Physical Exercise Is Confirmed to Reduce Low Back Pain Symptoms in Office Workers: A Systematic Review of the Evidence to Improve Best Practices in the Workplace

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
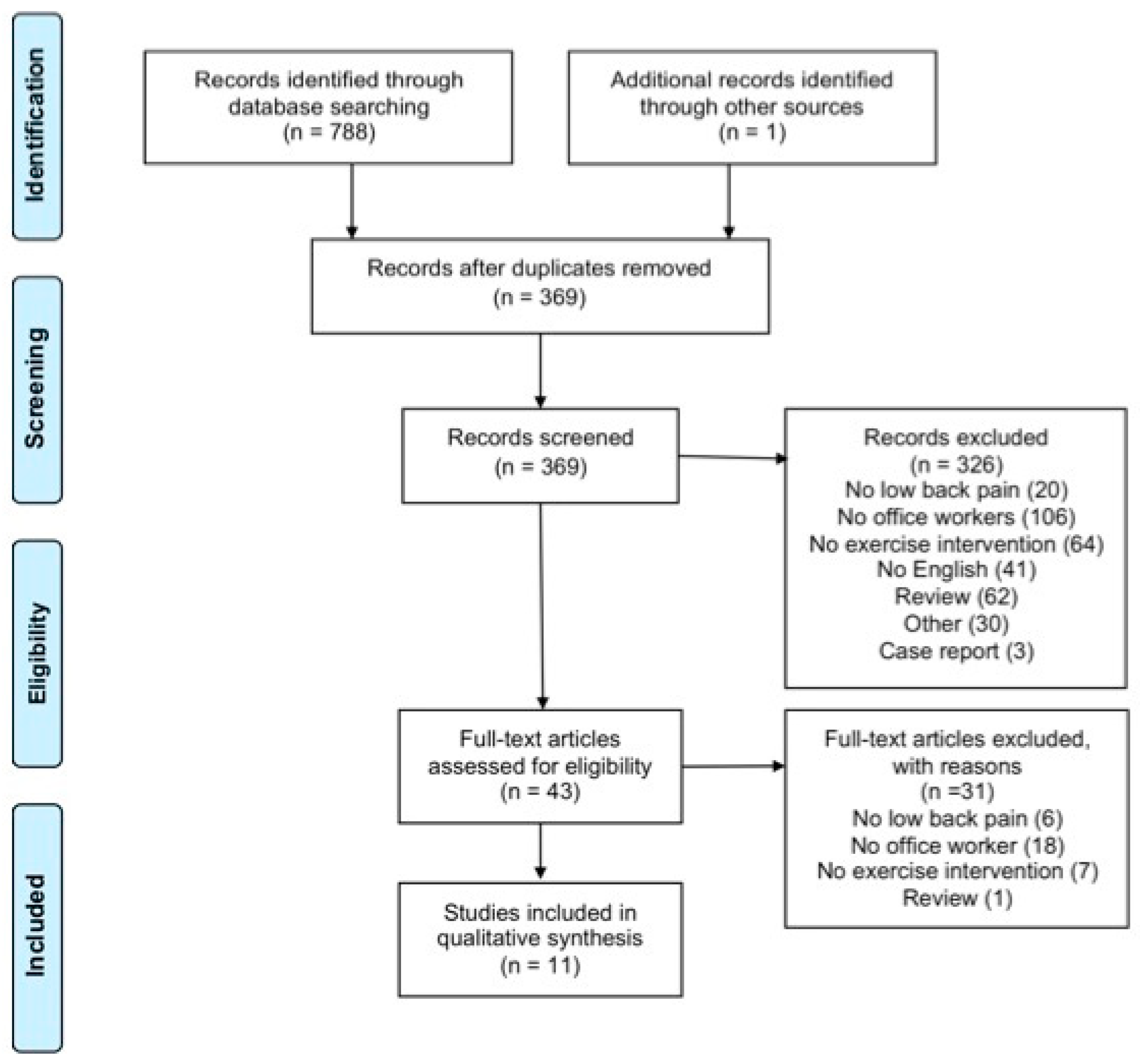
2.1. Study Design
2.2. Literature Research
2.3. Inclusion and Exclusion Criteria
2.4. Study Quality Assessment
2.5. Data Extraction and Synthesis
3. Results
3.1. Pain and Disability
3.2. Flexibility, ROM, and Muscular Strength
3.3. Quality of Life
4. Discussion
4.1. Effects of Physical Exercise on Pain and Disability
4.2. Effects of Physical Exercise on Flexibility, ROM, and Muscular Strength
4.3. Effects of Physical Exercise on Quality of Life
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Van Dieen, J.H.; Kuijer, P.P.; Burdorf, A.; Marras, W.S.; Adams, M.A. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.C.; Chenot, J.F.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. Acsm’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer: Alfon am Rhein, The Netherlands, 2018. [Google Scholar]
- Hochschuler, S.H. Back Pain Risk Factors: What Can Increase the Potential for Back Problems? Available online: https://www.spine-health.com/conditions/lower-back-pain/back-pain-risk-factors-what-can-increase-potential-back-problems (accessed on 2 September 2019).
