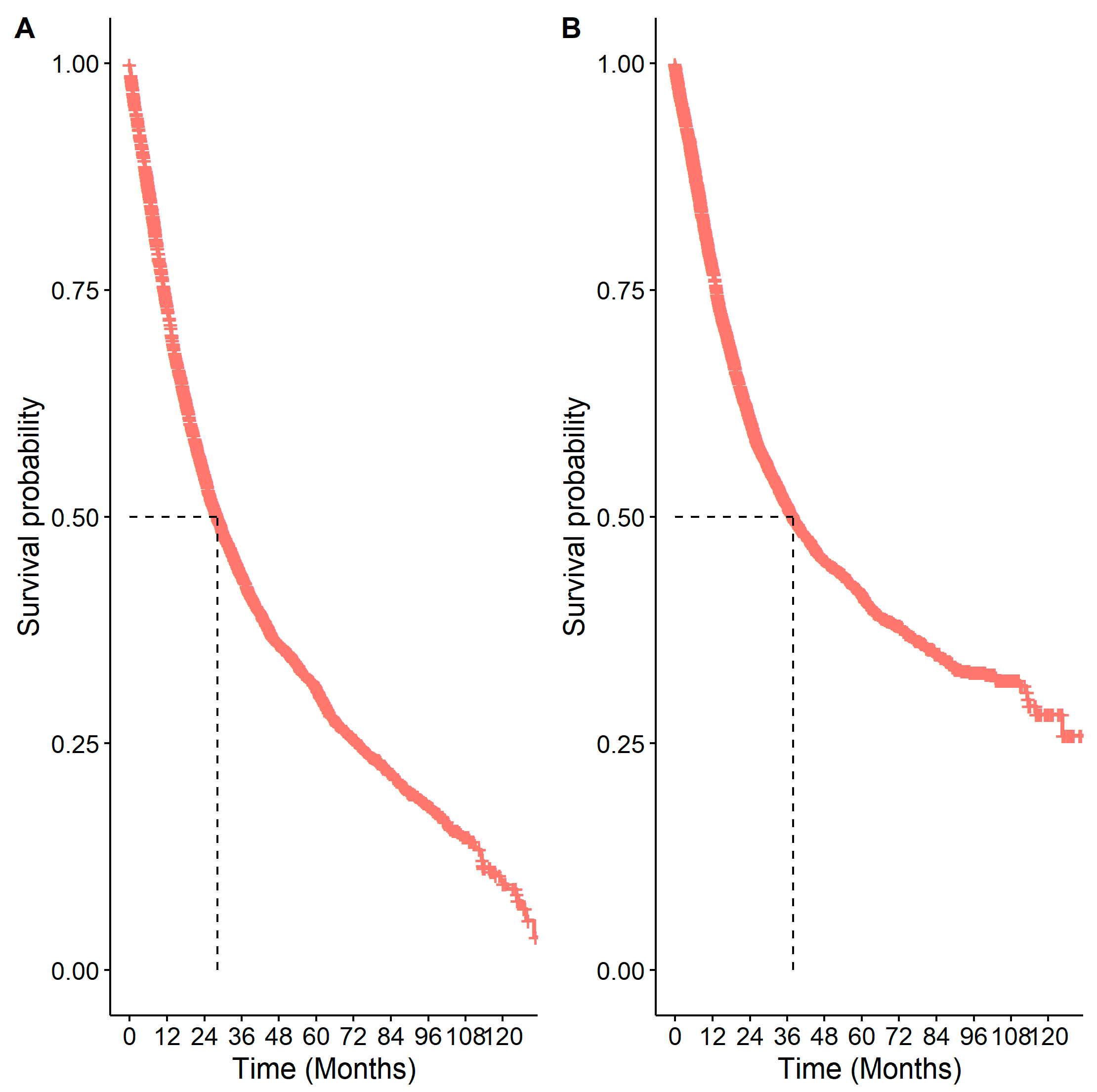
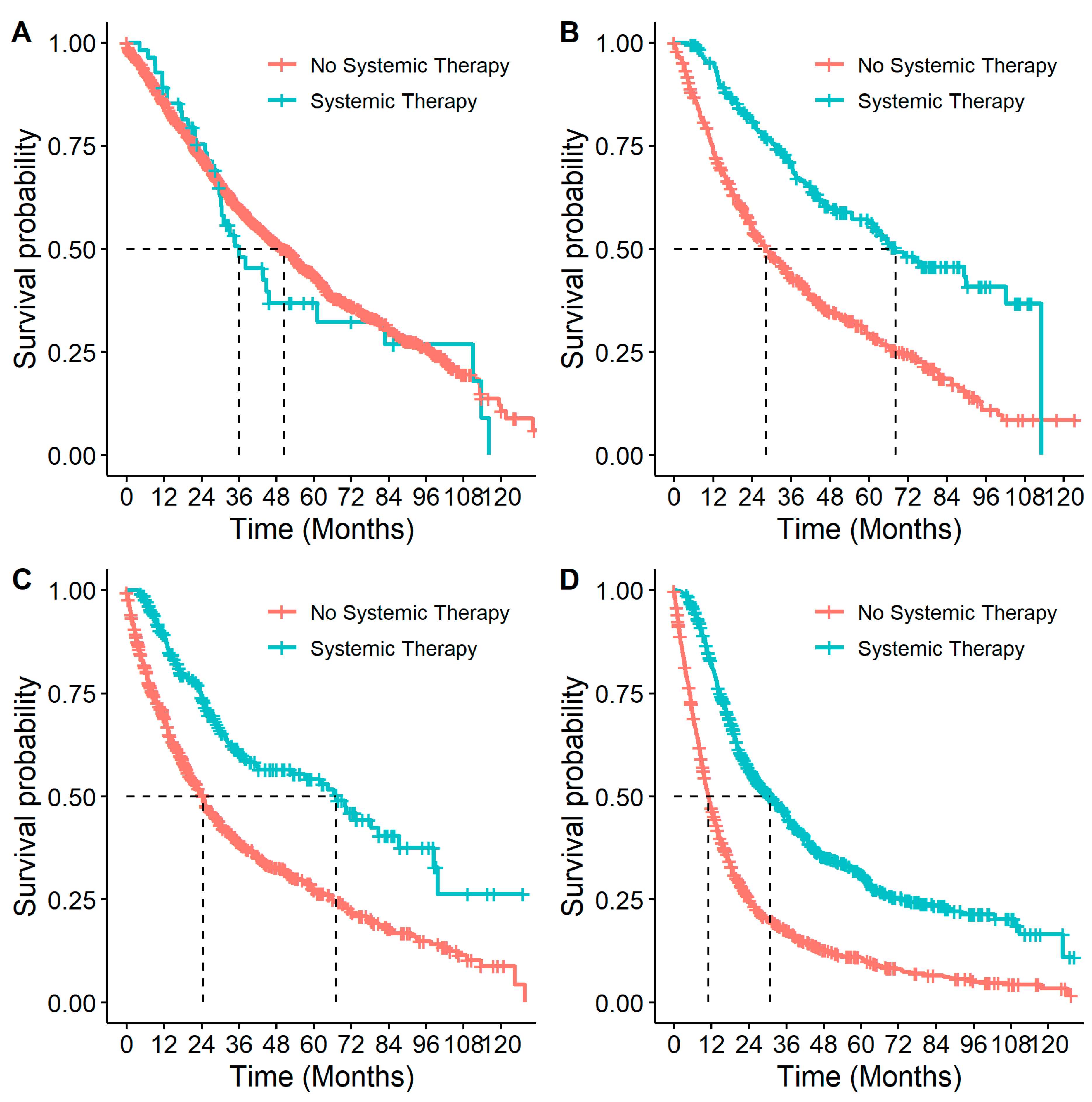
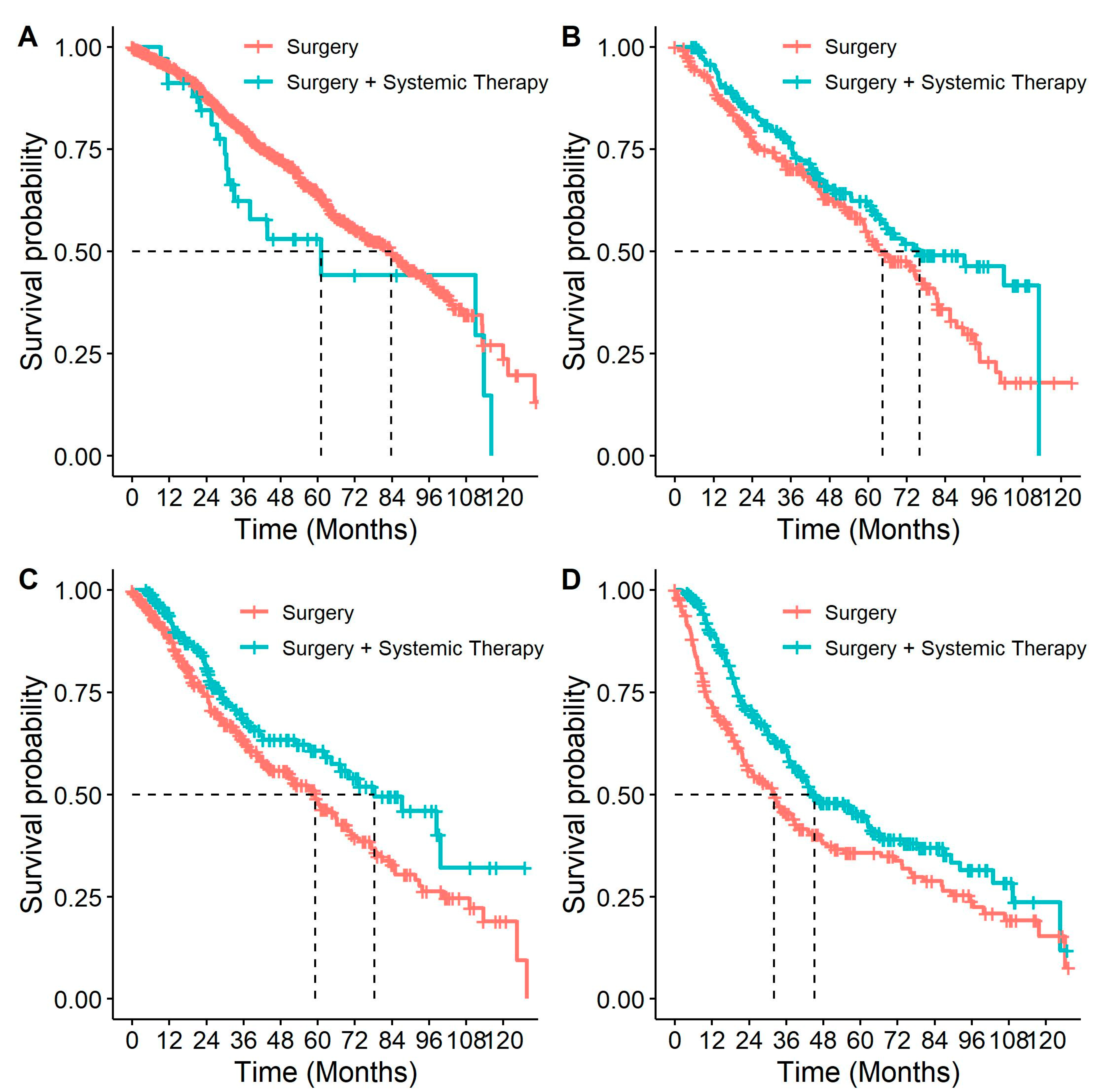
3.3. Survival Outcomes
3.4. Healthcare Resource Utilization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brenner, D.R.; Poirier, A.; Woods, R.R.; Ellison, L.F.; Billette, J.M.; Demers, A.A.; Zhang, S.X.; Yao, C.; Finley, C.; Fitzgerald, N.; et al. Canadian Cancer Statistics Advisory Committee. Projected estimates of cancer in Canada in 2022. Can. Med. Assoc. J. 2022, 194, E601–E607. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Knight, S.B.; Phil, A.; Crosbie, P.A.; Balata, H.; Chudziak, J.; Hussell, T.; Dive, C. Progress and prospects of early detection in lung cancer. Open Biol. 2017, 7, 170070. [Google Scholar] [CrossRef]
- Balata, H.; Fong, K.M.; Hendriks, L.E.; Lam, S.; Ostroff, J.S.; Peled, N.; Wu, N.; Aggarwal, C. Prevention and early detection for NSCLC: Advances in thoracic oncology 2018. J. Thorac. Oncol. 2019, 14, 1513–1527. [Google Scholar] [CrossRef] [PubMed]
- Seung, S.; Hurry, M.; Walton; Evans, W. Real-world treatment patterns and survival in stage IV non-small-cell lung cancer in Canada. Curr. Oncol. 2020, 27, 361–367. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Research Team; Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef]
