
Clinical and Parasitological Profiles of Gestational, Placental and Congenital Malaria in Northwestern Colombia

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
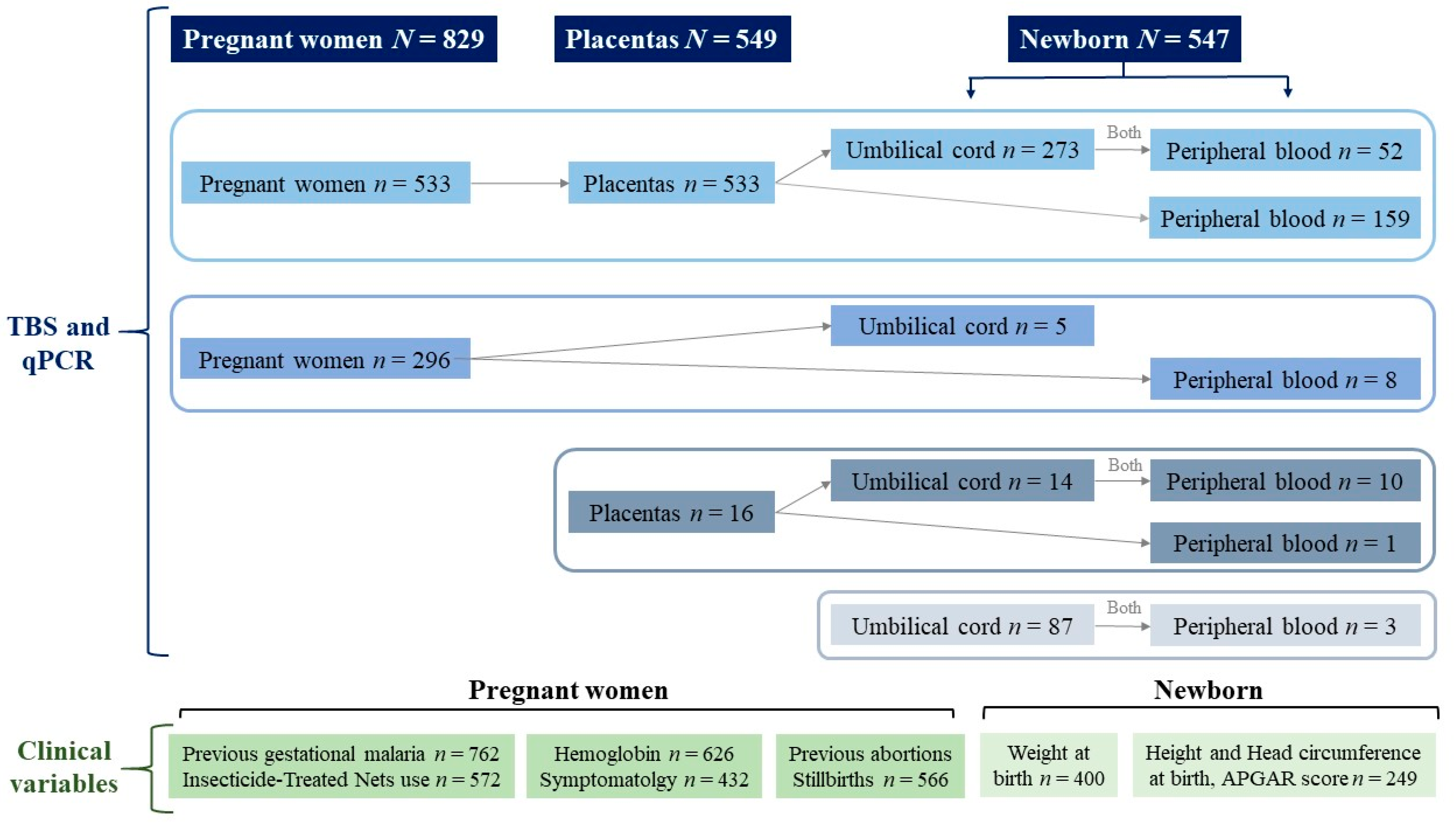
2.1. Type and Subjects of Study
2.2. Diagnosis of Malaria Infection
2.3. Source of Clinical Information
2.4. Statistical Analysis
2.5. Ethic
3. Results
4. Discussion
Limitations and Strengths of This Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2022. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 (accessed on 15 January 2023).
