
Identification of Dermatophyte and Non-Dermatophyte Agents in Onychomycosis by PCR and DNA Sequencing—A Retrospective Comparison of Diagnostic Tools

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Acquisition
2.2. Diagnostic Approach
2.2.1. Fungal DNA Extraction
2.2.2. 28S rDNA Amplification
2.2.3. Species Identification by DNA Sequencing
2.3. Statistics
3. Results
3.1. Whole Study Population
3.2. PCR/Sequencing Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sigurgeirsson, B.; Baran, R. The prevalence of onychomycosis in the global population—A literature study. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1480–1491. [Google Scholar] [CrossRef]
- Gupta, A.K.; Jain, H.C.; Lynde, C.W.; Macdonald, P.; Cooper, E.A.; Summerbell, R.C. Prevalence and epidemiology of onychomycosis in patients visiting physicians’ offices: A multicenter canadian survey of 15,000 patients. J. Am. Acad. Dermatol. 2000, 43, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Faergemann, J.; Baran, R. Epidemiology, clinical presentation and diagnosis of onychomycosis. Br. J. Dermatol. 2003, 149 (Suppl. 65), 1–4. [Google Scholar] [CrossRef] [PubMed]
- Lipner, S.R.; Scher, R.K. Onychomycosis: Clinical overview and diagnosis. J. Am. Acad. Dermatol. 2019, 80, 835–851. [Google Scholar] [CrossRef]
- Eenglish, M.P. Nails and fungi. Br. J. Dermatol. 1976, 94, 697–701. [Google Scholar] [CrossRef]
- Gupta, A.K.; Cooper, E.A.; MacDonald, P.; Summerbell, R.C. Utility of inoculum counting (Walshe and English criteria) in clinical diagnosis of onychomycosis caused by nondermatophytic filamentous fungi. J. Clin. Microbiol. 2001, 39, 2115–2121. [Google Scholar] [CrossRef] [PubMed]
- Summerbell, R.C.; Cooper, E.; Bunn, U.; Jamieson, F.; Gupta, A.K. Onychomycosis: A critical study of techniques and criteria for confirming the etiologic significance of nondermatophytes. Med. Mycol. 2005, 43, 39–59. [Google Scholar] [CrossRef]
- Ameen, M.; Lear, J.T.; Madan, V.; Mohd Mustapa, M.F.; Richardson, M. British Association of Dermatologists’ guidelines for the management of onychomycosis 2014. Br. J. Dermatol. 2014, 171, 937–958. [Google Scholar] [CrossRef] [PubMed]
- Venkatakrishnan, K.; von Moltke, L.L.; Greenblatt, D.J. Effects of the antifungal agents on oxidative drug metabolism: Clinical relevance. Clin. Pharmacokinet. 2000, 38, 111–180. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, D.P.; Voyack, M.J. Onychomycosis: Current trends in diagnosis and treatment. Am. Fam. Physician 2013, 88, 762–770. [Google Scholar] [PubMed]
