
[18F]fluciclovine vs. [18F]fluorocholine Positron Emission Tomography/Computed Tomography: A Head-to-Head Comparison for Early Detection of Biochemical Recurrence in Prostate Cancer Patients
 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Imaging Protocol and Analysis
2.3. Image Analysis
2.4. Data Analysis
2.5. Statistical Analysis
3. Results
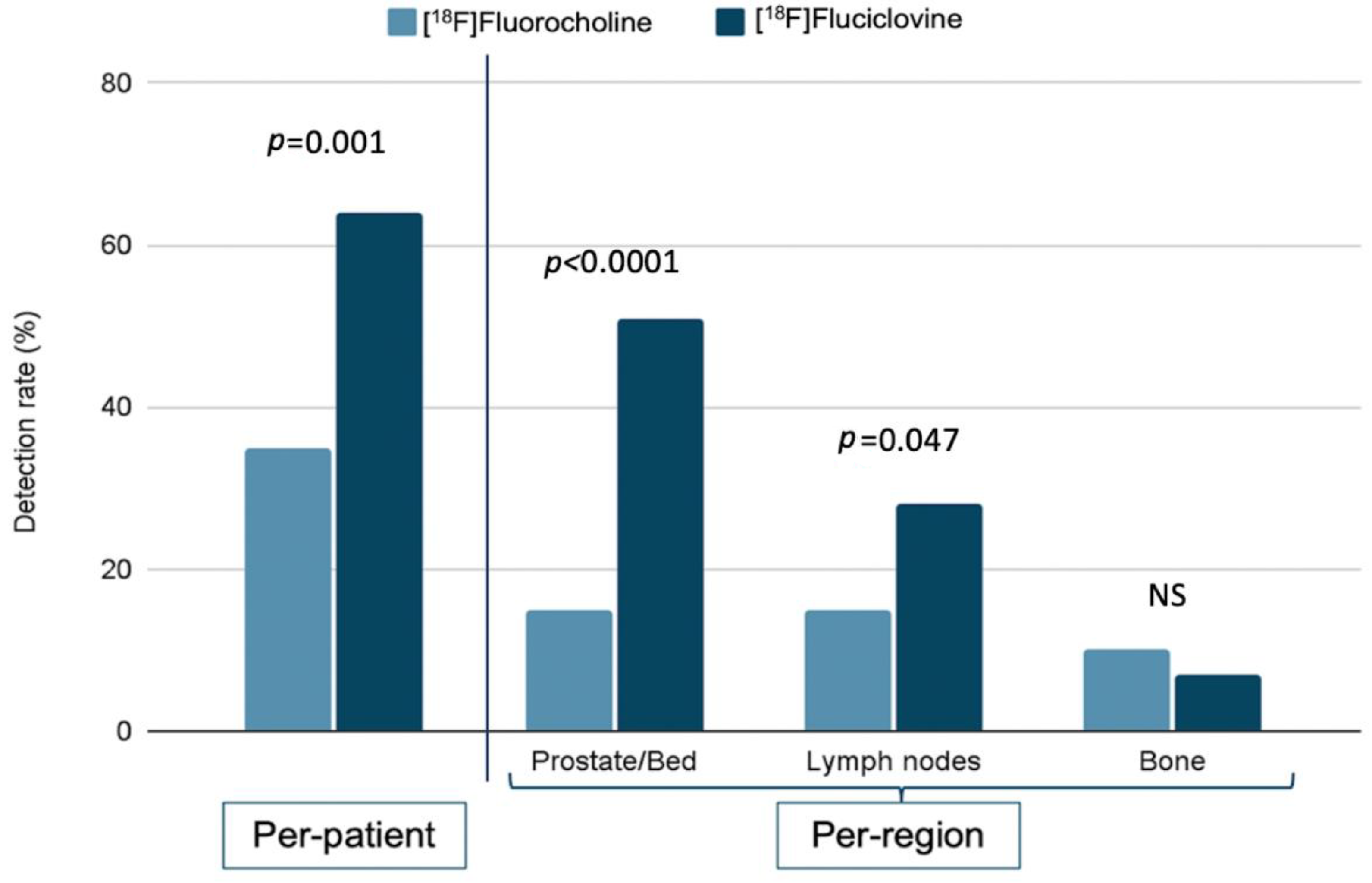
3.1. Per-Patient and Per-Region Detection Rate
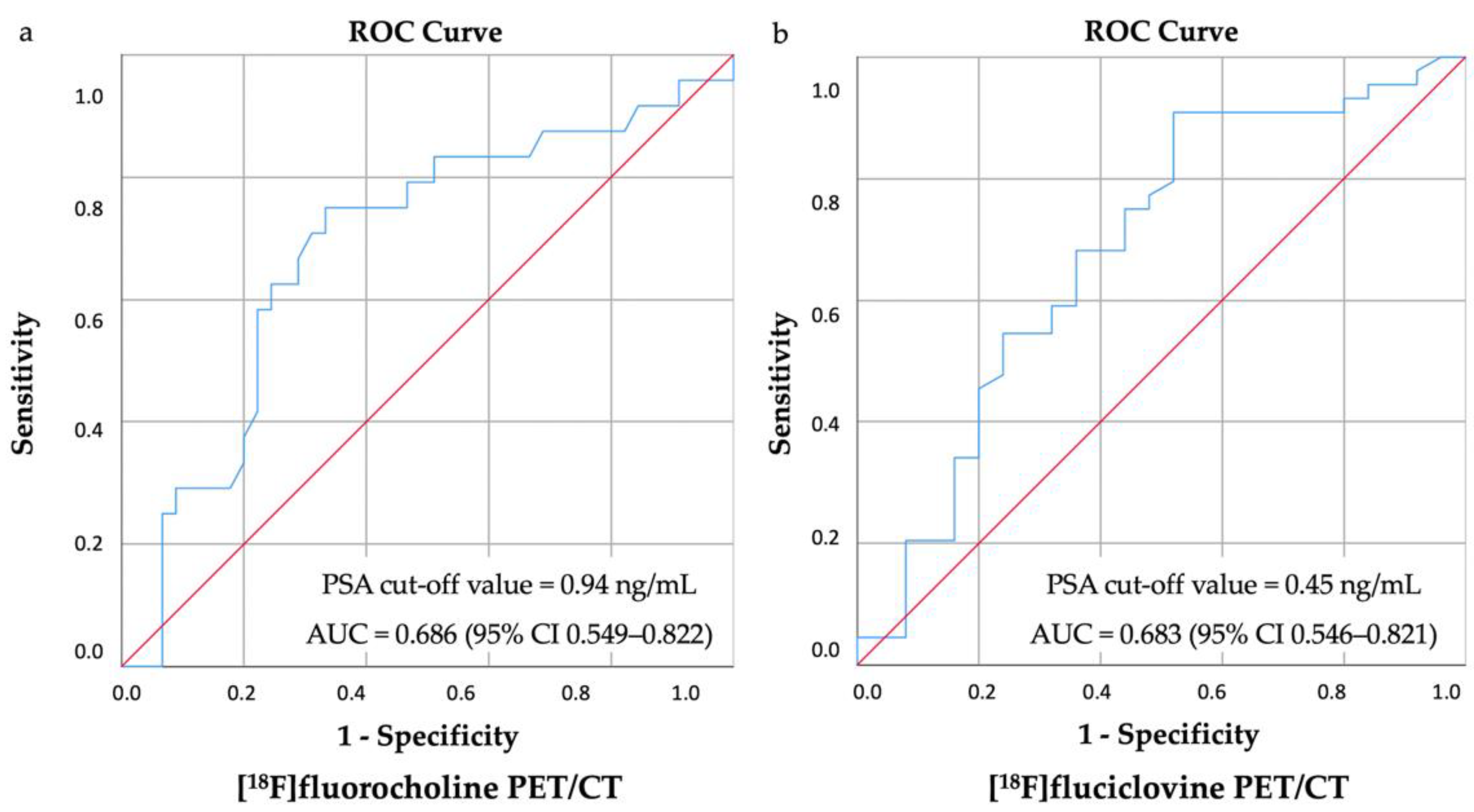
3.2. Biochemical Parameters
3.3. Clinical and Histological Parameters
3.4. Recurrent Lesions’ Number: A Subanalysis
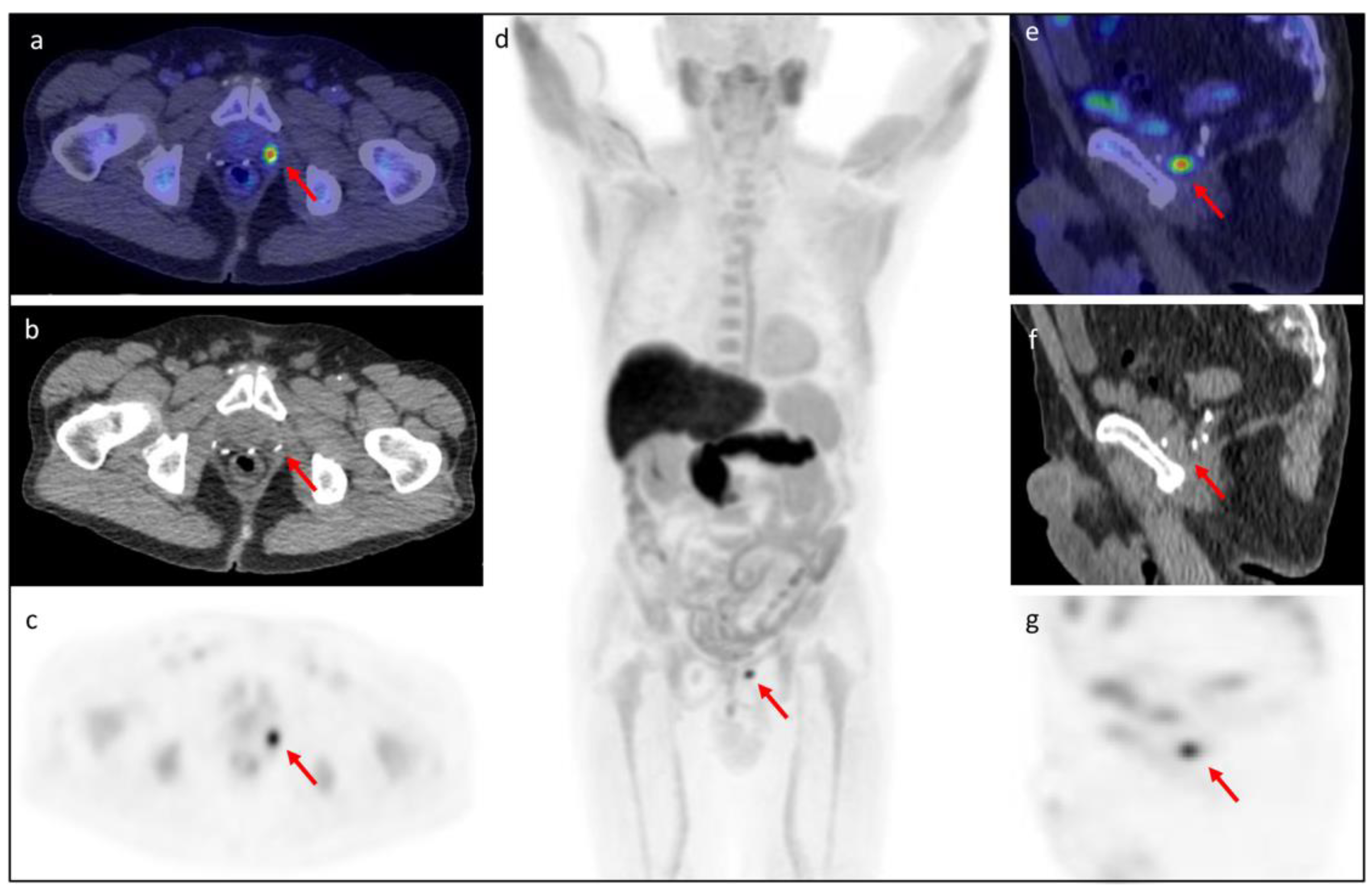
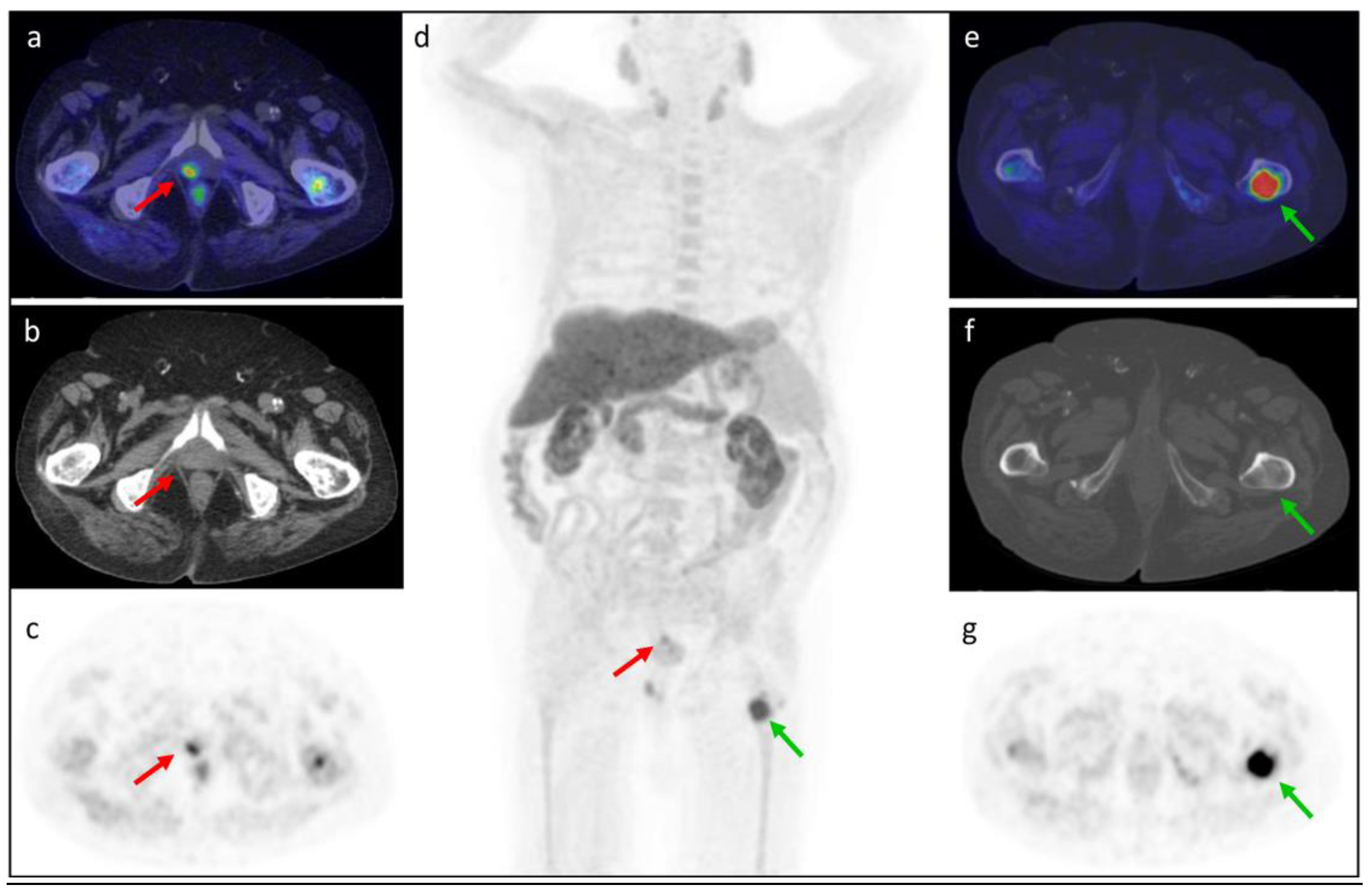
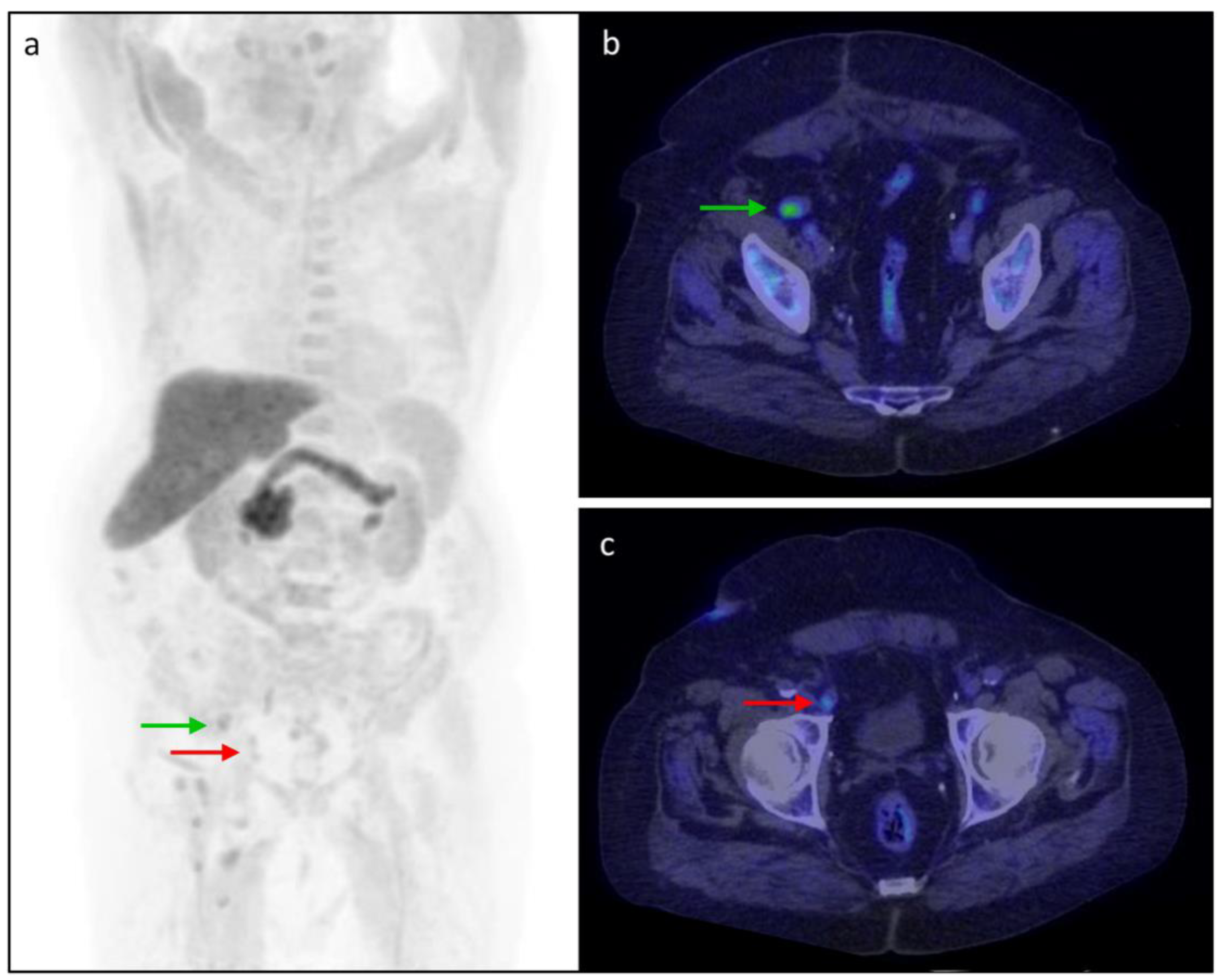
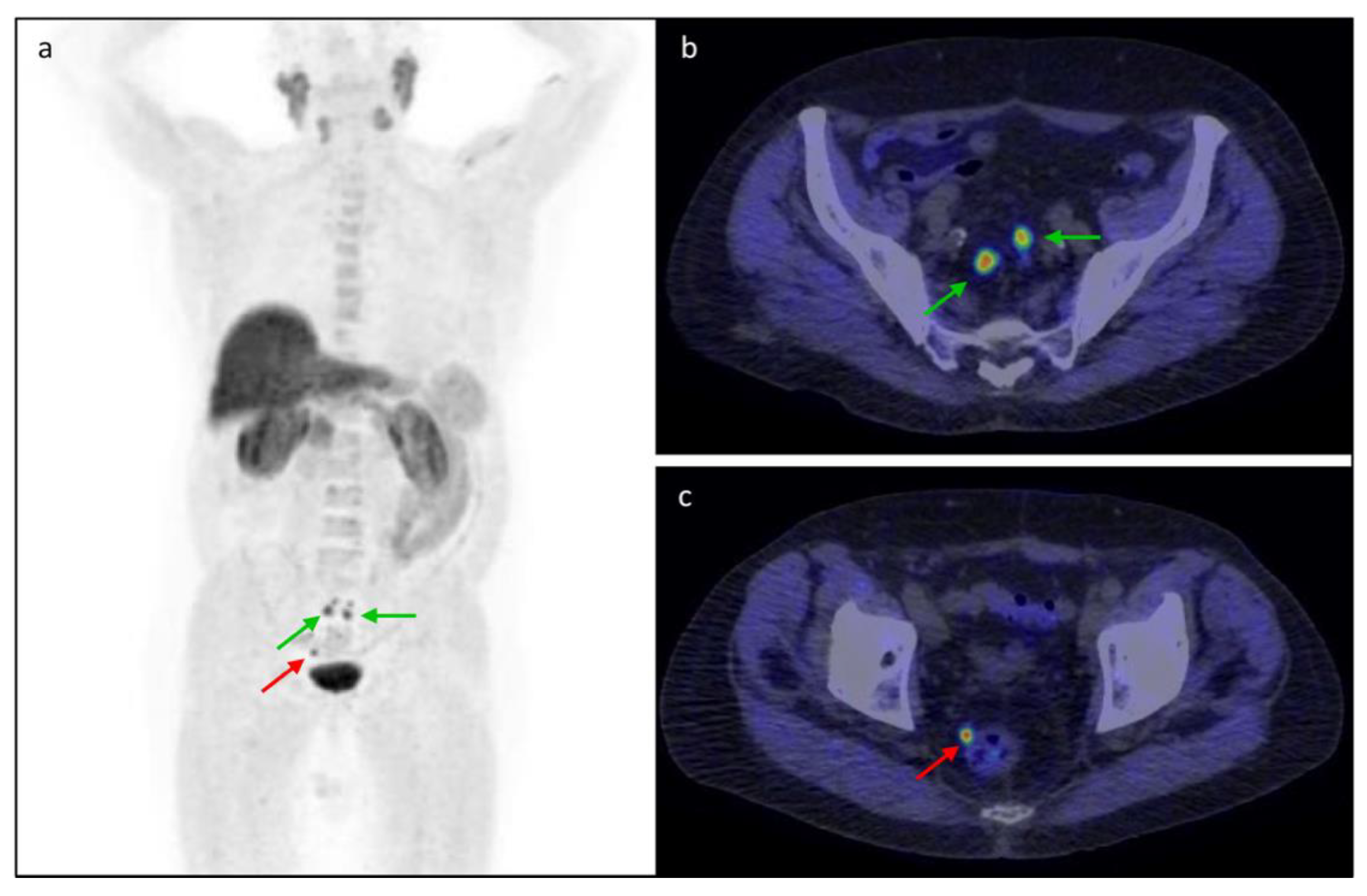
