

Paroxysmal Nocturnal Hemoglobinuria: A Case Report in a Pandemic Environment

 , and
, and
Abstract
:1. Introduction
2. Detailed Case Description
3. Discussion
4. Conclusions
Patient Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parker, C.; Omine, M.; Richards, S.; Nishimura, J.-I.; Bessler, M.; Ware, R.; Hillmen, P.; Luzzatto, L.; Young, N.; Kinoshita, T.; et al. Diagnosis and management of paroxysmal nocturnal hemoglobinuria. Blood 2005, 106, 3699–3709. [Google Scholar] [CrossRef] [PubMed]
- Takeda, J.; Miyata, T.; Kawagoe, K.; Iida, Y.; Endo, Y.; Fujita, T.; Takahashi, M.; Kitani, T.; Kinoshita, T. Deficiency of the GPI anchor caused by a somatic mutation of the PIG-A gene in paroxysmal nocturnal hemoglobinuria. Cell 1993, 73, 703–711. [Google Scholar] [CrossRef] [PubMed]
- de Latour, R.P.; Mary, J.Y.; Salanoubat, C.; Terriou, L.; Etienne, G.; Mohty, M.; Roth, S.; de Guibert, S.; Maury, S.; Cahn, J.Y.; et al. Paroxysmal nocturnal hemoglobinuria: Natural history of disease subcategories. Blood 2008, 112, 3099–3106. [Google Scholar] [CrossRef] [PubMed]
- Yenerel, M.N.; Muus, P.; Wilson, A.; Szer, J. Clinical course and disease burden in patients with paroxysmal nocturnal hemoglobinuria by hemolytic status. Blood Cells Mol. Dis. 2017, 65, 29–34. [Google Scholar] [CrossRef]
- Brodsky, R.A. How do PIG-A mutant paroxysmal nocturnal hemoglobinuria stem cells achieve clonal dominance? Expert Rev. Hematol. 2009, 2, 353–356. [Google Scholar] [CrossRef]
- Ploug, M.; Plesner, T.; Ronne, E.; Ellis, V.; Hoyer-Hansen, G.; Hansen, N.E.; Dano, K. The receptor for urokinase-type plasminogen activator is deficient on peripheral blood leukocytes in patients with paroxysmal nocturnal hemoglobinuria. Blood 1992, 79, 1447–1455. [Google Scholar] [CrossRef]
- Hill, A.; Kelly, R.J.; Hillmen, P. Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood 2013, 121, 4985–4996. [Google Scholar] [CrossRef]
- Wiedmer, T.; Hall, S.E.; Ortel, T.L.; Kane, W.H.; Rosse, W.F.; Sims, P.J. Complement-induced vesiculation and exposure of membrane prothrombinase sites in platelets of paroxysmal nocturnal hemoglobinuria. Blood 1993, 82, 1192–1196. [Google Scholar] [CrossRef]
- Ziakas, P.D.; Poulou, L.S.; Rokas, G.I.; Bartzoudis, D.; Voulgarelis, M. Thrombosis in paroxysmal nocturnal hemoglobinuria: Sites, risks, outcome. An overview. J. Thromb. Haemost. 2007, 5, 642–645. [Google Scholar] [CrossRef]
- VAN Bijnen, S.T.A.; VAN Heerde, W.L.; Muus, P. Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria. J. Thromb. Haemost. 2012, 10, 1–10. [Google Scholar] [CrossRef]
