
Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
- Indications and contraindications of CSIs;
- Planning and designing CSIs;
- Surgical protocol and associated complications;
- Prosthetic protocol and associated complications;
- Peri-implant supportive therapy;
- General recommendations and future perspectives.
3. Results
3.1. Literature Review
3.2. Clinical Guidelines Based on the Results of the Consensus Meeting
- 1.
- Indications and contraindications of CSIs.
- 1.1.
- CSIs indications:
- 1.1.1.
- Patients who present insufficient bone to place standard dental implants;
- 1.1.2.
- When complex regenerative techniques cannot be performed or are not accepted by the patients because of the associated morbidity;
- 1.1.3.
- Patients who do not tolerate removable prostheses or when these cannot be made;
- 1.1.4.
- CSIs might be considered as an alternative to zygomatic implants when a fixed prosthesis is required;
- 1.1.5.
- CSIs should be used with caution in cases of partial edentulism since the available clinical data are limited in these situations (EO).
- 1.2.
- CSI contraindications:
- 1.2.1.
- Patients with systemic pathologies that contraindicate the surgical procedure;
- 1.2.2.
- Patients under treatment with therapies or drugs that contraindicate the surgical procedure.
- 2.
- Planning and designing CSIs.
- 2.1.
- A thorough diagnosis is paramount for adequate treatment planning. High-resolution computer tomography (CT) following the instructions provided by the CSI manufacturer is mandatory. Cone-beam computer tomography (CBCT) is not suitable for designing CSIs (EO);
- 2.2.
- A proper diagnosis should include the occlusal position, a standard tessellation language (STL) file with the intraoral anatomy, and a CT scan;
- 2.3.
- Passive fit of the CSI to the surrounding bone is critical since this is a custom-made device;
- 2.4.
- Since the most frequent complication is CSI exposure, a polished titanium surface is recommended (EO);
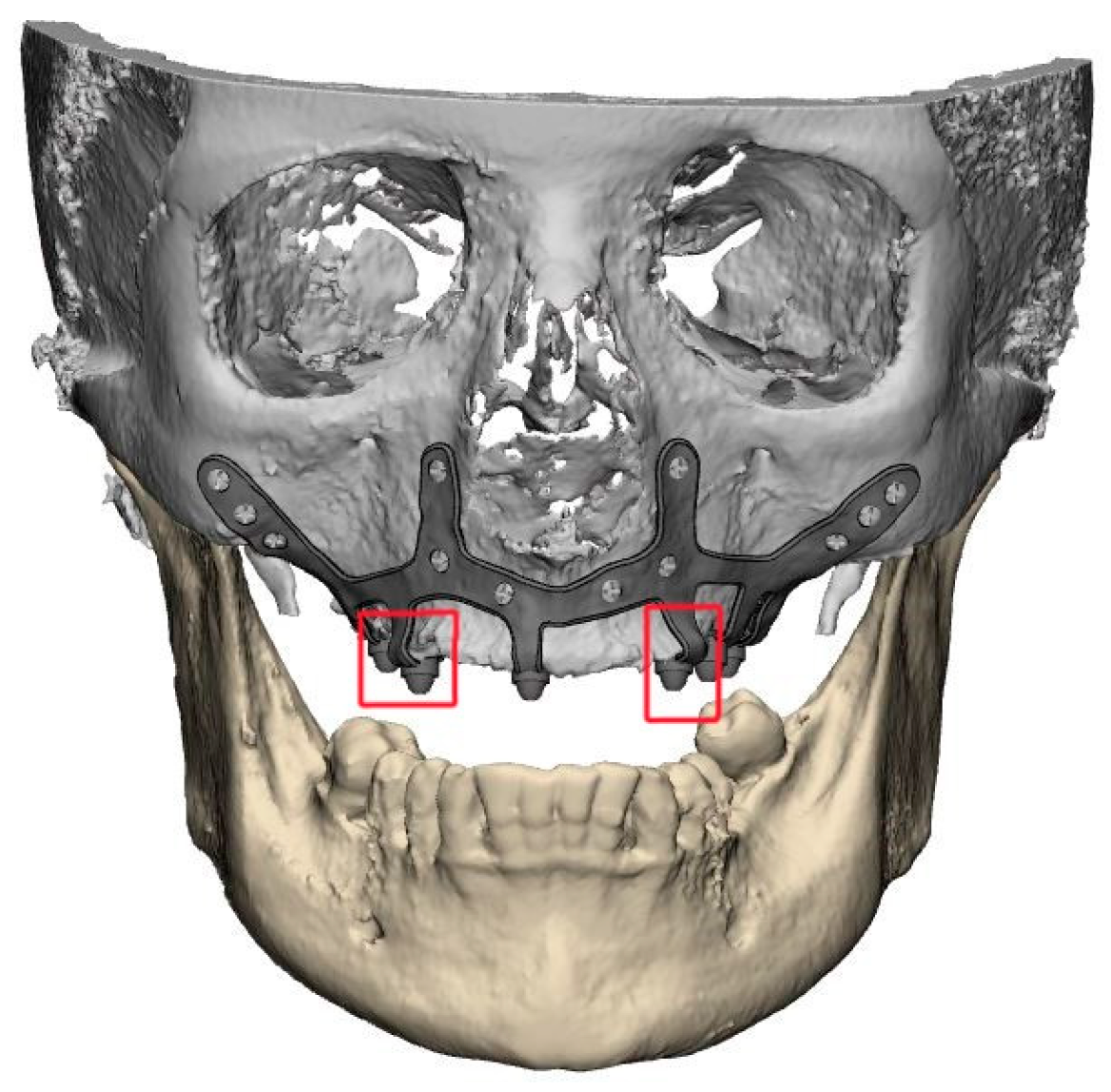
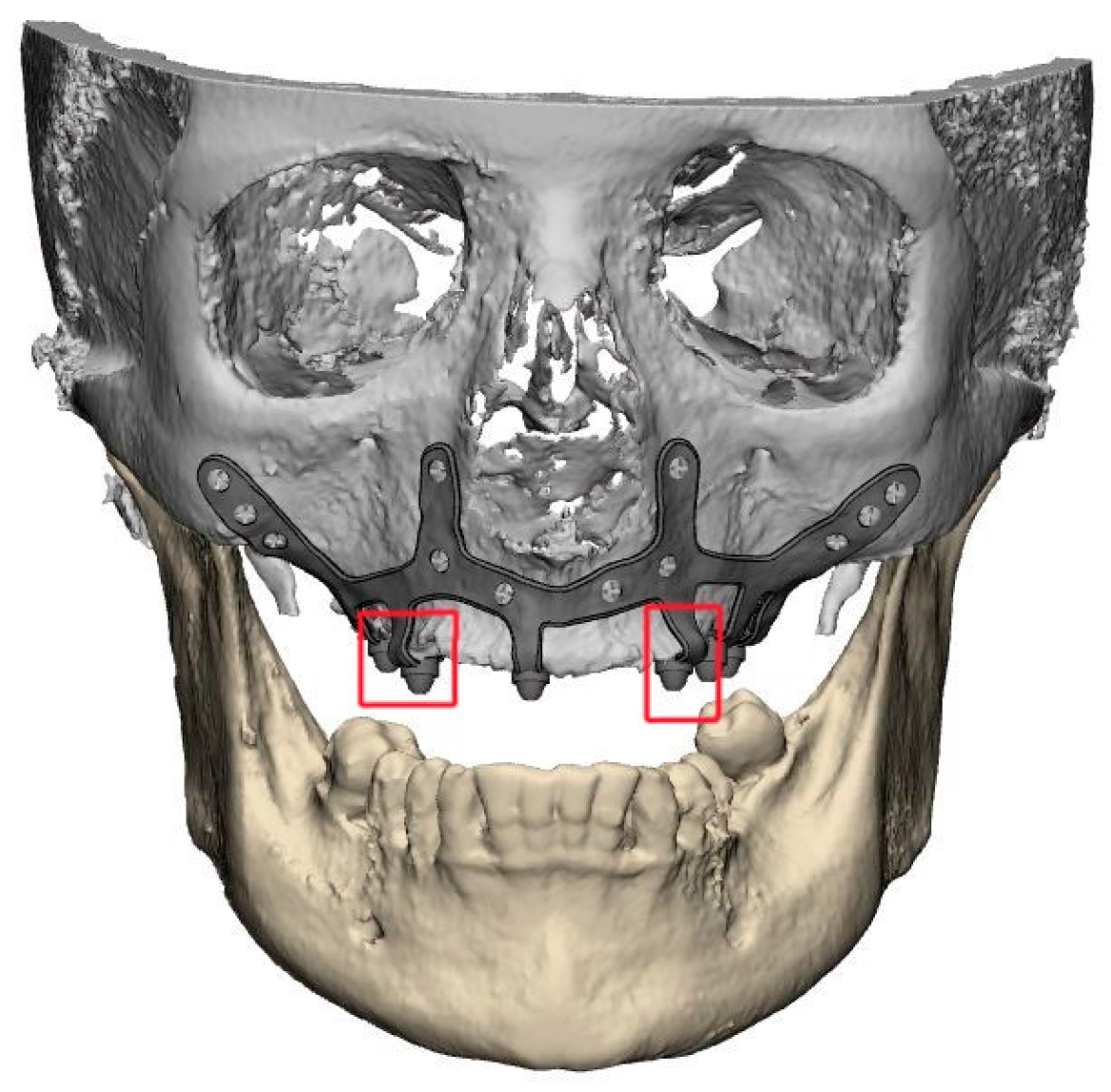
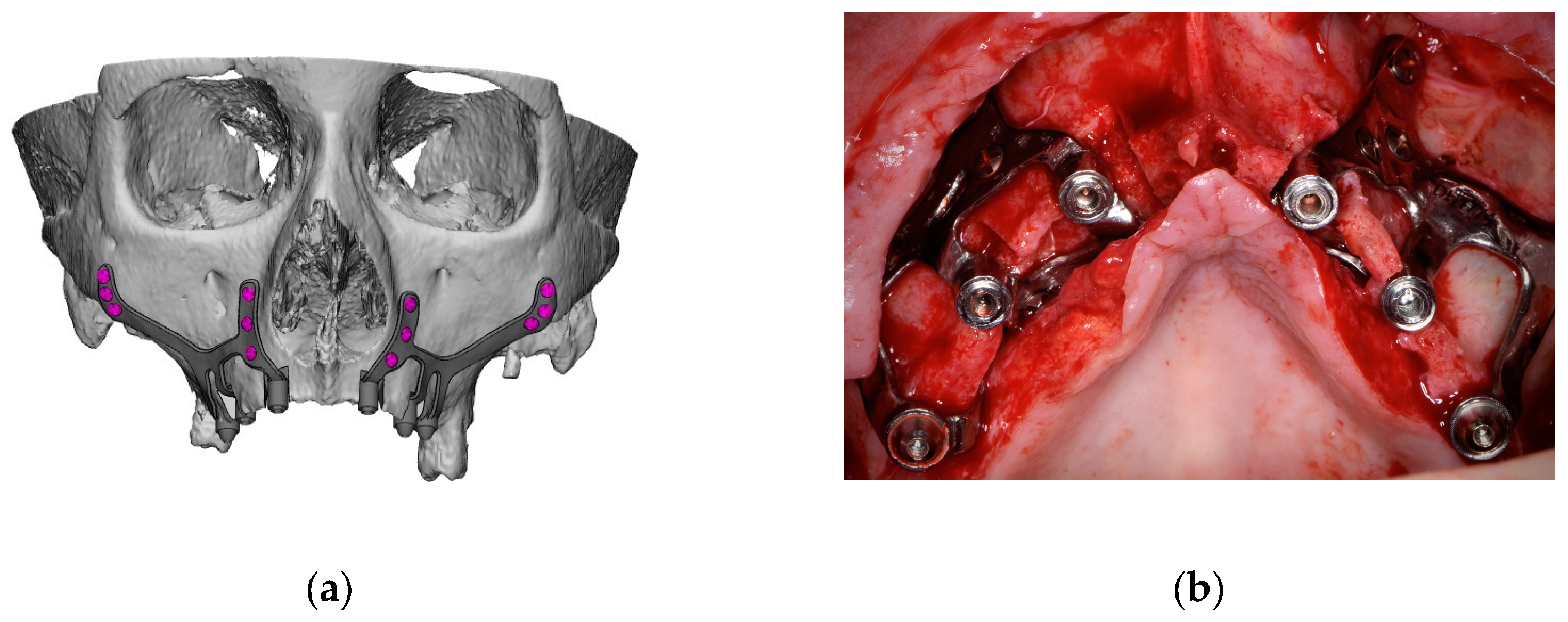
- 2.5.