- Agenjo González, M. Malaria and Pregnancy: Complications, Prevention and Treatment; Elsevier: Amsterdam, The Netherlands, 2014; Volume 57, pp. 468–471. Available online: https://www.elsevier.es/es-revista-progresos-obstetricia-ginecologia-151 (accessed on 15 January 2023).
- Liu, Y.; Griffin, J.B.; Muehlenbachs, A.; Rogerson, S.J.; Bailis, A.J.; Sharma, R.; Sullivan, D.J.; Tshefu, A.K.; Landis, S.H.; Kabongo, J.-M.M.; et al. Diagnosis of placental malaria in poorly fixed and processed placental tissue. Malar. J. 2016, 15, 272. [Google Scholar] [CrossRef] [PubMed]
- Agudelo-García, O.M.; Arango-Flórez, E.M.; Carona-Fonseca, J. Submicroscopic and asymptomatic congenital infection by Plasmodium vivax or P. falciparum in Colombia: 37 Cases with placental histopathology and cytokine profile in maternal and placental blood. J. Trop. Med. 2017, 2017, 3680758. [Google Scholar] [CrossRef] [PubMed]
- Menendez, C.; Mayor, A. Congenital malaria: The least known consequence of malaria in pregnancy. Semin. Fetal Neonatal. Med. 2007, 12, 207–213. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Malaria Policy Advisory Group—WHO. Meeting Report of the Evidence Review Group on Malaria in Pregnancy; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- CDC. Intermittent Preventive Treatment of Malaria for Pregnant Women (IPTp). 23 July 2018. Available online: https://www.cdc.gov/malaria/malaria_worldwide/reduction/iptp.html#:~:text=Malaria%20infection%20during%20pregnancy%20can,a%20risk%20factor%20for%20death (accessed on 15 January 2023).
- Cardona-Arias, J.A.; Carmona-Fonseca, J. Frequency of gestational malaria and maternal–neonatal outcomes, in Northwestern Colombia 2009–2020. Sci. Rep. 2022, 12, 10944. [Google Scholar] [CrossRef]
- Cardona-Arias, J.A.; Carmona-Fonseca, J. Frequency of placental malaria and its associated factors in northwestern Colombia, pooled analysis 2009–2020. PLoS ONE 2022, 17, e0268949. [Google Scholar] [CrossRef]
- Cardona-Arias, J.A.; Carmona-Fonseca, J. Congenital malaria: Frequency and epidemiology in Colombia, 2009–2020. PLoS ONE 2022, 17, e0263451. [Google Scholar] [CrossRef]
- Ministerio de Salud y Protección Social de Colombia. Guía de Práctica Clínica Diagnóstico y Tratamiento de la Malaria; Ministerio de Salud y Protección Social: Bogotá, Colombia, 2020; 117p. [Google Scholar]
- Lopez-Perez, M.; Pacheco, M.A.; Buriticá, L.; Escalante, A.A.; Herrera, S.; Arévalo-Herrera, M. Malaria in pregnancy: A passive surveillance study of pregnant women in low transmission areas of Colombia, Latin America. Malar. J. 2016, 15, 66. [Google Scholar] [CrossRef]
- Assabri, A.M.; Muharram, A.A. Malaria in pregnancy in Hodiedah, Republic of Yemen. East Mediterr. Health J. 2002, 8, 245–253. [Google Scholar] [CrossRef]
- Kwizera, A.; Ntasumumuyange, D.; Small, M.; Rulisa, S.; Moscovitz, A.N.; Magriples, U. Assessment of perinatal outcomes of pregnant women with severe versus simple malaria. PLoS ONE 2021, 16, e0247053. [Google Scholar] [CrossRef]
- Carmona-Fonseca, J. La Región “Urabá Antioqueño-Cuencas altas de los ríos Sinú y San Jorge-Bajo Cauca Antioqueño”: “Guarida” del paludismo colombiano Revista de la Universidad Industrial de Santander. Salud 2017, 49, 577–589. [Google Scholar]
- Zheng, Z.; Cheng, Z. Advances in Molecular Diagnosis of Malaria. Adv. Clin. Chem. 2017, 80, 155–192. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Salud de Colombia. Manual para el Diagnóstico de Malaria no Complicada en Puestos de Diagnóstico y Tratamiento; INS: Bogotá, Colombia, 2015; 74p. [Google Scholar]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; Technical Document; WHO: Geneva, Switzerland, 2011; Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1 (accessed on 30 January 2023).
