
Role of Sport Vision in Performance: Systematic Review

 ,
, 
Abstract
1. Introduction
1.1. Sport Vision and Sports Skills
1.2. The Interaction between Visual and Locomotor Systems
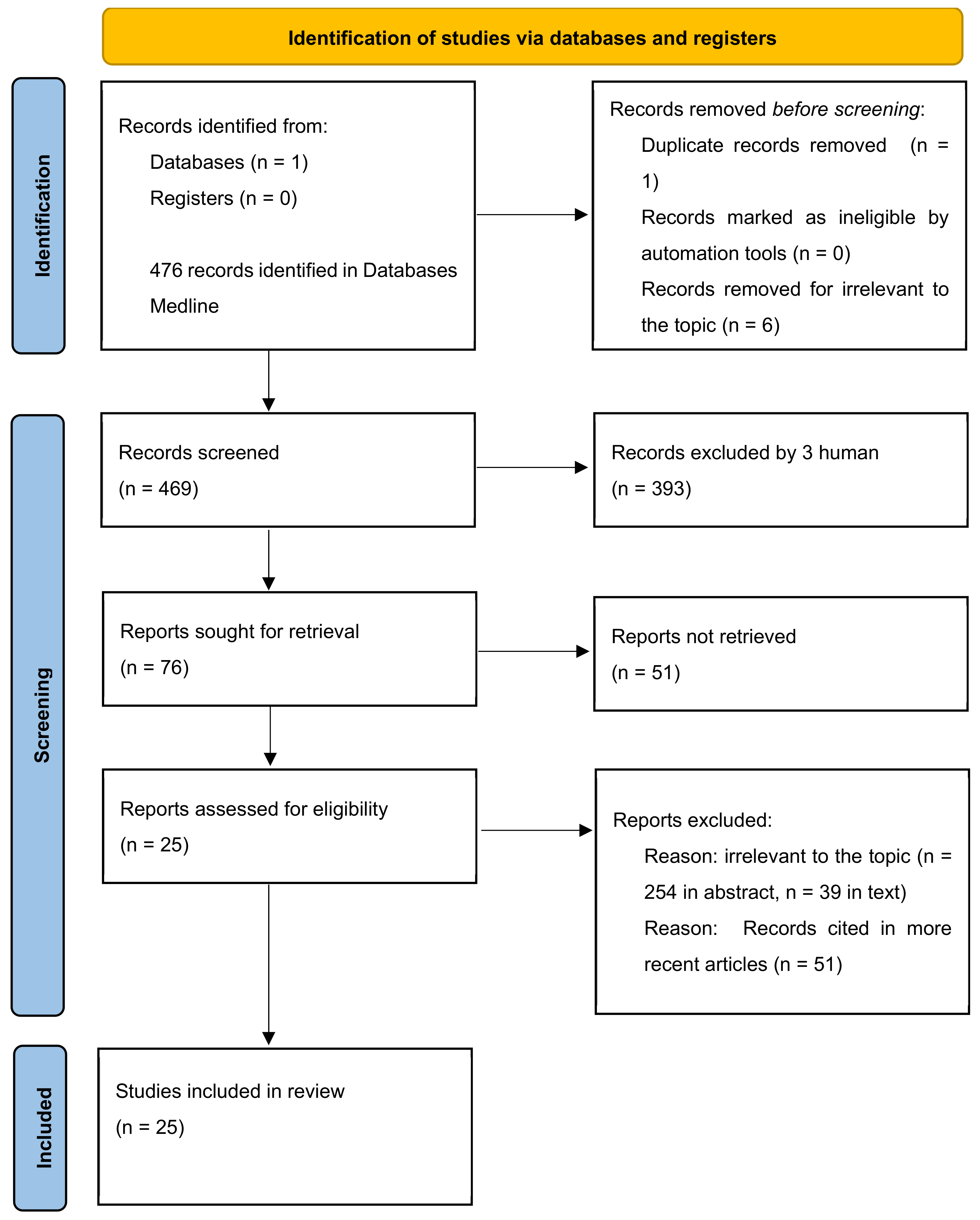
2. Materials and Methods
2.1. Strategy
- MESH: 4 Results
- MESH:13 Results
- MESH:451 Results
- MESH:451 Results
- MESH: 5 Results
2.2. Selection Criteria
2.3. Evaluation Methods
3. Results
3.1. Visual Skills in Different Sports
3.2. Impact of Visual Training on Performance
3.3. How to Evaluate Visual Performance
4. Discussion
4.1. Visual Skills Training
4.2. The Role of Cognitive Factors
4.3. Osteopathy and Prevention
Limitations and Risk of Bias of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nascimento, H.; Martinez-Perez, C.; Alvarez-Peregrina, C.; Sánchez-Tena, M.Á. Citations Network Analysis of Vision and Sport. Int. J. Environ. Res. Public Health 2020, 17, 7574. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, H.; Martinez-Perez, C.; Alvarez-Peregrina, C.; Sánchez-Tena, M.Á. Reply to Laby, D.M.; Appelbaum, L.G. Comment on “Nascimento et al. Citations Network Analysis of Vision and Sport. Int. J. Environ. Res. Public Health 2020, 17, 7574”. Int. J. Environ. Res. Public Health 2021, 18, 6521. [Google Scholar] [CrossRef]
- Nascimento, H.; Alvarez-Peregrina, C.; Martinez-Perez, C.; Sánchez-Tena, M.Á. Vision in Futsal Players: Coordination and Reaction Time. Int. J. Environ. Res. Public Health 2021, 18, 9069. [Google Scholar] [CrossRef] [PubMed]
- Presta, V.; Vitale, C.; Ambrosini, L.; Gobbi, G. Stereopsis in Sports: Visual Skills and Visuomotor Integration Models in Professional and Non-Professional Athletes. Int. J. Environ. Res. Public Health 2021, 18, 11281. [Google Scholar] [CrossRef]
- Sharma, P. The pursuit of stereopsis. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2018, 22, 2.e1–2.e5. [Google Scholar] [CrossRef] [PubMed]
- Matthis, J.S.; Yates, J.L.; Hayhoe, M.M. Gaze and the Control of Foot Placement When Walking in Natural Terrain. Curr. Biol. 2018, 28, 1224–1233.e5. [Google Scholar] [CrossRef] [PubMed]
- Bonnen, K.; Matthis, J.S.; Gibaldi, A.; Banks, M.S.; Levi, D.M.; Hayhoe, M. Binocular vision and the control of foot placement during walking in natural terrain. Sci. Rep. 2021, 11, 20881. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.G.; Panesar, G.K.; MacLellan, M.J.; Pacey, I.E.; Barrett, B.T. Changes to control of adaptive gait in individuals with long-standing reduced stereoacuity. Investig. Ophthalmol. Vis. Sci. 2010, 51, 2487–2495. [Google Scholar] [CrossRef]
- Timmis, M.A.; Pardhan, S. Patients with central visual field loss adopt a cautious gait strategy during tasks that present a high risk of falling. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4120–4129. [Google Scholar] [CrossRef]