- Gupta, A.K.; Renaud, H.J.; Quinlan, E.M.; Shear, N.H.; Piguet, V. The Growing Problem of Antifungal Resistance in Onychomycosis and Other Superficial Mycoses. Am. J. Clin. Dermatol. 2021, 22, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Monod, M.; Méhul, B. Recent Findings in Onychomycosis and Their Application for Appropriate Treatment. J. Fungi 2019, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Baudraz-Rosselet, F.; Ruffieux, C.; Lurati, M.; Bontems, O.; Monod, M. Onychomycosis insensitive to systemic terbinafine and azole treatments reveals non-dermatophyte moulds as infectious agents. Dermatology 2010, 220, 164–168. [Google Scholar] [CrossRef]
- Lurati, M.; Baudraz-Rosselet, F.; Vernez, M.; Spring, P.; Bontems, O.; Fratti, M.; Monod, M. Efficacious treatment of non-dermatophyte mould onychomycosis with topical amphotericin B. Dermatology 2011, 223, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Summerbell, R.C.; Venkataraman, M.; Quinlan, E.M. Nondermatophyte mould onychomycosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1628–1641. [Google Scholar] [CrossRef] [PubMed]
- Monod, M.; Feuermann, M.; Salamin, K.; Fratti, M.; Makino, M.; Alshahni, M.M.; Makimura, K.; Yamada, T. Trichophyton rubrum Azole Resistance Mediated by a New ABC Transporter, TruMDR3. Antimicrob. Agents Chemother. 2019, 63, e00863-19. [Google Scholar] [CrossRef]
- Shankarnarayan, S.A.; Shaw, D.; Sharma, A.; Chakrabarti, A.; Dogra, S.; Kumaran, M.S.; Kaur, H.; Ghosh, A.; Rudramurthy, S.M. Rapid detection of terbinafine resistance in Trichophyton species by Amplified refractory mutation system-polymerase chain reaction. Sci. Rep. 2020, 10, 1297. [Google Scholar] [CrossRef]
- Yamada, T.; Yaguchi, T.; Maeda, M.; Alshahni, M.M.; Salamin, K.; Guenova, E.; Feuermann, M.; Monod, M. Gene Amplification of CYP51B: A New Mechanism of Resistance to Azole Compounds in Trichophyton indotineae. Antimicrob. Agents Chemother. 2022, 66, e0005922. [Google Scholar] [CrossRef]
- Yamada, T.; Yaguchi, T.; Salamin, K.; Guenova, E.; Feuermann, M.; Monod, M. MFS1, a Pleiotropic Transporter in Dermatophytes That Plays a Key Role in Their Intrinsic Resistance to Chloramphenicol and Fluconazole. J. Fungi 2021, 7, 542. [Google Scholar] [CrossRef]
- Uhrlaß, S.; Verma, S.B.; Gräser, Y.; Rezaei-Matehkolaei, A.; Hatami, M.; Schaller, M.; Nenoff, P. Trichophyton indotineae—An Emerging Pathogen Causing Recalcitrant Dermatophytoses in India and Worldwide—A Multidimensional Perspective. J. Fungi 2022, 8, 757. [Google Scholar] [CrossRef]
