
Towards a First-Person Perspective Mixed Reality Guidance System for Needle Interventions




Abstract
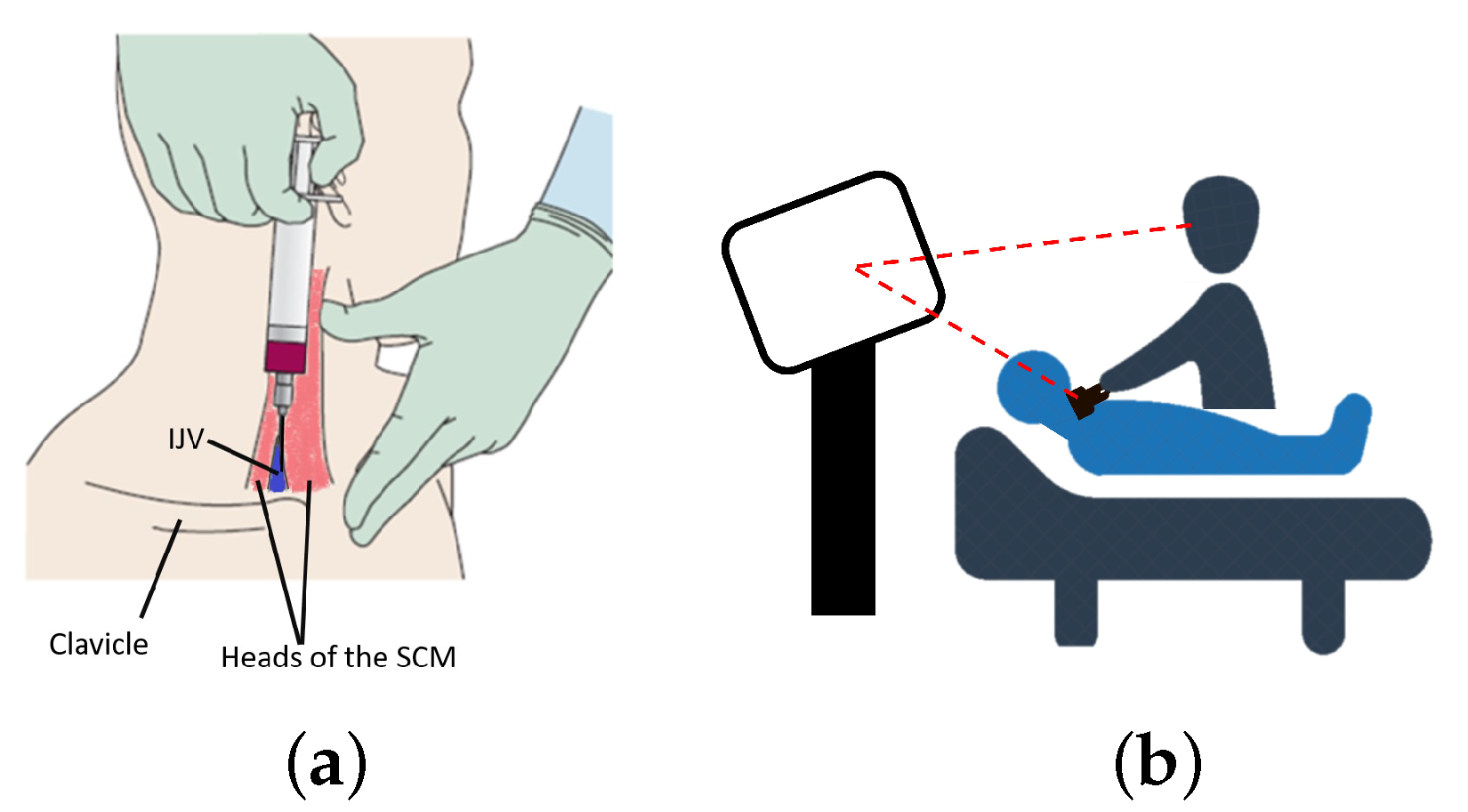
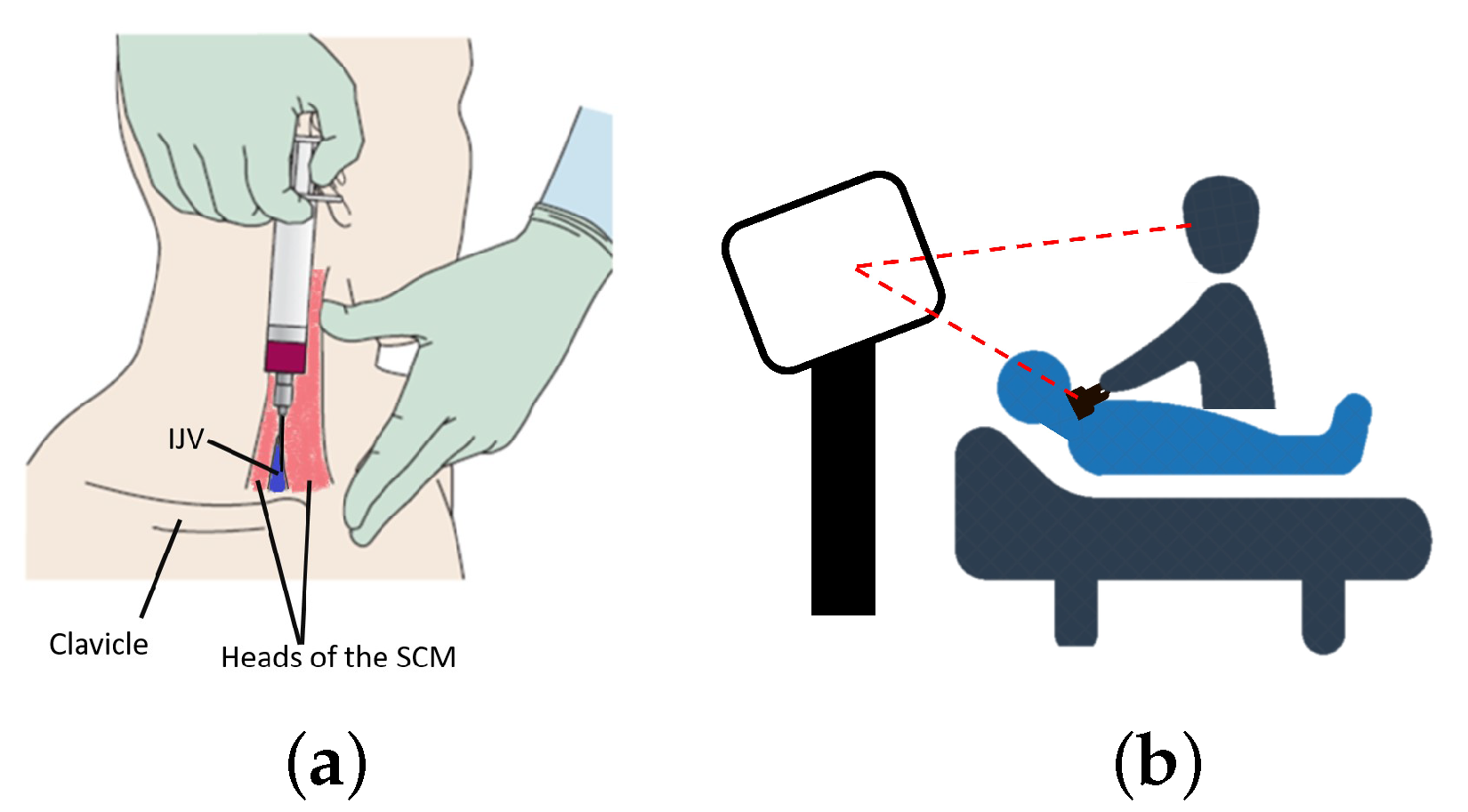
:1. Introduction
2. Materials and Methods
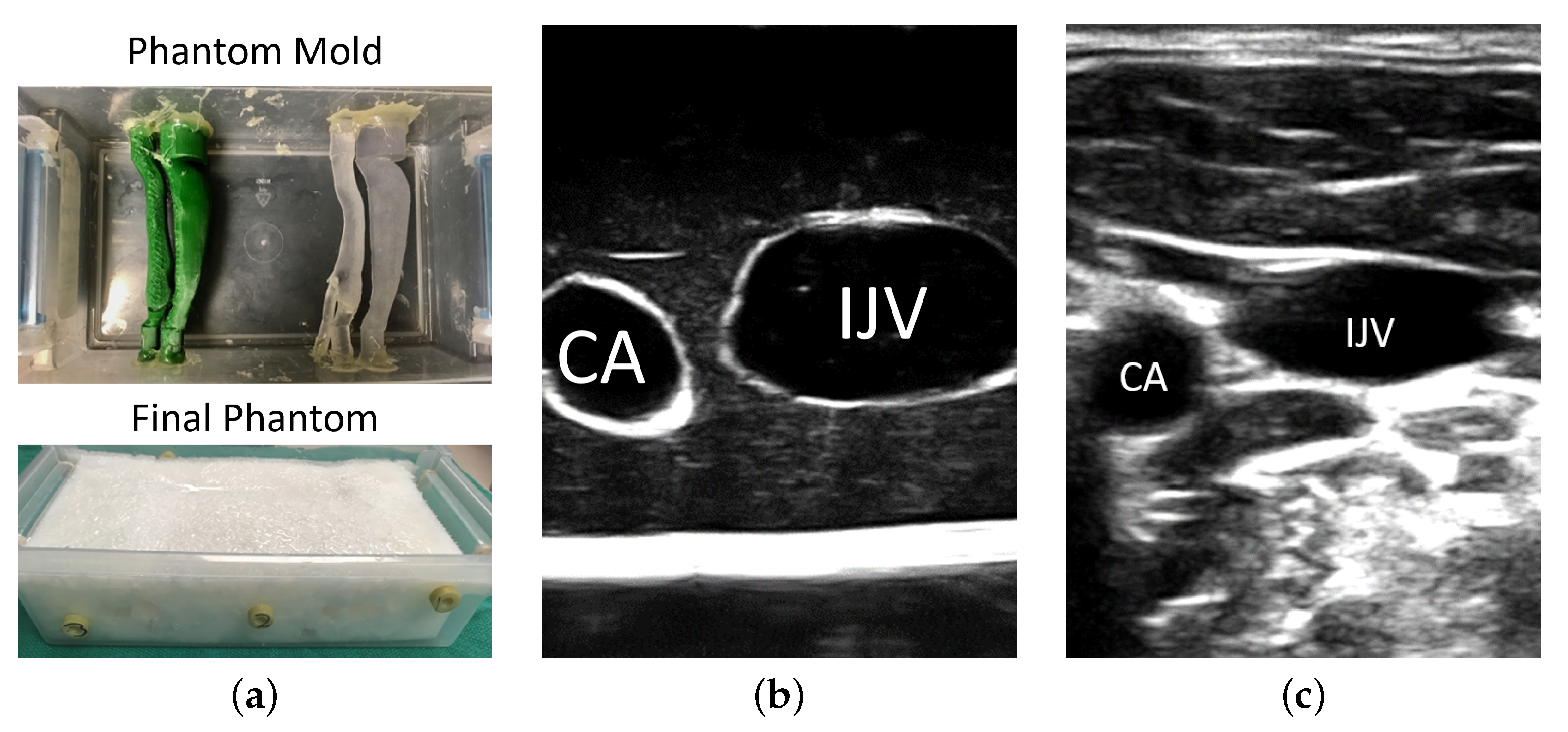
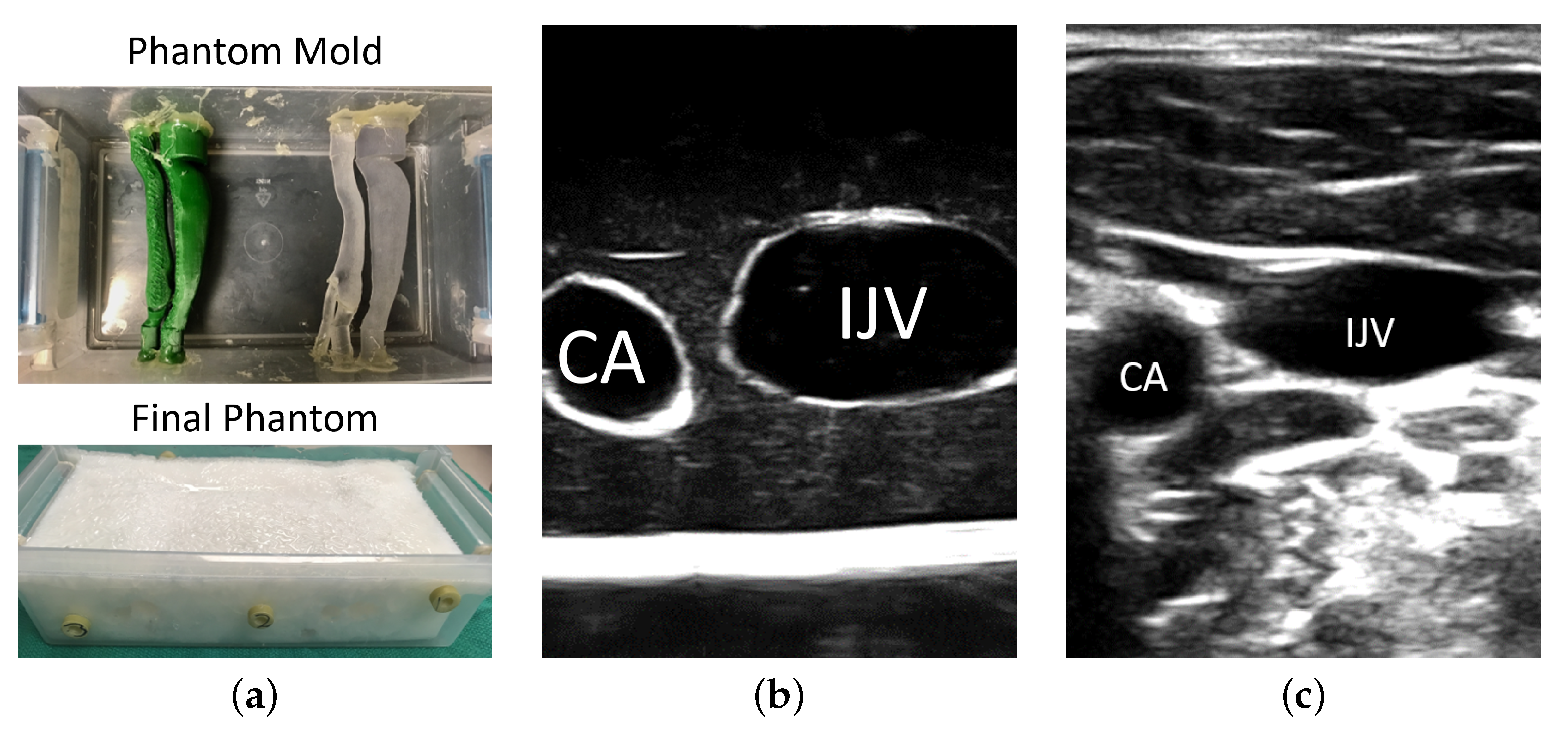
2.1. Anthropomorphic Phantom
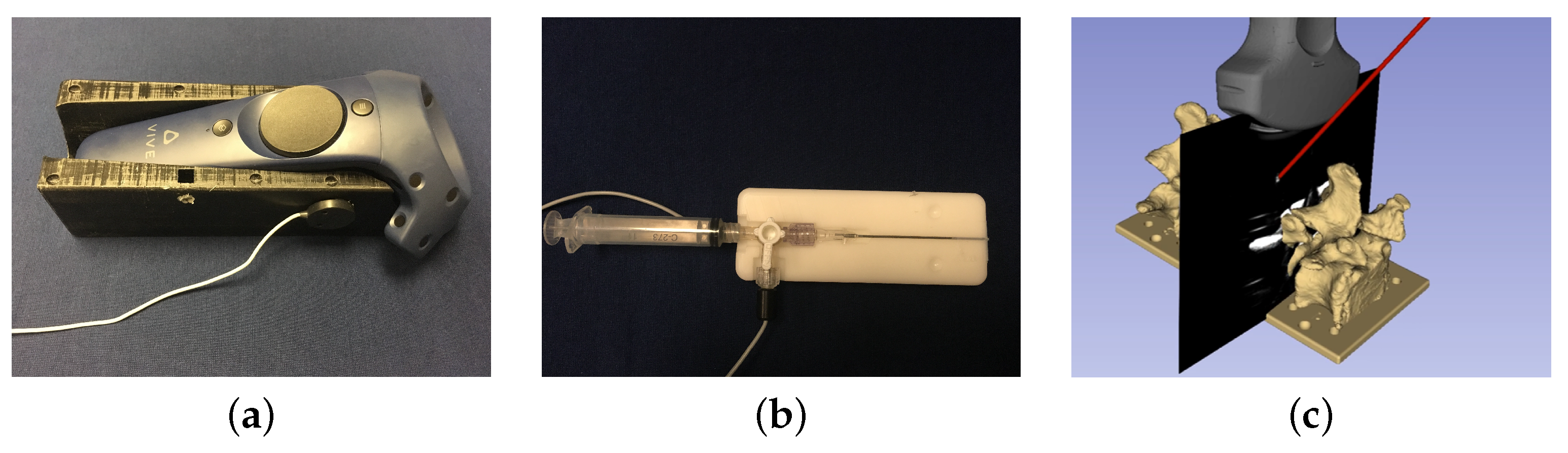
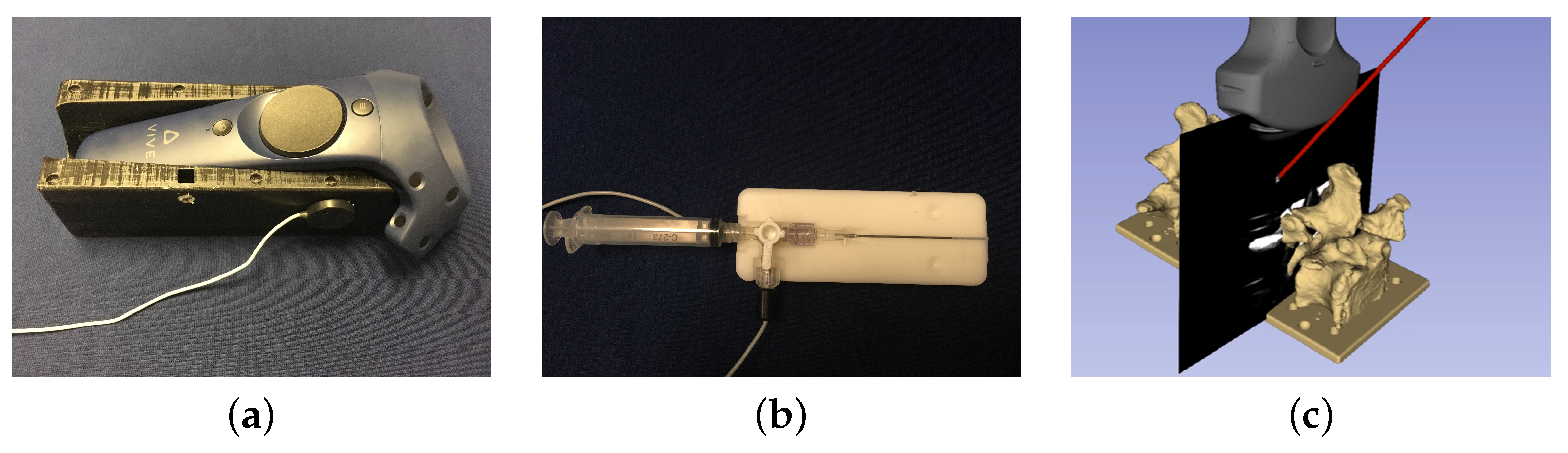
2.2. Spatial Calibration for Tracked Apparatuses
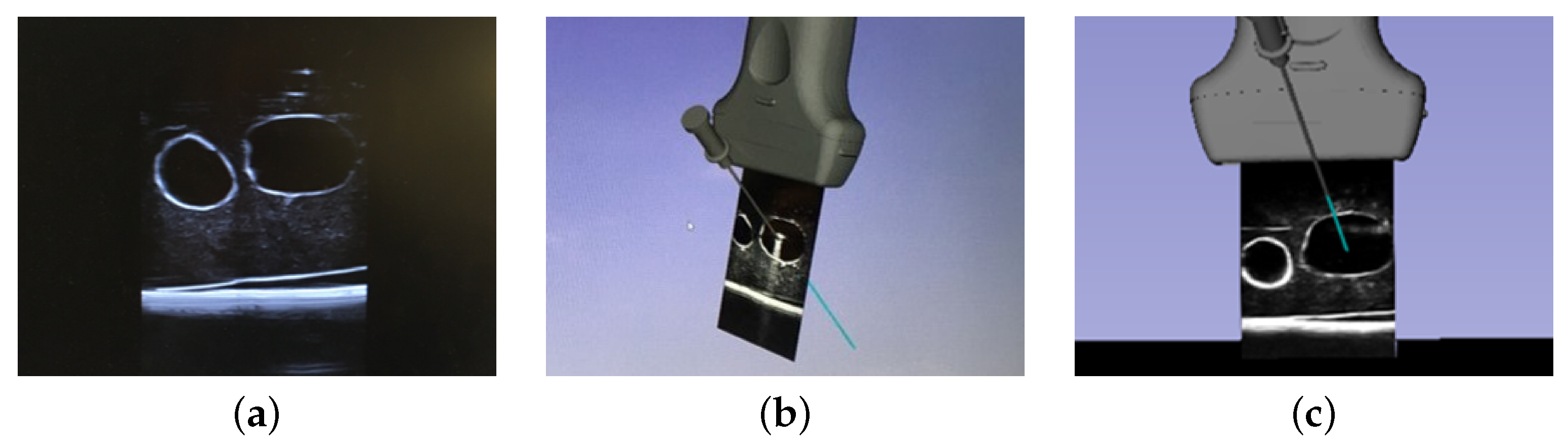
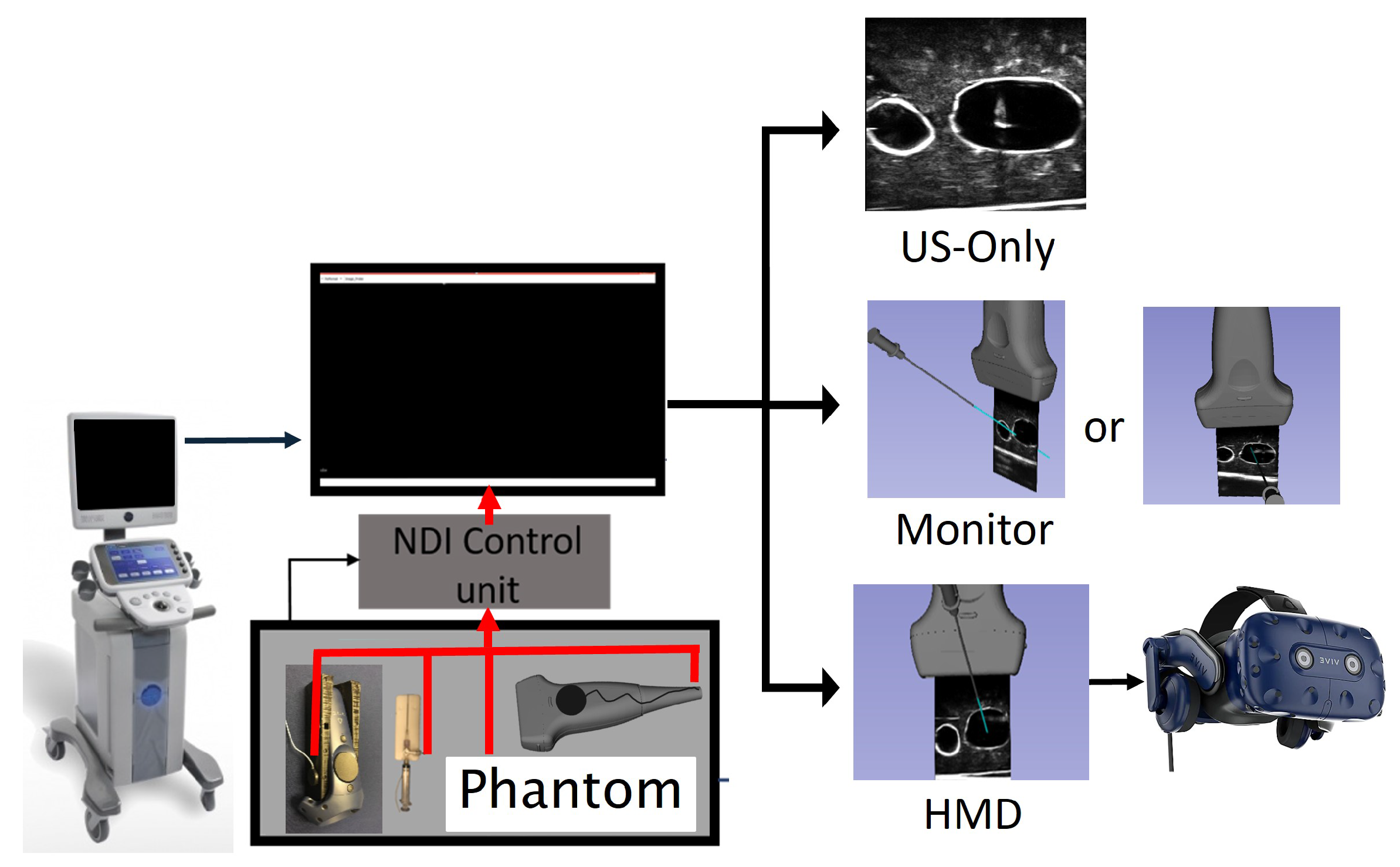
2.3. Visualization Paradigm
2.4. Participants
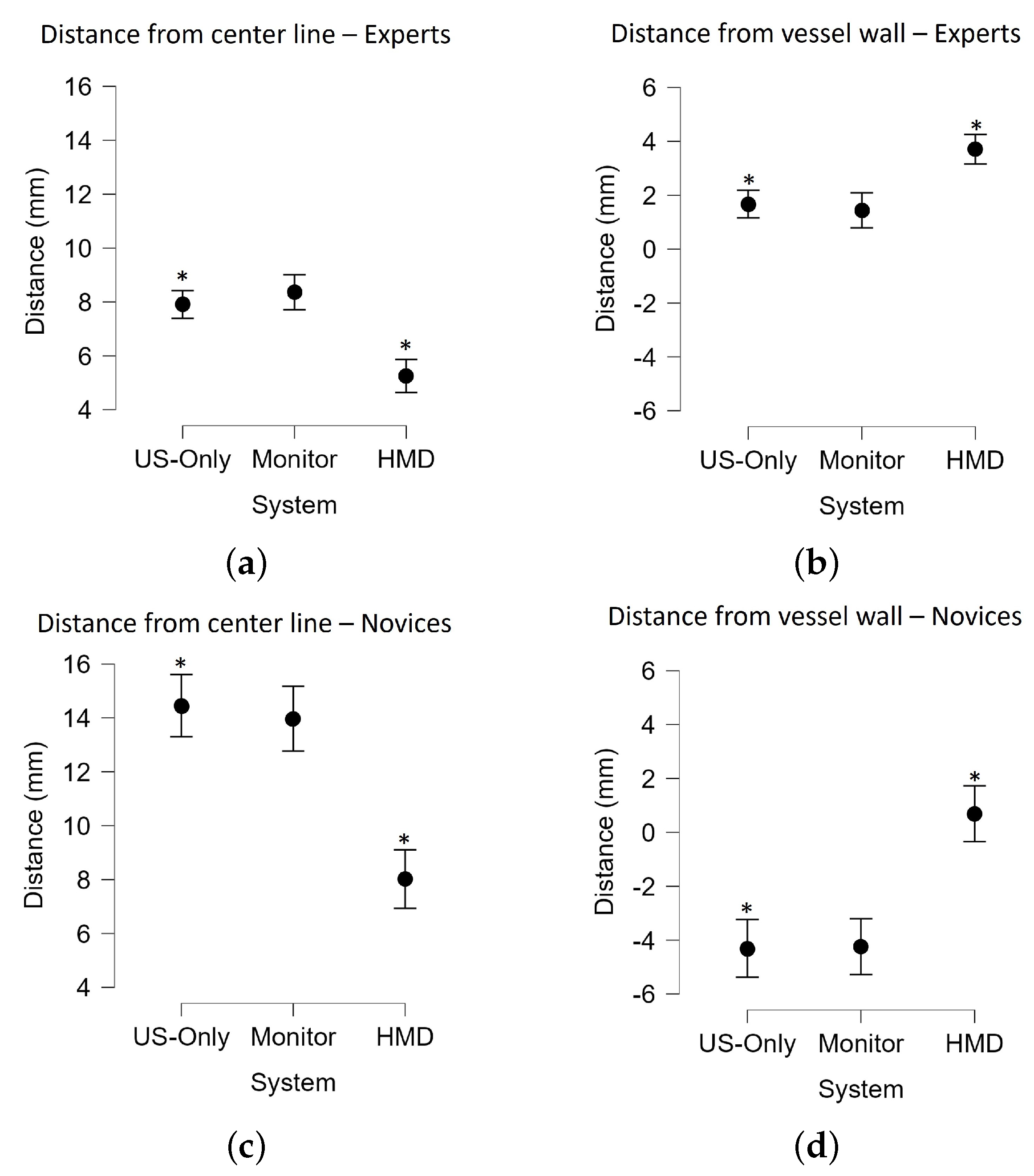
2.5. Data Analysis
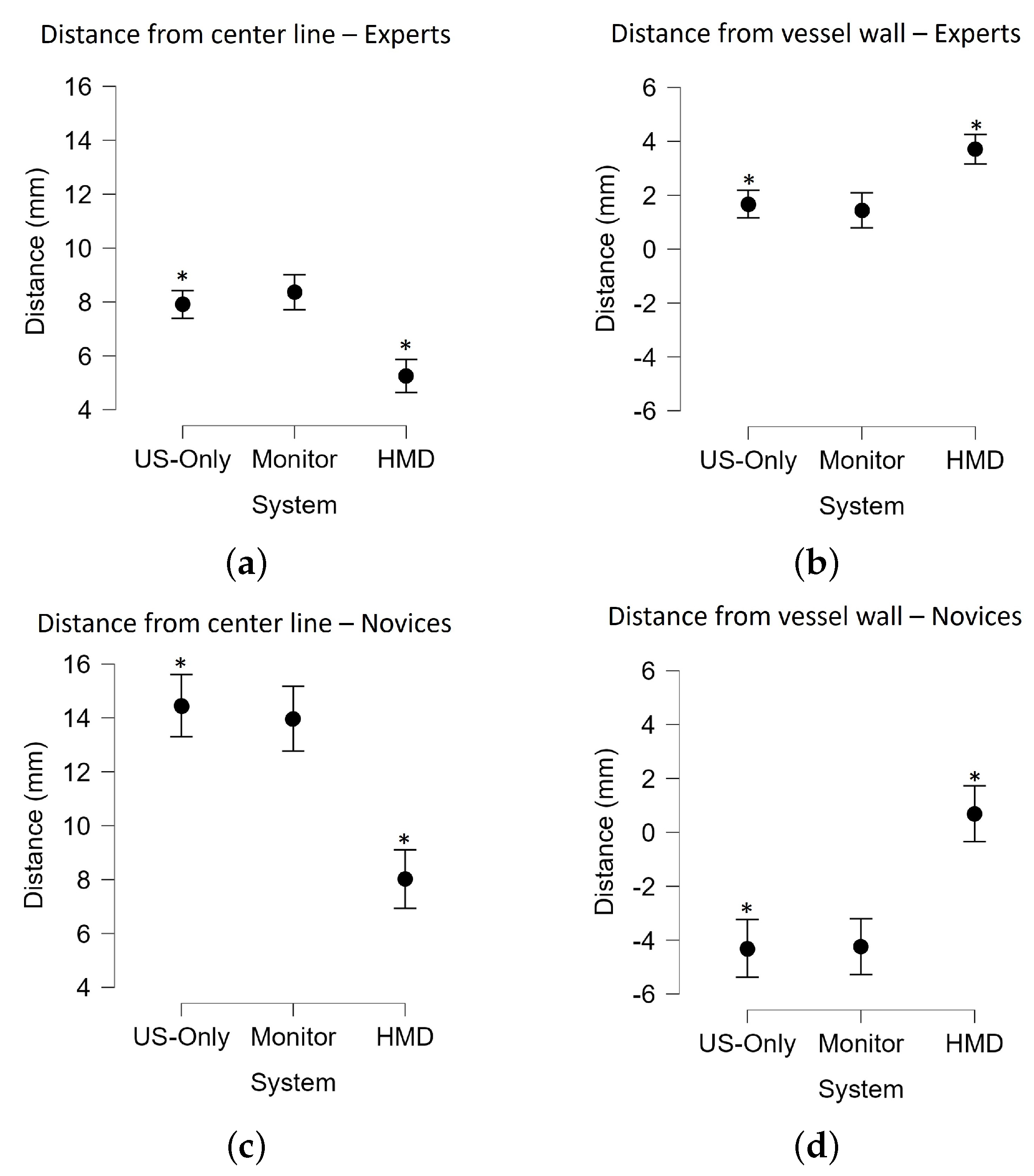
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 2D | Two-Dimentional |
| 3D | Three-Dimentional |
| AR | Augmented Reality |
| AV | Augmented Virtuality |
| CA | Carotid Artery |
| CVC | Central Venous Catheterization |
| DoF | Degrees of Freedom |
| FoV | Field of View |
| IJV | Internal Jugular Vein |
| LAX | Long Axis |
| HMD | Head Mounted Display |
| MR | Mixed Reality |
| MTS | Magnetic Tracking System |
| PVAc | polyvinyl alcohol cryogel |
| SAX | Short Axis |
| SoS | Speed of Sound |
| US | Ultrasound |
| VPT | Video Pass Through |
| VR | Virtual Reality |
References
- McGee, D.C.; Gould, M.K. Preventing Complications of Central Venous Catheterization. N. Engl. J. Med. 2003, 348, 1123–1133. [Google Scholar] [CrossRef]
- Calvert, N.; Hind, D.; McWilliams, R.G.; Thomas, S.M.; Beverley, C.; Davidson, A. The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: A systematic review and economic evaluation. Health Technol. Assess. 2003, 7, 1–84. [Google Scholar] [CrossRef] [Green Version]