- Zhao, J.; Allison, R.S. The Role of Binocular Vision in Avoiding Virtual Obstacles While Walking. IEEE Trans. Vis. Comput. Graph. 2021, 27, 3277–3288. [Google Scholar] [CrossRef]
- Cinelli, M.E.; Patla, A.E.; Allard, F. Strategies used to walk through a moving aperture. Gait Posture 2008, 27, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Mazyn, L.I.; Lenoir, M.; Montagne, G.; Delaey, C.; Savelsbergh, G.J. Stereo vision enhances the learning of a catching skill. Exp. Brain Res. 2007, 179, 723–726. [Google Scholar] [CrossRef] [PubMed]
- Dunn, K.; Marshall, J.G.; Wells, A.L.; Backus, J.E.B. Examining the role of MEDLINE as a patient care information resource: An analysis of data from the Value of Libraries study. J. Med. Libr. Assoc. 2017, 105, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Katikar, M.D.; Ahuja, V.; Doctor, J.R. Not just keywords but MeSH keywords: Do mention for better visibility of your publication. Indian J. Anaesth. 2023, 67, 243–244. [Google Scholar] [CrossRef] [PubMed]
- Olivo, S.A.; Macedo, L.G.; Gadotti, I.C.; Fuentes, J.; Stanton, T.; Magee, D.J. Scales to Assess the Quality of Randomized Controlled Trials: A Systematic Review. Phys. Ther. 2008, 2, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Manzari, L.; Perez-Fernandez, N.; Tramontano, M. Editorial: Gaze and postural stability rehabilitation. Front. Neurol. 2022, 13, 1034012. [Google Scholar] [CrossRef] [PubMed]
- Dalton, K.; Guillon, M.; Naroo, S.A. Ocular Dominance and Handedness in Golf Putting. Optom. Vis. Sci. 2015, 92, 968–975. [Google Scholar] [CrossRef]
- Burris, K.; Vittetoe, K.; Ramger, B.; Suresh, S.; Tokdar, S.T.; Reiter, J.P.; Appelbaum, L.G. Sensorimotor abilities predict on-field performance in professional baseball. Sci. Rep. 2018, 8, 116. [Google Scholar] [CrossRef]
- Formenti, D.; Duca, M.; Trecroci, A.; Ansaldi, L.; Bonfanti, L.; Alberti, G.; Iodice, P. Perceptual vision training in non-sport-specific context: Effect on performance skills and cognition in young females. Sci. Rep. 2019, 9, 18671. [Google Scholar] [CrossRef] [PubMed]
- Regan, D. Visual factors in hitting and catching. J. Sports Sci. 1997, 15, 533–558. [Google Scholar] [CrossRef] [PubMed]
- Guzzetta, A.; Baldini, S.; Bancale, A.; Baroncelli, L.; Ciucci, F.; Ghirri, P.; Putignano, E.; Sale, A.; Viegi, A.; Berardi, N.; et al. Massage accelerates brain development and the maturation of visual function. J. Neurosci. 2009, 29, 6042–6051. [Google Scholar] [CrossRef] [PubMed]
- Zieliński, G.; Filipiak, Z.; Ginszt, M.; Matysik-Woźniak, A.; Rejdak, R.; Gawda, P. The Organ of Vision and the Stomatognathic System—Review of Association Studies and Evidence-Based Discussion. Brain Sci. 2022, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Abdollahipour, R.; Psotta, R.; Land, W.M. The Influence of Attentional Focus Instructions and Vision on Jump Height Performance. Res. Q. Exerc. Sport. 2016, 87, 408–413. [Google Scholar] [CrossRef] [PubMed]
