
FDG-PET/MRI for Nonoperative Management of Rectal Cancer: A Prospective Pilot Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
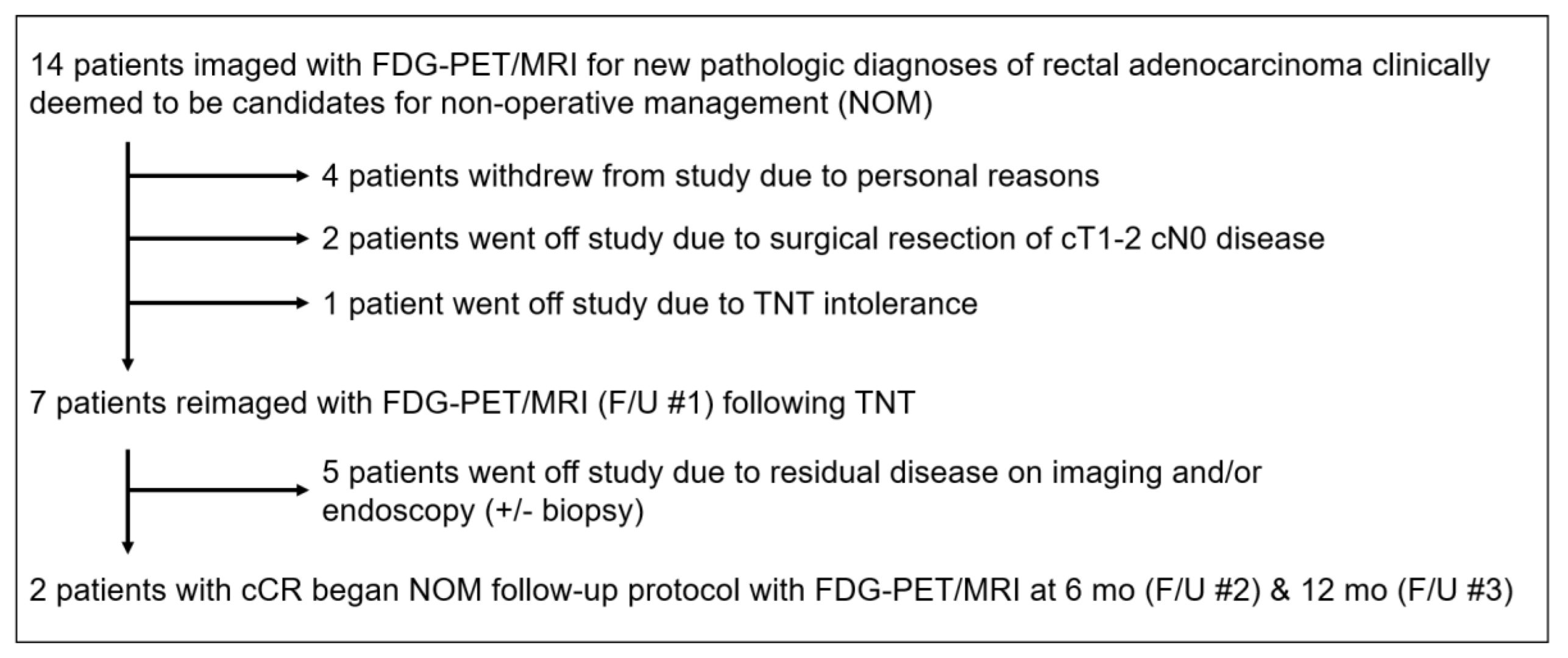
2.1. Subjects
2.2. Imaging and Clinical Management Algorithm
2.3. FDG-PET/MRI Imaging Protocol
2.4. Image Review and Analysis
- mrTRG 1: no/minimal fibrosis visible (tiny linear scar) and no tumor signal
- mrTRG 2: dense fibrotic scar but no macroscopic tumor signal
- mrTRG 3: fibrosis predominates but obvious measurable areas of tumor signal
- mrTRG 4: tumor signal predominates with little/minimal fibrosis
- mrTRG 5: tumor signal only (no fibrosis) or tumor progression
- pmrTRG 1: mrTRG 1–2 and no appreciable tumor signal on PET (FDG uptake in rectal wall similar to or less than background rectum)
- pmrTRG 2: mrTRG 1–2 and possible tumor on PET (focal FDG uptake in wall of rectum equivocally above background rectal wall)
- pmrTRG 3: mrTRG 3–5 or definite tumor on PET (focal FDG uptake in wall of rectum clearly above background rectal wall)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Aguilar, J.; Patil, S.; Gollub, M.J.; Kim, J.K.; Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Omer, D.M.; Lee, M.; Dunne, R.F.; et al. Organ Preservation in Patients With Rectal Adenocarcinoma Treated With Total Neoadjuvant Therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef] [PubMed]
- Habr-Gama, A.; Gama-Rodrigues, J.; Julião, G.P.S.; Proscurshim, I.; Sabbagh, C.; Lynn, P.B.; Perez, R.O. Local Recurrence After Complete Clinical Response and Watch and Wait in Rectal Cancer After Neoadjuvant Chemoradiation: Impact of Salvage Therapy on Local Disease Control. Int. J. Radiat. Oncol. 2014, 88, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Appelt, A.L.; Pløen, J.; Harling, H.; Jensen, F.S.; Jensen, L.H.; Jørgensen, J.C.R.; Lindebjerg, J.; Rafaelsen, S.R.; Jakobsen, A. High-dose chemoradiotherapy and watchful waiting for distal rectal cancer: A prospective observational study. Lancet Oncol. 2015, 16, 919–927. [Google Scholar] [CrossRef]