- It is essential to avoid abrupt transitions and sharp angles in the areas between the CSI frame and the prosthetic connections (Figure 1);
- 2.6.
- Fixation of the CSI is a key factor for achieving a successful treatment outcome. The fixation elements should be placed in high anatomic buttress areas (nasal and zygomatic) and the palatal region. The use of self-drilling screws is recommended;
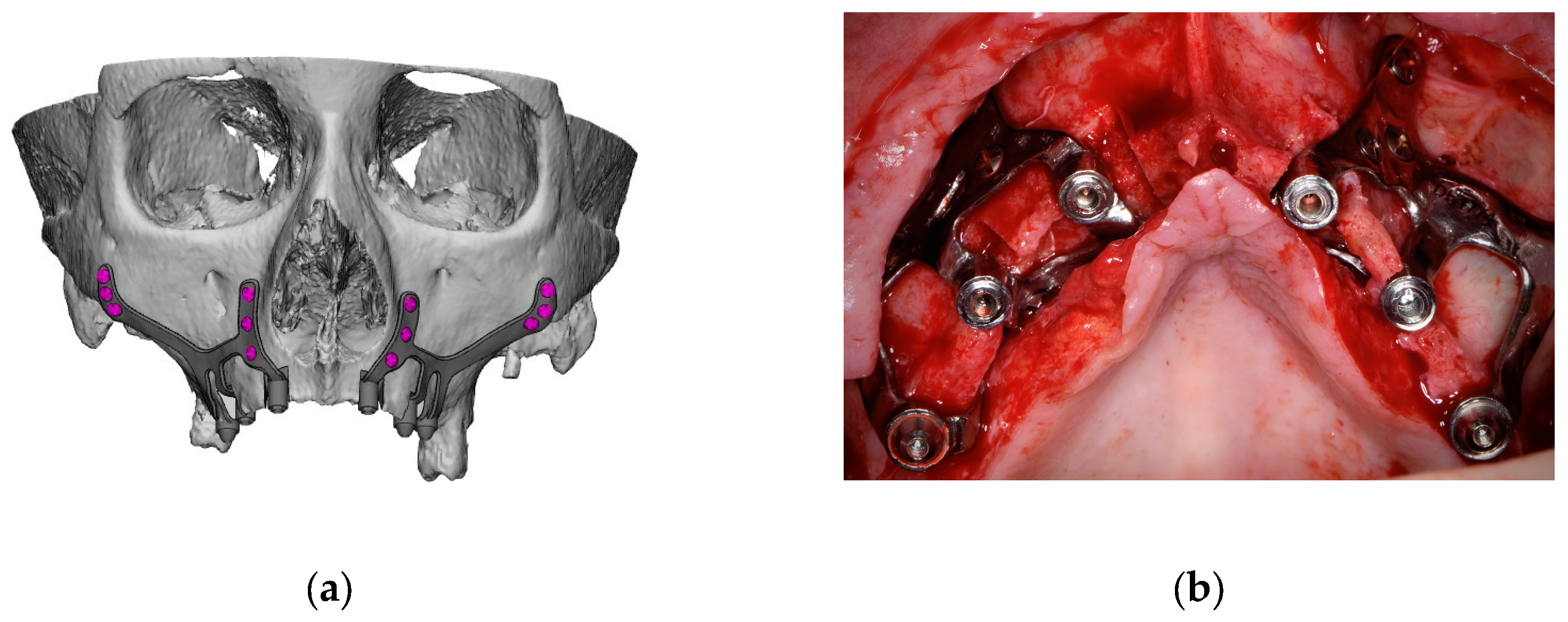
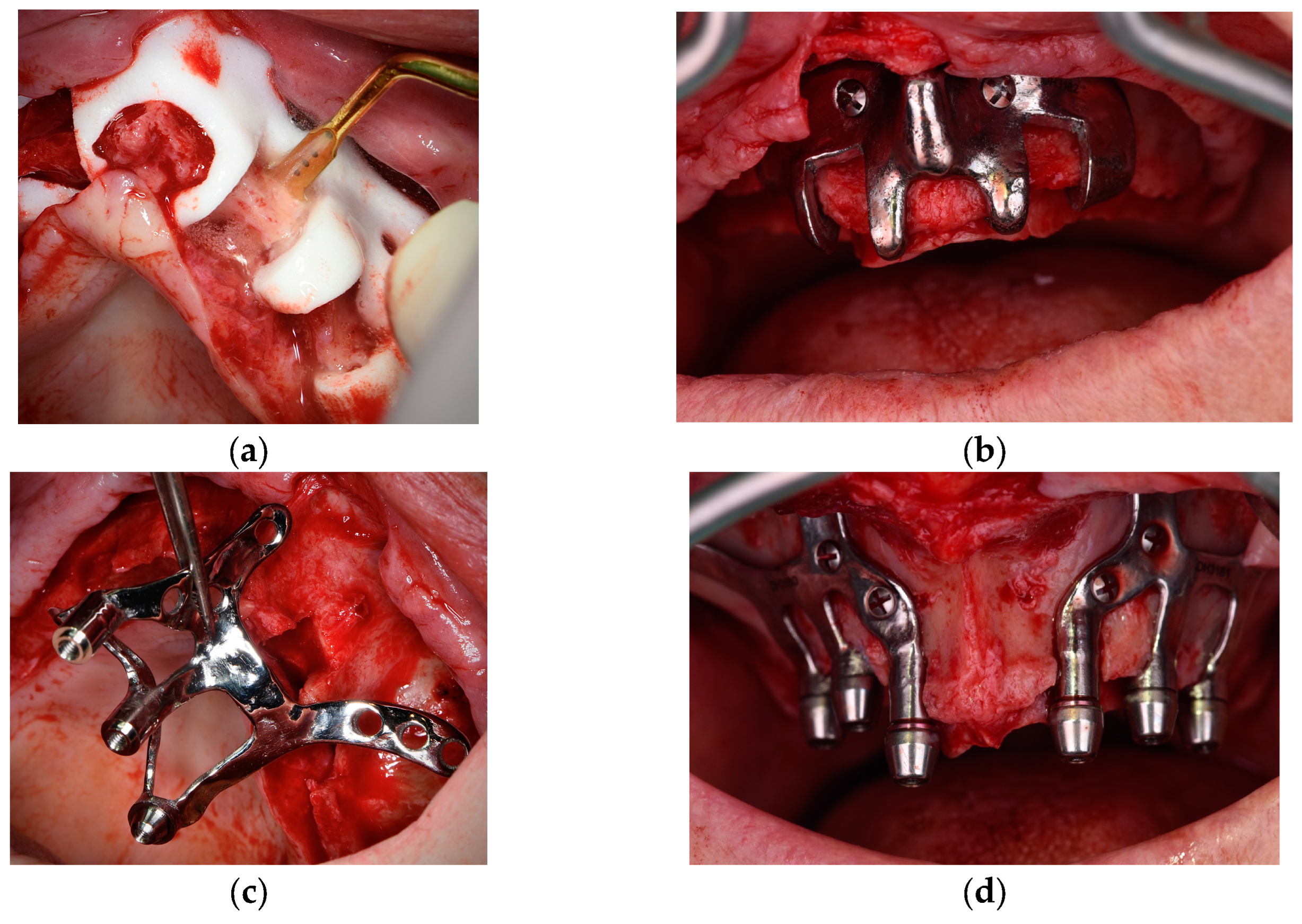
- 2.7.
- In cases with totally edentulous arches, clinicians should consider designing two independent frames to facilitate the implant insertion path during the procedure (Figure 2). This issue is particularly important when high fixation zones are selected (EO);
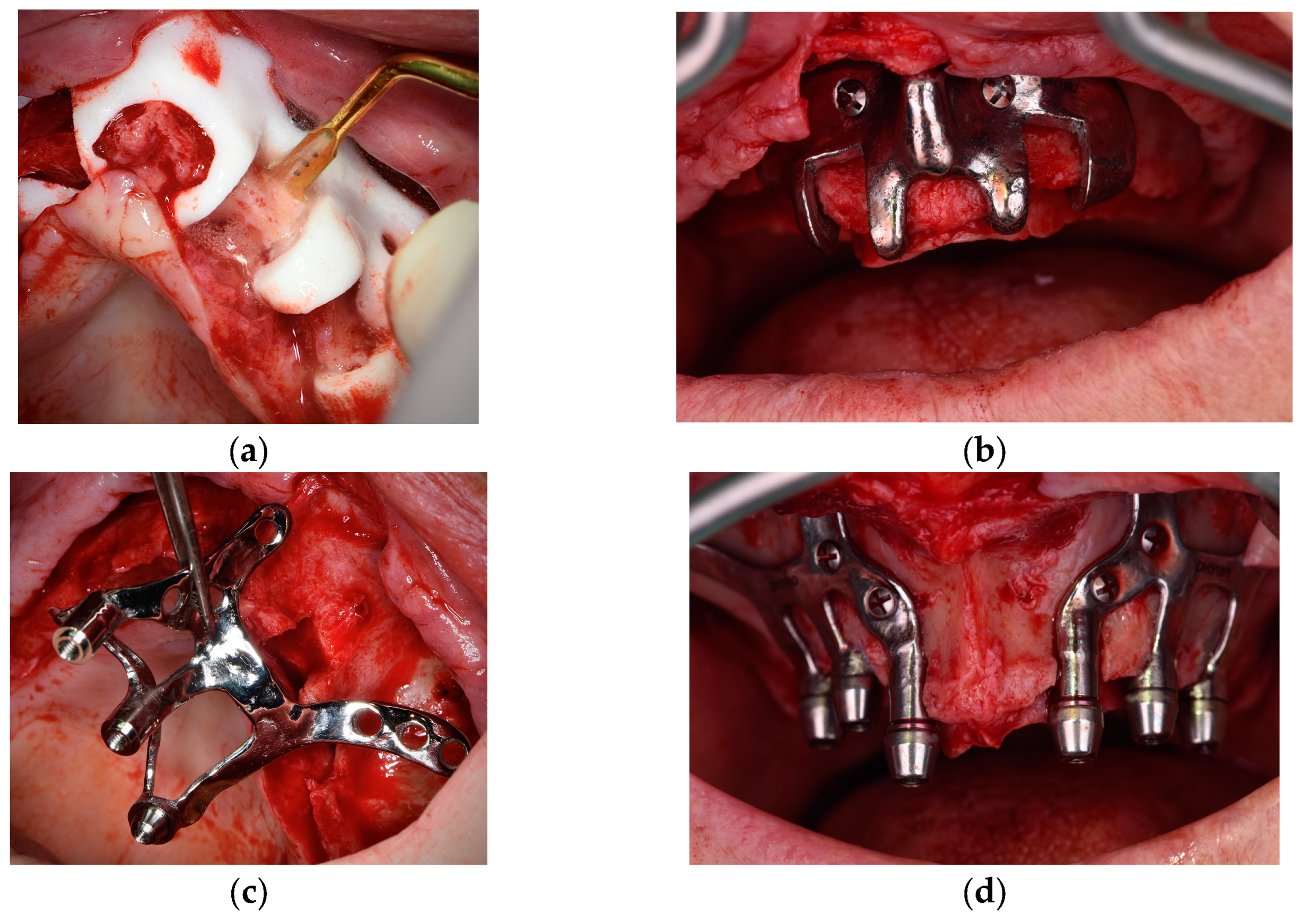
- 2.8.