- De Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- Durm, G.A.; Jabbour, S.K.; Althouse, S.K.; Liu, Z.; Sadiq, A.A.; Zon, R.T.; Jalal, S.I.; Kloecker, G.H.; Williamson, M.J.; Reckamp, K.L.; et al. A phase 2 trial of consolidation pembrolizumab following concurrent chemoradiation for patients with unresectable stage III non–small cell lung cancer: Hoosier Cancer Research Network LUN 14-179. Cancer 2020, 126, 4353–4361. [Google Scholar] [CrossRef]
- Cheema, P.K.; Rothenstein, J.; Melosky, B.; Brade, A.; Hirsh, V. Perspectives on treatment advances for stage III locally advanced unresectable non-dmall-cell lung cancer. Curr. Oncol. 2019, 26, 37–42. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Csőszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. IMpower010 Investigators. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): A randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.H.; Shalata, W.; Yakobson, A.; Agbarya, A. Neoadjuvant and adjuvant immunotherapy in early-stage non-small-cell lung cancer, past, present, and future. J. Clin. Med. 2021, 10, 5614. [Google Scholar] [CrossRef]
- Pennell, N.A.; Neal, J.W.; Chaft, J.E.; Azzoli, C.G.; Jänne, P.A.; Govindan, R.; Evans, T.L.; Costa, D.B.; Wakelee, H.A.; Heist, R.S.; et al. SELECT: A phase II trial of adjuvant erlotinib in patients with resected epidermal growth factor receptor–mutant non–small-cell lung cancer. J. Clin. Oncol. 2019, 37, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Yue, D.; Xu, S.; Wang, Q.; Li, X.; Shen, Y.; Zhao, H.; Chen, C.; Mao, W.; Liu, W.; Liu, J.; et al. Erlotinib versus vinorelbine plus cisplatin as adjuvant therapy in Chinese patients with stage IIIA EGFR mutation-positive non-small-cell lung cancer (EVAN): A randomised, open-label, phase 2 trial. Lancet Respir. Med. 2018, 6, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Chaft, J.E.; Rimner, A.; Weder, W.; Azzoli, C.G.; Kris, M.G.; Cascone, T. Evolution of systemic therapy for stages I–III non-metastatic non-small-cell lung cancer. Nat. Rev. Clin. Oncol. 2021, 18, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Notice of Compliance Information for TAGRISSO. Available online: https://health-products.canada.ca/noc-ac/nocInfo?no=25023"https://health-products.canada.ca/noc-ac/nocInfo?no=25023 (accessed on 28 November 2023).
- Health Canada. Notice of Compliance Information for TECENTRIQ. Available online: https://health-products.canada.ca/noc-ac/nocInfo?no=27396 (accessed on 28 November 2023).