- Hillmen, P.; Hall, C.; Marsh, J.C.; Elebute, M.; Bombara, M.P.; Petro, B.E.; Cullen, M.J.; Richards, S.J.; Rollins, S.A.; Mojcik, C.F.; et al. Effect of eculizumab on hemolysis and transfusion requirements in patients with paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 2004, 350, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Gralinski, L.E.; Sheahan, T.P.; Morrison, T.E.; Menachery, V.D.; Jensen, K.; Leist, S.R.; Whitmore, A.; Heise, M.T.; Baric, R.S. Complement Activation Contributes to Severe Acute Respiratory Syndrome Coronavirus Pathogenesis. mBio 2018, 9, e01753-18. [Google Scholar] [CrossRef] [PubMed]
- Annane, D.; Heming, N.; Grimaldi-Bensouda, L.; Frémeaux-Bacchi, V.; Vigan, M.; Roux, A.-L.; Marchal, A.; Michelon, H.; Rottman, M.; Moine, P. Eculizumab as an emergency treatment for adult patients with severe COVID-19 in the intensive care unit: A proof-of-concept study. eClinicalMedicine 2020, 28, 100590. [Google Scholar] [CrossRef]
- I Rafailidis, P.; Mourtzoukou, E.G.; Varbobitis, I.C.; E Falagas, M. Severe cytomegalovirus infection in apparently immunocompetent patients: A systematic review. Virol. J. 2008, 5, 47. [Google Scholar] [CrossRef]
- Taglietti, F.; Drapeau, C.M.; Grilli, E.; Capone, A.; Noto, P.; Topino, S.; Petrosillo, N. Hemolytic anemia due to acute cytomegalovirus infection in an immunocompetent adult: A case report and review of the literature. J. Med. Case Rep. 2010, 4, 334. [Google Scholar] [CrossRef]
- Leclercq, P.; Micoud, M.; Gavazzi, G.; Morand, P.; Bosseray, A.; Bouchard, O. Association between Primary Cytomegalovirus Infection and Severe Hemolytic Anemia in an Immunocompetent Adult. Eur. J. Clin. Microbiol. Infect. Dis. 1999, 18, 299–301. [Google Scholar] [CrossRef]
- Van Spronsen, D.J.; Breed, W.P.M. Cytomegalovirus-induced thrombocytopenia and haemolysis in an immunocompetent adult. Br. J. Haematol. 1996, 92, 218–220. [Google Scholar] [CrossRef]
- VMoyo, V.M.; Mukhina, G.L.; Garrett, E.S.; Brodsky, R.A. Natural history of paroxysmal nocturnal haemoglobinuria using modern diagnostic assays. Br. J. Haematol. 2004, 126, 133–138. [Google Scholar] [CrossRef]
- Loschi, M.; Porcher, R.; Barraco, F.; Terriou, L.; Mohty, M.; de Guibert, S.; Mahe, B.; Lemal, R.; Dumas, P.-Y.; Etienne, G.; et al. Impact of eculizumab treatment on paroxysmal nocturnal hemoglobinuria: A treatment versus no-treatment study. Am. J. Hematol. 2016, 91, 366–370. [Google Scholar] [CrossRef]
- Hall, C.; Richards, S.; Hillmen, P. Primary prophylaxis with warfarin prevents thrombosis in paroxysmal nocturnal hemoglobinuria (PNH). Blood 2003, 102, 3587–3591. [Google Scholar] [CrossRef] [PubMed]