3.5. Clinical Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, A.; Bellmunt, J.; Bolla, M.; Joniau, S.; Mason, M.; Matveev, V.; Mottet, N.; Schmid, H.P.; Van Der Kwast, T.; Wiegel, T.; et al. EAU guidelines on prostate cancer. Part 1: Screening, diagnosis, and treatment of clinically localised disease. Eur. Urol. 2011, 59, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, A.J.; Scardino, P.T.; Eastham, J.A.; Bianco, F.J.; Dotan, Z.A.; Fearn, P.A.; Kattan, M.W. Preoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J. Natl. Cancer Inst. 2006, 98, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Triviño-Ibáñez, E.M.; Puche-Sanz, I.; Gómez-Río, M.; Cózar Olmo, J.M.; Llamas-Elvira, J.M.; Rodríguez-Fernández, A. Usefulness of 18F-fluorocoline PET/CT in prostate cancer patients with biochemical recurrence: Influence of PSA kinetics and hormone therapy. Med. Clin. 2019, 153, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; van der Kwast, T.H.; Lam, T.B.; et al. EAU-EANM-ESTRO-ESUR-ISUP_SIOG Guidelines on Prostate Cancer 2022. Eur. Urol. 2022, 79, 243–262. [Google Scholar] [CrossRef]
- Altini, C.; Asabella, A.N.; Lavelli, V.; Bianco, G.; Ungaro, A.; Pisani, A.; Merenda, N.; Ferrari, C.; Rubini, G. Role of 18F-FDG PET/CT in comparison with CECT for whole-body assessment of patients with esophageal cancer. Recent. Prog. Med. 2019, 110, 144–150. [Google Scholar] [CrossRef]
- Jadvar, H. Is There Use for FDG-PET in Prostate Cancer? Semin. Nucl. Med. 2016, 46, 502–506. [Google Scholar] [CrossRef]