- Martens, M.H.; Maas, M.; Heijnen, L.A.; Lambregts, D.M.; Leijtens, J.W.; Stassen, L.P.; Breukink, S.O.; Hoff, C.; Belgers, E.J.; Melenhorst, J.; et al. Long-term Outcome of an Organ Preservation Program After Neoadjuvant Treat-ment for Rectal Cancer. J. Natl. Cancer Inst. 2016, 108, djw171. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Beets-Tan, R.G.; Lambregts, D.M.; Lammering, G.; Nelemans, P.J.; Engelen, S.M.; van Dam, R.M.; Jansen, R.L.; Sosef, M.; Leijtens, J.W.; et al. Wait-and-See Policy for Clinical Complete Responders After Chemoradiation for Rectal Cancer. J. Clin. Oncol. 2011, 29, 4633–4640. [Google Scholar] [CrossRef] [PubMed]
- Broek, J.J.V.D.; van der Wolf, F.S.W.; Lahaye, M.J.; Heijnen, L.A.; Meischl, C.; Heitbrink, M.A.; Schreurs, W.H. Accuracy of MRI in Restaging Locally Advanced Rectal Cancer After Preoperative Chemoradiation. Dis. Colon Rectum. 2017, 60, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Capirci, C.; Rubello, D.; Chierichetti, F.; Crepaldi, G.; Fanti, S.; Mandoliti, G.; Salviato, S.; Boni, G.; Rampin, L.; Polico, C.; et al. Long-Term Prognostic Value of 18F-FDG PET in Patients with Locally Advanced Rectal Cancer Previously Treated with Neoadjuvant Radiochemotherapy. Am. J. Roentgenol. 2006, 187, W202–W208. [Google Scholar] [CrossRef] [PubMed]
- Crimì, F.; Spolverato, G.; Lacognata, C.; Garieri, M.; Cecchin, D.; Urso, E.D.; Zucchetta, P.; Pucciarelli, S.; Pomerri, F. 18F-FDG PET/MRI for Rectal Cancer TNM Restaging After Preoperative Chemoradiotherapy: Initial Experience. Dis. Colon Rectum 2020, 63, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://abdominalradiology.org/sar-subpages/dfp-panels/ (accessed on 14 September 2022).