- Janwantanakul, P.; Pensri, P.; Jiamjarasrangsri, V.; Sinsongsook, T. Prevalence of self-reported musculoskeletal symptoms among office workers. Occup. Med. 2008, 58, 436–438. [Google Scholar] [CrossRef]
- Samanta, J.; Kendall, J.; Samanta, A. 10-minute consultation: Chronic low back pain. BMJ 2003, 326, 535. [Google Scholar] [CrossRef]
- Sowah, D.; Boyko, R.; Antle, D.; Miller, L.; Zakhary, M.; Straube, S. Occupational interventions for the prevention of back pain: Overview of systematic reviews. J. Saf. Res. 2018, 66, 39–59. [Google Scholar] [CrossRef]
- Rasotto, C.; Bergamin, M.; Simonetti, A.; Maso, S.; Bartolucci, G.B.; Ermolao, A.; Zaccaria, M. Tailored exercise program reduces symptoms of upper limb work-related musculoskeletal disorders in a group of metalworkers: A randomized controlled trial. Man. Ther. 2015, 20, 56–62. [Google Scholar] [CrossRef]
- CDC. Worksite Physical Activity. Available online: https://www.cdc.gov/physicalactivity/worksite-pa/index.htm (accessed on 19 July 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 151, 264–269. [Google Scholar]
- Van Tulder, M.W.; Assendelft, W.J.; Koes, B.W.; Bouter, L.M. Method guidelines for systematic reviews in the cochrane collaboration back review group for spinal disorders. Spine 1997, 22, 2323–2330. [Google Scholar] [CrossRef]
- Bullo, V.; Gobbo, S.; Vendramin, B.; Duregon, F.; Cugusi, L.; Di Blasio, A.; Bocalini, D.S.; Zaccaria, M.; Bergamin, M.; Ermolao, A. Nordic walking can be incorporated in the exercise prescription to increase aerobic capacity, strength, and quality of life for elderly: A systematic review and meta-analysis. Rejuvenation Res. 2018, 21, 141–161. [Google Scholar] [CrossRef]
- Gobbo, S.; Bergamin, M.; Sieverdes, J.C.; Ermolao, A.; Zaccaria, M. Effects of exercise on dual-task ability and balance in older adults: A systematic review. Arch. Gerontol. Geriatr. 2014, 58, 177–187. [Google Scholar] [CrossRef]
- Vendramin, B.; Bergamin, M.; Gobbo, S.; Cugusi, L.; Duregon, F.; Bullo, V.; Zaccaria, M.; Neunhaeuserer, D.; Ermolao, A. Health benefits of zumba fitness training: A systematic review. PM R 2016, 8, 1181–1200. [Google Scholar] [CrossRef]
- Phattharasupharerk, S.; Purepong, N.; Eksakulkla, S.; Siriphorn, A. Effects of qigong practice in office workers with chronic non-specific low back pain: A randomized controlled trial. J. Bodyw. Mov. Ther. 2019, 23, 375–381. [Google Scholar] [CrossRef]
- Shariat, A.; Cleland, J.A.; Danaee, M.; Kargarfard, M.; Sangelaji, B.; Tamrin, S.B.M. Effects of stretching exercise training and ergonomic modifications on musculoskeletal discomforts of office workers: A randomized controlled trial. Braz. J. Phys. Ther. 2018, 22, 144–153. [Google Scholar] [CrossRef]
- Suni, J.H.; Rinne, M.; Tokola, K.; Manttari, A.; Vasankari, T. Effectiveness of a standardised exercise programme for recurrent neck and low back pain: A multicentre, randomised, two-arm, parallel group trial across 34 fitness clubs in finland. BMJ Open Sport Exerc. Med. 2017, 3, e000233. [Google Scholar] [CrossRef][Green Version]
- Shariat, A.; Lam, E.T.; Kargarfard, M.; Tamrin, S.B.; Danaee, M. The application of a feasible exercise training program in the office setting. Work 2017, 56, 421–428. [Google Scholar] [CrossRef]