- West, C.G.; Gildengorin, G.; Haegerstrom-Portnoy, G.; Schneck, M.E.; Lott, L.; Brabyn, J.A. Is vision function related to physical functional ability in older adults? J. Am. Geriatr. Soc. 2002, 50, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Futagi, Y. Eye-Hand-Mouth Coordination in the Human Newborn. Pediatr. Neurol. 2017, 75, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Jobe, J.B.; Smith, D.M.; Ball, K.; Tennstedt, S.L.; Marsiske, M.; Willis, S.L.; Rebok, G.W.; Morris, J.N.; Helmers, K.F.; Leveck, M.D.; et al. ACTIVE: A cognitive intervention trial to promote independence in older adults. Control Clin. Trials 2001, 22, 453–479. [Google Scholar] [CrossRef] [PubMed]
- Bach, A.; Bach, M.; Frankel, S. Effect of Osteopathic Cranial Manipulative Medicine on Visual Function. J. Am. Osteopath. Assoc. 2017, 117, 681–682. [Google Scholar] [CrossRef]
- Sandhouse, M.E.; Shechtman, D.; Fecho, G.; Timoshkin, E.M. Effect of Osteopathic Cranial Manipulative Medicine on Visual Function. J. Am. Osteopath. Assoc. 2016, 116, 706–714. [Google Scholar]
- Mardini, D.; Peña, N.; Talsma, J.; Pierce-Talsma, S. Osteopathic Cranial Manipulative Medicine: Frontal and Parietal Lift Techniques. J. Am. Osteopath. Assoc. 2019, 119, e44–e45. [Google Scholar] [CrossRef]
- Yeh, M.L.; Chen, H.H.; Chung, Y.C. One year study on the integrative intervention of acupressure and interactive multimedia for visual health in school children. Complement. Ther. Med. 2012, 20, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Lenoir, M.; Musch, E.; La Grange, N. Ecological relevance of stereopsis in one-handed ball-catching. Percept. Mot. Ski. 1999, 89, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Coco, M.; Buscemi, A.; Tušak, M.; Perciavalle, V.; Nifosì, A.; Cavallari, P.; Di Corrado, D.; Perciavalle, V. Attentive Processes and Blood Lactate in the Sambo. Int. J. Environ. Res. Public Health 2022, 19, 1113. [Google Scholar] [CrossRef] [PubMed]
- Coco, M.; Buscemi, A.; Ramaci, T.; Tusak, M.; Corrado, D.D.; Perciavalle, V.; Maugeri, G.; Perciavalle, V.; Musumeci, G. Influences of Blood Lactate Levels on Cognitive Domains and Physical Health during a Sports Stress. Brief Review. Int. J. Environ. Res. Public Health 2020, 17, 9043. [Google Scholar] [CrossRef] [PubMed]
- Visher, K.C.; Malmanger, D.E. Development of Non-Athlete Norms for the Pacific Sports Visual Performance Profile; Pacific University: Forest Grove, OR, USA, 1988. [Google Scholar]
- Gazzetta Ufficiale il Decreto del Presidente della Repubblica del 7 Luglio 2021, n. 131. Available online: https://www.gazzettaufficiale.it/eli/id/2021/09/29/21G00140/sg (accessed on 7 July 2021).