- Chao, A.; Lai, C.H.; Chan, K.C.; Yeh, C.C.; Yeh, H.M.; Fan, S.Z.; Sun, W.Z. Performance of central venous catheterization by medical students: A retrospective study of students’ logbooks. BMC Med. Educ. 2014, 14, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajaram, S.S.; Desai, N.K.; Kalra, A.; Gajera, M.; Cavanaugh, S.K.; Brampton, W.; Young, D.; Harvey, S.; Rowan, K. Pulmonary artery catheters for adult patients in intensive care. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akoglu, H.; Piskinpasa, S.; Yenigun, E.C.; Ozturk, R.; Dede, F.; Odabas, A.R. Real-time ultrasound guided placement of temporary internal jugular vein catheters: Assessment of technical success and complication rates in nephrology practice. Nephrology 2012, 17, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Kornbau, C.; Lee, K.; Hughes, G.; Firstenberg, M. central-line complications. Int. J. Crit. Illn. Inj. Sci. 2015, 5, 170–178. [Google Scholar]
- Brass, P.; Hellmich, M.; Kolodziej, L.; Schick, G.; Smith, A.F. Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Scheeren, T.W.L.; Teboul, J.L. Ultrasound-guided central venous catheter placement: A structured review and recommendations for clinical practice. Crit. Care 2017, 21, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenssen, C.; Brkljacic, B.; Hocke, M.; Ignee, A.; Piscaglia, F.; Radzina, M.; Sidhu, P.S.; Dietrich, C.F. EFSUMB Guidelines on Interventional Ultrasound (INVUS), Part VI – Ultrasound-Guided Vascular Interventions. Ultraschall Med. 2016, 37, 473–476. [Google Scholar] [CrossRef] [Green Version]