- Patel, U.B.; Taylor, F.; Blomqvist, L.; George, C.; Evans, H.; Tekkis, P.; Quirke, P.; Sebag-Montefiore, D.; Moran, B.; Heald, R.; et al. Magnetic Resonance Imaging–Detected Tumor Response for Locally Advanced Rectal Cancer Predicts Survival Outcomes: MERCURY Experience. J. Clin. Oncol. 2011, 29, 3753–3760. [Google Scholar] [CrossRef] [PubMed]
- Akce, M.; El-Rayes, B.F. Management of Rectal Cancer. J. Oncol. Pract. 2019, 15, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Dossa, F.; Chesney, T.R.; Acuna, S.A.; Baxter, N.N. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 501–513. [Google Scholar] [CrossRef]
- Chin, R.-I.; Roy, A.; Pedersen, K.S.; Huang, Y.; Hunt, S.R.; Glasgow, S.C.; Tan, B.R.; Wise, P.E.; Silviera, M.L.; Smith, R.K.; et al. Clinical Complete Response in Patients with Rectal Adenocarcinoma Treated with Short-Course Radiation Therapy and Nonoperative Management. Int. J. Radiat. Oncol. 2021, 112, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Capelli, G.; Campi, C.; Bao, Q.R.; Morra, F.; Lacognata, C.; Zucchetta, P.; Cecchin, D.; Pucciarelli, S.; Spolverato, G.; Crimì, F. 18F-FDG-PET/MRI texture analysis in rectal cancer after neoadjuvant chemoradiotherapy. Nucl. Med. Commun. 2022, 43, 815–822. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Tumor Characteristics | All (n = 14) | TNT (n = 7) |
|---|---|---|
| Clinical T-stage | ||
| cT1 | 0 | 0 |
| cT2 | 5 | 3 |
| cT3a | 0 | 0 |
| cT3b | 3 | 1 |
| cT3c | 2 | 1 |
| cT3d | 1 | 1 |
| cT4a | 0 | 0 |
| cT4b | 3 | 1 |
| Extramural vascular invasion | ||
| Positive | 2 | 1 |
| Negative | 12 | 6 |
| Location in rectum (from anal verge) | ||
| Low (0–4.9 cm) | 7 | 4 |
| Mid (5–9.9 cm) | 5 | 2 |
| High (10–15 cm) | 2 | 1 |
| Clinical N-stage | ||
| cN0 | 6 | 3 |
| cN1a | 1 | 0 |
| cN1b | 1 | 1 |
| cN1c | 0 | 0 |
| cN2a | 2 | 1 |
| cN2b | 4 | 2 |
| Subject # | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Initial Stage | cT3b cN1b | cT3c cN2b | cT3d cN2a | cT2 cN0 | cT4b cN1b | cT2 cN0 | cT2 cN0 |
| mrTRG—F/U #1 | |||||||
| Reader 1 | 1 | 2 | 1 | 3 | 3 | 2 | 3 |
| Reader 2 | 3 | 1 | 2 | 3 | 3 | 1 | 3 |
| Consensus | 1 | 1 | 2 | 3 | 3 | 2 | 3 |
| Tumor status (MRI)—F/U #1 | |||||||
| Reader 1 | − | − | − | + | + | − | + |
| Reader 2 | + | − | − | + | + | − | + |
| Consensus | − | − | − | + | + | − | + |
| Node status (MRI)—F/U #1 | |||||||
| Reader 1 | − | − | − | − | − | − | − |
| Reader 2 | − | − | − | − | − | − | − |
| Consensus | − | − | − | − | − | − | − |
| pmrTRG—F/U #1 | |||||||
| Reader 1 | 1 | 1 | 2 | 3 | 3 | 1 | 3 |
| Reader 2 | 3 | 2 | 2 | 3 | 3 | 1 | 3 |
| Consensus | 1 | 2 | 2 | 3 | 3 | 1 | 3 |
| Tumor status (PET/MRI)—F/U #1 | |||||||
| Reader 1 | − | − | + | + | + | − | + |
| Reader 2 | + | + | + | + | + | − | + |
| Consensus | − | + | + | + | + | − | + |
| Node status (PET/MRI)—F/U #1 | |||||||
| Reader 1 | − | − | − | − | − | − | − |
| Reader 2 | − | − | − | − | − | − | − |
| Consensus | − | − | − | − | − | − | − |
| Added value of PET—F/U #1 | |||||||
| Reader 1 | Y | Y | Y | N | Y | Y | Y |
| Reader 2 | Y | Y | Y | N | Y | Y | Y |
| Consensus | Y | Y | Y | N | Y | Y | Y |
| Endoscopy +/− biopsy—F/U #1 | − | + | − | − | + | − | + |
| Reference standard | F/U * | Path. | Path. | Path. | Path. | F/U * | Path. |
| Reference stage (post-TNT) | cT0 cN0 | ypT2 ypN0 | ypT2 ypN0 | ypT1 ypN0 | ypT2 ypN0 | cT0 cN0 | ypT2 ypN0 |
