
XBeats: A Real-Time Electrocardiogram Monitoring and Analysis System



Abstract
:1. Introduction
2. Background and Related Work
2.1. Single Lead ECG
2.2. Two ECG Leads or More
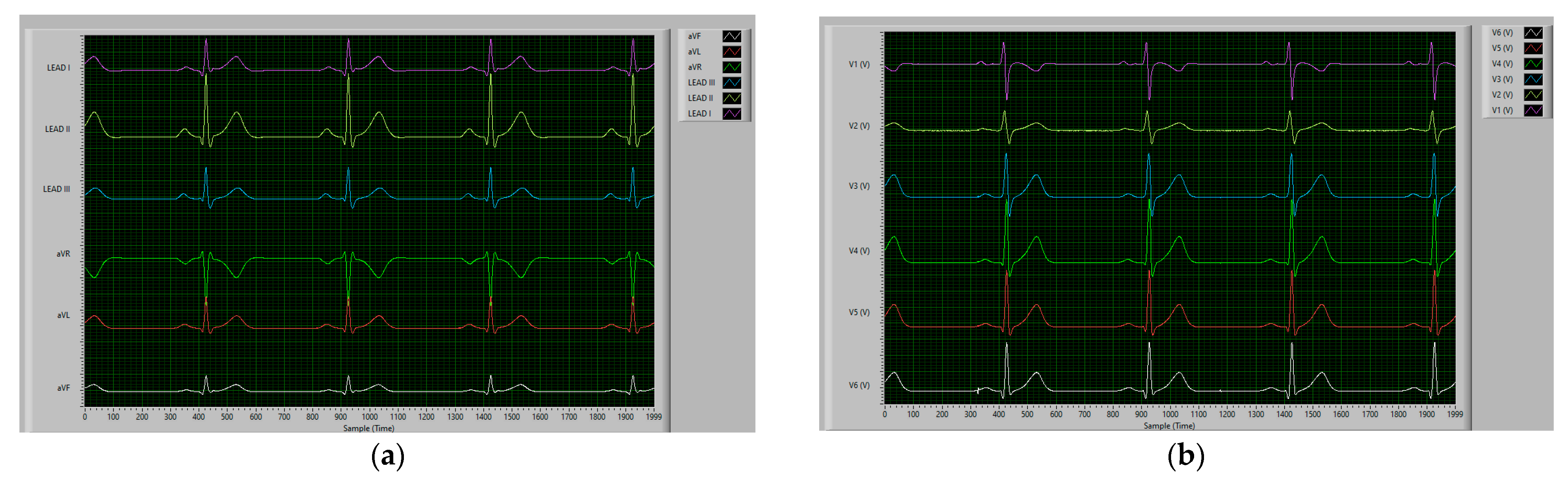
2.3. Standard 12-Lead ECG
2.4. Commercial ECG Devices
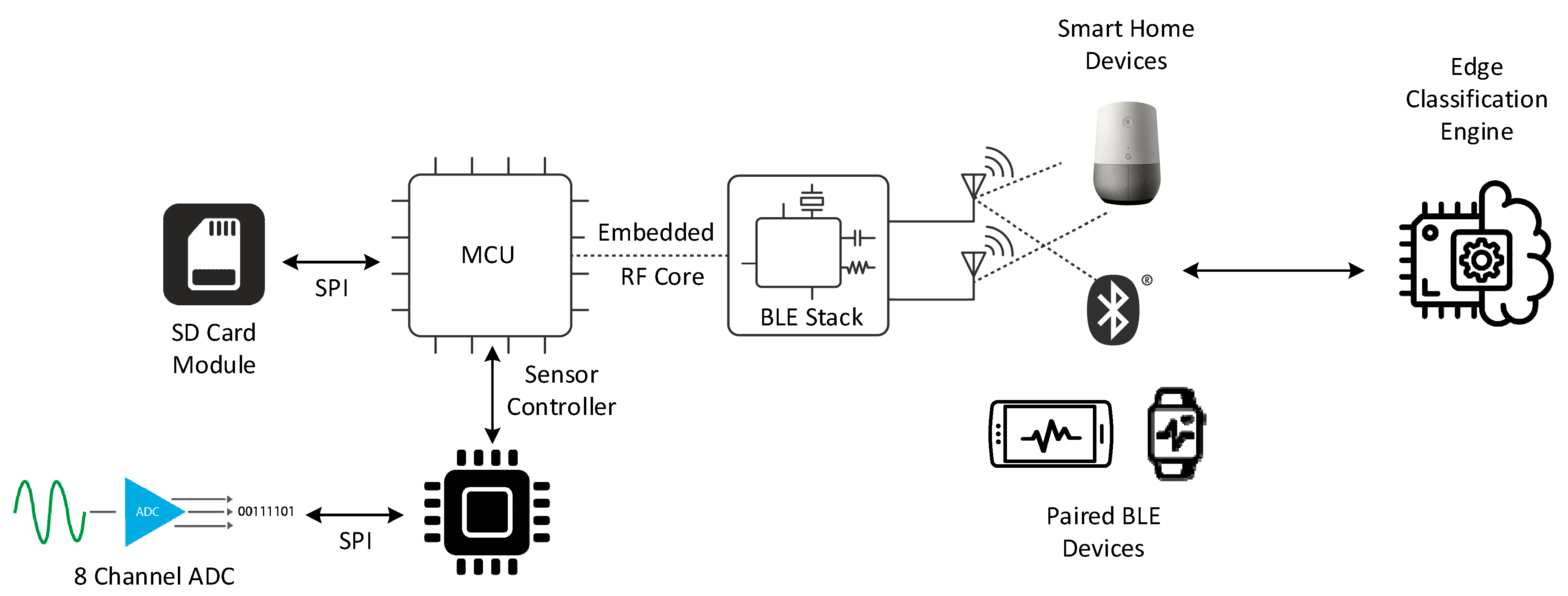
3. XBeats System Architecture
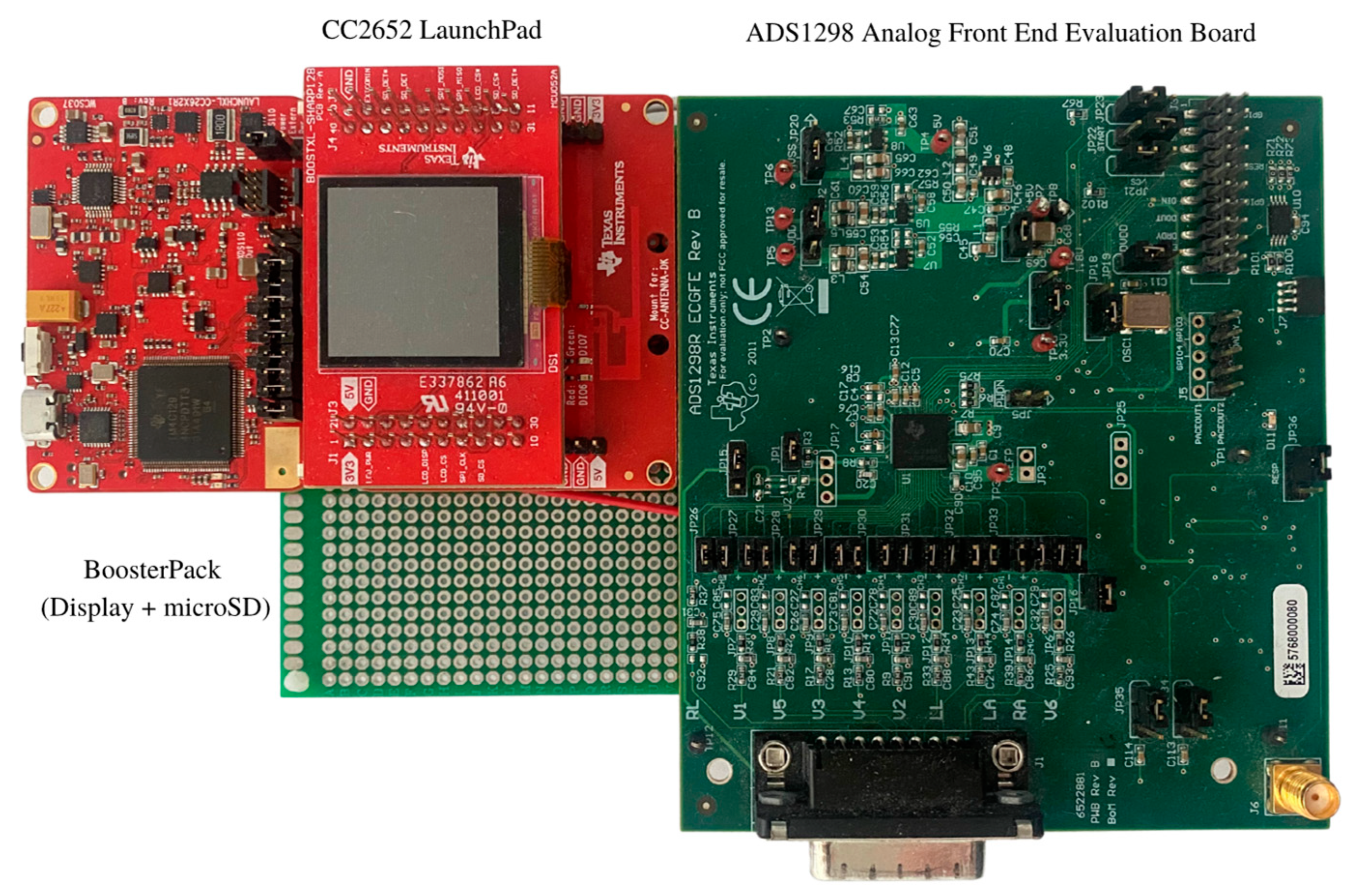
3.1. Hardware Specifications
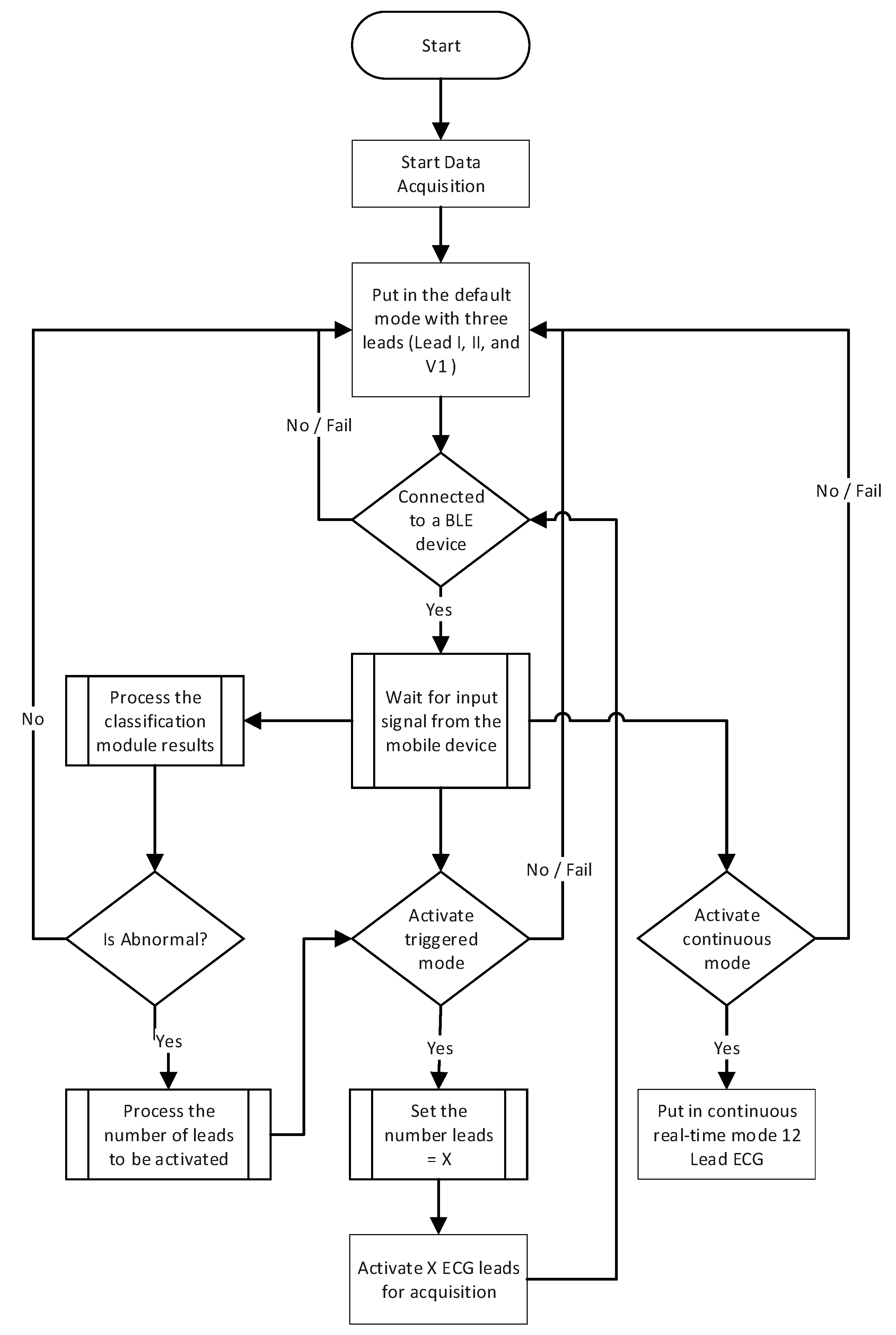
- The continuous mode provides an unbounded real-time high-resolution data stream of the 12-lead ECG data transmitted directly to a backend system. Physicians sometimes require this mode of operation if abnormal heart conditions are detected or the patient’s case requires 24/7 monitoring. However, this mode has a significant power consumption profile that affects the device’s battery lifetime due to the continuous transmission of the collected ECG data wirelessly to the backend system via a communication gateway;
- The offline mode records the 12-lead ECG data on the Multimedia Card (MMC) storage when no paired BLE device is nearby to connect to the ECG patch. This mode is enabled for the entire data acquisition period until a paired BLE device connects to the patch and synchronizes the data transfer to the backend system; and
- The triggered mode is optimized for power saving. The device sends keep-alive signals in normal heart conditions and only transmits ECG signals when a potential heart abnormality is detected. The ECG patch chooses from three data acquisition settings where the number of leads is configurable. The default setting for this operation mode is three ECG leads (e.g., Lead I, II, and V1), which can be changed dynamically in real-time. The patient and healthcare provider can reconfigure the number of enabled ECG leads through a paired BLE-enabled device or the backend system.