- Habibi, E.; Soury, S. The effect of three ergonomics interventions on body posture and musculoskeletal disorders among stuff of isfahan province gas company. J. Educ. Health Promot. 2015, 4, 65. [Google Scholar] [CrossRef]
- Kim, T.H.; Kim, E.H.; Cho, H.Y. The effects of the core programme on pain at rest, movement-induced and secondary pain, active range of motion, and proprioception in female office workers with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2015, 29, 653–662. [Google Scholar] [CrossRef]
- Mehrparvar, A.H.; Heydari, M.; Mirmohammadi, S.J.; Mostaghaci, M.; Davari, M.H.; Taheri, M. Ergonomic intervention, workplace exercises and musculoskeletal complaints: A comparative study. Med. J. Islam. Repub. Iran 2014, 28, 69. [Google Scholar]
- del Pozo-Cruz, B.; Gusi, N.; del Pozo-Cruz, J.; Adsuar, J.C.; Hernandez-Mocholi, M.; Parraca, J.A. Clinical effects of a nine-month web-based intervention in subacute non-specific low back pain patients: A randomized controlled trial. Clin. Rehabil. 2013, 27, 28–39. [Google Scholar] [CrossRef]
- del Pozo-Cruz, B.; Parraca, J.A.; del Pozo-Cruz, J.; Adsuar, J.C.; Hill, J.; Gusi, N. An occupational, internet-based intervention to prevent chronicity in subacute lower back pain: A randomised controlled trial. J. Rehabil. Med. 2012, 44, 581–587. [Google Scholar] [CrossRef]
- Pensri, P.; Janwantanakul, P. Effectiveness of brief education combined with a home-based exercise program on pain and disability of office workers with chronic low back pain: A pilot study. J. Phys. Ther. Sci. 2012, 24, 217–222. [Google Scholar] [CrossRef]
- Macedo, A.C.; Trindade, C.S.; Brito, A.P.; Socorro Dantas, M. On the effects of a workplace fitness program upon pain perception: A case study encompassing office workers in a portuguese context. J. Occup. Rehabil. 2011, 21, 228–233. [Google Scholar] [CrossRef]
- Sihawong, R.; Janwantanakul, P.; Jiamjarasrangsi, W. A prospective, cluster-randomized controlled trial of exercise program to prevent low back pain in office workers. Eur. Spine J. 2014, 23, 786–793. [Google Scholar] [CrossRef]
- Nakata, H.; Sakamoto, K.; Kakigi, R. Meditation reduces pain-related neural activity in the anterior cingulate cortex, insula, secondary somatosensory cortex, and thalamus. Front. Psychol. 2014, 5, 1489. [Google Scholar] [CrossRef]
- Robroek, S.J.; van Lenthe, F.J.; van Empelen, P.; Burdorf, A. Determinants of participation in worksite health promotion programmes: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 26. [Google Scholar] [CrossRef]
- Lee, J.; Park, S. The relationship between physical capacity and fear avoidance beliefs in patients with chronic low back pain. J. Phys. Ther. Sci. 2017, 29, 1712–1714. [Google Scholar] [CrossRef]
- Lee, A.S.; Cholewicki, J.; Reeves, N.P.; Zazulak, B.T.; Mysliwiec, L.W. Comparison of trunk proprioception between patients with low back pain and healthy controls. Arch. Phys. Med. Rehabil. 2010, 91, 1327–1331. [Google Scholar] [CrossRef]
- Ellegaard, H.; Pedersen, B.D. Stress is dominant in patients with depression and chronic low back pain. A qualitative study of psychotherapeutic interventions for patients with non-specific low back pain of 3-12 months’ duration. BMC Musculoskelet. Disord. 2012, 13, 166. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Morso, L.; Bendix, T.; Manniche, C. Supervised and non-supervised nordic walking in the treatment of chronic low back pain: A single blind randomized clinical trial. BMC Musculoskelet. Disord. 2010, 11, 30. [Google Scholar] [CrossRef]