- Weinberg, J.M.; Koestenblatt, E.K.; Tutrone, W.D.; Tishler, H.R.; Najarian, L. Comparison of diagnostic methods in the evaluation of onychomycosis. J. Am. Acad. Dermatol. 2003, 49, 193–197. [Google Scholar] [CrossRef]
- Petinataud, D.; Berger, S.; Contet-Audonneau, N.; Machouart, M. Molecular diagnosis of onychomycosis. J. Mycol. Med. 2014, 24, 287–295. [Google Scholar] [CrossRef]
- Verrier, J.; Monod, M. Diagnosis of Dermatophytosis Using Molecular Biology. Mycopathologia 2017, 182, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Brillowska-Dąbrowska, A.; Nielsen, S.S.; Nielsen, H.V.; Arendrup, M.C. Optimized 5-hour multiplex PCR test for the detection of tinea unguium: Performance in a routine PCR laboratory. Med. Mycol. 2010, 48, 828–831. [Google Scholar] [CrossRef]
- Brillowska-Dabrowska, A.; Saunte, D.M.; Arendrup, M.C. Five-hour diagnosis of dermatophyte nail infections with specific detection of Trichophyton rubrum. J. Clin. Microbiol. 2007, 45, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Monod, M.; Bontems, O.; Zaugg, C.; Léchenne, B.; Fratti, M.; Panizzon, R. Fast and reliable PCR/sequencing/RFLP assay for identification of fungi in onychomycoses. J. Med. Microbiol. 2006, 55, 1211–1216. [Google Scholar] [CrossRef]
- Winter, I.; Uhrlass, S.; Krüger, C.; Herrmann, J.; Bezold, G.; Winter, A.; Barth, S.; Simon, J.C.; Graser, Y.; Nenoff, P. Molecular biological detection of dermatophytes in clinical samples when onychomycosis or tinea pedis is suspected. A prospective study comparing conventional dermatomycological diagnostics and polymerase chain reaction. Hautarzt 2013, 64, 283–289. [Google Scholar] [CrossRef]
- Bontems, O.; Hauser, P.M.; Monod, M. Evaluation of a polymerase chain reaction-restriction fragment length polymorphism assay for dermatophyte and nondermatophyte identification in onychomycosis. Br. J. Dermatol. 2009, 161, 791–796. [Google Scholar] [CrossRef]
- Monod, M.; Baudraz-Rosselet, F.; Ramelet, A.A.; Frenk, E. Direct mycological examination in dermatology: A comparison of different methods. Dermatologica 1989, 179, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Kwong-Chung, K.J.; Bennet, J.E. Medical Mycology; Lea & Febiger: Philadelphia, PA, USA, 1992; pp. 1–806. [Google Scholar]
- Bontems, O.; Fratti, M.; Salamin, K.; Guenova, E.; Monod, M. Epidemiology of Dermatophytoses in Switzerland According to a Survey of Dermatophytes Isolated in Lausanne between 2001 and 2018. J. Fungi 2020, 6, 95. [Google Scholar] [CrossRef]