- Specific surgical templates are recommended to guide the removal of the residual alveolar ridge (Figure 3). This will improve the adaptation of the CSI, facilitate its design, and reduce the risk of postoperative soft tissue dehiscence (EO);
- 2.9.
- From a biomechanical perspective, there is no contraindication for connecting CSIs with previously placed conventional dental implants (EO);
- 2.10.
- It is advisable to print a 3D model of the patient before surgery (EO).
- 3.
- Surgical protocol and associated complications.
- 3.1.
- Although it is possible to place CSIs under local anesthesia, it is advisable to combine them with conscious sedation techniques or general anesthesia;
- 3.2.
- Surgical asepsis guidelines must be followed during the procedure;
- 3.3.
- The incision should be performed considering the final position of the keratinized mucosa since this tissue is essential to prevent long-term complications (EO);
- 3.4.
- If the keratinized mucosa width is insufficient, it is advisable to perform soft tissue augmentation procedures;
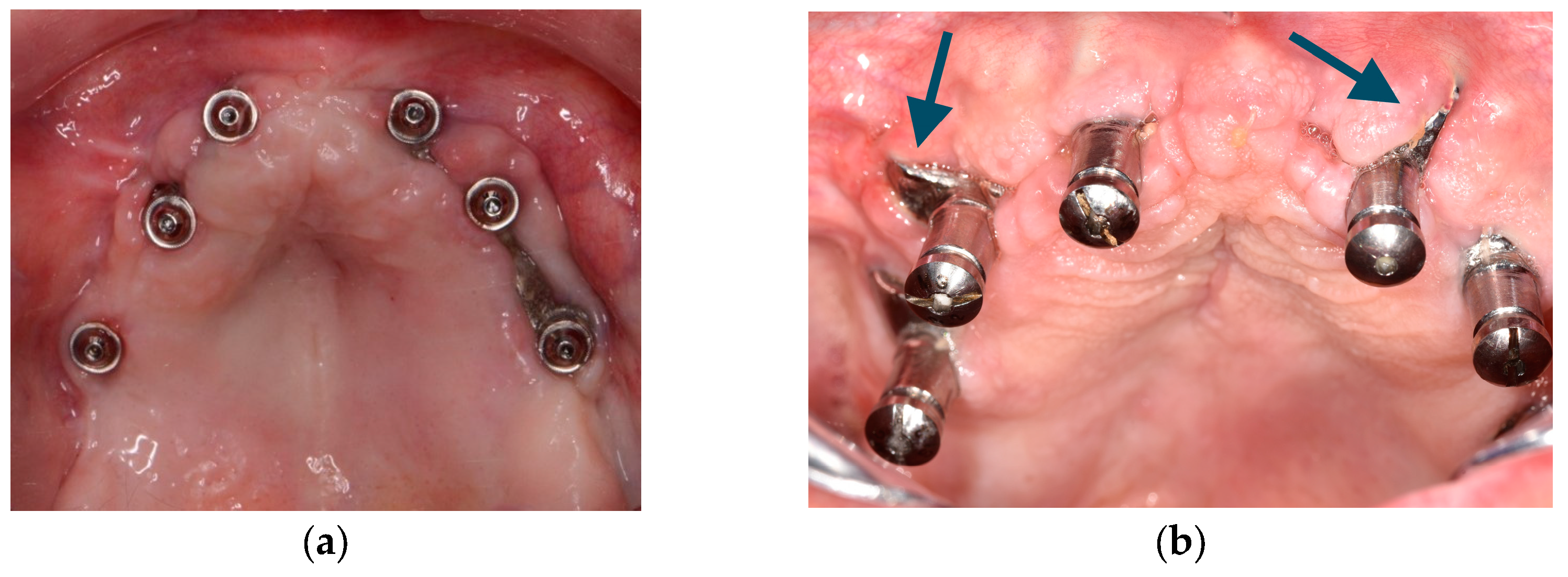
- 3.5.
- Soft tissue dehiscence leading to exposure of the CSI is the most common postoperative complication (Figure 4). This complication does not seem to affect CSI survival in the short term.
- 3.6.
- Removal of the CSI is indicated when the implant has lost its stability or when recurrent infections occur;
- 3.7.
- It is advisable to have a sterile 3D model of the patient present during the surgical procedure (Figure 5) (EO);
- 3.8.
- After testing the insertion of the implant in the model, the CSI should be securely fixed with screws to the maxilla or mandible. The flap should be repositioned, leaving the abutments exposed.
- 4.
- Prosthetic protocol and associated complications.
- 4.1.
- A thorough and complete preoperative prosthetic diagnosis is mandatory. This prosthetic planning is essential for designing the CSI correctly;
- 4.2.
- The prosthodontic treatment principles and steps used in rehabilitation with conventional dental implants should be followed when using CSI. It is essential to create a prosthesis with ovoid pontics that allows correct assessment for oral hygiene;
- 4.3.
- The clinical results of this group of experts support the use of fixed screw-retained restorations over CSIs. The literature also reports on the use of other types of rehabilitation (EO);
- 4.4.
- The CSI can be immediately loaded;
- 4.5.
- The provisional and definitive prostheses should not apply pressure on the soft tissues (EO);
- 4.6.