{kind=link}
| PICOS | Details |
|---|---|
| Participants | Office workers with LBP symptoms |
| Interventions | Supervised or non-supervised exercise protocol, performed at home or in the workplace |
| Comparative factors | Exercise intervention for LBP management |
| Outcomes | Primary outcomes: LBP symptoms Secondary outcomes: flexibility and ROM of the trunk, muscular strength of the trunk, QoL |
| Study designs | Pilot study, RCT, no-RCT, exploratory study, Randomized pilot trial |
| Citation | Randomization Procedure | Similarity of Study Groups | Inclusion or Exclusion Criteria | Dropouts | Blinding | Compliance | Intention-to-Treat Analysis | Timing of Outcomes Assessment | Follow-up | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Phattharasupharerk S. et al. (2018) [15] | + | − | + | + | + | − | + | + | − | 6/9 |
| Shariat A. et al. (2018) [16] | + | + | + | + | + | - | − | − | − | 5/9 |
| Suni J.H. et al. (2017) [17] | + | + | + | + | + | + | − | − | + | 7/9 |
| Shariat A. et al. (2017) [18] | + | + | − | − | − | − | − | − | − | 2/9 |
| Habibi E. et al. (2015) [19] | − | + | − | − | − | − | − | + | − | 2/9 |
| Kim T.H. et al. (2015) [20] | + | + | + | + | + | + | − | − | + | 7/9 |
| Mehrparvar A. H. et al. (2014) [21] | + | − | + | + | − | − | − | − | − | 3/9 |
| del Pozo-Cruz B. et al. (2013) [22] | + | + | + | + | + | + | − | − | − | 6/9 |
| del Pozo-Cruz B. et al. (2012) [23] | + | + | + | + | + | + | + | − | − | 7/9 |
| Pensri P. et al. (2012) [24] | − | − | + | + | − | + | − | + | + | 5/9 |
| Macedo A.C. et al. (2011) [25] | − | − | − | + | − | + | − | − | − | 2/9 |
| Study | Subjects | Grouping | Training Modality, Program and Intensity | Duration and Frequency |
|---|---|---|---|---|
| Phattharasupharerk S. et al. (2018) [15] | N: 72 Age: 20–40 years old Chronic LBP | EG (36) EdG (36) | EG: Qigong protocol Based on static and dynamic posture, meditation/imagination, and breathing exercise. Week 1: 25 min of static qigong, 5 min of dynamic qigong, 2 min of acupressure at acupoint GV20, 10 min of Wu Chi meditation. Week 2: 28 min of static qigong, 4 min of acupressure at acupoint K11, 15 min of Wu Chi meditation. Week 3: 28 min of static qigong, 5 min of dynamic qigong, 4 min of acupressure at acupoint LI4, 15 min of Wu Chi meditation Week 4: 28 min of static qigong, 5 min of dynamic qigong, 4 min of acupressure at acupoint PC6, 15 min of Wu Chi meditation. Week 5: 28 min of static qigong, 5 min of dynamic qigong, 4 min of acupressure at acupoint ST36, 15 min of Wu Chi meditation. Week 6: 4 min of static qigong, 10 min of dynamic qigong, 4 min of acupressure at acupoint HT7, 15 min of Wu Chi meditation. EdG: Education protocol General advice on managing LBP in order to reduce it, and the recommendation to stay active. | 6 weeks 60 min 1 d/w At home every day Adh: n.r. |