- Ninet, B.; Jan, I.; Bontems, O.; Lechenne, B.; Jousson, O.; Panizzon, R.; Lew, D.; Monod, M. Identification of dermatophyte species by 28S ribosomal DNA sequencing with a commercial kit. J. Clin. Microbiol. 2003, 41, 826–830. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Gupta, G.; Jain, H.C.; Lynde, C.W.; Foley, K.A.; Daigle, D.; Cooper, E.A.; Summerbell, R.C. The prevalence of unsuspected onychomycosis and its causative organisms in a multicentre Canadian sample of 30,000 patients visiting physicians’ offices. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Wisselink, G.J.; van Zanten, E.; Kooistra-Smid, A.M.D. Trapped in keratin; a comparison of dermatophyte detection in nail, skin and hair samples directly from clinical samples using culture and real-time PCR. J. Microbiol. Methods 2011, 85, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Mügge, C.; Haustein, U.-F.; Nenoff, P. Causative agents of onychomycosis--a retrospective study. J. Dtsch. Dermatol. Ges. 2006, 4, 218–228. [Google Scholar] [CrossRef]
- Verrier, J.; Pronina, M.; Peter, C.; Bontems, O.; Fratti, M.; Salamin, K.; Schürch, S.; Gindro, K.; Wolfender, J.-L.; Harshman, K.; et al. Identification of infectious agents in onychomycoses by PCR-terminal restriction fragment length polymorphism. J. Clin. Microbiol. 2012, 50, 553–561. [Google Scholar] [CrossRef]
- Al-Hatmi, A.M.S.; Bonifaz, A.; Calderón, L.; Curfs-Breuker, I.; Meis, J.F.; van Diepeningen, A.D.; de Hoog, G.S. Proximal subungual onychomycosis caused by Fusarium falciforme successfully cured with posaconazole. Br. J. Dermatol. 2015, 173, 253–255. [Google Scholar] [CrossRef]
- Dhib, I.; Fathallah, A.; Yaacoub, A.; Hadj Slama, F.; Said, M.B.; Zemni, R. Multiplex PCR assay for the detection of common dermatophyte nail infections. Mycoses 2014, 57, 19–26. [Google Scholar] [CrossRef]
- Gustafson, E.; Bakotic, W.; Bennett, L.; Page, L.; McCarthy, L. DNA-based detection for onychomycosis correlates better to histopathology than does fungal culture. Dermatol. Online J. 2019, 25, 13030. [Google Scholar] [CrossRef]
- Walberg, M.; Mørk, C.; Sandven, P.; Jorde, A.T.; Bjørås, M.; Gaustad, P. 18S rDNA polymerase chain reaction and sequencing in onychomycosis diagnostics. Acta Derm. Venereol. 2006, 86, 223–226. [Google Scholar] [CrossRef]
- Mehlig, L.; Garve, C.; Ritschel, A.; Zeiler, A.; Brabetz, W.; Weber, C.; Bauer, A. Clinical evaluation of a novel commercial multiplex-based PCR diagnostic test for differential diagnosis of dermatomycoses. Mycoses 2014, 57, 27–34. [Google Scholar] [CrossRef]