- Hillmen, P.; Muus, P.; Dührsen, U.; Risitano, A.M.; Schubert, J.; Luzzatto, L.; Schrezenmeier, H.; Szer, J.; Brodsky, R.A.; Hill, A.; et al. Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria. Blood 2007, 110, 4123–4128. [Google Scholar] [CrossRef]
- Brodsky, R.A. How I treat paroxysmal nocturnal hemoglobinuria. Blood 2021, 137, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
- Jarrah, K.; Al Mahmasani, L.; Atoui, A.; Bou-Fakhredin, R.; Taher, A.T. Manifestation of paroxysmal nocturnal hemoglobinuria after COVID-19 mRNA vaccination. Blood Cells Mol. Dis. 2022, 93, 102641. [Google Scholar] [CrossRef] [PubMed]
- Gerber, G.F.; Yuan, X.; Yu, J.; Cher, B.A.Y.; Braunstein, E.M.; Chaturvedi, S.; Brodsky, R.A. COVID-19 vaccines induce severe hemolysis in paroxysmal nocturnal hemoglobinuria. Blood 2021, 137, 3670–3673. [Google Scholar] [CrossRef]
- Green, H.; Eliakim-Raz, N.; Zimra, Y.; Gafter-Gvili, A. Paroxysmal nocturnal hemoglobinuria diagnosed after influenza vaccine: Coincidence or consequence? Isr. Med. Assoc. J. 2014, 16, 122–124. [Google Scholar]
- Nakayama, T. Causal relationship between immunological responses and adverse reactions following vaccination. Vaccine 2019, 37, 366–371. [Google Scholar] [CrossRef]
- Marshall, G.S.; Abbing-Karahagopian, V.; Marshall, H.S.; Cenci, S.; Conway, J.H.; Occhipinti, E.; Bekkat-Berkani, R.; Banzhoff, A.; Sohn, W.-Y. A comprehensive review of clinical and real-world safety data for the four-component serogroup B meningococcal vaccine (4CMenB). Expert Rev. Vaccines 2023, 22, 530–544. [Google Scholar] [CrossRef]
- Clyne, B.; Olshaker, J.S. The C-reactive protein. J. Emerg. Med. 1999, 17, 1019–1025. [Google Scholar] [CrossRef]
- Rüfer, A.; Wuillemin, W.A. Die Milz bei nicht-malignen hämatologischen Erkrankungen. Ther. Umsch. 2013, 70, 157–162. [Google Scholar] [CrossRef]
- Marietta, M.; Coluccio, V.; Luppi, M. Potential mechanisms of vaccine-induced thrombosis. Eur. J. Intern. Med. 2022, 105, 1–7. [Google Scholar] [CrossRef]
- Peerschke, E.I.; Yin, W.; Ghebrehiwet, B. Platelet Mediated Complement Activation. Curr. Top. Complement II 2008, 632, 77–87. [Google Scholar] [CrossRef]
- Gralnick, H.R.; Vail, M.; McKeown, L.P.; Merryman, P.; Wilson, O.; Chu, I.; Kimball, J. Activated platelets in paroxysmal nocturnal haemoglobinuria. Br. J. Haematol. 1995, 91, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Rawish, E.; Sauter, M.; Sauter, R.; Nording, H.; Langer, H.F. Complement, inflammation and thrombosis. Br. J. Pharmacol. 2021, 178, 2892–2904. [Google Scholar] [CrossRef] [PubMed]