- Buscemi, A.; Martino, S.; Scirè Campisi, S.; Rapisarda, A.; Coco, M. Endocannabinoids release after Osteopathic Manipulative Treatment. A brief review. J. Complement. Integr. Med. 2020, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Arcuri, L.; Consorti, G.; Tramontano, M.; Petracca, M.; Esteves, J.E.; Lunghi, C. “What you feel under your hands”: Exploring professionals’ perspective of somatic dysfunction in osteopathic clinical practice-a qualitative study. Chiropr. Man. Ther. 2022, 30, 32. [Google Scholar] [CrossRef]
- Akkaş, M.B.; Belviranli, M.; Okudan, N. The effect of osteopathic manipulative treatment on anaerobic performance and lactate clearance in male athletes: A double-blind, randomized, sham-controlled, crossover study. J. Sports Med. Phys. Fit. 2022, 62, 500–507. [Google Scholar] [CrossRef]

{kind=link}
| Author/Year | Reference | Type of Study | Rating Scale | Scale Score | Aim of the Study | Population Studied | Sport Studied | Parameters Analyzed | Means of Evaluation |
|---|---|---|---|---|---|---|---|---|---|
| Nascimento 2020 | [2] | Comment | Not applicable | Not applicable | Use Sport Vision citation networks in order to analyze the relationships between different sports | Not applicable | Not applicable | Not applicable | Not applicable |
| Nascimento 2021 | [3] | Cross-sectional Study | Newcastle–Ottawa scale | ******* | Explore if a group of futsal players, in a laboratory setting, would have better results in actions in which vision is relevant than a control group that has nothing in common with futsal or any other sport. | 10 futsal athletes 35 control group | Futsal | COI-SV software (https://coi-sl.es/software/ accessed on 9 may 2024) | Tests that measure the most relevant visual abilities for futsal |
| Presta 2021 | [4] | Review | Amstar 2 | >1 | The purpose of this review is to take stock of the effects of stereopsis on athletic performance, examining, at the same time, training tools to improve visual abilities and potential differences in the visuomotor integration processes of professional and non-professional athletes. | Professional and non-professional athletes | Interceptive sports (baseball, cricket and tennis,). Strategic Sports (basketball, soccer and volleyball) | Dynamic stereopsis, visual skills (peripheral and spatial vision) | Nike SPARQ—Speed, Power, Agility, Reaction, and Quickness—Sensory Training Station |
| Sharma 2018 | [5] | Review | Amstar 2 scale | >1 | Review of clinical studies on the restoration of alignment and stereopsis in cases of amblyopia, esotropia, strabismus. Medical treatment combined with exercises/video games in monocular and binocular vision. | Children and adults | Not applicable | Stereopsis in children and in adults. | Medical treatment and perceptual training with monocular or binocular video games |
| Matthis 2018 | [6] | Cohort Study | Newcastle–Ottawa scale | ** | Examine the relationship between vision and walking | Walkers | Trekking |
Positive Science mobile eye tracker Motion Shadow inertial measurement unit (IMU) | Techniques that record the gaze of the subjects and the kinematics of the body during the journey |
| Bonnen 2021 | [7] | Observational Study | Newcastle–Ottawa scale | ** | Examine the role of binocular information in the visuomotor control of walking on complex ground | 8-normally-sighted participants 2 had anisometropic amblyopia 2 participants had strabismus | Trekking | Battery of acuity, stereoacuity, and motor tests. | Evaluation of visual tests and measurements of physical function. |
| Buckley 2010 | [8] | Comparative Study (controlled clinical study) | Jadad scale | 2 | Adaptation of the gait in individuals with long-standing stereopsis deficit compared to subjects with normal vision and partial blurring of vision (condition caused for the test). | 12 visually normal subjects and 16 individuals with deficient stereopsis due to amblyopia and/or its associated conditions | Obstacle-crossing performance. Trial with floor-based obstacles of different heights (7–22 cm). | Subjective refraction and binocular vision assessment (cover test, ocular motility, stereo threshold). | Test Chart 2000, Thomson Software (https://thomson-software-solutions.com/products/test-chart-solutions/ accessed on 9 may 2024) Solutions, Herts UK. |