- Cardona-Arias, J.A.; Carmona-Fonseca, J. Meta-analysis of the prevalence of malaria associated with pregnancy in Colombia 2000–2020. PLoS ONE 2021, 16, e0255028. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, G.; Moussiliou, A.; Luty, A.J.; Cot, M.; Fievet, N.; Massougbodji, A.; Deloron, P.; Tuikue Ndam, N. Submicroscopic Plasmodium falciparum infections are associated with maternal anemia, premature births, and low birth weight. Clin. Infect. Dis. 2015, 60, 1481–1488. [Google Scholar] [CrossRef]
- Alkan, M.L. The importance of submicroscopic diagnosis of malaria. Clin. Infect. Dis. 2020, 71, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Moxon, C.A.; Gibbins, M.P.; McGuinness, D.; Milner, D.A., Jr.; Marti, M. New Insights into Malaria Pathogenesis. Annu. Rev. Pathol. 2020, 15, 315–343. [Google Scholar] [CrossRef]
- Knudson, A.; Sánchez, R.; Pérez, M.; Cortés, L.; Guerra, A.; Nicholls, R. Perfil clínico y parasitológico de la malaria por Plasmodium falciparum y Plasmodium vivax no complicada en Córdoba, Colombia. Rev. Fac. Med. 2015, 63, 595–607. [Google Scholar] [CrossRef]
- Lin, J.T.; Saunders, D.L.; Meshnick, S.R. The role of submicroscopic parasitemia in malaria transmission: What is the evidence? Trends Parasitol. 2014, 3, 183–190. [Google Scholar] [CrossRef]
- Chen, I.; Clarke, S.E.; Gosling, R.; Hamainza, B.; Killeen, G.; Magill, A.; O’Meara, W.; Price, R.N.; Riley, E.M. “Asymptomatic” malaria: A chronic and debilitating ifection that should be treated. PLoS Med. 2016, 13, e1001942. [Google Scholar] [CrossRef]
- Oyegoke, O.O.; Maharaj, L.; Akoniyon, O.P.; Kwoji, I.; Roux, A.T.; Adewumi, T.S.; Maharaj, R.; Oyebola, B.T.; Adeleke, M.A.; Okpeku, M. Malaria diagnostic methods with the elimination goal in view. Parasitol. Res. 2022, 121, 1867–1885. [Google Scholar] [CrossRef]
- Rantala, A.M.; Taylor, S.M.; Trottman, P.A.; Luntamo, M.; Mbewe, B.; Maleta, K.; Kulmala, T.; Ashorn, P.; Meshnick, S.R. Comparison of real-time PCR and microscopy for malaria parasite detection in Malawian pregnant women. Malar. J. 2010, 9, 269. [Google Scholar] [CrossRef]
- Dayananda, K.K.; Achur, R.N.; Gowda, D.C. Epidemiology, drug resistance, and pathophysiology of Plasmodium vivax malaria. J. Vector Borne Dis. 2018, 55, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Briggs, J.; Ategeka, J.; Kajubi, R.; Ochieng, T.; Kakuru, A.; Ssemanda, C.; Wasswa, R.; Jagannathan, P.; Greenhouse, B.; Rodriguez-Barraquer, I.; et al. Impact of microscopic and submicroscopic parasitemia during pregnancy on placental malaria in a high-transmission setting in Uganda. J. Infect. Dis. 2019, 220, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Zakama, A.K.; Ozarslan, N.; Gaw, S.L. Placental Malaria. Curr. Trop. Med. Rep. 2020, 7, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Otuli Noël, L.; Nguma Jean-Didier, B.; Alongo Mike-Antoine, M.; Bosunga Gedeon, K.; Mukonkole Jean-Paulin, M.; Likwela Joris, L.; Okenge Jean-Pascal, M. Prevalence of Congenital Malaria in Kisangani, A Stable Malaria Transmission Area in Democratic Republic of the Congo. Infect. Dis. Obstet. Gynecol. 