- Emadi, A.; Brodsky, R.A. Successful discontinuation of anticoagulation following eculizumab administration in paroxysmal nocturnal hemoglobinuria. Am. J. Hematol. 2009, 84, 699–701. [Google Scholar] [CrossRef]
- Risitano, A.M.; Notaro, R.; Marando, L.; Serio, B.; Ranaldi, D.; Seneca, E.; Ricci, P.; Alfinito, F.; Camera, A.; Gianfaldoni, G.; et al. Complement fraction 3 binding on erythrocytes as additional mechanism of disease in paroxysmal nocturnal hemoglobinuria patients treated by eculizumab. Blood 2009, 113, 4094–4100. [Google Scholar] [CrossRef]
- Szlendak, U.; Budziszewska, B.; Spychalska, J.; Drozd-Sokołowska, J.; Patkowska, E.; Nowak, J. Paroxysmal nocturnal hemoglobinuria: Advances in the understanding of pathophysiology, diagnosis, and treatment. Pol. Arch. Intern. Med. 2022, 132, 16271. [Google Scholar] [CrossRef]
- Magro, G. COVID-19: Review on latest available drugs and therapies against SARS-CoV-2. Coagulation and inflammation cross-talking. Virus Res. 2020, 286, 198070. [Google Scholar] [CrossRef]
- Laurence, J.; Mulvey, J.J.; Seshadri, M.; Racanelli, A.; Harp, J.; Schenck, E.J.; Zappetti, D.; Horn, E.M.; Magro, C.M. Anti-complement C5 therapy with eculizumab in three cases of critical COVID-19. Clin. Immunol. 2020, 219, 108555. [Google Scholar] [CrossRef]
- Diurno, F.; Numis, F.G.; Porta, G.; Cirillo, F.; Maddaluno, S.; Ragozzino, A.; De Negri, P.; Di Gennaro, C.; Pagano, A.; Allegorico, E.; et al. Eculizumab treatment in patients with COVID-19: Preliminary results from real life ASL Napoli 2 Nord experience. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4040–4047. [Google Scholar] [CrossRef]
- Mastellos, D.C.; da Silva, B.G.P.; Fonseca, B.A.; Fonseca, N.P.; Auxiliadora-Martins, M.; Mastaglio, S.; Ruggeri, A.; Sironi, M.; Radermacher, P.; Chrysanthopoulou, A.; et al. Complement C3 vs C5 inhibition in severe COVID-19: Early clinical findings reveal differential biological efficacy. Clin. Immunol. 2020, 220, 108598. [Google Scholar] [CrossRef] [PubMed]
- Shibabaw, T.; Molla, M.D.; Teferi, B.; Ayelign, B. Role of IFN and Complements System: Innate Immunity in SARS-CoV-2. J. Inflamm. Res. 2020, 13, 507–518. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
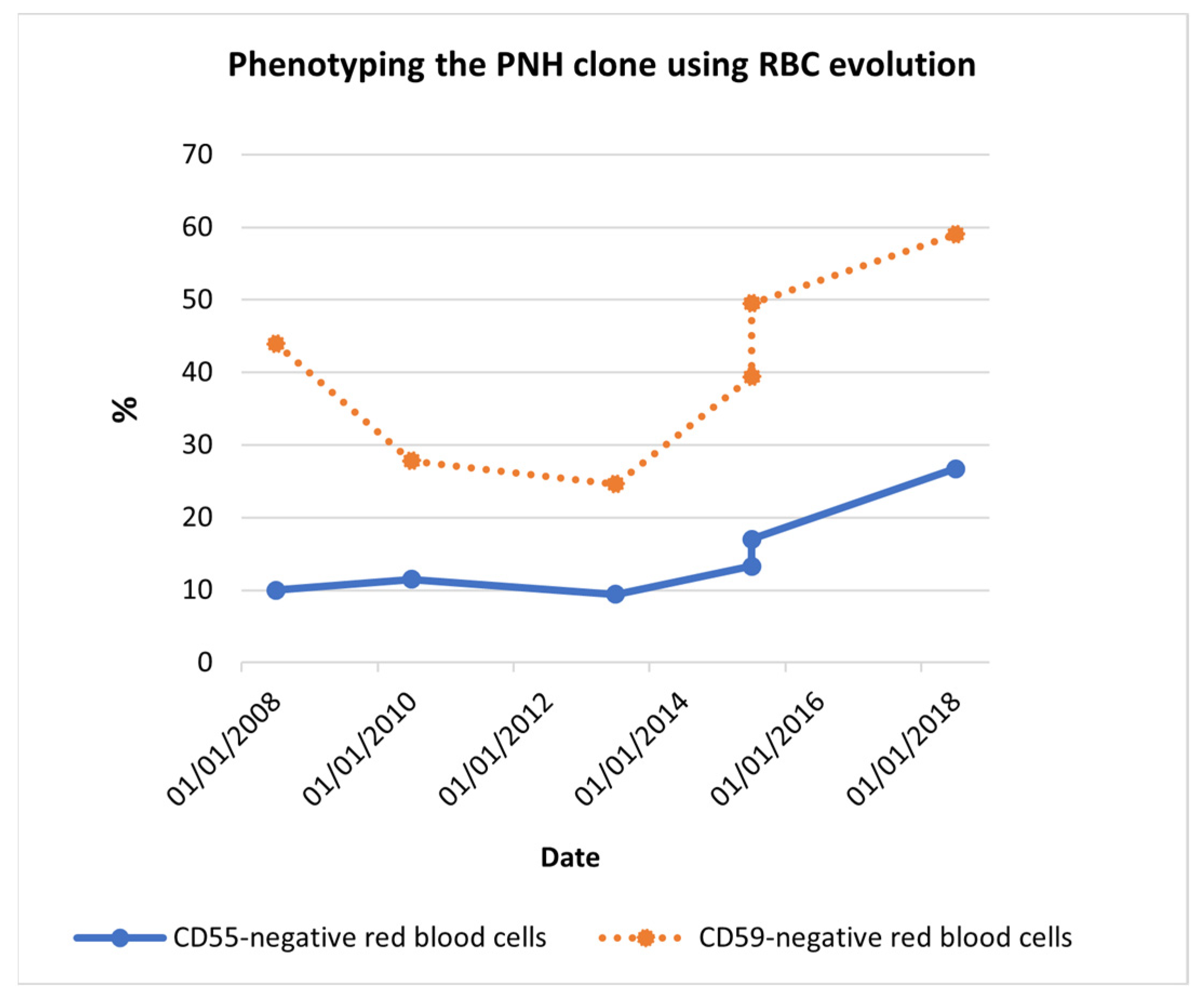
| Date | % CD55− RBCs | % CD59− RBCs |
|---|---|---|
| 17 July 2008 | 10.0 | 44.0 |
| 30 April 2010 | 11.5 | 27.8 |
| 9 May 2013 | 9.4 | 24.6 |
| 22 April 2015 | 13.3 | 39.4 |
| 29 September 2015 | 17.0 | 49.5 |
| 5 September 2018 | 26.7 | 59.0 |
| Date | Hb (g/dL) | Leucocytes (109/L) | Platelets (109/L) | LDH (U/L) | CRP (mg/L) |