| Shariat A. et al. (2018) [16] | N: 142 (47 M; 95 F) Age: 20–50 years old Subacute LBP | WBG (43) EgG (37) WB+EgG (34) CG (28) | WBG: stretching protocol Office-based stretching exercises adopted from McKenzie’s exercises, William’s exercises, and ACSM guidelines. The exercises were performed constant, controlled, and slow. Tension was progressively increased to the end of the joint’s ROM until the mild discomfort point is touched. 10 repetitions (or last for a period of 10–15 sec) and 3 sets (with a rest of 60–90 sec. Ergonomic protocol Total workplace occupational safety and health and ergonomic intervention (chair height and working desk, sitting posture, distance and level between the eyes and the monitor). | 6 months 3 d/w 10–15 min Adh: n.r. |
| Suni J.H. et al. (2017) [17] | N: 143 Age 30–50 years old Subacute LBP | EG (75) CG (68) | Warm-up: 10 min of aerobic exercise. Main part: 10 functional flexibility exercises, 4 strength, and 5 core exercises. Cool-down: 10 min of stretching. | EG: 10 weeks 2 d/w 60 min Adh: 67% |
| Shariat A. et al. (2017) [18] | N: 40 Age: mean 28 years old | WBG (20) CG (20) | 13 office-based stretching exercises. Each exercise was designed to have slow, controlled, and constant movements. Tension was progressively increased to the end of the joint’s ROM until the mild discomfort point is touched. The entire set of exercise was performed for 3 times with a rest of 60–90 sec between sets. Week 1–2: learn and practice. Week 3–5: 10 sec for each exercise. Week 6–8: 20 sec for each exercise. Week 9–11: 30 sec for each exercise. | 11 weeks 10–15 min 3 d/w Adh: n.r. |
| Habibi E. et al. (2015) [19] | N: 75 (52 M; 23 F) Age: mean 41.2 years old | EgG (25) EG (25) WBG (25) | Ergonomic protocol Different courses based on educational needs. The objectives were understanding office ergonomics principles, self-evaluation of workplace conditions, and arranging and organizing personal workspace. EG: water protocol Water exercise to strengthen the muscles around the spine. SG: web-based exercise Exercises during work time. They were designed for short periods of time, and for many of them, there was no need to get up and stand. At regular intervals the app reminded the user to exercise. | EgG and WBG 2.5 months EG 2.5 months 2–3 d/w 20 min Adh: n.r. |
| Kim T.H. et al. (2014) [20] | N: 53, F Age: 20–40 years old Chronic LBP | HG (27) TG (26) | HG: Exercise protocol + TENS Warm-up Main part: isometric contraction of core muscles, including internal/external oblique, rectus abdominis, and erector spinae muscles. Cool-down: slow and controlled movement, controlling their breathing. TG: TENS treatment 20 min of TENS and 15 min of hot-pack treatment. | 8 weeks 30 min exercise (only HG) 20 min TENS 15 min hot pack 5 d/w Adh: 85.5% |
| Mehrparvar A. H. et al. (2014) [21] | N: 164 (81 M; 83 F) Age: mean 38 years old | EgG (83) WBG (81) | Ergonomic protocol Change in desk placement, seat height, position of keyboard, mouse and monitor, following OSHA VDT workstation checklist. SG: Exercise protocol One training session to learn exercise. Stretching of neck, shoulder, writ, back, and low back. | 1 months 15 min 2 times/day, every day Adh: n.r. |
| del Pozo-Cruz B. et al. (2013) [22] del Pozo-Cruz B. et al. (2012) [23] | N: 90 (12 M; 78 F) Age: mean 46 years old Subacute LBP | WBG (46)CG (44) | Postural stability muscles (abdominal, lumbar, hip and thigh muscles) exercise to strength, flexibility, mobility, and stretching. Mobility exercises: large movements of the joints associated with the postural stability muscles. Flexibility exercises: static work methodology. Strengthening exercises: shortening and stretching motion that progressively changed in speed (1:1, 1:2, 1:3, 2:1, 3:1) combined with slight isometric contractions of the muscles involved in the exercises. Stretching exercises: moderate stretching of the muscles involved in the session. | 9 months 11 min 5 d/w Adh: 92% |