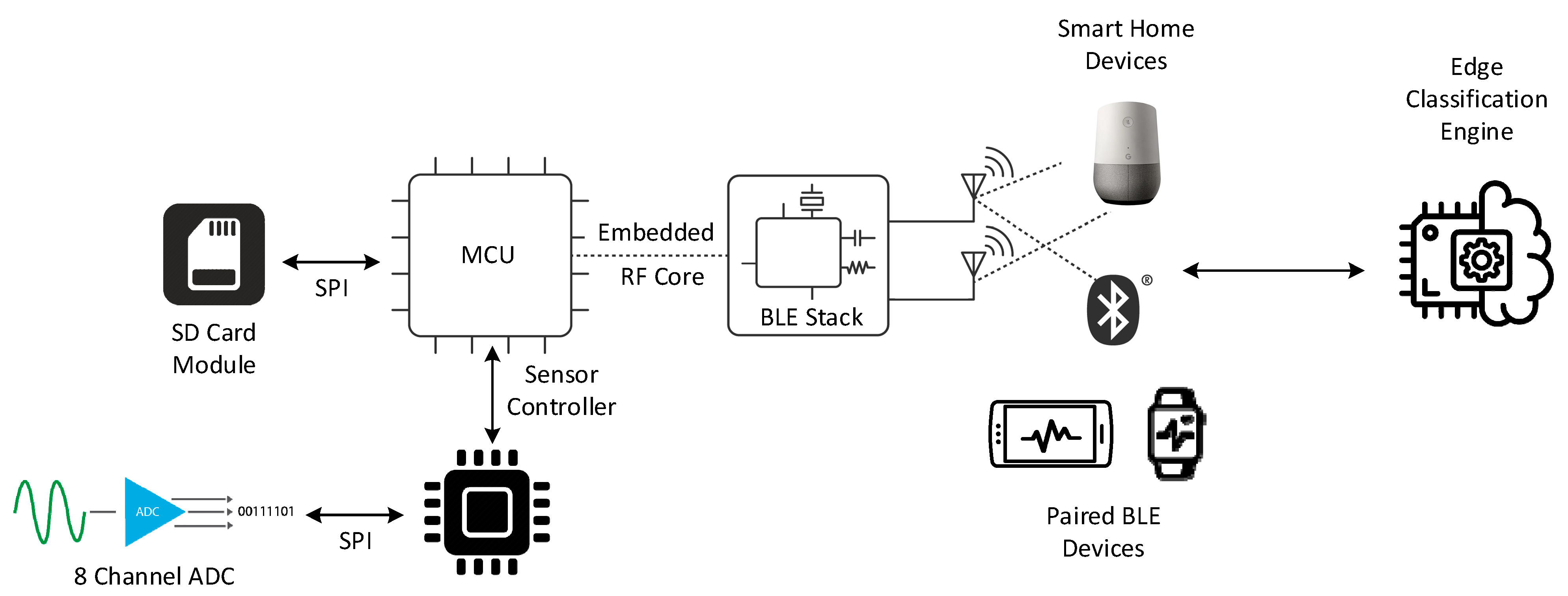
3.1.1. Data Acquisition
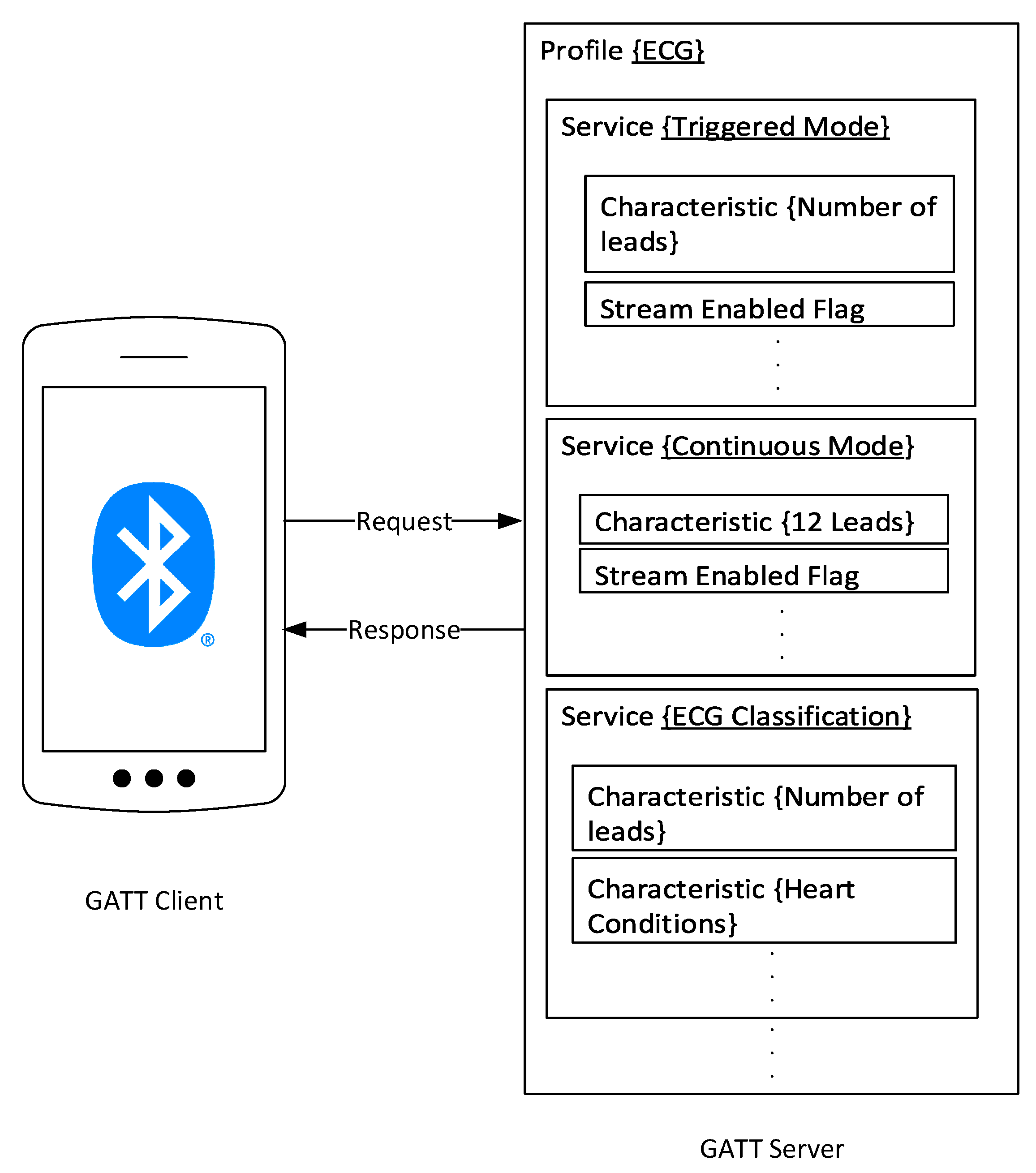
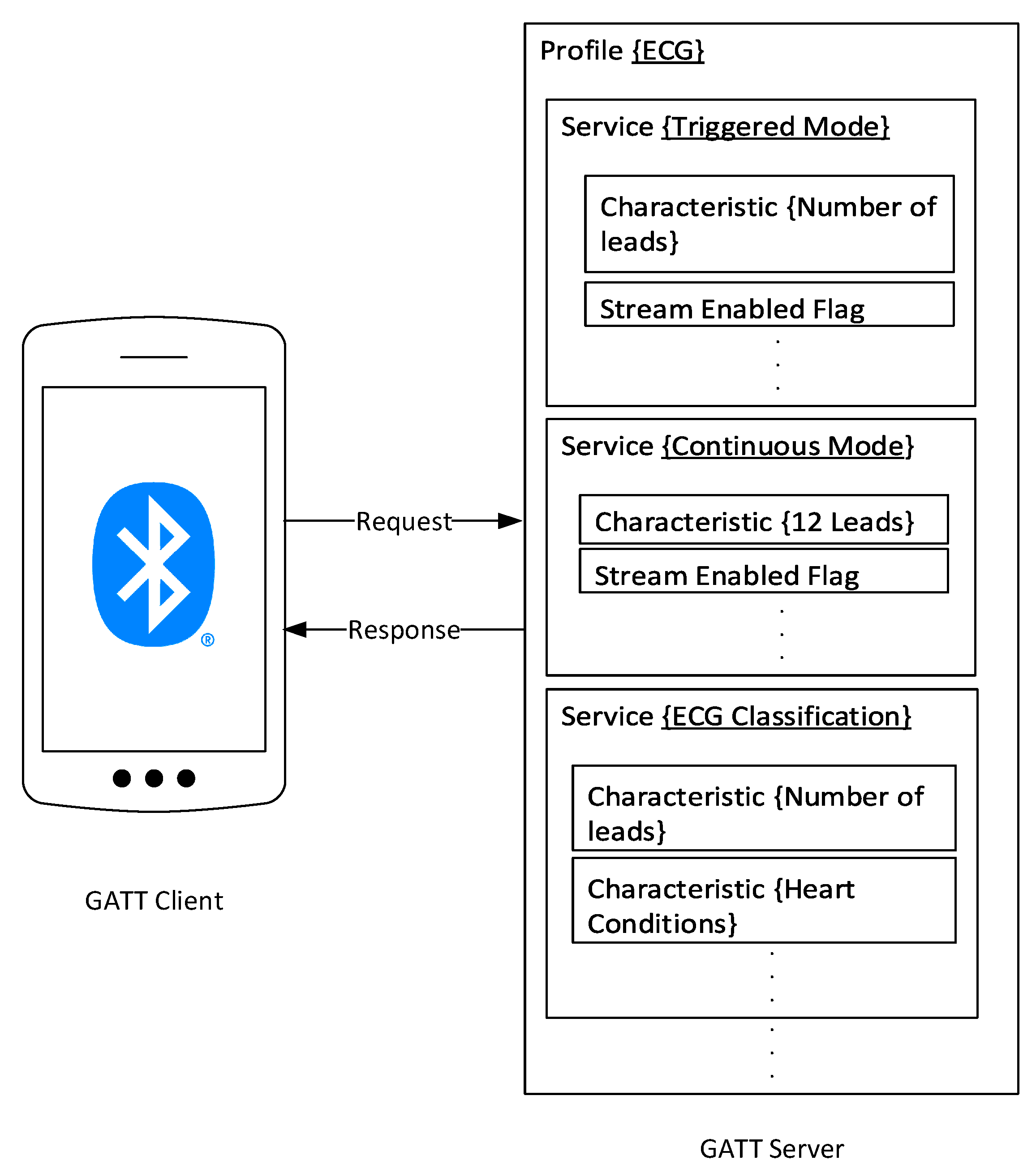
3.1.2. Data Transmission and Protocols
3.1.3. Data Logging
3.1.4. Edge Classification
4. Prototype Implementation
4.1. Data Acquisition and Logging
4.2. Data Transmission
5. Experimental Results and Discussions
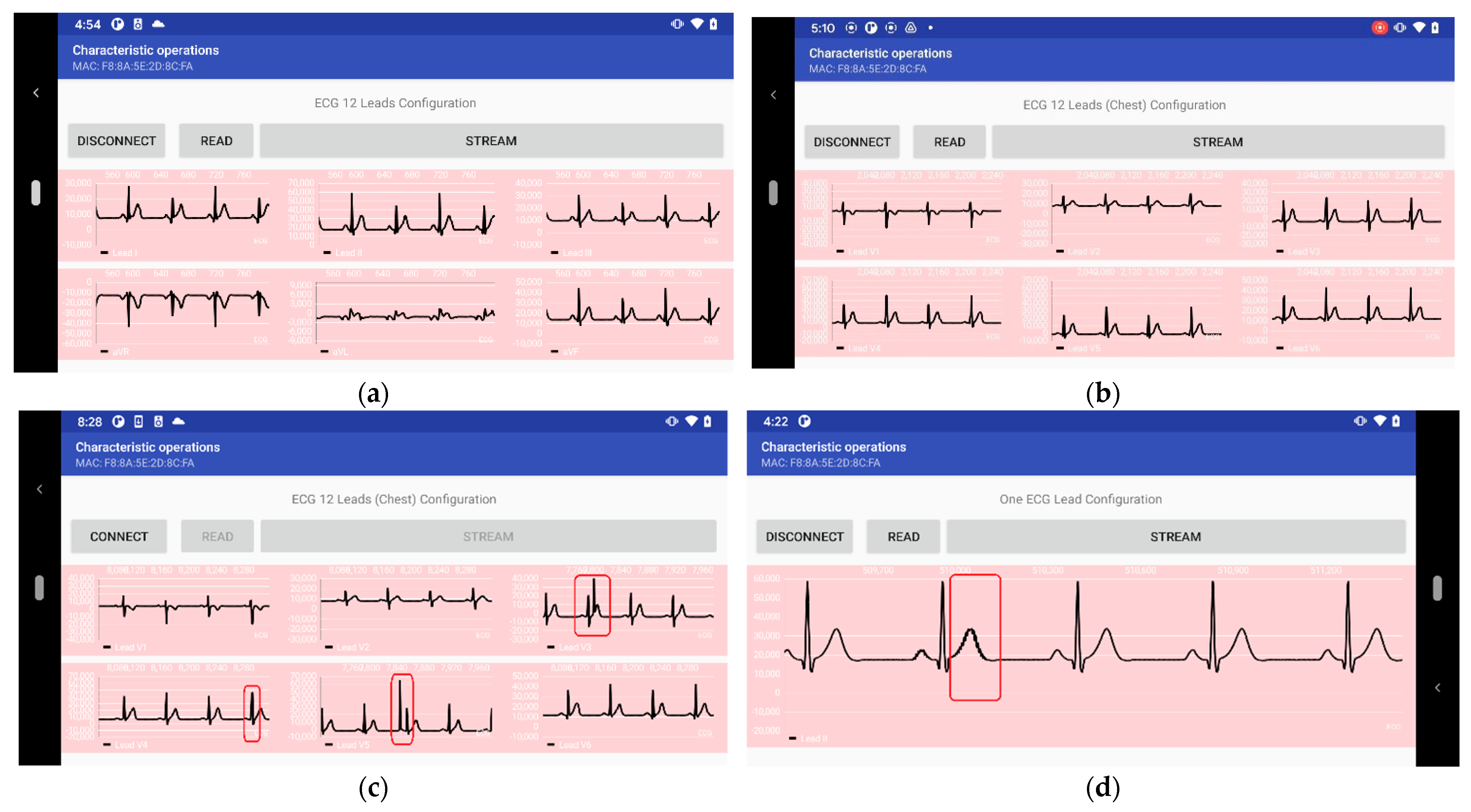
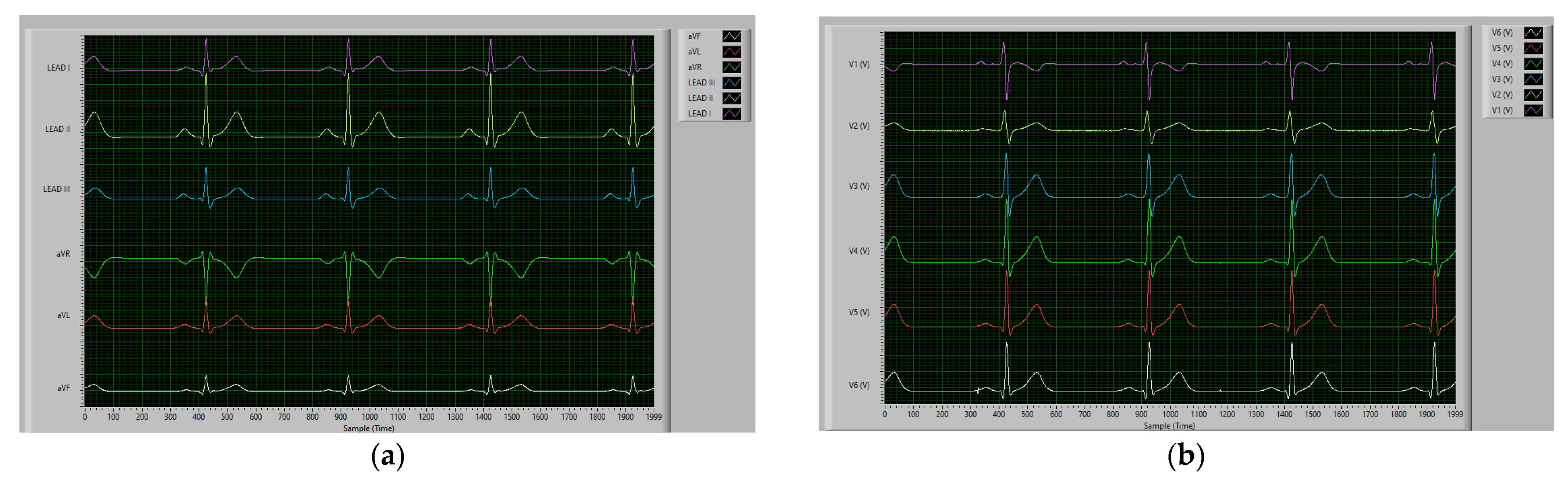
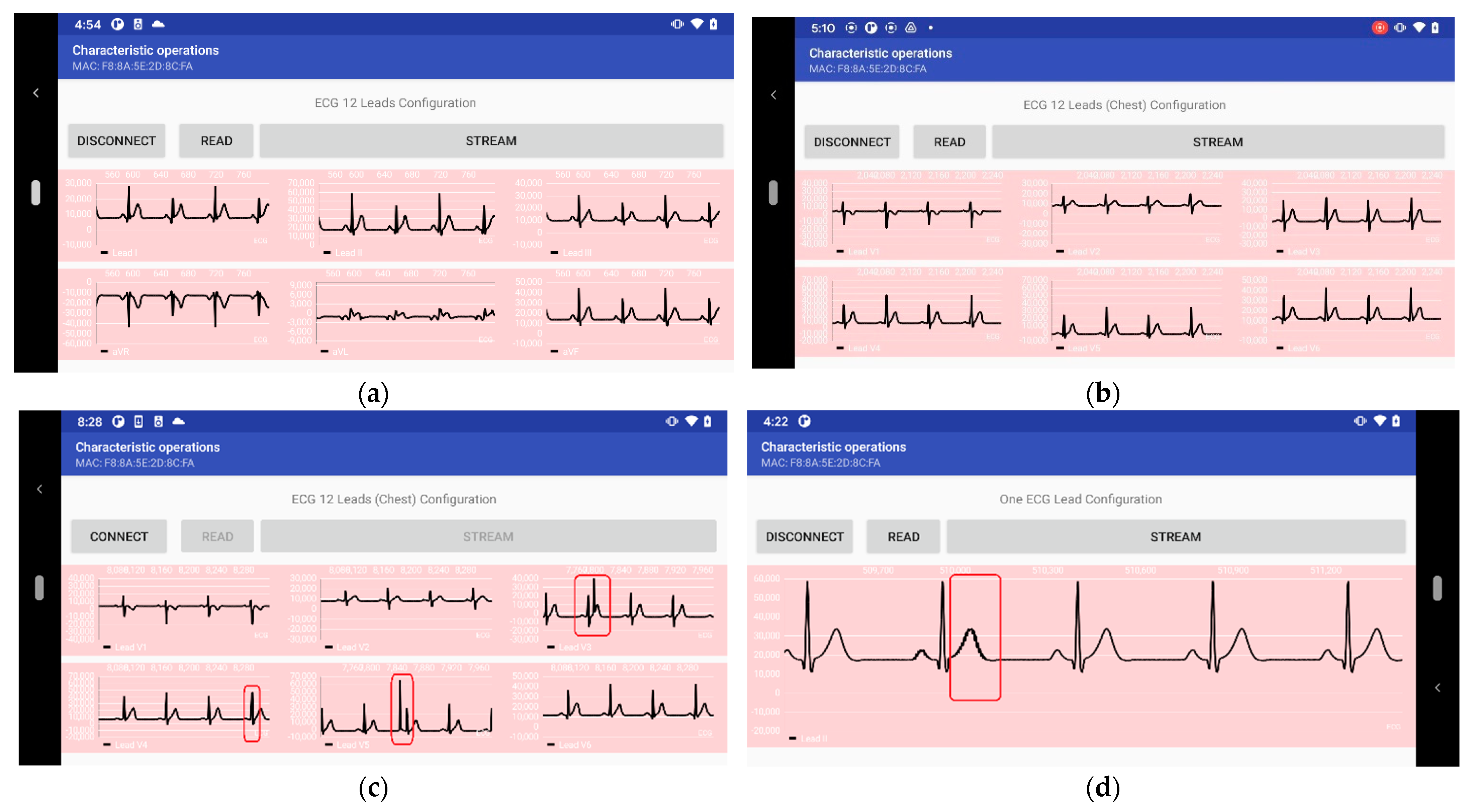
- Collect ECG data in real-time using the prototype hardware of the ECG patch. The experiment includes acquiring ECG data at different modes of operation: standard 12-Lead ECG data under the “continuous” mode of operation; one and three ECG leads under the triggered mode of operation; standard 12-lead ECG data under the offline mode of operation;
- Evaluate the effective ECG data sampling rate compared to the theoretical data acquisition values provided by the analog to digital converter. The evaluation is performed on each of the operation modes above;
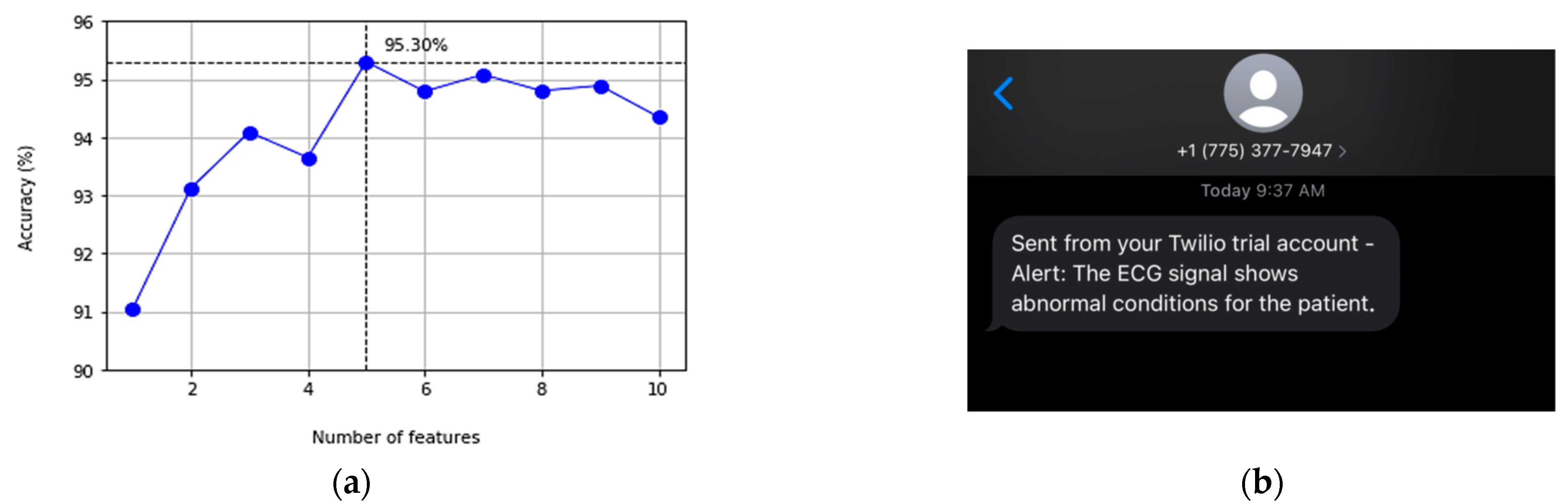
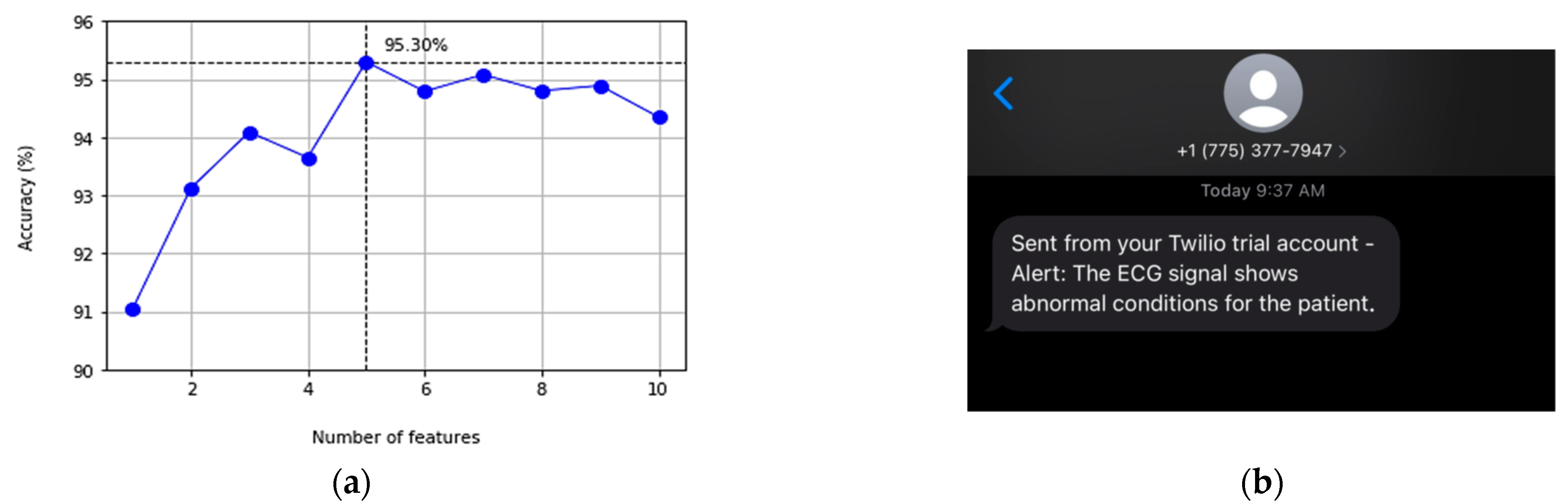
- Evaluate the proposed ECG classification service implemented on an edge node. The evaluation steps include comparing the accuracy and processing time of six different techniques, which is concluded by the selected classification techniques for our edge classification service; and
- Calculate the power consumption footprint and the energy-saving of applying the triggered operation mode while activating the edge classification service.
5.1. Data Sources Description
5.2. Data Acquisition and Data Transmission
5.3. Signal Detection and Classification
5.4. Energy Consumption
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Cardiovascular Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 25 January 2022).
- Ashley, E.A.; Niebauer, J. Conquering the ECG. In Cardiology Explained; Remedica: London, UK, 2004; pp. 15–33. [Google Scholar]