- Bowdle, A. Vascular complications of central venous catheter placement: Evidence-based methods for prevention and yreatment. J. Cardiothorac. Vasc. Anesth. 2014, 28, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Weiner, M.M.; Geldard, P.; Mittnacht, A.J.C. Ultrasound-guided vascular access: A comprehensive review. J. Cardiothorac. Vasc. Anesth. 2013, 27, 345–360. [Google Scholar] [CrossRef]
- Turba, U.C.; Uflacker, R.; Hannegan, C.; Selby, J.B. Anatomic relationship of the internal jugular vein and the common carotid artery applied to percutaneous transjugular procedures. Cardiovasc. Interv. Radiol. 2005, 28, 303–306. [Google Scholar] [CrossRef]
- Benter, T.; Teichgräber, U.K.M.; Klühs, L.; Papadopoulos, S.; Köhne, C.H.; Felix, R.; Dörken, B. Anatomical variations in the internal jugular veins of cancer patients affecting central venous access. Ultraschall Med. 2001, 22, 23–26. [Google Scholar]
- Troianos, C.A.; Hartman, G.S.; Glas, K.E.; Skubas, N.J.; Eberhardt, R.T.; Walker, J.D.; Reeves, S.T. Guidelines for Performing Ultrasound Guided Vascular Cannulation: Recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Anesth. Analg. 2012, 114, 46–72. [Google Scholar] [CrossRef]
- Rupp, S.M.; Apfelbaum, J.L.; Blitt, C.; Caplan, R.A.; Connis, R.T.; Domino, K.B.; Fleisher, L.A.; Grant, S.; Mark, J.B.; Morray, J.P.; et al. Practice guidelines for central venous access: A report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiology 2012, 116, 539–573. [Google Scholar]