- Health Canada. Notice of Compliance Information for OPDIVO. Available online: https://health-products.canada.ca/noc-ac/nocInfo?no=28801 (accessed on 28 November 2023).
- Health Canada. Notice of Compliance Information for KEYTRUDA. Available online: https://health-products.canada.ca/noc-ac/nocInfo?no=30562 (accessed on 28 November 2023).
- Waser, N.; Vo, L.; McKenna, M.; Penrod, J.; Goring, S. Real-world treatment patterns in resectable (stages I–III) non-small-cell lung cancer: A systematic literature review. Futur. Oncol. 2022, 18, 1519–1530. [Google Scholar] [CrossRef]
- Arnold, B.N.; Thomas, D.C.; Rosen, J.E.; Salazar, M.C.; Blasberg, J.D.; Boffa, D.J.; Detterbeck, F.C.; Kim, A.W. Lung cancer in the very young: Treatment and survival in the national cancer data base. J. Thorac. Oncol. 2016, 11, 1121–1131. [Google Scholar] [CrossRef]
- Pinquié, F.; Goupil, F.; Oster, J.P.; Dixmier, A.; Renault, P.A.; Lévy, A.; Mathieu, J.P.; Paillot, N.; Goutorbe, F.C.; Masson, P.; et al. Therapeutic strategies in patients undergoing surgery for non-small cell lung cancer. Results of the ESCAP-2011-CPHG study, promoted by the French College of General Hospital Respiratory Physicians (CPHG). Rev. Mal. Respir. 2017, 34, 976–990. [Google Scholar] [CrossRef]
- Gould, M.K.; Munoz-Plaza, C.E.; Hahn, E.E.; Lee, J.S.; Parry, C.; Shen, E. Comorbidity profiles and their effect on treatment selection and survival among patients with lung cancer. Ann. Am. Thorac. Soc. 2017, 14, 1571–1580. [Google Scholar] [CrossRef]
- Vinod, S.K.; Wai, E.; Alexander, C.; Tyldesley, S.; Murray, N. Stage III non–small-cell lung cancer: Population-based patterns of treatment in British Columbia, Canada. J. Thorac. Oncol. 2012, 7, 1155–1163. [Google Scholar] [CrossRef]
- Chi, A.; Fang, W.; Sun, Y.; Wen, S. Comparison of long-term survival of patients with early-stage non–small cell lung cancer after surgery vs stereotactic body radiotherapy. JAMA Netw. Open 2019, 2, e1915724. [Google Scholar] [CrossRef] [PubMed]
- Van Schil, P.E. Surgery for non-small cell lung cancer. Lung Cancer 2001, 34 (Suppl. S2), S127–S132. [Google Scholar] [CrossRef] [PubMed]
- Rajaram, R.; Paruch, J.L.; Mohanty, S.; Holl, J.L.; Bilimoria, K.Y.; Ko, C.Y.; Winchester, D.P.; Patel, J.D.; DeCamp, M.M. Patterns and predictors of chemotherapy use for resected non-small cell lung cancer. Ann. Thorac. Surg. 2015, 101, 533–540. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Riquet, M.; Berna, P.; Fabre, E.; Arame, A.; Dujon, A.; Foucault, C.; Barthes, F.L.P. Evolving characteristics of lung cancer: A surgical appraisal. Eur. J. Cardio-Thorac. Surg. 2012, 41, 1019–1024. [Google Scholar] [CrossRef]
- Buck, P.O.; Saverno, K.R.; Miller, P.J.; Arondekar, B.; Walker, M.S. Treatment patterns and health resource utilization among patients diagnosed with early stage resected non–small cell lung cancer at US community oncology practices. Clin. Lung Cancer 2014, 16, 486–495. [Google Scholar] [CrossRef]
- Soares, M.; Antunes, L.; Redondo, P.; Borges, M.; Hermans, R.; Patel, D.; Grimson, F.; Munro, R.; Chaib, C.; Lacoin, L.; et al. Treatment and outcomes for early non-small-cell lung cancer: A retrospective analysis of a Portuguese hospital database. Lung Cancer Manag. 2021, 10, LMT46. [Google Scholar] [CrossRef] [PubMed]
- Valle, L.F.; Jagsi, R.; Bobiak, S.N.; Zornosa, C.; D’Amico, T.A.; Pisters, K.M.; Dexter, E.U.; Niland, J.C.; Hayman, J.A.; Kapadia, N.S. Variation in definitive therapy for localized non-small cell lung cancer among national comprehensive cancer network institutions. Int. J. Radiat. Oncol. 2015, 94, 360–367. [Google Scholar] [CrossRef]