- Fanti, S.; Minozzi, S.; Castellucci, P.; Balduzzi, S.; Herrmann, K.; Krause, B.J.; Oyen, W.; Chiti, A. PET/CT with (11)C-choline for evaluation of prostate cancer patients with biochemical recurrence: Meta-analysis and critical review of available data. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 55–69. [Google Scholar] [CrossRef]
- Nappi, A.G.; Ferrari, C.; Mammucci, P.; Rubini, D.; Lavelli, V.; Sardaro, A.; Pisani, A.R.; Rubini, G. [18F]Fluciclovine PET/CT Improves the Clinical Management of Early Recurrence Prostate Cancer Patients. Cancers 2022, 14, 1461. [Google Scholar] [CrossRef]
- García Garzón, J.R.; de Arcocha Torres, M.; Delgado-Bolton, R.; Ceci, F.; Alvarez Ruiz, S.; Orcajo Rincón, J.; Caresia Aróztegui, A.P.; García Velloso, M.J.; García Vicente, A.M. 68Ga-PSMA PET/CT in prostate cancer. Rev. Esp. Med. Nucl. Imagen Mol. 2018, 37, 130–138. [Google Scholar] [CrossRef]
- Zanoni, L.; Mei, R.; Bianchi, L.; Giunchi, F.; Maltoni, L.; Pultrone, C.V.; Nanni, C.; Bossert, I.; Matti, A.; Schiavina, R.; et al. The Role of [18 F]Fluciclovine PET/CT in the Characterization of High-Risk Primary Prostate Cancer: Comparison with [11C]Choline PET/CT and Histopathological Analysis. Cancers 2021, 13, 1575. [Google Scholar] [CrossRef]
- Memorial Sloan Kettering Cancer Center. Prostate Cancer Nomograms: PSA Doubling Time. Available online: https://www.mskcc.org/nomograms/prostate/psa_doubling_time (accessed on 30 August 2022).