- A minimum of 4 prosthetic connections are required to rehabilitate an entire arch;
- 4.7.
- Whenever possible, the use of transepithelial abutments should be considered (EO);
- 4.8.
- The materials employed in conventional implant-supported prostheses are also suitable for rehabilitation with CSIs;
- 4.9.
- It is advisable to use an occlusal splint after the prosthetic rehabilitation to prevent the occurrence of mechanical complications, especially when the patient has natural dentition or a fixed implant-supported rehabilitation in the opposing arch (EO).
- 5.
- Peri-implant supportive therapy.
- 5.1.
- There is no specific evidence reporting the maintenance protocol for CSI restorations;
- 5.2.
- Control visits are recommended every 6 months to avoid or diagnose biological (e.g., bone loss under CSIs) or mechanical complications (e.g., prosthetic fracture) (EO);
- 5.3.
- The main goal of peri-implant supportive therapy is to remove plaque accumulation and biofilm around implant abutments and prostheses. In the case of screw-retained restorations, these can be removed to thoroughly clean the surfaces (EO);
- 5.4.
- Patients should be informed of the importance of these visits for the long-term maintenance of their rehabilitation and of the most common pathologies or complications. Patients should also be advised to seek clinical attention in cases of CSI mobility or soft tissue dehiscences (CSI exposure) (EO);
- 5.5.
- These visits should include professional advice in case of risk factors/indicators. Patients should be informed that redness, bleeding, or inflammation of the peri-implant mucosa are important signs that, if left untreated, might result in significant long-term complications (EO).
- 6.
- General recommendations and future perspectives (EO).
- 6.1.
- The available data on the use of CSIs are very scarce, precluding the establishment of clinical recommendations based on scientific evidence. It is essential to perform randomized clinical trials to compare the use of CSIs with other therapeutic alternatives. Additionally, cohort studies with a long-term follow-up could help determine the incidence, repercussions, and prognosis of complications associated with CSIs;
- 6.2.
- Finite analysis studies evaluating different CSI designs would be desirable;
- 6.3.
- Professionals are encouraged to undergo specific training in the use of CSIs;
- 6.4.
- Professionals could benefit from developing additional tools or guides to reduce the margin of error. The creation of specifically designed custom guides for all steps of the treatment would be desirable;
- 6.5.
- The development of specific prosthetic connections for CSIs might be interesting.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tofé-Povedano, A.; Parras-Hernández, J.; Herce-López, J.; Matute-García, D.; González-Moguena, V.A.; Rollón-Mayordomo, A. Design modifications in subperiosteal implants to avoid complications. Presentation of a case series study and literature re-view. Rev. Esp. Cir. Oral Maxilofac. 2023, 45, 57–63. [Google Scholar]
- Branemark, P.-I. Surgery and fixture installation. In Zygomaticus Fixture Clinical Procedures, 1st ed.; Nobel Biocare AB: Goteborg, Sweden, 1998. [Google Scholar]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Survival and complications of zygomatic implants: An updated systematic review. J. Oral Maxillofac. Surg. 2016, 74, 1949–1964. [Google Scholar] [CrossRef] [PubMed]
- Pons, M.C.; Gallo, J.A.; Perez, L.M.; Martinez, G.D.; Vicario, A.C. Subperiosteal personalised implants for the rehabilitation of the severely deficient edentulous maxilla. Revision of a clinical series of 8 cases. Rev. Esp. Cir. Oral Maxilofac. 2021, 43, 140–148. [Google Scholar]
- Borre, C.V.D.; Rinaldi, M.; De Neef, B.; Loomans, N.A.J.; Nout, E.; Van Doorne, L.; Naert, I.; Politis, C.; Schouten, H.; Klomp, G.; et al. Radiographic evaluation of bone re-modeling after additively manufactured subperiosteal jaw implantation (Amsji) in the maxilla: A one-year follow-up study. J. Clin. Med. 2021, 10, 3542. [Google Scholar] [CrossRef] [PubMed]
- Borre, C.V.D.; Rinaldi, M.; De Neef, B.; Loomans, N.; Nout, E.; Van Doorne, L.; Naert, I.; Politis, C.; Schouten, H.; Klomp, G.; et al. Patient- and clinician-reported outcomes for the additively manufactured sub-periosteal jaw implant (AMSJI) in the maxilla: A prospective multicentre one-year follow-up study. Int. J. Oral Maxillofac. Surg. 2022, 51, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Korn, P.; Gellrich, N.C.; Jehn, P.; Spalthoff, S.; Rahlf, B. A new strategy for patient-specific implant-borne dental rehabilitation in patients with extended maxillary defects. Front. Oncol. 2021, 11, 718872. [Google Scholar] [CrossRef]
- Rahlf, B.; Korn, P.; Zeller, A.-N.; Spalthoff, S.; Jehn, P.; Lentge, F.; Gellrich, N.-C. Novel approach for treating challenging implant-borne maxillary dental rehabilitation cases of cleft lip and palate: A retrospective study. Int. J. Implant. Dent. 2022, 8, 6. [Google Scholar] [CrossRef]
- Mommaerts, M.Y. Additively manufactured sub-periosteal jaw implants. Int. J. Oral Maxillofac. Surg. 2017, 46, 938–940. [Google Scholar] [CrossRef]
- Mommaerts, M.Y. Evolutionary steps in the design and biofunctionalization of the additively manufactured sub-periosteal jaw implant ‘AMSJI’ for the maxilla. Int. J. Oral Maxillofac. Surg. 2019, 48, 108–114. [Google Scholar] [CrossRef]