- Galli, A.; Ambrosini, F.; Lombardi, F. Holter Monitoring and Loop Recorders: From Research to Clinical Practice. Arrhythmia Electrophysiol. Rev. 2016, 5, 136–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mubarik, A.; Iqbal, A.M. Holter Monitor. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chua, S.-K.; Chen, L.-C.; Lien, L.-M.; Lo, H.-M.; Liao, Z.-Y.; Chao, S.-P.; Chuang, C.-Y.; Chiu, C.-Z. Comparison of Arrhythmia Detection by 24-Hour Holter and 14-Day Continuous Electrocardiography Patch Monitoring. Acta Cardiol. Sin. 2020, 36, 251–259. [Google Scholar]
- Serhani, M.A.; El Kassabi, H.T.; Ismail, H.; Navaz, A.N. ECG monitoring systems: Review, architecture, processes, and key challenges. Sensors 2020, 20, 1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshamrani, M. IoT and artificial intelligence implementations for remote healthcare monitoring systems: A survey. J. King Saud Univ.-Comput. Inf. Sci. 2021. [Google Scholar] [CrossRef]
- Nasir, F.; Abubakar, A.; Emmanuel, I.; Folawiyo, Y.Y.; Adewole, K.S.; Mojeed, H.A.; Oloyede, A.A.; Olawoyin, L.A.; Sikiru, I.A.; Nehemiah, A.; et al. A comprehensive survey on low-cost ECG acquisition systems: Advances on design specifications, challenges and future direction. Biocybern. Biomed. Eng. 2021, 41, 474–502. [Google Scholar]
- Kwon, S.; Lee, S.-R.; Choi, E.-K.; Ahn, H.-J.; Song, H.-S.; Lee, Y.-S.; Oh, S. Validation of Adhesive Single-Lead ECG Device Compared with Holter Monitoring among Non-Atrial Fibrillation Patients. Sensors 2021, 21, 3122. [Google Scholar] [CrossRef]
- Sahoo, P.K.; Thakkar, H.K.; Lin, W.-Y.; Chang, P.-C.; Lee, M.-Y. On the design of an efficient cardiac health monitoring system through combined analysis of ECG and SCG signals. Sensors 2018, 18, 379. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, P.K.; Thakkar, H.K.; Lee, M.-Y. A cardiac early warning system with multi channel SCG and ECG monitoring for mobile health. Sensors 2017, 17, 711. [Google Scholar] [CrossRef]