- Tilki, D.; Preisser, F.; Graefen, M.; Huland, H.; Pompe, R.S. External Validation of the European Association of Urology Biochemical Recurrence Risk Groups to Predict Metastasis and Mortality After Radical Prostatectomy in a European Cohort. Eur. Urol. 2019, 75, 896–900. [Google Scholar] [CrossRef]
- Nanni, C.; Zanoni, L.; Bach-Gansmo, T.; Minn, H.; Willoch, F.; Bogsrud, T.V.; Edward, E.P.; Savir-Baruch, B.; Teoh, E.; Ingram, F.; et al. [18 F]Fluciclovine PET/CT: Joint EANM and SNMMI procedure guideline for prostate cancer imaging-version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 579–591. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Dreicer, R.; Paciorek, A.; Carroll, P.R.; Konety, B. A model that predicts the probability of positive imaging in prostate cancer cases with biochemical failure after initial definitive local therapy. J. Urol. 2008, 179, 906–910. [Google Scholar] [CrossRef]
- Schuster, D.M.; Nanni, C.; Fanti, S.; Oka, S.; Okudaira, H.; Inoue, Y.; Sörensen, J.; Owenius, R.; Choyke, P.; Turkbey, B.; et al. Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid: Physiologic uptake patterns, incidental findings, and variants that may simulate disease. J. Nucl. Med. 2014, 55, 1986–1992. [Google Scholar] [CrossRef]
- Rouvière, O.; Vitry, T.; Lyonnet, D. Imaging of prostate cancer local recurrences: Why and how? Eur. Radiol. 2010, 20, 1254–1266. [Google Scholar] [CrossRef]
- Treglia, G.; Ceriani, L.; Sadeghi, R.; Giovacchini, G.; Giovanella, L. Relationship between prostate-specific antigen kinetics and detection rate of radiolabelled choline PET/CT in restaging prostate cancer patients: A meta-analysis. Clin. Chem. Lab. Med. 2014, 52, 725–733. [Google Scholar] [CrossRef]
- Evangelista, L.; Zattoni, F.; Guttilla, A.; Saladini, G.; Zattoni, F.; Colletti, P.M.; Rubello, D. Choline PET or PET/CT and biochemical relapse of prostate cancer: A systematic review and meta-analysis. Clin. Nucl. Med. 2013, 38, 305–314. [Google Scholar] [CrossRef]
- Picchio, M.; Spinapolice, E.G.; Fallanca, F.; Crivellaro, C.; Giovacchini, G.; Gianolli, L.; Messa, C. [11C]Choline PET/CT detection of bone metastases in patients with PSA progression after primary treatment for prostate cancer: Comparison with bone scintigraphy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 13–26. [Google Scholar] [CrossRef]
- Castellucci, P.; Ceci, F.; Graziani, T.; Schiavina, R.; Brunocilla, E.; Mazzarotto, R.; Pettinato, C.; Celli, M.; Lodi, F.; Fanti, S. Early biochemical relapse after radical prostatectomy: Which prostate cancer patients may benefit from a restaging 11C-Choline PET/CT scan before salvage radiation therapy? J. Nucl. Med. 2014, 55, 1424–1429. [Google Scholar] [CrossRef]
- Bach-Gansmo, T.; Nanni, C.; Nieh, P.T.; Zanoni, L.; Bogsrud, T.V.; Sletten, H.; Korsan, K.A.; Kieboom, J.; Tade, F.I.; Odewole, O.; et al. Multisite Experience of the Safety, Detection Rate and Diagnostic Performance of Fluciclovine (18 F) Positron Emission Tomography/Computerized Tomography Imaging in the Staging of Biochemically Recurrent Prostate Cancer. J. Urol. 2017, 197, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Dreyfuss, A.D.; Ahn, G.S.; Barsky, A.R.; Gillman, J.A.; Vapiwala, N.; Pantel, A.R. 18F-Fluciclovine PET/CT in Therapeutic Decision Making for Prostate Cancer: A Large Single-Center Practice-Based Analysis. Clin. Nucl. Med. 2021, 46, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.; Abiodun-Ojo, O.A.; Jani, A.B.; Schuster, D.M. Clinical utility of 18F-Fluciclovine PET/CT in recurrent prostate cancer with very low (≤0.3 ng/mL) prostate-specific antigen levels. Am. J. Nucl. Med. Mol. Imaging 2021, 11, 406–414. [Google Scholar] [PubMed]