2020, 2020, 2176140. [Google Scholar] [CrossRef]
- Fitri, L.E.; Jahja, N.E.; Huwae, I.R.; Nara, M.B.; Berens-Riha, N. Congenital malaria in newborns selected for low birth-weight, anemia, and other possible symptoms in Maumere, Indonesia. Korean J. Parasitol. 2014, 52, 639–644. [Google Scholar] [CrossRef]
- Meuris, S.; Piko, B.B.; Eerens, P.; Vanbellinghen, A.M.; Dramaix, M.; Hennart, P. Gestational malaria: Assessment of its consequences on fetal growth. Am. J. Trop. Med. Hyg. 1993, 48, 603–609. [Google Scholar] [CrossRef]
- Walther, B.; Miles, D.J.; Waight, P.; Palmero, M.S.; Ojuola, O.; Touray, E.S.; Whittle, H.; van der Sande, M.; Crozier, S.; Flanagan, K.L. Placental malaria is associated with attenuated CD4 T-cell responses to tuberculin PPD 12 months after BCG vaccination. BMC Infect. Dis. 2012, 12, 6. [Google Scholar] [CrossRef]
- Dombrowski, J.G.; Souza, R.M.; Lima, F.A.; Bandeira, C.L.; Murillo, O.; Costa, D.S.; Peixoto, E.P.M.; Cunha, M.D.P.; Zanotto, P.M.A.; Bevilacqua, E.; et al. Association of Malaria Infection During Pregnancy With Head Circumference of Newborns in the Brazilian Amazon. JAMA Netw. Open 2019, 2, e193300. [Google Scholar] [CrossRef]
- Koladjo, B.F.; Yovo, E.; Accrombessi, M.; Agbota, G.; Atade, W.; Ladikpo, O.T.; Mehoba, M.; Degbe, A.; Jackson, N.; Massougbodji, A.; et al. Malaria in the First Trimester of Pregnancy and Fetal Growth: Results from a Beninese Preconceptional Cohort. J. Infect. Dis. 2022, 225, 1777–1785. [Google Scholar] [CrossRef]


{kind=link}
| Plasmodial Infection According to qPCR and Thick Blood Smear | ||||
|---|---|---|---|---|
| Gestational | Placental | Congenital | ||
| Cord | Newborn | |||
| The number of samples | 829 | 549 | 379 | 233 |
| Positive for Plasmodium % (n) | 35.8 (297/829) | 20.9 (115/549) | 12.4 (47/379) | 2.2 (5/233) |
| Submicroscopic (positive PCR and negative TBS) | ||||
| % (n) of total | 16.2 (134/829) | 19.9 (109/549) | 12.4 (47/379) | 2.2 (5/233) |
| % (n) of positives | 45.1 (134/297) | 94.8 (109/115) | 100 (47/47) | 100 (5/5) |
| P. vivax | ||||
| % (n) of total | 22.6 (187/829) | 9.3 (51/549) | 3.4 (13/379) | 1.3 (3/233) |
| % (n) of positives | 63.0 (187/297) | 44.3 (51/115) | 27.7 (13/47) | 60.0 (3/5) |
| P. falciparum | ||||
| % (n) of total | 12.3 (102/829) | 9.3 (51/549) | 8.2 (31/379) | 0.9 (2/233) |