- Klum, M.; Leib, F.; Oberschelp, C.; Martens, D.; Pielmus, A.-G.; Tigges, T.; Penzel, T.; Orglmeister, R. Wearable Multimodal Stethoscope Patch for Wireless Biosignal Acquisition and Long-Term Auscultation. In 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); Institute of Electrical and Electronics Engineers (IEEE): Berlin, Germany, 2019; pp. 5781–5785. [Google Scholar]
- Rashkovska, A.; Depolli, M.; Tomašić, I.; Avbelj, V.; Trobec, R. Medical-grade ECG sensor for long-term monitoring. Sensors 2020, 20, 1695. [Google Scholar] [CrossRef] [Green Version]
- Rincon, J.A.; Guerra-Ojeda, S.; Carrascosa, C.; Julian, V. An IoT and Fog Computing-Based Monitoring System for Cardiovascular Patients with Automatic ECG Classification Using Deep Neural Networks. Sensors 2020, 20, 7353. [Google Scholar] [CrossRef]
- Ahsanuzzaman, S.; Ahmed, T.; Rahman, A. Low Cost, Portable ECG Monitoring and Alarming System Based on Deep Learning. In Proceedings of the 2020 IEEE Region 10 Symposium (TENSYMP), Dhaka, Bangladesh, 5–7 June 2020; pp. 316–319. [Google Scholar]
- Gao, Z.; Wu, J.; Zhou, J.; Jiang, W.; Feng, L. Design of ECG Signal Acquisition and Processing System. In 2012 International Conference on Biomedical Engineering and Biotechnology; IEEE Computer Society: Washington, DC, USA, 2012; pp. 762–764. [Google Scholar]
- Klum, M.; Urban, M.; Tigges, T.; Pielmus, A.-G.; Feldheiser, A.; Schmitt, T.; Orglmeister, R. Wearable cardiorespiratory monitoring employing a multimodal digital patch stethoscope: Estimation of ECG, pep, lvetand respiration using a 55 mm single-lead ECG and phonocardiogram. Sensors 2020, 20, 2033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, L.; Yuan, Y.; Zhou, Z.; Bai, Y.; Wu, S. A Fetal ECG Monitoring System Based on the Android Smartphone. Sensors 2019, 19, 446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.-H.; Zhang, W.; Guan, M.-H.; Jiang, S.-Y.; Fan, M.-H.; Abu, P.A.R.; Chen, C.-A.; Chen, S.-L. A Low-Power High-Data-Transmission Multi ECG Acquisition Sensor System. Sensors 2019, 19, 4996. [Google Scholar] [CrossRef] [Green Version]