| Timmis 2012 | [9] | Comparative Study (controlled clinical study) | Jadad scale | 1 | Study how patients with central visual field loss (CFL) complete adaptive gait tasks compared to subjects with normal vision and determine if the difficulty of the task significantly affects the control of the movement. | Ten patients with CFL and 12 visual normals | Walking through floor-based obstacles (of different heights, 5 and 10 cm) and also across an unobstructed laboratory (no obstacle present) | Motion analysis systems; Humphrey Field Analyzer. | Analysis of the kinematics of human movement for each task. |
| Zhao 2021 | [10] | Cohort Study | Newcastle–Ottawa scale | **** | The role of binocular vision in virtual locomotion | Ten people (7 males, 3 females, age: 24–39 | Walking | Stride length, Stride height, Foot lifting distance to obstacles or gaps, Foot planting distance to obstacles or gaps, Foot clearance to obstacles, Foot speed of mid swing, Number of strides, Number of collisions. | Walking experiments in virtual environments using a linear treadmill and a novel projected display known as the Wide Immersive Stereo Environment (WISE) |
| Cinelli 2008 | [11] | Analytical study | Newcastle–Ottawa scale | *** | Strategies used to pass through a swinging target and analysis of the movement to reach it. | 7 healthy female students (age: 20–24 years) | Not applicable | Kinematic data | Optotrak (Northern Digital Inc., Waterloo, ON, Canada) system. |
| Mazyn 2007 | [12] | Non-randomized controlled study | Jadad scale | 3 | The contribution of stereopsis in the interceptional task. | 23 female, (22.2 +/− 4.4 years of age) | Tennis | Number of interceptions of balls in training with sessions of different speeds and | Each trial was scored as a catch or amiss. |
| Manzari 2022 | [18] | Editorial | Not applicable | Not applicable | Evaluate the gaze and the postural function both in static and dynamic conditions; new rehabilitation strategies for balance disorders. | Not applicable | Not applicable | Video Head Impulse Test | The gaze stability exercises, standard rehabilitation, galvanic vestibular stimulation |
| Dalton 2015 | [19] | Cohort Study | Newcastle–Ottawa scale | ** | Assess ocular dominance both in primary gaze and direct gaze. | 31 golfers (14 amateur, 7 club professionals, and 10 top professionals) | Golf | Measuring pointing ocular dominance | Retrospective analysis of data collected during optometric examinations, optometric screenings, and putting vision assessments |
| Burris 2018 | [20] | Cohort Study | Newcastle–Ottawa scale | **** | Evaluate connections between sensorimotor skills and sports performance on the field | 252 professional baseball players | Baseball | Sensorimotor abilities | Nike Sensory Station assessment battery |
| Formenti 2019 | [21] | Randomized Controlled Trial | Jadad scale | 3 | Hypothesis of the study: “Does visual training in a non-specific context improve sport-specific skills?” | 51 volleyball players | Volleyball | Volleyball-specific skills (setting, serving, passing), clinical reaction time, visual search task. | Sport vision training programmes |
| Regan 1997 | [22] | Review | Amstar 2 | >1 | Visual factors in hitting and catching | Not applicable | Cricket | Not applicable | Application of sports physics |
| Guzzetta 2009 | [23] | Clinical trial | Jadad scale | 2 | To explore the effects of body massage in preterm infants and found that massage accelerates the maturation of electroencephalographic activity and of visual function, in particular visual acuity. | Rat pups | Not applicable | Level of IGF-1 in the cortex | Body massage |
| Zieliński 2022 | [24] | Review | Amstar 2 scale | >1 | Connections between the organ of vision and the stomatognathic system | Not applicable | Not applicable | Not applicable | Not applicable |