| % (n) of positives | 34.3 (102/297) | 44.3 (51/115) | 65.9 (31/47) | 40.0 (2/5) |
| Mixed-malaria | ||||
| % (n) of total | 1.0 (8/829) | 2.4 (13/549) | 0.8 (3/379) | 0 |
| % (n) of positives | 2.7 (8/297) | 11.3 (13/115) | 6.4 (3/47) | 0 |
| Total N = 432 % (n) | Gestational Malaria | p Chi2 | Causal Species | ||||
|---|---|---|---|---|---|---|---|
| Negative N = 312 | Positive N = 120 | P. falciparum N = 24 | P. vivax N = 94 | p Chi2 | |||
| % (n) a | % (n) a | % (n) a | % (n) a | ||||
| Headache | 48.6 (210) | 39.1 (122) | 73.3 (88) | <0.001 | 50.0 (12) | 80.9 (76) | <0.001 b |
| Fever | 23.8 (103) | 10.3 (32) | 59.2 (71) | <0.001 | 8.3 (2) | 73.4 (69) | <0.001 b |
| Musculoskeletal ain | 13.0 (56) | 6.7 (21) | 29.2 (35) | <0.001 | 4.2 (1) | 36.2 (34) | <0.001 b |
| Shaking chills | 10.9 (47) | 7.4 (23) | 20.0 (24) | <0.001 | 4.2 (1) | 24.5 (23) | <0.001 b |
| Vomiting | 10.9 (47) | 8.0 (25) | 18.3 (22) | 0.002 | 0.0 (0) | 23.4 (22) | <0.001 b |
| Abdominal pain | 7.4 (32) | 5.8 (18) | 11.7 (14) | 0.036 | 4.2 (1) | 13.8 (13) | 0.060 |
| Cough | 4.9 (21) | 3.2 (10) | 9.2 (11) | 0.010 | 16.7 (4) | 7.4 (7) | 0.014 |
| Sweating | 5.3 (23) | 0.3 (1) | 18.3 (22) | <0.001 | 0.0 (0) | 23.4 (22) | <0.001 b |
| Diarrhea | 4.4 (19) | 4.8 (15) | 3.3 (4) | 0.503 | 0.0 (0) | 4.3 (4) | 0.723 |
| Asthenia–Adynamia | 4.6 (20) | 0.0 (0) | 16.7 (20) | <0.001 | 0.0 (0) | 21.3 (20) | <0.001 b |
| Coluria | 3.9 (17) | 2.2 (7) | 8.3 (10) | 0.004 | 4.2 (1) | 9.6 (9) | 0.016 b |
| Loss of appetite | 4.2 (18) | 0.0 (0) | 15.0 (18) | <0.001 | 0.0 (0) | 19.1 (18) | <0.001 b |
| Nausea | 3.2 (14) | 0.0 (0) | 11.7 (14) | <0.001 | 0.0 (0) | 14.9 (14) | <0.001 b |
| Sore throat | 2.3 (10) | 0.6 (2) | 6.7 (8) | <0.001 | 8.3 (2) | 6.4 (6) | 0.002 |
| Conjunctival Pallor | 2.5 (11) | 0.0 (0) | 9.2 (11) | <0.001 | 0.0 (0) | 11.7 (11) | <0.001 b |
| Palmar pallor | 1.9 (8) | 0.0 (0) | 6.7 (8) | <0.001 | 0.0 (0) | 8.5 (8) | <0.001 b |
| Maternal Anemia c | 32.3 (202/626) | 24.9 (103/414) | 46.7 (99/212) | <0.001 | 35.8 (29/81) | 54.8 (69/126) | <0.001 b |
| Without Gestational Malaria (A) N = 312 % (n) | Submicroscopic Gestational Malaria (B) N = 38 % (n) | Microscopic Gestational Malaria (C) N = 82 % (n) | p (X2) | |
|---|---|---|---|---|
| Bonferroni C = B > A | ||||
| Maternal anemia a | 24.9 (103/414) | 45.7 (59/129) | 47.0 (39/83) | <0.001 |
| Cough | 3.2 (10) | 10.5 (4) | 8.5 (7) | 0.032 |
| Sore throat | 0.6 (2) | 5.3 (2) | 7.3 (6) | 0.001 |
| Bonferroni C > B > A | ||||
| Headache | 39.1 (122) | 47.4 (18) | 85.4 (70) | <0.001 |
| Bonferroni C > A = B | ||||
| Fever | 10.3 (32) | 7.9 (3) | 82.9 (68) | <0.001 |
| Coluria | 2.2 (7) | 2.6 (1) | 11.0 (9) | 0.001 |
| Bonferroni C > A > B | ||||