| Pensri P. et al. (2012) [24] | N: 30 (6 M; 24 F) Age: 18–60 years old Chronic LBP | HG (30) | Brief education regarding LBP and home-based exercise protocol. Home-based exercises were categorized in core stability, stretching, and mobility. Each exercise was performed for 5–15 sec and repeat 5 times per set. Sometimes they received treatment including hot packs, lumbar packs, lumbar traction, and/or electrotherapy. | 8 weeks 3 t/d Adh: 33 day of 40 |
| Macedo A.C. et al. (2011) [25] | N: 40 Age: 40.8 years old | EG (29) CG (21) | Stretching exercises for the body parts most affected by pain complaints. Playful and recreational activities. Massage with physiotherapy ball and exercises with Pilates balls. Relaxation exercises/stretches on an individual basis, in pairs and in groups performed with background music. | 8 months 15 min 3 d/w Adh: 48% |
| Study | Group Comparison | Results |
|---|---|---|
| Phattharasupharerk S. et al. (2018) [15] | EG versus EdG | Pain and disability VAS (sc): ↑EG *; ↓EdG; ** RMDQ (sc): ↑EG *; ↓EdG; ** Quality of life ST-5 (sc): ↑EG; ↓EdG; ** Flexibility, ROM and muscular strength Lumbar flexion (°): ↑EG *; ↓EdG; ** Lumbar extension (°): #; ↑EG *; =EdG; ** Lumbar rotation R (°): ↑EG; ↓EdG; ** Lumbar rotation L (°): #; ↑EG *; =EdG; ** Lumbar bending R (°): ↑EG *; =EdG; ** Lumbar bending R (°): ↑EG *; =EdG; ** Core stability index (mmHg * sec): ↑EG *; ↓EdG; ** |
| Shariat A. et al. (2018) [16] | WBG versus EgG | Pain and disability LB CMDQ (sc): ↑EG *; ↑EgG * |
| WBG versus WB+EgG | Pain and disability LB CMDQ (sc): ↑EG *; ↑E+EgG * | |
| WBG versus CG | Pain and disability LB CMDQ (sc): ↑EG *; =CG; ** | |
| EgG versus WB+EgG | Pain and disability LB CMDQ (sc): ↑EgG *; ↑E+EgG * | |
| EgG versus CG | Pain and disability LB CMDQ (sc): ↑EgG *; =CG | |
| WB+EgG versus CG | Pain and disability LB CMDQ (sc): ↑E+EgG *; =CG; ** | |
| Suni J.H. et al. (2017) [17] | EG versus CG | Pain and disability LB VAS (sc): ↑EG; ↑CG LBP frequency (sc): ↑EG; ↑CG LB strain after work (sc): ↑EG; ↑CG Quality of life SF-36-PF: ↑EG; ↑CG; ** SF-36-RP: ↑EG *; ↑CG SF-36-BP: ↑EG; ↑CG; ** SF-36-GH: ↑EG *; ↑CG SF-36-VT: ↑EG *; ↑CG SF-36-SF: n.r. SF-36-RE: ↑EG; ↓CG SF-36-MH: n.r. Flexibility, ROM and muscular strength Trunk-side bending (cm): ↑EG *; ↑CG; ** Static wall squat test (sec): ↑EG *; ↑CG; ** |
| Shariat A. et al. (2017) [18] | WBG versus CG | Pain and disability LB CMDQ (sc): ↑WBG *; =CG; ** Flexibility, ROM and muscular strength Hip R (°): ↑WBG; ↓CG; ** Hip L (°): ↑WBG; =CG; ** Knee R (°): ↑WBG; =CG; ** Knee L (°): ↑WBG; =CG; ** |
| Habibi E. et al. (2015) [19] | EG versus EgG | Pain and disability LBP incidence (%): ↑EG *; ↑EgG * |
| EG versus WBG | Pain and disability LBP incidence (%): ↑EG *; =WBG | |
| EgG versus WBG | Pain and disability LBP incidence (%): ↑EgG *; =WBG | |