- Frankel, H.L.; Kirkpatrick, A.W.; Elbarbary, M.; Blaivas, M.; Desai, H.; Evans, D.; Summerfield, D.T.; Slonim, A.; Breitkreutz, R.; Price, S.; et al. Guidelines for the Appropriate Use of Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients-Part I: General Ultrasonography. Crit. Care Med. 2015, 43, 2479–2502. [Google Scholar] [CrossRef]
- Schmidt, G.A.; Maizel, J.; Slama, M. Ultrasound-guided central venous access: What’s new? Intensive Care Med. 2015, 41, 705–707. [Google Scholar] [CrossRef]
- Blaivas, M.; Brannam, L.; Fernandez, E. Short-axis versus Long-axis approaches for teaching ultrasound-guided vascular access on a new inanimate model. Acad. Emerg. Med. 2003, 10, 1307–1311. [Google Scholar] [CrossRef]
- Chittoodan, S.; Breen, D.; O’Donnell, B.D.; Iohom, G. Long versus Short Axis ultrasound guided approach for internal jugular vein cannulation: A prospective randomised controlled trial. Med. Ultrason. 2011, 13, 21–25. [Google Scholar]
- Blaivas, M.; Adhikari, S. An unseen danger: Frequency of posterior vessel wall penetration by needles during attempts to place internal jugular vein central catheters using ultrasound guidance. Crit. Care Med. 2009, 37, 2345–2349. [Google Scholar] [CrossRef]
- Wilson, J.G.; Breyer, K.E.W. Critical Care Ultrasound: A Review for Practicing Nephrologists. Adv. Chronic Kidney Dis. 2016, 23, 141–145. [Google Scholar] [CrossRef]
- Theodoro, D.; Krauss, M.; Kollef, M.; Evanoff, B. Risk factors for acute adverse events during ultrasound-guided central venous cannulation in the emergency department. Acad. Emerg. Med. 2010, 17, 1055–1061. [Google Scholar] [CrossRef]