- Abtahi, F.; Snäll, J.; Aslamy, B.; Abtahi, S.; Seoane, F.; Lindecrantz, K. Biosignal PI, an Affordable Open-Source ECG and Respiration Measurement System. Sensors 2015, 15, 93–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozkan, H.; Ozhan, O.; Karadana, Y.; Gulcu, M.; Macit, S.; Husain, F. A Portable Wearable Tele-ECG Monitoring System. IEEE Trans. Instrum. Meas. 2019, 69, 173–182. [Google Scholar] [CrossRef]
- Pineda-López, F.; Martínez-Fernández, A.; Rojo-Álvarez, J.L.; García-Alberola, A.; Blanco-Velasco, M. A flexible 12-lead/Holter device with compression capabilities for low-bandwidth mobile-ECG telemedicine applications. Sensors 2018, 18, 3773. [Google Scholar] [CrossRef] [Green Version]
- Boehm, A.; Yu, X.; Neu, W.; Leonhardt, S.; Teichmann, D. A Novel 12-Lead ECG T-Shirt with Active Electrodes. Electronics 2016, 5, 75. [Google Scholar] [CrossRef] [Green Version]
- Uktveris, T.; Jusas, V. Development of a Modular Board for EEG Signal Acquisition. Sensors 2018, 18, 2140. [Google Scholar] [CrossRef] [Green Version]
- Medtronic, Cardiac Monitors. Available online: https://www.medtronic.com/us-en/healthcare-professionals/products/cardiac-rhythm/cardiac-monitors.html (accessed on 25 January 2021).
- ZioXT by iRhythm. Available online: https://www.irhythmtech.com/products-services/zio-xt (accessed on 25 January 2022).
- Wearable Biosensor by Philips. Available online: https://www.usa.philips.com/healthcare/product/HC989803196871/wearable-biosensor-wireless-remote-sensing-device (accessed on 25 January 2021).
- Savvy ECG–Savvy. Available online: http://www.savvy.si/en/Savvy_1/ (accessed on 25 January 2022).
- ePatch–BioTelemetry, Inc. Available online: https://www.gobio.com/epatch (accessed on 25 January 2022).
- QardioCore Wearable ECG EKG Monitor. Available online: https://www.getqardio.com/en/qardiocore-wearable-ecg-ekg-monitor-iphone (accessed on 25 January 2022).