- Filippi, L.; Bagni, O.; Crisafulli, C.; Cerio, I.; Brunotti, G.; Chiaravalloti, A.; Schillaci, O.; Dore, F. Detection Rate and Clinical Impact of PET/CT with 18F-FACBC in Patients with Biochemical Recurrence of Prostate Cancer: A Retrospective Bicentric Study. Biomedicines 2022, 10, 177. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, J.M.; Martin, C.R.; Dechet, C.; Morton, K.; Evans, D.; Ambrose, J.; Maughan, B.L.; O’Neil, B.; Lowrance, W. 18F-fluciclovine PET CT detection of biochemical recurrent prostate cancer at specific PSA thresholds after definitive treatment. Urol. Oncol. 2020, 38, 636.e1–636.e6. [Google Scholar] [CrossRef]
- Wang, Y.; Chow, D.Z.; Ebert, E.; Tajmir, S.; Scott, J.A.; Palmer, E.L. Utility of 18F-Fluciclovine PET/CT for Detecting Prostate Cancer Recurrence in Patients with Low (<1 ng/mL) or Very Low (<0.3 ng/mL) Prostate-Specific Antigen Levels. Am. J. Roentgenol. 2020, 215, 997–1001. [Google Scholar] [CrossRef]
- Nanni, C.; Schiavina, R.; Boschi, S.; Ambrosini, V.; Pettinato, C.; Brunocilla, E.; Martorana, G.; Fanti, S. Comparison of 18F-FACBC and 11C-choline PET/CT in patients with radically treated prostate cancer and biochemical relapse: Preliminary results. Eur. J. Nucl. Med. Mol. Imaging 2013, 40 (Suppl. S1), 11–17. [Google Scholar] [CrossRef]
- Nanni, C.; Schiavina, R.; Brunocilla, E.; Borghesi, M.; Ambrosini, V.; Zanoni, L.; Gentile, G.; Vagnoni, V.; Romagnoli, D.; Martorana, G.; et al. 18F-FACBC compared with 11C-choline PET/CT in patients with biochemical relapse after radical prostatectomy: A prospective study in 28 patients. Clin. Genitourin. Cancer 2014, 12, 106–110. [Google Scholar] [CrossRef]
- Nanni, C.; Schiavina, R.; Brunocilla, E.; Boschi, S.; Borghesi, M.; Zanoni, L.; Pettinato, C.; Martorana, G.; Fanti, S. 18F-Fluciclovine PET/CT for the Detection of Prostate Cancer Relapse: A Comparison to 11C-Choline PET/CT. Clin. Nucl. Med. 2015, 40, e386–e391. [Google Scholar] [CrossRef]
- Wang, R.; Shen, G.; Huang, M.; Tian, R. The Diagnostic Role of 18F-Choline, 18F-Fluciclovine and 18F-PSMA PET/CT in the Detection of Prostate Cancer with Biochemical Recurrence: A Meta-Analysis. Front. Oncol. 2021, 11, 684629. [Google Scholar] [CrossRef]
- Ma, W.; Mao, J.; Yang, J.; Wang, T.; Zhao, Z.H. Comparing the diagnostic performance of radiotracers in prostate cancer biochemical recurrence: A systematic review and meta-analysis. Eur. Radiol. 2022. [Google Scholar] [CrossRef]
- Pernthaler, B.; Kvaternik, H.; Aigner, R.M. A Prospective Head-to-Head Comparison of 18F-Fluciclovine with 68Ga-PSMA-11 in Biochemical Recurrence of Prostate Cancer in PET/CT: A Special Aspect in Imaging Local Recurrence: Reply. Clin. Nucl. Med. 2020, 45, 498–499. [Google Scholar] [CrossRef]
- Tsechelidis, I.; Vrachimis, A. PSMA PET in imaging prostate cancer. Front. Oncol. 2022, 12, 831429. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | ||||
|---|---|---|---|---|
| Variables | Total (n = 138) | [18F]fluorocholine (n = 69) | [18F]fluciclovine (n = 69) | p-Value |
| Age—y | ||||
| Mean ± SD | 71.22 ± 6.72 | 71.80 ± 6.46 | 70.65 ± 6.96 | 0.705 |
| Median (Range) | 71.50 (50–87) | 72 (52–87) | 71 (50–83) | |
| PSA—ng/mL | ||||
| Mean ± SD | 1.20 ± 1.17 | 1.25 ± 1.22 | 1.17 ± 1.11 | 0.244 |
| PSA value—no. (%) | ||||
| <0.5 ng/mL | 49 (36%) | 25 (36%) | 23 (34%) | 0.508 |
| 0.5–1 ng/mL | 36 (26%) | 16 (23%) | 21 (30%) | |
| >1 ng/mL | 53 (38%) | 28 (41%) | 25 (36%) | |
| PSAdt—months | ||||
| Mean ± SD | 37.22 ± 221.03 | 12.92 ± 13.70 | 50.14 ± 273.70 | 0.131 |
| Median (Range) | 10.70 (0.10–2241.10) | 8.20 (0.10–70.90) | 10.75 (1.10–2241.10) | |
| PSAdt—no. (%) | ||||
| ≤12 months | 58 (51%) | 22 (48%) | 36 (53%) | 0.356 |
| >12 months | 56 (49%) | 24 (52%) | 32 (47%) | |
| GS—no. (%) | ||||
| <8 | 96 (70%) | 49 (71%) | 47 (68%) | 0.427 |