|---|---|---|---|---|---|
| 31 May 2017 | 8.1 | 3.14 | 121 | 1870 | 8.1 |
| 26 December 2018 | 7.8 | 3.38 | 131 | 1674 | 16.0 |
| 20 February 2019 | 8.8 | 3.98 | 107 | 1826 | 48.9 |
| 30 March 2019 | 8.5 | 2.84 | 119 | 2301 | 13.3 |
| 8 May 2019 | 6.8 | 2.65 | 113 | 2091 | 8.3 |
| Date | Vaccine Administration |
|---|---|
| 1st phase | |
| 24 May 2019 | Prevenar® and Hiberix® |
| 11 June 2019 | Nimenrix® (1st dose) and Bexsero® (1st dose) |
| 2nd phase | |
| 10 December 2019 | Bexsero® (2nd dose) |
| 23 January 2020 | Pneumovax® |
| 2 March 2020 | Nimenrix® (2nd dose) |
| Date | Hb (g/dL) | Leucocytes (109/L) | Platelets (109/L) | LDH (U/L) | CRP (mg/L) |
|---|---|---|---|---|---|
| (a) After 1st phase vaccination | |||||
| 26 June 2019 | 5.8 | 3.32 | 113 | 1343 | 72.9 |
| 3 July 2019 | 7.3 | 3.31 | 104 | 1847 | 63.6 |
| (b) After anticoagulant therapy | |||||
| 9 October 2019 | 8.7 | 4.08 | 82 | 2324 | 71.8 |
| (c) After eculizumab initiation | |||||
| 29 October 2019 | 8.0 | 3.27 | 99 | 1123 | 11.6 |
| 13 November 2019 | 9.3 | 3.23 | 107 | 532 | 5.8 |
| 20 November 2019 | 9.2 | 3.18 | 99 | 486 | 11.2 |
| 3 December 2019 | 8.6 | 5.10 | 89 | 401 | 22.9 |
| (d) After Bexsero® (2nd dose) | |||||
| 17 December 2019 | 6.8 | 5.28 | 98 | 568 | 76.1 |
| (e) After the recovery of the vaccination outcome | |||||
| 26 December 2019 | 10.2 | 3.19 | 124 | 428 | 7.6 |
| 15 January 2020 | 10.6 | 4.29 | 109 | 441 | 4.8 |
| 20 May 2020 | 10.2 | 3.18 | 89 | 405 | 7.4 |
| 18 June 2020 | 10.3 | 2.58 | 90 | 328 | 6.5 |
| 11 November 2021 | 10.1 | 2.91 | 104 | 394 | 6.5 |
| 22 April 2022 | 9.9 | 3.01 | 108 | 360 | 6.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peixoto, V.; Carneiro, A.; Trigo, F.; Vieira, M.; Prudêncio, C. Paroxysmal Nocturnal Hemoglobinuria: A Case Report in a Pandemic Environment. Reports 2023, 6, 42. https://doi.org/10.3390/reports6030042
Peixoto V, Carneiro A, Trigo F, Vieira M, Prudêncio C. Paroxysmal Nocturnal Hemoglobinuria: A Case Report in a Pandemic Environment. Reports. 2023; 6(3):42. https://doi.org/10.3390/reports6030042
Chicago/Turabian StylePeixoto, Vanda, Ana Carneiro, Fernanda Trigo, Mónica Vieira, and Cristina Prudêncio. 2023. "Paroxysmal Nocturnal Hemoglobinuria: A Case Report in a Pandemic Environment" Reports 6, no. 3: 42. https://doi.org/10.3390/reports6030042
APA StylePeixoto, V., Carneiro, A., Trigo, F., Vieira, M., & Prudêncio, C. (2023). Paroxysmal Nocturnal Hemoglobinuria: A Case Report in a Pandemic Environment. Reports, 6(3), 42. https://doi.org/10.3390/reports6030042