- Watanabe, S.-I.; Nakagawa, K.; Suzuki, K.; Takamochi, K.; Ito, H.; Okami, J.; Aokage, K.; Saji, H.; Yoshioka, H.; Zenke, Y.; et al. Lung Cancer Surgical Study Group (LCSSG) of the Japan Clinical Oncology Group (JCOG). Neoadjuvant and adjuvant therapy for Stage III non-small cell lung cancer. Ultrasound Med. Biol. 2017, 47, 1112–1118. [Google Scholar] [CrossRef]
- Berghmans, T.; Paesmans, M.; Meert, A.; Mascaux, C.; Lothaire, P.; Lafitte, J.; Sculier, J. Survival improvement in resectable non-small cell lung cancer with (neo)adjuvant chemotherapy: Results of a meta-analysis of the literature. Lung Cancer 2005, 49, 13–23. [Google Scholar] [CrossRef]
- NSCLC Meta-analyses Collaborative Group; Arriagada, R.; Auperin, A.; Burdett, S.; Higgins, J.P.; Johnson, D.H.; Le Chevalier, T.; Le Pechoux, C.; Parmar, M.K.; Pignon, J.P.; et al. Adjuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: Two meta-analyses of individual patient data. Lancet 2010, 375, 1267–1277. [Google Scholar] [CrossRef]
- Pignon, J.-P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.-Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung adjuvant cisplatin evaluation: A pooled analysis by the LACE collaborative group. J. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Quintero, J.H.; Kamel, M.K.; Jindani, R.; Zhu, R.; Friedmann, P.; Vimolratana, M.; Chudgar, N.P.; Stiles, B. Is underutilization of adjuvant therapy in resected non-small-cell lung cancer associated with socioeconomic disparities? Eur. J. Cardiothorac. Surg. 2023, 64, ezad383. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Li, L.; Chen, X.; Chen, N.; Song, W.; Cui, J. Neoadjuvant and adjuvant immunotherapy: Opening new horizons for patients with early-stage non-small cell lung cancer. Front. Oncol. 2020, 10, 575472. [Google Scholar] [CrossRef] [PubMed]
- Sandler, J.E.; D’aiello, A.; Halmos, B. Changes in store for early-stage non-small cell lung cancer. J. Thorac. Dis. 2019, 11, 2117–2125. [Google Scholar] [CrossRef]
- Winget, M.; Stanger, J.; Gao, Z.; Butts, C. Predictors of surgery and consult with an oncologist for adjuvant chemotherapy in early stage NSCLC patients in Alberta, Canada. J. Thorac. Oncol. 2009, 4, 629–634. [Google Scholar] [CrossRef]
- O’Sullivan, D.E.; Jarada, T.N.; Yusuf, A.; Hu, L.X.Y.; Gogna, P.; Brenner, D.R.; Abbie, E.; Rose, J.B.; Eaton, K.; Elia-Pacitti, J.; et al. Prevalence, treatment patterns, and outcomes of individuals with EGFR positive metastatic non-small cell lung cancer in a Canadian real-world setting: A comparison of exon 19 deletion, L858R, and exon 20 insertion EGFR mutation carriers. Curr. Oncol. 2022, 29, 7198–7208. [Google Scholar] [CrossRef]
- O’Sullivan, D.E.; Cheung, W.Y.; Syed, I.A.; Moldaver, D.; Shanahan, M.K.; Bebb, D.G.; Sit, C.; Brenner, D.R.; Boyne, D.J. Real-world treatment patterns, clinical outcomes, and health care resource utilization in extensive-stage small cell lung cancer in Canada. Curr. Oncol. 2021, 28, 3091–3103. [Google Scholar] [CrossRef]
- University of Calgary. Alberta Thoracic Oncology Program. Available online: https://cumming.ucalgary.ca/research/interventional-pulmonary-medicine/thoracic-oncology-program (accessed on 15 December 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 5126) | Systemic Therapy (n = 1210) | No Systemic Therapy (n = 3916) | p-Value | SMD |
|---|---|---|---|---|---|
| Age, years (mean (SD)) | 71.3 (10.3) | 65.5 (8.7) | 73.0 (10.1) | <0.001 | 0.79 |
| Age (n (%)) | |||||
| <65 years | 1285 (25.1) | 520 (43.0) | 765 (19.5) | <0.001 | 0.523 |
| 65+ years | 3841 (74.9) | 690 (57.0) | 3151 (80.5) | ||