| Shaking chills | 7.4 (23) | 2.6 (1) | 28.0 (23) | <0.001 |
| Musculoskeletal pain | 6.7 (21) | 0.0 (0) | 42.7 (35) | <0.001 |
| Vomiting | 8.0 (25) | 0.0 (0) | 26.8 (22) | <0.001 |
| Abdominal pain | 5.8 (18) | 0.0 (0) | 17.1 (14) | <0.001 |
| Sweating | 0.3 (1) | 0.0 (0) | 26.8 (22) | <0.001 |
| Asthenia–adynamia | 0.0 (0) | 0.0 (0) | 24.4 (20) | <0.001 |
| The lack of appetite | 0.0 (0) | 0.0 (0) | 22.0 (18) | <0.001 |
| Nausea | 0.0 (0) | 0.0 (0) | 17.1 (14) | <0.001 |
| Conjunctival pallor | 0.0 (0) | 0.0 (0) | 13.4 (11) | <0.001 |
| Palmar pallor | 0.0 (0) | 0.0 (0) | 9.8 (8) | <0.001 |
| Placental Malaria | p Fisher | Causal Species | ||||
|---|---|---|---|---|---|---|
| Negative N = 396 | Positive N = 36 | P. falciparum N = 14 | P. vivax N = 17 | p Chi2 | ||
| % (n) a | % (n) a | % (n) a | % (n) a | |||
| Headache | 45.2 (179) | 47.2 (17) | 0.816 b | 57.1 (8) | 47.1 (8) c | 0.529 |
| Fever | 14.9 (59) | 16.7 (6) | 0.777 b | 14.3 (2) | 23.5 (4) | 0.603 |
| Musculoskeletal pain | 7.1 (28) | 11.1 (4) | 0.327 | 14.3 (2) | 11.8 (2) | 0.593 |
| Shaking chills | 9.1 (36) | 16.7 (6)) | 0.142 b | 14.3 (2) | 21.4 (3) | 0.515 |
| Vomiting | 7.8 (31) | 2.8 (1) | 0.501 | 0 (0) | 5.9 (1) | 0.636 |
| Abdominal pain | 3.0 (12) | 0 (0) | 0.609 | 0 (0) | 0 (0) | 0.772 |
| Cough | 6.1 (24) | 0 (0) | 0.246 | 0 (0) | 0 (0) | 0.511 |
| Sweating | 0 (0) | 0 (0) | -- | 0 (0) | 0 (0) | -- |
| Diarrhea | 3.0 (12) | 0 (0) | 0.609 | 0 (0) | 0 (0) | 0.772 |
| Asthenia–adynamia | 0 (0) | 0 (0) | -- | 0 (0) | 0 (0) | -- |
| Coluria | 3.8 (15) | 0 (0) | 0.625 | 0 (0) | 0 (0) | 0.703 |
| Loss of appetite | 0 (0) | 0 (0) | -- | 0 (0) | 0 (0) | -- |
| Nausea | 0 (0) | 0 (0) | -- | 0 (0) | 0 (0) | -- |
| Sore throat | 2.3 (9) | 0 (0) | 1.000 | 0 (0) | 0 (0) | 0.841 |
| Conjunctival pallor | 0 (0) | 0 (0) | -- | 0 (0) | 0 (0) | -- |
| Palmar pallor | 0 (0) | 0 (0) | -- | 0 (0) | 0 (0) | -- |
| Anemia d | 22.0 (62/281) | 45.7 (43/94) | <0.001 | 48.9 (23/47) | 54.3 (19/35) | <0.001 |
| Weight Kg s | Head Circumference cm | Height at Birth cm | APGAR Score | |||
|---|---|---|---|---|---|---|
| n | Median (IR) | n | Median (IR) | Median (IR) a | Median (IR) a | |
| Gestational Malaria | ||||||
| Negative | 307 | 3.2 (2.9–3.4) | 216 | 34 (33–35) | 50 (49–51) | 8 (7–9) |
| Microscopic | 20 | 3.0 (2.7–3.2) b | 8 | 34 (32–35) | 50 (49–50) | 8 (7–9) |
| Submicroscopic | 73 | 3.1 (2.7–3.2) b | 25 | 33 (32–34) b | 49 (48–51) | 8 (8–9) |
| p Kruskal–Wallis | 0.027 | 0.031 | 0.654 | 0.694 | ||
| Causal species of gestational malaria | ||||||
| Negative | 307 | 3.2 (2.9–3.4) | 216 | 34 (33–35) | 50 (49–51) | 8 (7–9) |
| P. vivax | 45 | 3.0 (2.8–3.3) b | 15 | 33 (32–34) b | 50 (49–50) | 8 (8–9) |