- Mehta, N.; Valesky, W.W.; Guy, A.; Sinert, R. Systematic review: Is real-time ultrasonic-guided central-line placement by ED physicians more successful than the traditional landmark approach? Emerg. Med. J. 2013, 30, 355–359. [Google Scholar] [CrossRef]
- Milgram, P.; Kishino, F. A Taxonomy of Mixed Reality Visual Displays. IEICE Trans. Inf. Syst. 1994, E77-D, 1321–1329. [Google Scholar]
- Rochlen, L.R.; Levine, R.; Tait, A.R. First-Person Point-of-View–Augmented Reality for central-line insertion training: A usability and feasibility study. Simul. Healthc. 2017, 12, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.Y.; Thomas, J.B.; Alismail, A.; Cohen, A.; Almutairi, W.; Daher, N.S.; Terry, M.H.; Tan, L.D. The use of augmented reality glasses in central-line simulation: “See one, simulate many, do one competently, and teach everyone”. Adv. Med Educ. Pract. 2018, 9, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Ameri, G.; Baxter, J.S.H.; Bainbridge, D.; Peters, T.M.; Chen, E.C.S. Mixed reality ultrasound guidance system: A case study in system development and a cautionary tale. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 495–505. [Google Scholar] [CrossRef]
- Surry, K.J.M.; Austin, H.J.B.; Fenster, A.; Peters, T.M. Poly(vinyl alcohol) cryogel phantoms for use in ultrasound and MR imaging. Phys. Med. Biol. 2004, 49, 5529–5546. [Google Scholar] [CrossRef]