| Sex (n (%)) | 0.02 | 0.079 | |||
| Male | 2433 (47.5) | 611 (50.5) | 1822 (46.5) | ||
| Female | 2693 (52.5) | 599 (49.5) | 2094 (53.5) | ||
| AJCC Stage (n (%)) | <0.001 | 0.975 | |||
| IB | 1590 (31.0) | 55 (4.6) | 1535 (39.2) | ||
| IIA | 686 (13.4) | 191 (15.8) | 495 (12.6) | ||
| IIB | 909 (17.7) | 217 (17.9) | 692 (17.7) | ||
| IIIA | 1941 (37.9) | 747 (61.7) | 1194 (30.5) | ||
| Subtype (n (%)) | 0.98 | 0.002 | |||
| Squamous | 1560 (30.4) | 369 (30.5) | 1191 (30.4) | ||
| Non-squamous | 3566 (69.6) | 841 (69.5) | 2725 (69.6) | ||
| Categories of Neighbourhood Annual Household Income (n (%)) | 0.18 | 0.076 | |||
| 0–25 k | 203 (4.0) | 35 (2.9) | 168 (4.3) | ||
| 25–35 k | 942 (18.4) | 225 (18.6) | 717 (18.3) | ||
| 35–45 | 1708 (33.3) | 404 (33.4) | 1304 (33.3) | ||
| 45 k+ | 2265 (44.2) | 545 (45.0) | 1720 (43.9) | ||
| Missing | 8 (0.2) | 1 (0.1) | 7 (0.2) | ||
| Categories of Neighbourhood Education (n (%)) | 0.06 | 0.092 | |||
| 0.00–0.60 | 363 (7.1) | 66 (5.5) | 297 (7.6) | ||
| 0.60–0.70 | 733 (14.3) | 169 (14.0) | 564 (14.4) | ||
| 0.70–0.80 | 1391 (27.1) | 345 (28.5) | 1046 (26.7) | ||
| 0.80+ | 2631 (51.3) | 629 (52.0) | 2002 (51.1) | ||
| Missing | 8 (0.2) | 1 (0.1) | 7 (0.2) | ||
| Charlson Comorbidity Index (n (%)) | <0.001 | 0.375 | |||
| 0 | 2169 (42.3) | 615 (50.8) | 1554 (39.7) | ||
| 1 | 1665 (32.5) | 420 (34.7) | 1245 (31.8) | ||
| 2 | 681 (13.3) | 109 (9.0) | 572 (14.6) | ||
| 3 | 327 (6.4) | 44 (3.6) | 283 (7.2) | ||
| 4+ | 284 (5.5) | 22 (1.8) | 262 (6.7) | ||
| Cardiovascular disease (n (%)) 1 | 838 (16.3) | 108 (8.9) | 730 (18.6) | <0.001 | 0.285 |
| Diabetes (n (%)) | 981 (19.1) | 189 (15.6) | 792 (20.2) | <0.001 | 0.120 |
| Chronic Obstructive Pulmonary Disease (n (%)) | 1908 (37.2) | 403 (33.3) | 1505 (38.4) | 0.001 | 0.107 |
| Connective Tissue Disease (n (%)) | 112 (2.2) | 21 (1.7) | 91 (2.3) | 0.26 | 0.042 |
| Liver disease (n (%)) | 95 (1.9) | 24 (2.0) | 71 (1.8) | 0.79 | 0.012 |
| Renal disease (n (%)) | 230 (4.5) | 15 (1.2) | 215 (5.5) | <0.001 | 0.237 |
| Variable | Overall (n = 5126) | IB (n = 1590) | II (n = 1595) | IIIA (n = 1941) | p-Value | SMD |
|---|---|---|---|---|---|---|
| Surgery (%) | 2367 (47.2) | 941 (59.2) | 927 (58.1) | 499 (25.7) | <0.001 | 0.479 |
| Systemic therapy (%) | 1210 (23.6) | 55 (3.5) | 408 (25.6) | 747 (38.5) | <0.001 | 0.631 |
| Radiation therapy (%) | 1706 (33.3) | 338 (21.3) | 410 (25.7) | 958 (49.4) | <0.001 | 0.408 |
| No Surgery (%) | 2759 (53.8) | 649 (40.8) | 668 (41.9) | 1442 (74.3) | <0.001 | 0.479 |
| Systemic therapy | 548 (19.9) | 21 (3.2) | 64 (9.6) | 463 (32.1) | <0.001 | 0.552 |
| Radiation therapy | 1506 (54.6) | 322 (49.6) | 352 (52.7) | 832 (57.7) | 0.002 | 0.108 |
| Neoadjuvant 1 (%) | 71 (3.0) | <10 | 14 (1.5) | 53 (10.6) | <0.001 | 0.319 |
| Systemic therapy | 66 (2.8) | <10 | 12 (1.3) | 51 (10.2) | <0.001 | 0.318 |
| Radiation therapy | 58 (2.5) | <10 | 11 (1.2) | 46 (9.2) | <0.001 | 0.315 |
| Adjuvant 2 (%) | 699 (29.5) | 44 (4.7) | 363 (39.2) | 292 (58.5) | <0.001 | 0.911 |
| Systemic therapy | 616 (26.0) | 31 (3.3) | 333 (35.9) | 254 (50.9) | <0.001 | 0.819 |
| Radiation therapy | 150 (6.3) | 16 (1.7) | 50 (5.4) | 84 (16.8) | <0.001 | 0.370 |
| Variable | Overall (n = 5126) | IB (n = 1590) | IIA (n = 1595) | IIIA (n = 1941) |
|---|---|---|---|---|
| Referred to Medical Oncologist (n [%]) | 2323 (45.3) | 377 (23.7) | 815 (51.1) | 1131 (58.3) |
| Systemic Therapy among Referred Patients (n [%]) | 1181 (50.8) | 49 (13.0) | 394 (48.3) | 738 (65.3) |
| Variable | Strata | Median Survival 1 (95% CI) | 1-Year Survival (95% CI) | 2-Year Survival (95% CI) | 5-Year Survival (95% CI) | Log-Rank Test p-Value | Crude Hazard Ratio (95% CI) |