| P. falciparum | 44 | 2.9 (2.7–3.1) b | 16 | 34 (33–34) | 49 (48–51) | 8 (7–9) |
| Mixed | 4 | 2.5 (2.3–2.7) b c | 2 | 31 (31–31) b c | 45 (45–46) b c | 9 (9–9) |
| P Kruskal–Wallis | 0.001 | 0.001 | 0.012 | 0.332 | ||
| Placental Malaria | ||||||
| Negative | 296 | 3.2 (3.0–3.5) | 223 | 34 (33–35) | 50 (49–51) | 8 (7–9) |
| Positive | 104 | 2.9 (2.6–3.1) | 26 | 33 (32–34) | 50 (48–51) | 8 (7–9) |
| p Mann–Whitney | <0.001 | 0.001 | 0.216 | 0.728 | ||
| Causal species of placental malaria | ||||||
| Negative | 296 | 3.2 (2.9–3.5) | 223 | 34 (33–35) | 50 (49–51) | 8 (7–9) |
| P. vivax | 46 | 2.9 (2.6–3.0) b | 17 | 33 (32–34) b | 50 (48–50) | 8 (7–9) |
| P. falciparum | 47 | 2.9 (2.6–3.1) b | 7 | 34 (32–34) b | 50 (48–51) | 8 (7–9) |
| Mixed | 11 | 2.9 (2.2–3.2) b | 2 | 32 (32–32) b | 50 (50–51) | 9 (8–9) |
| p H de Kruskal–Wallis | <0.001 | 0.007 | 0.385 | 0.822 | ||
| Congenital Malaria | ||||||
| Negative | 350 | 3.1 (2.9–3.4) | 240 | 34 (33–34) | 50 (49–51) | 8 (7–9) |
| Positive | 50 | 3.0 (2.7–3.2) | 9 | 32 (32–33) | 49 (49–50) | 8 (7–9) |
| p Mann–Whitney | 0.007 | 0.013 | 0.518 | 0.756 | ||
| Causal species of congenital malaria | ||||||
| Negative | 350 | 3.1 (2.9–3.4) | 240 | 34 (33–34) | 50 (49–51) | 8 (7–9) |
| P. vivax | 16 | 3.0 (2.9–3.1) b | 3 | 32 (32–34) b | 50 (49–50) | 8 (7–8) |
| P. falciparum | 32 | 2.9 (2.7–3.2) b d | 6 | 33 (33–33) b | 49 (49–49) | 9 (9–9) |
| Mixed | 2 | 2.7 (2.5–8.8) b c | -- | -- | -- | -- |
| p Kruskal–Wallis | 0.043 | 0.038 | 0.748 | 0.453 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardona-Arias, J.A.; Higuita-Gutiérrez, L.F.; Carmona-Fonseca, J. Clinical and Parasitological Profiles of Gestational, Placental and Congenital Malaria in Northwestern Colombia. Trop. Med. Infect. Dis. 2023, 8, 292. https://doi.org/10.3390/tropicalmed8060292
Cardona-Arias JA, Higuita-Gutiérrez LF, Carmona-Fonseca J. Clinical and Parasitological Profiles of Gestational, Placental and Congenital Malaria in Northwestern Colombia. Tropical Medicine and Infectious Disease. 2023; 8(6):292. https://doi.org/10.3390/tropicalmed8060292
Chicago/Turabian StyleCardona-Arias, Jaiberth Antonio, Luis Felipe Higuita-Gutiérrez, and Jaime Carmona-Fonseca. 2023. "Clinical and Parasitological Profiles of Gestational, Placental and Congenital Malaria in Northwestern Colombia" Tropical Medicine and Infectious Disease 8, no. 6: 292. https://doi.org/10.3390/tropicalmed8060292
APA StyleCardona-Arias, J. A., Higuita-Gutiérrez, L. F., & Carmona-Fonseca, J. (2023). Clinical and Parasitological Profiles of Gestational, Placental and Congenital Malaria in Northwestern Colombia. Tropical Medicine and Infectious Disease, 8(6), 292. https://doi.org/10.3390/tropicalmed8060292