- Gellrich, N.-C.; Zimmerer, R.M.; Spalthoff, S.; Jehn, P.; Pott, P.-C.; Rana, M.; Rahlf, B. A customised digitally engineered solution for fixed dental rehabilitation in severe bone deficiency: A new innovative line extension in implant dentistry. J. Craniomaxillofac. Surg. 2017, 45, 1632–1638. [Google Scholar] [CrossRef]
- Cerea, M.; Dolcini, G.A. Custom-made direct metal laser sintering titanium subperiosteal implants: A retrospective clinical study on 70 patients. Biomed. Res. Int. 2018, 2018, 5420391. [Google Scholar] [CrossRef] [PubMed]
- Claffey, N.; Bashara, H.; O’Reilly, P.; Polyzois, I. Evaluation of new bone formation and osseointegration around subperiosteal titanium implants with histometry and nanoindentation. Int. J. Oral Maxillofac. Implant. 2015, 30, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Peev, S.; Sabeva, E. Subperiosteal implants in treatment of total and partial edentulism—A long term follow up. Int. J. Sci. Res. 2016, 5, 98–99. [Google Scholar]
- Harbour, R.; Miller, J. A new system for grading recommendations in evidence based guidelines. BMJ 2001, 323, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Rams, T.E.; Balkin, B.E.; Roberts, T.W.; Molzan, A.K. Microbiological aspects of human mandibular subperiosteal dental implants. J. Oral Implantol. 2013, 39, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Bianchi, A.; Mangano, F.G.; Dana, J.; Colombo, M.; Solop, I.; Admakin, O. Custom-made 3D printed subperiosteal titanium implants for the prosthetic restoration of the atrophic posterior mandible of elderly patients: A case series. 3D Print. Med. 2020, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Carretero, J.L.C.; Vera, J.L.D.C.P.d.; García, N.M.; Martínez, P.G.; Martínez, M.M.P.; Niño, I.A.; Cuéllar, I.N.; Cuéllar, C.N. Virtual surgical planning and customized subperiosteal titanium maxillary implant (CSTMI) for three dimensional reconstruction and dental implants of maxillary defects after oncological resection: Case series. J. Clin. Med. 2022, 11, 4594. [Google Scholar] [CrossRef]
- Nemtoi, A.; Covrig, V.; Nemtoi, A.; Stoica, G.; Vatavu, R.; Haba, D.; Zetu, I. Custom-made direct metal laser sintering titanium sub-periosteal implants in oral and maxillofacial surgery for severe bone-deficient patients-A pilot study. Diagnostics 2022, 12, 2531. [Google Scholar] [CrossRef]
- Dimitroulis, G.; Gupta, B.; Wilson, I.; Hart, C. The atrophic edentulous alveolus. A preliminary study on a new generation of subperiosteal implants. Oral Maxillofac. Surg. 2023, 27, 69–78. [Google Scholar] [CrossRef]
- Vatteroni, E.; Covani, U.; Menchini Fabris, G.B. The new generation of subperiosteal implants for patient-specific treatment of atrophic jawbone: Literature review and a two-case report. Int. J. Periodontics Restor. Dent. 2023, 43, 735–741. [Google Scholar] [CrossRef]
- Alotaibi, F.F.; Rocchietta, I.; Buti, J.; D’Aiuto, F. Comparative evidence of different surgical techniques for the management of vertical alveolar ridge defects in terms of complications and efficacy: A systematic review and network meta-analysis. J. Clin. Periodontol. 2023, 50, 1487–1519. [Google Scholar] [CrossRef]
- McKenna, G.J.; Gjengedal, H.; Harkin, J.; Holland, N.; Moore, C.; Srinivasan, M. Effect of autogenous bone graft site on dental implant survival and donor site complications: A systematic review and meta-analysis. J. Evid. Based Dent. Pr. 2022, 22, 101731. [Google Scholar] [CrossRef] [PubMed]
- Strappa, E.M.; Memè, L.; Cerea, M.; Roy, M.; Bambini, F. Custom-made additively manufactured subperiosteal implant. Minerva Dent. Oral Sci. 2022, 71, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Davo, R.; Malevez, C.; Rojas, J. Immediate function in the atrophic maxilla using zygoma implants: A preliminary study. J. Prosthet. Dent. 2007, 97, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Franch, M. Immediate/Early loading of zygomatic implants: Clinical experiences after 2 to 5 years of follow-up. Clin. Implant. Dent. Relat. Res. 2010, 12, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Kämmerer, P.W.; Fan, S.; Aparicio, C.; Bedrossian, E.; Davó, R.; Morton, D.; Raghoebar, G.M.; Zarrine, S.; Al-Nawas, B. Evaluation of surgical techniques in survival rate and complications of zygomatic implants for the rehabilitation of the atrophic edentulous maxilla: A systematic review. Int. J. Implant. Dent. 2023, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Surovas, A. A digital workflow for modeling of custom dental implants. 3D Print. Med. 2019, 5, 9. [Google Scholar] [CrossRef]
- de Tapia, B.; Mozas, C.; Valles, C.; Nart, J.; Sanz, M.; Herrera, D. Adjunctive effect of modifying the implant-supported prosthesis in the treatment of peri-implant mucositis. J. Clin. Periodontol. 2019, 46, 1050–1060. [Google Scholar] [CrossRef]
- Insua, A.; Monje, A.; Wang, H.L.; Inglehart, M. Patient-centered perspectives and understanding of peri-implantitis. J. Periodontol. 2017, 88, 1153–1162. [Google Scholar] [CrossRef]
- Monje, A.; Aranda, L.; Diaz, K.T.; Alarcón, M.A.; Bagramian, R.A.; Wang, H.L.; Catena, A. Impact of maintenance therapy for the prevention of peri-implant diseases: A systematic review and meta-analysis. J. Dent. Res. 2016, 95, 372–379. [Google Scholar] [CrossRef]