- Jiang, S.; Liu, S.; Feng, W. PVA hydrogel properties for biomedical application. J. Mech. Behav. Biomed. Mater. 2011, 4, 1228–1233. [Google Scholar] [CrossRef]
- Chu, K.C.; Rutt, B.K. Polyvinyl alcohol cryogel: An ideal phantom material for MR studies of arterial flow and elasticity. Magn. Reson. Med. 1997, 37, 314–319. [Google Scholar] [CrossRef]
- Horn, B.K.P. Closed-form solution of absolute orientation using unit quaternions. J. Opt. Soc. Am. A 1987, 4, 629–642. [Google Scholar] [CrossRef]
- Arun, K.S.; Huang, T.S.; Blostein, S.D. Least-Squares Fitting of Two 3-D Point Sets. IEEE Trans. Pattern Anal. Mach. Intell. 1987, PAMI-9, 698–700. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.C.S.; Peters, T.M.; Ma, B. Guided ultrasound calibration: Where, how, and how many calibration fiducials. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.C.; Lasso, A.; Fichtinger, G. Chapter 31—External tracking devices and tracked tool calibration. In Handbook of Medical Image Computing and Computer Assisted Intervention; Zhou, S.K., Rueckert, D., Fichtinger, G., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 777–794. [Google Scholar]
- Groves, L.A.; Carnahan, P.; Allen, D.R.; Adam, R.; Peters, T.M.; Chen, E.C.S. Accuracy assessment for the co-registration between optical and VIVE head-mounted display tracking. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1207–1215. [Google Scholar] [CrossRef]