| Index test adjudication—F/U #1 | |||||||
| Endoscopy +/− biopsy | TN | TP | FN | FN | TP | TN | TP |
| mrTRG consensus | TN | FN | FN | TP | TP | TN | TP |
| pmrTRG consensus | TN | TP | TP | TP | TP | TN | TP |
| Subject # | 1 | 6 |
|---|---|---|
| Initial Stage | cT3b cN1b | cT2 cN0 |
| mrTRG—F/U #2 | ||
| Reader 1 | 2 | 2 |
| Reader 2 | 2 | 1 |
| Consensus | 2 | 1 |
| pmrTRG—F/U #2 | ||
| Reader 1 | 1 | 1 |
| Reader 2 | 1 | 1 |
| Consensus | 1 | 1 |
| Added value of PET—F/U #2 | ||
| Reader 1 | Y | Y |
| Reader 2 | Y | Y |
| Consensus | Y | Y |
| Endoscopy +/− biopsy—F/U #2 | − | − |
| mrTRG—F/U #3 | ||
| Reader 1 | 2 | 2 |
| Reader 2 | 2 | 1 |
| Consensus | 2 | 1 |
| pmrTRG—F/U #3 | ||
| Reader 1 | 1 | 1 |
| Reader 2 | 1 | 1 |
| Consensus | 1 | 1 |
| Added value of PET—F/U #3 | ||
| Reader 1 | Y | Y |
| Reader 2 | Y | Y |
| Consensus | Y | Y |
| Endoscopy +/− biopsy—F/U #3 | − | − |
| Subject # | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Initial Stage | cT3b cN1b | cT3c cN2b | cT3d cN2a | cT2 cN0 | cT4b cN1b | cT2 cN0 | cT2 cN0 |
| Maximum SUV—initial staging | 21.2 | 15.7 | 14.3 | 21.9 | 20.3 | 4.2 | 18.9 |
| Maximum SUV—F/U #1 | 2.9 | 4.7 | 3.6 | 2.0 | 7.2 | 1.9 | 2.0 |
| ∆ SUV (absolute) | −18.3 | −11.0 | −10.7 | −19.9 | −13.1 | −2.3 | −16.9 |
| ∆ SUV (relative) | −86% | −70% | −75% | −91% | −65% | −55% | −89% |
| Reference standard | F/U * | Path. | Path. | Path. | Path. | F/U * | Path. |
| Reference stage (post-TNT) | cT0 cN0 | ypT2 ypN0 | ypT2 ypN0 | ypT1 ypN0 | ypT2 ypN0 | cT0 cN0 | ypT2 ypN0 |
| mrTRG | R2: 1 | R2: 2 | R2: 3 | R2: 4 | R2: 5 | |||
| R1: 1 | 0 | 1 | 1 | 0 | 0 | |||
| R1: 2 | 2 | 0 | 0 | 0 | 0 | |||
| R1: 3 | 0 | 0 | 3 | 0 | 0 | |||
| R1: 4 | 0 | 0 | 0 | 0 | 0 | |||
| R1: 5 | 0 | 0 | 0 | 0 | 0 | |||
| kappa = 0.10 | ||||||||
| mrTRG | R2: 1–2 | R2: 3–5 | ||||||
| R1: 1-2 | 3 | 1 | ||||||
| R1: 3-5 | 0 | 3 | ||||||
| kappa = 0.72 | ||||||||
| pmrTRG | R2: 1 | R2: 2 | R2: 3 | |||||
| R1: 1 | 1 | 1 | 1 | |||||
| R1: 2 | 0 | 1 | 0 | |||||
| R1: 3 | 0 | 0 | 3 | |||||
| kappa = 0.56 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ince, S.; Itani, M.; Henke, L.E.; Smith, R.K.; Wise, P.E.; Mutch, M.G.; Glasgow, S.C.; Silviera, M.L.; Pedersen, K.S.; Hunt, S.R.; et al. FDG-PET/MRI for Nonoperative Management of Rectal Cancer: A Prospective Pilot Study. Tomography 2022, 8, 2723-2734. https://doi.org/10.3390/tomography8060227
Ince S, Itani M, Henke LE, Smith RK, Wise PE, Mutch MG, Glasgow SC, Silviera ML, Pedersen KS, Hunt SR, et al. FDG-PET/MRI for Nonoperative Management of Rectal Cancer: A Prospective Pilot Study. Tomography. 2022; 8(6):2723-2734. https://doi.org/10.3390/tomography8060227
Chicago/Turabian StyleInce, Semra, Malak Itani, Lauren E. Henke, Radhika K. Smith, Paul E. Wise, Matthew G. Mutch, Sean C. Glasgow, Matthew L. Silviera, Katrina S. Pedersen, Steven R. Hunt, and et al. 2022. "FDG-PET/MRI for Nonoperative Management of Rectal Cancer: A Prospective Pilot Study" Tomography 8, no. 6: 2723-2734. https://doi.org/10.3390/tomography8060227
APA StyleInce, S., Itani, M., Henke, L. E., Smith, R. K., Wise, P. E., Mutch, M. G., Glasgow, S. C., Silviera, M. L., Pedersen, K. S., Hunt, S. R., Kim, H., & Fraum, T. J. (2022). FDG-PET/MRI for Nonoperative Management of Rectal Cancer: A Prospective Pilot Study. Tomography, 8(6), 2723-2734. https://doi.org/10.3390/tomography8060227