| Kim T.H. et al. (2015) [20] | HG versus TG | Pain and disability VAS at rest (mm): ↑HG *; ↑TG; ** VAS during movement (mm): ↑HG *; ↑TG; ** PPT quadratus lumborum (Kg/cm2): ↑HG *; ↑TG; ** PPT sacroiliac joint (Kg/cm2): ↑HG *; ↑TG; ** Flexibility, ROM and muscular strength Active ROM trunk flexion (°):↑HG *; ↑TG; **Active ROM trunk extension (°):↑HG *; ↑TG; ** Propioception at 20° flexion (°):↑HG *; ↑TG; ** Propioception at 10° extension (°):↑HG *; ↑TG; ** |
| Mehrparvar A.H. et al. (2014) [21] | WGB versus EgG | Pain and disability Pain frequency: ↑WBG *; ↑EgG *; ** |
| Del Pozo–Cruz B. et al. (2013) [22] | WBG versus CG | Pain and disability VAS (%): ** ODI (%): ** SBST (%): ** Quality of life EQ-5D-3L (%): ** Mobility: ** Self-care: ** Daily task: Pain/discomfort: ** Anxiety/depression: ** |
| Del Pozo-Cruz B. et al. (2012) [23] | WBG versus CG | Pain and disability SBST, total (sc): ↑WBG *; =CG; ** Item1 - Bothersomeness: ↑WBG; ↓CG Item2 - Referred leg pain: ↑WBG; ↓CG Item3 - Co-morbid pain: ↑WBG; ↑CG Item4 - Fear avoidance: ↑WBG; ↑CG; ** Item5 - Functional disability: ↑WBG; ↓CG; ** Item6 - Functional disability: ↑WBG; ↑CG; ** Item7 - Catastrophizing: ↑WBG; ↑CG Item8 - Anxiety: ↑WBG; ↓CG Item9 - Depression: ↑WBG; ↑CG Low risk of chronicity (%): ↑WBG; ↓CG ** Medium risk of chronicity (%): ↑WBG; ↓CG High risk of chronicity (%): ↑WBG; ↓CG |
| Pensri P. et al. (2012) [24] | HG | Pain and disability VAS (sc): ↑ * Backache Index (sc): ↑ |
| Macedo AC et al. (2011) [25] | EG versus CG | Pain and disability VAS – L lumbar zone (mm): ↑EG *; ↓CG; ** VAS – R lumbar zone (mm): ↑EG *; ↓CG; ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gobbo, S.; Bullo, V.; Bergamo, M.; Duregon, F.; Vendramin, B.; Battista, F.; Roma, E.; Bocalini, D.S.; Rica, R.L.; Alberton, C.L.; et al. Physical Exercise Is Confirmed to Reduce Low Back Pain Symptoms in Office Workers: A Systematic Review of the Evidence to Improve Best Practices in the Workplace. J. Funct. Morphol. Kinesiol. 2019, 4, 43. https://doi.org/10.3390/jfmk4030043
Gobbo S, Bullo V, Bergamo M, Duregon F, Vendramin B, Battista F, Roma E, Bocalini DS, Rica RL, Alberton CL, et al. Physical Exercise Is Confirmed to Reduce Low Back Pain Symptoms in Office Workers: A Systematic Review of the Evidence to Improve Best Practices in the Workplace. Journal of Functional Morphology and Kinesiology. 2019; 4(3):43. https://doi.org/10.3390/jfmk4030043
Chicago/Turabian StyleGobbo, Stefano, Valentina Bullo, Manuele Bergamo, Federica Duregon, Barbara Vendramin, Francesca Battista, Enrico Roma, Danilo Sales Bocalini, Roberta Luksevicius Rica, Cristine Lima Alberton, and et al. 2019. "Physical Exercise Is Confirmed to Reduce Low Back Pain Symptoms in Office Workers: A Systematic Review of the Evidence to Improve Best Practices in the Workplace" Journal of Functional Morphology and Kinesiology 4, no. 3: 43. https://doi.org/10.3390/jfmk4030043
APA StyleGobbo, S., Bullo, V., Bergamo, M., Duregon, F., Vendramin, B., Battista, F., Roma, E., Bocalini, D. S., Rica, R. L., Alberton, C. L., Cruz-Diaz, D., Priolo, G., Pancheri, V., Maso, S., Neunhaeuserer, D., Ermolao, A., & Bergamin, M. (2019). Physical Exercise Is Confirmed to Reduce Low Back Pain Symptoms in Office Workers: A Systematic Review of the Evidence to Improve Best Practices in the Workplace. Journal of Functional Morphology and Kinesiology, 4(3), 43. https://doi.org/10.3390/jfmk4030043