|---|---|---|---|---|---|---|---|
| Age | <65 years | 54.74 (45.60–60.30) | 0.829 (0.809–0.851) | 0.676 (0.650–0.704) | 0.472 (0.441–0.505) | <0.001 | Ref (1.0) |
| ≥65 years | 24.26 (23.08–25.35) | 0.698 (0.684–0.713) | 0.503 (0.487–0.520) | 0.258 (0.243–0.275) | 1.84 (1.69–2.00) | ||
| Sex | Male | 23.84 (22.45–22.15) | 0.699 (0.681–0.718) | 0.498 (0.478–0.519) | 0.272 (0.252–0.293) | <0.001 | Ref (1.0) |
| Female | 33.11 (31.00–35.54) | 0.760 (0.744–0.777) | 0.591 (0.572–0.610) | 0.347 (0.327–0.369) | 0.80 (0.74–0.85) | ||
| Comorbidity | No | 35.31 (32.71–37.97) | 0.797 (0.780–0.815) | 0.601 (0.580–0.623) | 0.361 (0.338–0.386) | <0.001 | Ref (1.0) |
| Yes | 24.49 (22.95–25.91) | 0.683 (0.666–0.700) | 0.507 (0.489–0.526) | 0.276 (0.258–0.295) | 1.32 (1.23–1.41) | ||
| Stage | IB | 49.01 (45.00–54.15) | 0.855 (0.837–0.873) | 0.724 (0.702–0.748) | 0.435 (0.407–0.465) | <0.001 | Ref (1.0) |
| IIA | 36.56 (32.94–42.25) | 0.798 (0.768–0.829) | 0.626 (0.590–0.665) | 0.369 (0.331–0.412) | 1.24 (1.10–1.39) | ||
| IIB | 29.23 (25.32–33.11) | 0.741 (0.712–0.770) | 0.561 (0.528–0.596) | 0.333 (0.298–0.372) | 1.44 (1.30–1.61) | ||
| IIIA | 16.50 (15.39–17.59) | 0.605 (0.584–0.628) | 0.373 (0.352–0.396) | 0.186 (0.167–0.206) | 2.23 (2.04–2.42) | ||
| Systemic therapy | No | 25.15 (24.07–26.70) | 0.691 (0.677–0.706) | 0.517 (0.501–0.533) | 0.287 (0.271–0.304) | <0.001 | Ref (1.0) |
| Yes | 37.51 (35.44–42.21) | 0.857 (0.837–0.877) | 0.641 (0.613–0.669) | 0.389 (0.358–0.422) | 0.69 (0.63–0.75) | ||
| Surgery | No | 15.29 (14.43–16.34) | 0.587 (0.569–0.606) | 0.352 (0.334–0.370) | 0.121 (0.107–0.136) | <0.001 | Ref (1.0) |
| Yes | 66.61 (63.45–73.32) | 0.907 (0.895–0.919) | 0.790 (0.773–0.808) | 0.553 (0.529–0.578) | 0.27 (0.25–0.29) | ||
| Radiation therapy | No | 36.13 (33.27–38.37) | 0.752 (0.737–0.767) | 0.601 (0.584–0.619) | 0.379 (0.361–0.399) | <0.001 | Ref (1.0) |
| Yes | 20.52 (19.00–22.12) | 0.692 (0.670–0.714) | 0.445 (0.421–0.469) | 0.181 (0.161–0.204) | 1.60 (1.49–1.71) | ||
| Systemic therapy in stage IB | No | 50.43 (45.53–54.67) | 0.854 (0.836–0.872) | 0.723 (0.700–0.747) | 0.437 (0.409–0.468) | 0.4 | Ref (1.0) |
| Yes | 36.00 (30.21–82.85) | 0.891 (0.812–0.977) | 0.754 (0.646–0.880) | 0.368 (0.247–0.550) | 1.16 (0.82–1.63) | ||
| Systemic therapy in stage IIA | No | 28.31 (24.26–34.29) | 0.738 (0.700–0.779) | 0.555 (0.512–0.602) | 0.293 (0.251–0.342) | <0.001 | Ref (1.0) |
| Yes | 68.15 (54.74-NA) | 0.952 (0.921–0.983) | 0.808 (0.752–0.867) | 0.562 (0.489–0.646) | 0.44 (0.35–0.56) | ||
| Systemic therapy in stage IIB | No | 24.49 (21.37–27.16) | 0.694 (0.660–0.730) | 0.505 (0.467–0.546) | 0.274 (0.237–0.317) | <0.001 | Ref (1.0) |
| Yes | 67.17 (42.21–98.37) | 0.887 (0.844–0.931) | 0.740 (0.680–0.806) | 0.543 (0.467–0.631) | 0.47 (0.38–0.60) | ||
| Systemic therapy in stage IIIA | No | 10.98 (10.16–11.97) | 0.469 (0.442–0.499) | 0.253 (0.229–0.280) | 0.109 (0.091–0.130) | <0.001 | Ref (1.0) |
| Yes | 30.81 (26.47–35.44) | 0.822 (0.794–0.850) | 0.564 (0.529–0.602) | 0.310 (0.274–0.350) | 0.43 (0.38–0.48) | ||
| Surgery and systemic therapy | Surgery only | 68.91 (63.88–74.93) | 0.901 (0.887–0.916) | 0.796 (0.776–0.817) | 0.561 (0.533–0.590) | 0.5 | Ref (1.0) |
| Both | 63.48 (57.07–74.10) | 0.920 (0.900–0.942) | 0.775 (0.742–0.809) | 0.532 (0.490–0.578) | 1.05 (0.96–1.20) | ||
| Surgery and systemic therapy in stage IB | Surgery only | 83.70 (74.33–92.94) | 0.952 (0.938–0.967) | 0.878 (0.855–0.901) | 0.645 (0.608–0.685) | 0.08 | Ref (1.0) |
| Both | 61.12 (32.98-NA) | 0.912 (0.821–1.000) | 0.845 (0.729–0.980) | 0.530 (0.368–0.763) | 1.56 (0.95–2.55) | ||