- Rokn, A.; Aslroosta, H.; Akbari, S.; Najafi, H.; Zayeri, F.; Hashemi, K. Prevalence of peri-implantitis in patients not participating in well-designed supportive periodontal treatments: A cross-sectional study. Clin. Oral Implant. Res. 2017, 28, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.O.; Costa, A.M.; Ferreira, S.D.; Lima, R.P.E.; Pereira, G.H.M.; Cyrino, R.M.; Oliveira, A.M.S.D.; Oliveira, P.A.D.; Cota, L.O.M. Long-term impact of patients’ compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: An 11-year prospective follow-up clinical study. Clin. Implant. Dent. Relat. Res. 2023, 25, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Periodontol. 2018, 89, 267–290. [Google Scholar] [CrossRef] [PubMed]
- Cercadillo-Ibarguren, I.; Sánchez-Torres, A.; Figueiredo, R.; Valmaseda-Castellón, E. Early complications of immediate loading in edentulous full-arch restorations: A retrospective analysis of 88 cases. Int. J. Oral Maxillofac. Implant. 2017, 32, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Torres, A.; Cercadillo-Ibarguren, I.; Figueiredo, R.; Gay-Escoda, C.; Valmaseda-Castellón, E. Mechanical complications of implant-supported complete-arch restorations and impact on patient quality of life: A retrospective cohort study. J. Prosthet. Dent. 2021, 125, 279–286. [Google Scholar] [CrossRef]
- De Bruyn, H.; Raes, S.; Matthys, C.; Cosyn, J. The current use of patient-centered/reported outcomes in implant dentistry: A systematic review. Clin. Oral Implant. Res. 2015, 26, 45–56. [Google Scholar] [CrossRef]
- Lang, N.P.; Zitzmann, N.U.; on behalf of Working Group 3 of the VIII European Workshop on Periodontology. Clinical research in implant dentistry: Evaluation of implant-supported restorations, aesthetic and patient-reported outcomes. J. Clin. Periodontol. 2012, 39, 133–138. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, and Country | Study Design | Number of Patients | Indication | Type of Prosthesis | Type of Implant | Complications | Follow-Up | Level of Evidence (SIGN) |
|---|---|---|---|---|---|---|---|---|
| Rams et al., 2013 [15], United States of America | Case series | 11 | Edentulous mandible | Overdenture | Implant frames were cast using a cobalt–chromium–molybdenum alloy (Vitallium) | 3 periimplantitis | 11.7 years ± 1.5 years (range 10–13 years) in patients with periimplantitis; 2.4 years ± 4.9 years (range 9–22 years) in healthy patients | 3 |
| Cerea and Dolcini 2018 [12], Italy | Retrospective cohort | 70 | Total or partial edentulism | Provisional prosthesis (resin), Definitive cement-retained metal–ceramic prosthesis | Laser sintering titanium CSI | 3 failures due to infections; 4 patients reported postoperative pain and swelling; 1 patient with recurrent infections 4 fractures of the provisional prosthesis; 2 patients with ceramic fractures (chipping) in the definitive prosthesis | 2 years | 2++ |
| Mangano et al., 2020 [16], Russia | Case series | 10 | Partial posterior mandibular edentulism | Cement-retained provisional prosthesis (PMMA) 10 days after surgery. New provisional prosthesis 1 month after surgery. Definitive cement-retained prosthesis (zirconia–ceramic) | Laser sintering titanium CSI (titanium grade 5 micro-powders) | 1 patient with postoperative pain and swelling; 2 patients with provisional prosthesis fractures | 1 year | 3 |
| Cebrián-Carretero et al., 2022 [17], Spain | Case series | 4 | Oncological defects | Provisional prosthesis Fixed metal–ceramic prosthesis | Laser sintering titanium CSI | No complications | 32 months (range 9 months–3 years) | 3 |
| Nemtoi et al., 2022 [18], Romania | Retrospective cohort | 16 | Edentulous maxilla (n = 10) Partially edentulous maxilla (n = 1) Edentulous mandible (n = 4) Partially edentulous mandible (n = 1) | Provisional prosthesis (resin) Fixed prosthesis (unspecified) | Laser sintering titanium CSI | 1 failure due to incorrect adjustment and recurrent infections; 6 soft tissue dehiscences leading to CSI exposure 1 fracture of the provisional prosthesis; | 6 months | 2++ |
| Dimitroulis et al., 2023 [19], Australia | Case series | 21 | Edentulous maxilla (n = 15) Edentulous mandible (n = 3) Partial edentulism (n = 2) Maxillectomy (n = 1) | Screw-retained provisional prosthesis (resin) Definitive prosthesis | Laser sintering titanium CSI | 5 patients with CSI exposure:
1 patient with implant mobility (additional retention screws were placed) 1 CSI was removed due to systemic causes (psychiatric disorder) | 22.1 months (range 5–57 months) | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herce-López, J.; Pingarrón, M.d.C.; Tofé-Povedano, Á.; García-Arana, L.; Espino-Segura-Illa, M.; Sieira-Gil, R.; Rodado-Alonso, C.; Sánchez-Torres, A.; Figueiredo, R. Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics 2024, 9, 61. https://doi.org/10.3390/biomimetics9010061
Herce-López J, Pingarrón MdC, Tofé-Povedano Á, García-Arana L, Espino-Segura-Illa M, Sieira-Gil R, Rodado-Alonso C, Sánchez-Torres A, Figueiredo R. Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics. 2024; 9(1):61. https://doi.org/10.3390/biomimetics9010061
Chicago/Turabian StyleHerce-López, Javier, Mariano del Canto Pingarrón, Álvaro Tofé-Povedano, Laura García-Arana, Marc Espino-Segura-Illa, Ramón Sieira-Gil, Carlos Rodado-Alonso, Alba Sánchez-Torres, and Rui Figueiredo. 2024. "Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review" Biomimetics 9, no. 1: 61. https://doi.org/10.3390/biomimetics9010061
APA StyleHerce-López, J., Pingarrón, M. d. C., Tofé-Povedano, Á., García-Arana, L., Espino-Segura-Illa, M., Sieira-Gil, R., Rodado-Alonso, C., Sánchez-Torres, A., & Figueiredo, R. (2024). Customized Subperiosteal Implants for the Rehabilitation of Atrophic Jaws: A Consensus Report and Literature Review. Biomimetics, 9(1), 61. https://doi.org/10.3390/biomimetics9010061