- Nguyen, B.V.; Prat, G.; Vincent, J.L.; Nowak, E.; Bizien, N.; Tonnelier, J.M.; Renault, A.; Ould-Ahmed, M.; Boles, J.M.; L’Her, E. Determination of the learning curve for ultrasound-guided jugular central venous catheter placement. Intensive Care Med. 2014, 40, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Gillies, D.J.; Awad, J.; Rodgers, J.R.; Edirisinghe, C.; Cool, D.W.; Kakani, N.; Fenster, A. Three-dimensional therapy needle applicator segmentation for ultrasound-guided focal liver ablation. Med. Phys. 2019, 46, 2646–2658. [Google Scholar] [CrossRef]
- Fenster, A.; Ding, M.; Hu, N.; Ladak, H.M.; Li, G.; Cardinal, N.; Downey, D.B. Visualization and Segmentation Techniques in 3D Ultrasound Images. In Computer Vision Beyond the Visible Spectrum; Springer: London, UK, 2005; pp. 241–269. [Google Scholar]
- Fenster, A.; Surry, K.J.M.; Mills, G.R.M.; Browney, D. 3D ultrasound guided breast biopsy system. Ultrasonics 2004, 42, 769–774. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experts | Mean Difference (mm) | t | pbonf | |
|---|---|---|---|---|
| US Only | Monitor | −0.5 | −0.5 | 1.00 |
| HMD | 2.7 | 3.1 | 0.008 ** | |
| Monitor | HMD | 3.1 | 3.7 | 0.001 ** |
| Novices | Mean Difference (mm) | t | pbonf | |
| US Only | Monitor | 0.5 | 0.300 | 1.00 |
| HMD | 6.4 | 4.0 | 0.001 ** | |
| Monitor | HMD | 6.0 | 3.6 | 0.002 ** |
| Experts | Mean Difference (mm) | t | pbonf | |
|---|---|---|---|---|
| US Only | Monitor | 0.2 | −1.8 | 1.0 |
| HMD | −2.0 | −4.0 | 0.04 * | |
| Monitor | HMD | −2.3 | −2.8 | 0.02 * |
| Novice | Mean Difference (mm) | t | pbonf | |
| US Only | Monitor | −0.07 | −0.05 | 1.0 |
| HMD | −5.0 | −8.7 | 0.005 ** | |
| Monitor | HMD | −4.9 | −3.3 | 0.006 ** |
| Success Rate (%) | US-Only | Monitor | HMD | p | |
|---|---|---|---|---|---|