| Abdollahipour 2016 | [25] | Observational Study | Newcastle–Ottawa scale | ** | The influence of vision on attentional focus during the execution of movements. | 24 adults, average age 25 years. | Maximum vertical jump | Measurement of jump height | Jump with external focus, internal focus, and control (no-focus instruction). |
| West 2002 | [26] | Cross-sectional study | Newcastle–Ottawa scale | ******* | Evaluate the relationship between visual functions and physical performance in older adults. | 782 adults aged 55 and older | Walking and balance | Comprehensive battery of vision tests and physical function measures. | Evaluation of visual tests and measurements of physical function. |
| Futagi 2017 | [27] | Review | Amstar 2 scale | >1 | Clarify the ontogenetic meaning of coordination during the first months of life and its neuronal mechanism according to the current knowledge of cognitive neuroscience | n 117 full-term normal newborns, | Not applicable | Hand-mouth coordination, Eye-hand coordination, Eye-mouth coordination | Clinical evaluation of video footage. |
| Jobe 2001 | [28] | Control Clin Trials | Jadad scale | 5 | Cognitive training and its effects on daily functioning | 2832 participants (predominantly female and ranging in age from 65–94 years with an average age of 73.6 years) | Not applicable | Tests of memory, telephone interview, in-person interview, MOS 36-item Short Form (SF-36) | Tests of memory, reasoning, and speed of information processing |
| Bach 2017 | [29] | Comment | Not applicable | Not applicable | With the numerous limitations that the authors discussed, including some of those we have mentioned, we question the validity of this study’s results (Sandhouse 2016). | Not applicable | Not applicable | Not applicable | Not applicable |
| Sandhouse 2016 | [30] | Randomized Controlled Trial | Jadad scale | 4 | The authors conducted a study that examined whether osteopathic cranial manipulative medicine produced a measurable change in visual function in adults with cranial asymmetry. | Adult volunteers aged between 18 and 35 years with unremarkable systemic or ocular history were recruited. 47 in the treatment group and 42 in the sham therapy group. | Not applicable | Preintervention and postintervention ophthalmic examinations consisted of distance visual acuity testing, accommodative system testing, local stereoacuity testing, pupillary size measurements, and vergence system testing. | Osteopathic cranial manipulative medicine |
| Mardini 2019 | [31] | Description of techniques | Not applicable | Not applicable | Many conditions may be helped by osteopathic manipulative treatment. These conditions include ocular dysfunction, such as strabismus and astigmatism. Description of the frontal and parietal lifting techniques | Not applicable | Not applicable | This video was produced by Touro University College of Osteopathic Medicine-CA. | Osteopathic Cranial Manipulative Medicine: Frontal and Parietal Lift Techniques |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buscemi, A.; Mondelli, F.; Biagini, I.; Gueli, S.; D’Agostino, A.; Coco, M. Role of Sport Vision in Performance: Systematic Review. J. Funct. Morphol. Kinesiol. 2024, 9, 92. https://doi.org/10.3390/jfmk9020092
Buscemi A, Mondelli F, Biagini I, Gueli S, D’Agostino A, Coco M. Role of Sport Vision in Performance: Systematic Review. Journal of Functional Morphology and Kinesiology. 2024; 9(2):92. https://doi.org/10.3390/jfmk9020092
Chicago/Turabian StyleBuscemi, Andrea, Flora Mondelli, Ilaria Biagini, Stella Gueli, Angela D’Agostino, and Marinella Coco. 2024. "Role of Sport Vision in Performance: Systematic Review" Journal of Functional Morphology and Kinesiology 9, no. 2: 92. https://doi.org/10.3390/jfmk9020092
APA StyleBuscemi, A., Mondelli, F., Biagini, I., Gueli, S., D’Agostino, A., & Coco, M. (2024). Role of Sport Vision in Performance: Systematic Review. Journal of Functional Morphology and Kinesiology, 9(2), 92. https://doi.org/10.3390/jfmk9020092