| ≥8 | 42 (30%) | 20 (29%) | 22 (32%) | |
| EAU BCR risk group—no. (%) | ||||
| Low | 65 (47%) | 38 (55%) | 27 (39%) | 0.060 |
| High | 73 (53%) | 31 (45%) | 42 (61%) | |
| Primary Treatment—no. (%) | ||||
| Prostatectomy Only | 77 (58%) | 42 (61%) | 35 (55%) | 0.105 |
| Radiotherapy Only | 13 (10%) | 9 (13%) | 4 (6%) | |
| Prostatectomy + Radiotherapy | 43 (32%) | 18 (26%) | 25 (39%) | |
| Ongoing HT—no. (%) | ||||
| Yes | 29 (21%) | 17 (25%) | 12 (17%) | 0.202 |
| No | 109 (79%) | 52 (75%) | 57 (83%) | |
| Per-Patient Analysis | |||
| PSA level | [18F]fluorocholine DR | [18F]fluciclovine DR | p-value |
| <0.5 ng/mL | 5/26 (19%) | 10/23 (43%) | 0.063 |
| 0.5–1 ng/mL | 4/15 (27%) | 14/21 (67%) | 0.018 |
| >1 ng/mL | 15/28 (54%) | 20/25 (80%) | 0.040 |
| Per-Region Analysis: Prostate/Prostate bed | |||
| PSA level | [18F]fluorocholine DR | [18F]fluciclovine DR | p-value |
| <0.5 ng/mL | 4/26 (15%) | 7/23 (30%) | 0.180 |
| 0.5–1 ng/mL | 3/15 (20%) | 11/21 (52%) | 0.049 |
| >1 ng/mL | 3/28 (11%) | 17/25 (68%) | <0.0001 |
| Per-Region Analysis: Lymph Node | |||
| PSA level | [18F]fluorocholine DR | [18F]fluciclovine DR | p-value |
| <0.5 ng/mL | 1/26 (4%) | 5/23 (22%) | 0.057 |
| 0.5–1 ng/mL | 1/15 (7%) | 5/21 (24%) | 0.174 |
| >1 ng/mL | 7/28 (25%) | 9/25 (36%) | 0.284 |
| Per-Region Analysis: Bone | |||
| PSA level | [18F]fluorocholine DR | [18F]fluciclovine DR | p-value |
| <0.5 ng/mL | 1/26 (4%) | 1/23 (4%) | 0.724 |
| 0.5–1 ng/mL | 0/15 (0%) | 2/21 (10%) | 0.219 |
| >1 ng/mL | 6/28 (21%) | 2/25 (8%) | 0.164 |
| Per-Patient Analysis | |||
|---|---|---|---|
| PSAdoubling time | [18F]fluorocholine DR | [18F]fluciclovine DR | p-value |
| ≤12 months | 12/22 (55%) | 22/36 (61%) | 0.412 |
| >12 months | 5/24 (21%) | 21/32 (66%) | 0.001 |
| Per-Patient Analysis | |||
|---|---|---|---|
| Gleason Score | [18F]fluorocholine DR | [18F]fluciclovine DR | p-value |
| <8 | 14/49 (29%) | 30/46 (65%) | <0.0001 |
| ≥8 | 10/20 (50%) | 14/23 (61%) | 0.342 |
| EAU BCR Risk Group | |||
| Low | 9/36 (25%) | 18/26 (69%) | 0.001 |
| High | 15/33 (45%) | 26/43 (60%) | 0.143 |
| Ongoing HT | |||
| Yes | 9/17 (53%) | 7/12 (58%) | 0.537 |
| No | 15/52 (29%) | 37/57 (65%) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, C.; Mammucci, P.; Lavelli, V.; Pisani, A.R.; Nappi, A.G.; Rubini, D.; Sardaro, A.; Rubini, G. [18F]fluciclovine vs. [18F]fluorocholine Positron Emission Tomography/Computed Tomography: A Head-to-Head Comparison for Early Detection of Biochemical Recurrence in Prostate Cancer Patients. Tomography 2022, 8, 2709-2722. https://doi.org/10.3390/tomography8060226
Ferrari C, Mammucci P, Lavelli V, Pisani AR, Nappi AG, Rubini D, Sardaro A, Rubini G. [18F]fluciclovine vs. [18F]fluorocholine Positron Emission Tomography/Computed Tomography: A Head-to-Head Comparison for Early Detection of Biochemical Recurrence in Prostate Cancer Patients. Tomography. 2022; 8(6):2709-2722. https://doi.org/10.3390/tomography8060226
Chicago/Turabian StyleFerrari, Cristina, Paolo Mammucci, Valentina Lavelli, Antonio Rosario Pisani, Anna Giulia Nappi, Dino Rubini, Angela Sardaro, and Giuseppe Rubini. 2022. "[18F]fluciclovine vs. [18F]fluorocholine Positron Emission Tomography/Computed Tomography: A Head-to-Head Comparison for Early Detection of Biochemical Recurrence in Prostate Cancer Patients" Tomography 8, no. 6: 2709-2722. https://doi.org/10.3390/tomography8060226
APA StyleFerrari, C., Mammucci, P., Lavelli, V., Pisani, A. R., Nappi, A. G., Rubini, D., Sardaro, A., & Rubini, G. (2022). [18F]fluciclovine vs. [18F]fluorocholine Positron Emission Tomography/Computed Tomography: A Head-to-Head Comparison for Early Detection of Biochemical Recurrence in Prostate Cancer Patients. Tomography, 8(6), 2709-2722. https://doi.org/10.3390/tomography8060226