- Chen, C.-L.; Chuang, C.-T. A QRS Detection and R Point Recognition Method for Wearable Single-Lead ECG. Sensors 2017, 17, 1969. [Google Scholar] [CrossRef] [Green Version]
- Townsend, K.; Cufí, C.; Davidson, R. Getting Started with Bluetooth Low Energy: Tools and Techniques for Low-Power Networking; O′Reilly Media, Inc.: Newton, MA, USA, 2014; Chapter 4. [Google Scholar]
- Heart Rate Profile 1.0–Bluetooth® Technology. Available online: https://www.bluetooth.com/specifications/specs/heart-rate-profile-1-0 (accessed on 25 January 2021).
- Bluetooth® Low Energy-Specifications. Available online: https://www.bluetooth.com/specifications/ (accessed on 25 January 2022).
- Bluetooth® Low Energy-Profiles. Available online: https://www.bluetooth.com/specifications/gatt (accessed on 25 January 2022).
- Yiadom, M.Y.A.B.; Baugh, C.W.; McWade, C.M.; Liu, X.; Song, K.J.; Patterson, B.W.; Jenkins, C.A.; Tanski, M.; Mills, A.M.; Salazar, G.; et al. Performance of Emergency Department Screening Criteria for an Early ECG to Identify ST-Segment Elevation Myocardial Infarction. J. Am. Heart Assoc. 2017, 6, e003528. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Wagner, P.; Strodthoff, N.; Bousseljot, R.-D.; Kreiseler, D.; Lunze, F.I.; Samek, W.; Schaeffter, T. PTB-XL, a large publicly available electrocardiography dataset. Sci. Data 2020, 7, 154. [Google Scholar] [CrossRef] [PubMed]
- Saenz-Cogollo, J.F.; Agelli, M. Investigating Feature Selection and Random Forests for Inter-Patient Heartbeat Classification. Algorithms 2020, 13, 75. [Google Scholar] [CrossRef] [Green Version]
- LE Data Length Extension. Available online: http://software-dl.ti.com/lprf/simplelink_cc2640r2_sdk/1.35.00.33/exports/docs/ble5stack/ble_user_guide/html/ble-stack/data-length-extensions.html (accessed on 25 January 2022).
- HE Instruments|Patient Simulators. Available online: https://www.heinstruments.com (accessed on 25 January 2022).