| Experts | % * | % | % * | 8.034 | 0.018 * |
| Medical Students | % * | % | % * | 13.71 | 0.001 * |
| System | |||
|---|---|---|---|
| Insertion Time | US-Only | Monitor | HMD |
| Experts | |||
| Novices | |||
| CA punctures | US-Only | Monitor | HMD |
| Experts | 1 | 0 | 0 |
| Novices | 2 | 0 | 0 |
| Question | Average Score |
|---|---|
| How viable is the HMD to use in the OR? | 4.35 ± 2.82 |
| If the system was clinically available how often would you use it? | 4.75 ± 2.7 |
| How useful do you think the HMD system would be for training US-guided CVC? | 7.04 ± 2.25 |
| How was the comfort associated with using the HMD? | 7.64 ± 2.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groves, L.; Li, N.; Peters, T.M.; Chen, E.C.S. Towards a First-Person Perspective Mixed Reality Guidance System for Needle Interventions. J. Imaging 2022, 8, 7. https://doi.org/10.3390/jimaging8010007
Groves L, Li N, Peters TM, Chen ECS. Towards a First-Person Perspective Mixed Reality Guidance System for Needle Interventions. Journal of Imaging. 2022; 8(1):7. https://doi.org/10.3390/jimaging8010007
Chicago/Turabian StyleGroves, Leah, Natalie Li, Terry M. Peters, and Elvis C. S. Chen. 2022. "Towards a First-Person Perspective Mixed Reality Guidance System for Needle Interventions" Journal of Imaging 8, no. 1: 7. https://doi.org/10.3390/jimaging8010007
APA StyleGroves, L., Li, N., Peters, T. M., & Chen, E. C. S. (2022). Towards a First-Person Perspective Mixed Reality Guidance System for Needle Interventions. Journal of Imaging, 8(1), 7. https://doi.org/10.3390/jimaging8010007