| Surgery and systemic therapy in stage IIA | Surgery only | 64.4 (58.72–80.48) | 0.893 (0.854–0.933) | 0.777 (0.725–0.834) | 0.542 (0.473–0.622) | 0.04 | Ref (1.0) |
| Both | 75.91 (63.45-NA) | 0.957 (0.926–0.989) | 0.842 (0.787–0.901) | 0.613 (0.536–0.701) | 0.73 (0.54–0.99) | ||
| Surgery and systemic therapy in stage IIB | Surgery only | 59.15 (45.07–69.67) | 0.887 (0.852–0.923) | 0.745 (0.696–0.798) | 0.484 (0.422–0.555) | 0.01 | Ref (1.0) |
| Both | 78.35 (64.37-NA) | 0.932 (0.894–0.972) | 0.810 (0.749–0.877) | 0.608 (0.523–0.705) | 0.69 (0.51–0.93) | ||
| Surgery and systemic therapy in stage IIIA | Surgery only | 32.09 (23.51–39.06) | 0.724 (0.665–0.787) | 0.562 (0.497–0.635) | 0.358 (0.293–0.438) | 0.002 | Ref (1.0) |
| Both | 45.17 (40.04–62.60) | 0.893 (0.857–0.931) | 0.707 (0.653–0.764) | 0.449 (0.388–0.520) | 0.70 (0.55–0.88) |
| Construct | Outcome | Year 1 (n = 5126) | Year 2 (n = 3524) | Year 3 (n = 2397) | Year 4 (n = 1668) | Year 5 (n = 1129) |
|---|---|---|---|---|---|---|
| Hospitalizations | No. of Hospitalizations | 1.39 | 0.67 | 0.51 | 0.49 | 0.46 |
| No. of Days Hospitalized | 13.52 | 8.27 | 6.26 | 5.25 | 5.01 | |
| Ambulatory Care Services | No. of Encounters | 11.89 | 7.58 | 6.92 | 6.44 | 6.15 |
| No. of Emergency Encounters | 1.98 | 1.54 | 1.35 | 1.2 | 1.23 | |
| No. of Non-emergency Encounters | 9.91 | 6.04 | 5.57 | 5.25 | 4.92 | |
| Cancer Physician Visits | No. of Visits | 4.68 | 2.58 | 2.18 | 1.92 | 1.73 |
| No. of Medical Oncologist Visits | 2.19 | 1.5 | 1.37 | 1.2 | 1.16 | |
| No. of Radiation Oncologist Visits | 2.1 | 0.84 | 0.64 | 0.58 | 0.45 | |
| No. of General/Family Practitioner Visits | 0.13 | 0.08 | 0.05 | 0.04 | 0.03 | |
| No. of Other Cancer Physician Visits | 0.26 | 0.17 | 0.12 | 0.11 | 0.09 | |
| Non-Cancer Practitioner Visits | No. of Encounters | 33.62 | 23.91 | 21.47 | 19.95 | 20.79 |
| No. of Claims | 68.11 | 41.84 | 36.98 | 34.76 | 35.87 | |
| Final Claims Assessment Amount | 7790.71 | 3456.5 | 2918.52 | 2719.26 | 2838.39 | |
| Radiation Therapy | No. of Days of Therapy | 7.97 | 1.18 | 0.92 | 0.78 | 0.62 |
| Chemotherapy Cycles | No. of Cycles | 1.72 | 0.78 | 0.69 | 0.67 | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Sullivan, D.E.; Boyne, D.J.; Ford-Sahibzada, C.; Inskip, J.A.; Smith, C.J.; Sripada, K.; Brenner, D.R.; Cheung, W.Y. Real-World Treatment Patterns, Clinical Outcomes, and Healthcare Resource Utilization in Early-Stage Non-Small-Cell Lung Cancer. Curr. Oncol. 2024, 31, 447-461. https://doi.org/10.3390/curroncol31010030
O’Sullivan DE, Boyne DJ, Ford-Sahibzada C, Inskip JA, Smith CJ, Sripada K, Brenner DR, Cheung WY. Real-World Treatment Patterns, Clinical Outcomes, and Healthcare Resource Utilization in Early-Stage Non-Small-Cell Lung Cancer. Current Oncology. 2024; 31(1):447-461. https://doi.org/10.3390/curroncol31010030
Chicago/Turabian StyleO’Sullivan, Dylan E., Devon J. Boyne, Chelsea Ford-Sahibzada, Jessica A. Inskip, Christopher J. Smith, Kaushik Sripada, Darren R. Brenner, and Winson Y. Cheung. 2024. "Real-World Treatment Patterns, Clinical Outcomes, and Healthcare Resource Utilization in Early-Stage Non-Small-Cell Lung Cancer" Current Oncology 31, no. 1: 447-461. https://doi.org/10.3390/curroncol31010030
APA StyleO’Sullivan, D. E., Boyne, D. J., Ford-Sahibzada, C., Inskip, J. A., Smith, C. J., Sripada, K., Brenner, D. R., & Cheung, W. Y. (2024). Real-World Treatment Patterns, Clinical Outcomes, and Healthcare Resource Utilization in Early-Stage Non-Small-Cell Lung Cancer. Current Oncology, 31(1), 447-461. https://doi.org/10.3390/curroncol31010030