- Bluetooth Low Energy–Advertising. Available online: https://www.bluetooth.com/blog/bluetooth-low-energy-it-starts-with-advertising/ (accessed on 25 January 2022).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Handle | Type | Type | Hex/Text Value (Default) | GATT Server Permissions | Notes |
|---|---|---|---|---|---|
| 0x10 | 0x2800 | GATT_PRIMARY_ SERVICE_UUID | 0 xBA55 (ECG_SERV_UUID) | GATT_PERMIT_READ | Start of ECG Profile Service |
| 0x11 | 0x2803 | ECG_PROFILE_ CHARACTER1_UUID | 12 00 (handle: 0x0012) | GATT_ PERMIT_READ | Characteristic1 declaration |
| AD 2B (UUID: 0x2BAD) | |||||
| 0x12 | 0x2BAD | FULL_ECG_12LEAD_UUID | 00:00:00:00:00:00:00:00:00:00:00:00 (224 bytes) | GATT_PERMIT_READ|GATT_PERMIT_ NOTIFY | ECG data value |
| 0x13 | 0x2902 | GATT_CLIENT_CHAR_CFG_UUID | 00:00 (2 bytes) | GATT_PERMIT_READ | GATT_ PERMIT_WRITE | BLE characteristic notifications enable/disable |
| 0x14 | 0x2901 | GATT_CHAR_USER_ DESC_UUID | “ECG Data Stream” (15 bytes) | GATT_PERMIT_READ | Characteristic1 user description |
| 0x15 | 0x2803 | ECG_PROFILE_ CHARACTER2_UUID | 16 00 (handle: 0x0016) | GATT_ PERMIT_READ | Characteristic2 declaration |
| AD 3B (UUID: 0x3BAD) | |||||
| 0x16 | 0x3BAD | ECG_NUM_CHANS | 0x08 (1 byte) | GATT_PERMIT_READ | Number of ECG Channels |
| 0x17 | 0x2901 | GATT_CHAR_USER_ DESC_UUID | “Number of ECG Channels” (22 bytes) | GATT_PERMIT_READ | Characteristic2 user description |
| 0x18 | 0x2803 | ECG_PROFILE_ CHARACTER3_UUID | 19 00 (handle: 0x0019) | GATT_ PERMIT_READ | Characteristic3 declaration |
| CD 2B (UUID: 0x2BCD) | |||||
| 0x19 | 0x2BCD | ECG_STREAM_FLAG_ COMMAND | 0x00 (1 byte) | GATT_PERMIT_READ|GATT_ PERMIT_WRITE | “01:00” to enable/”00:00” to disable |
| 0x1A | 0x2901 | GATT_CHAR_USER_ DESC_UUID | “Stream Flag Status” (18 bytes) | GATT_PERMIT_READ | Characteristic3 user description |
| Sampling Rate Time Interval | 250 SPS (Low-Power) | 500 SPS (High-Resolution) |
|---|---|---|
| 1 s | 6.75 Kilobyte (KB) | 13.5 KB |
| 1 min | 405 KB | 810 KB |
| 1 h | 24.3 Megabyte (MB) | 48.6 MB |
| 24 h | 583.2 MB | 1.1664 Gigabyte (GB) |
| Analog Input | Derived Lead | Polarity | Digitally Generated Leads |
|---|---|---|---|
| Channel 1 | V6 = V6 − WCT | Unipolar | Lead III = Lead II − Lead I |
| Channel 2 | Lead I = LA (1) – RA (2) | Bipolar | aVF = (Lead II + Lead III)/2 |
| Channel 3 | Lead II = LL (3) − RA | Bipolar | -aVR = (Lead I + Lead II)/2 |
| Channel 4 | V2 = V2 − WCT (*) | Unipolar | aVL = (Lead I − Lead III)/2 |
| Channel 5 | V3 = V3 − WCT (*) | Unipolar | |
| Channel 6 | V4 = V4 − WCT (*) | Unipolar | |
| Channel 7 | V5 = V5 − WCT (*) | Unipolar | |
| Channel 8 | V1 = V1 − WCT (*) | Unipolar |
| Operation Mode | Number of Channels | Number of ECG Leads | # Samples/ BLE Packet | Payload/ BLE Packet | Acquisition Rate |
|---|---|---|---|---|---|
| Offline | 8 | 12 | N/A | N/A | 480 SPS |
| Disconnected Mode | 8 | 12 | N/A | N/A | 370 SPS |
| Continuous Mode | 8 | 12 | 7 | 8 (CH) × 4 (Bytes) × 7 (Samples) = 224 Bytes | 343 SPS |
| Triggered Mode-1 | 1 | 1 (i.e., Lead II) | 56 | 1 × 4 × 56 = 224 Bytes | 441 SPS |
| Triggered Mode-2 | 2 | 3 (i.e., Leads I, II, and aVF) | 28 | 3 × 4 × 28 = 224 Bytes | 441 SPS |
| Rank | Feature | Definition |
|---|---|---|
| 1 | RR0/avgRR | The current R-R interval divided by the average of the last 32 beats |
| 2 | RR+1/RR0 | The next R-R interval divided by the current R-R interval |
| 3 | RR-1/RR0 | The previous R-R interval divided by the current R-R interval |
| 4 | RR+1/avgRR | The next R-R interval divided by the average of the last 32 beats |
| 5 | hbf_3 | The coefficients of fitting Hermite basis functions with polynomials degree = 3 |
| RF | SVM | KNN | LR | DT | Extra Trees | |
|---|---|---|---|---|---|---|
| Accuracy | 95.20% | 94.19% | 94.05% | 93.60% | 91.56% | 95.30% |
| Processing Time | 44.54 s | 89.13 s | 1.84 s | 0.857 s | 3.98 s | 5.78 s |
| RF | SVM | KNN | LR | DT | Extra Trees | ||
|---|---|---|---|---|---|---|---|
| N | Precision | 96.11% | 95.26% | 96.64% | 94.73% | 95.75% | 96.17% |
| Recall | 98.27% | 98.38% | 96.68% | 98.27% | 94.73% | 98.63% | |
| Fl-score | 97.19% | 96.79% | 96.66% | 96.47% | 95.23% | 97.38% | |
| ABN | Precision | 83.33% | 82.06% | 72.98% | 79.87% | 60.61% | 85.96% |
| Recall | 70.31% | 60.30% | 72.73% | 55.60% | 65.85% | 68.13% | |
| Fl-score | 76.27% | 69.51% | 72.86% | 65.56% | 63.12% | 77.03% |
| Power Consumption Results | Value |
|---|---|
| Mean, Min, and Max | 157.73 mW, 91.69 mW, and 364.133 mW |
| Average voltage | 3.3 V |
| Battery Capacity | 2000 mAh |
| Total Operation time | 1 Day, 13 h approximately |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badr, A.; Badawi, A.; Rashwan, A.; Elgazzar, K. XBeats: A Real-Time Electrocardiogram Monitoring and Analysis System. Signals 2022, 3, 189-208. https://doi.org/10.3390/signals3020013
Badr A, Badawi A, Rashwan A, Elgazzar K. XBeats: A Real-Time Electrocardiogram Monitoring and Analysis System. Signals. 2022; 3(2):189-208. https://doi.org/10.3390/signals3020013
Chicago/Turabian StyleBadr, Ahmed, Abeer Badawi, Abdulmonem Rashwan, and Khalid Elgazzar. 2022. "XBeats: A Real-Time Electrocardiogram Monitoring and Analysis System" Signals 3, no. 2: 189-208. https://doi.org/10.3390/signals3020013
APA StyleBadr, A., Badawi, A., Rashwan, A., & Elgazzar, K. (2022). XBeats: A Real-Time Electrocardiogram Monitoring and Analysis System. Signals, 3(2), 189-208. https://doi.org/10.3390/signals3020013