- Trovato, L.; Domina, M.; Calvo, M.; De Pasquale, R.; Scalia, G.; Oliveri, S. Use of real time multiplex PCR for the diagnosis of dermatophytes onychomycosis in patients with empirical antifungal treatments. J. Infect. Public Health 2022, 15, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Beifuss, B.; Bezold, G.; Gottlöber, P.; Borelli, C.; Wagener, J.; Schaller, M.; Korting, H.C. Direct detection of five common dermatophyte species in clinical samples using a rapid and sensitive 24-h PCR-ELISA technique open to protocol transfer. Mycoses 2011, 54, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Spiliopoulou, A.; Bartzavali, C.; Jelastopulu, E.; Anastassiou, E.D.; Christofidou, M. Evaluation of a commercial PCR test for the diagnosis of dermatophyte nail infections. J. Med. Microbiol. 2015, 64, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Luk, N.M.; Hui, M.; Cheng, T.S.; Tang, L.S.; Ho, K.M. Evaluation of PCR for the diagnosis of dermatophytes in nail specimens from patients with suspected onychomycosis. Clin. Exp. Dermatol. 2012, 37, 230–234. [Google Scholar] [CrossRef]
- Gupta, A.K.; Nakrieko, K.-A. Onychomycosis Infections: Do Polymerase Chain Reaction and Culture Reports Agree? J. Am. Podiatr. Med. Assoc. 2017, 107, 280–286. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Whole Study Population n = 16,094 | PCR/Sequencing Group n = 1148 | ||
|---|---|---|---|
| Age Median years (IQR 1) | 53 (23) | 54 (21) | |
| Sex n (%) | Female | 10,066 (62.5%) | 668 (58.2%) |
| Male | 6028 (37.5%) | 480 (41.8%) | |
| Sampling site N 3 (%) | Toenails | 12,170 (75.6%) | 925 (80.6%) |
| Fingernails | 1118 (7%) | 74 (6.4%) | |
| Nail NOS 2 | 2745 (17.1%) | 147 (12.8%) | |
| Subungual mass | 57 (0.4%) | 1 (0.1%) | |
| Detection of fungal elements by diagnostic methods n (%) | Positive Microscopy | 10,967 (68.1%) | 1145 (99.7%) |
| Positive Culture | 4617 (28.7%) | 250 (21.8%) | |
| Positive Sequencing | - | 729 (63.5%) | |
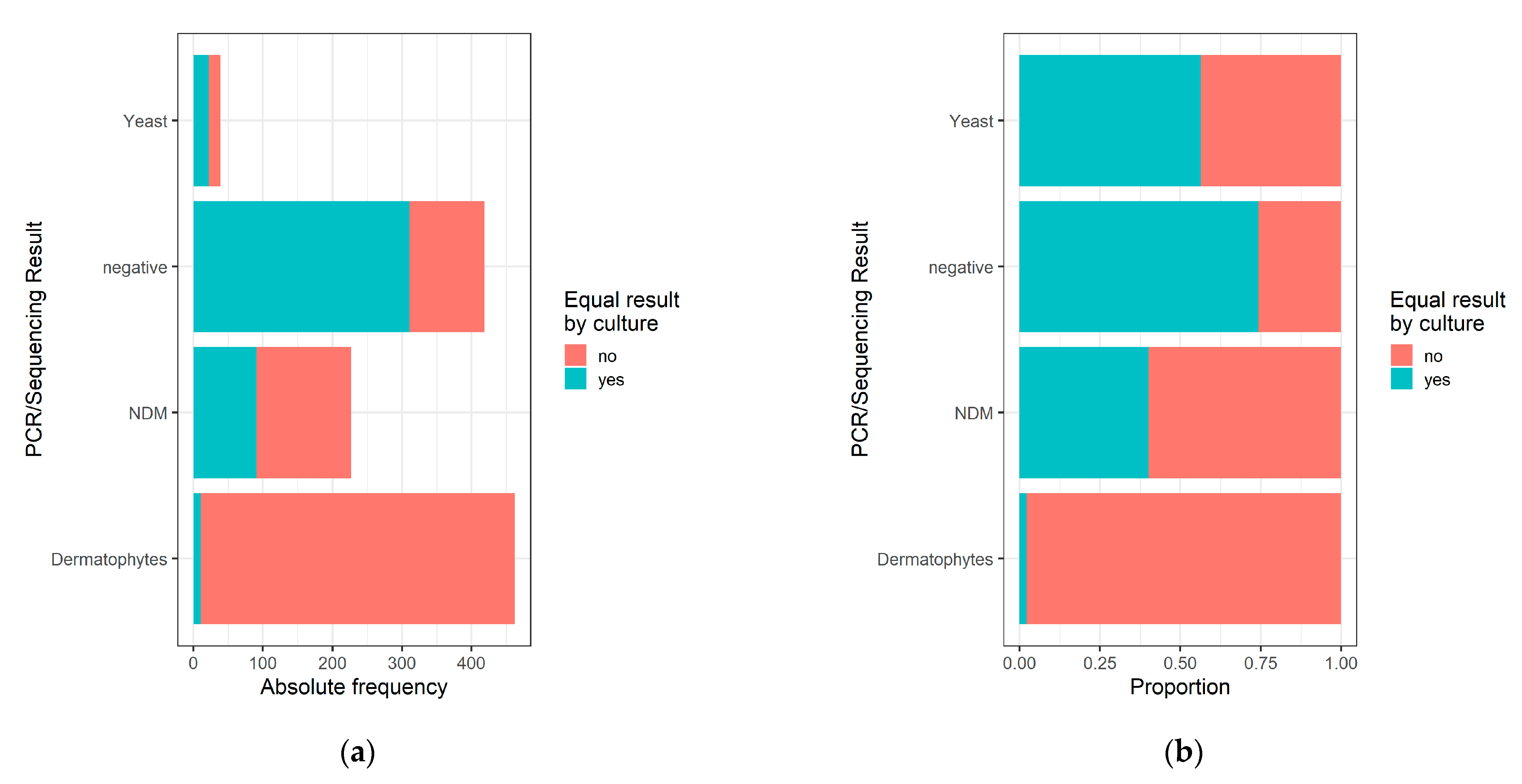
| PCR/Sequencing Results | |||||
|---|---|---|---|---|---|
| Dermatophyte | Yeast | NDM | Negative/Contamination | ||
| Culture Result | Dermatophyte n = 12 | 10 (2.2%) | 0 (0%) | 1 (0.4%) | 1 (0.2%) |
| Yeast n = 65 | 4 (0.9%) | 22 (56.4%) | 5 (2.2%) | 34 (8.1%) | |
| NDM n = 169 | 5 (1.1%) | 3 (7.7%) | 91 (40.1%) | 70 (16.7%) | |
| Mixed infection n = 4 | 1 (0.2%) | 0 (0%) | 0 (0%) | 3 (0.7%) | |
| Negative/Contamination n = 898 | 443 (95.7%) | 14 (35.9%) | 130 (57.3%) | 311 (74.2%) | |
| Total n = 1148 | 463 (100%) | 39 (100%) | 227 (100%) | 419 (100%) | |
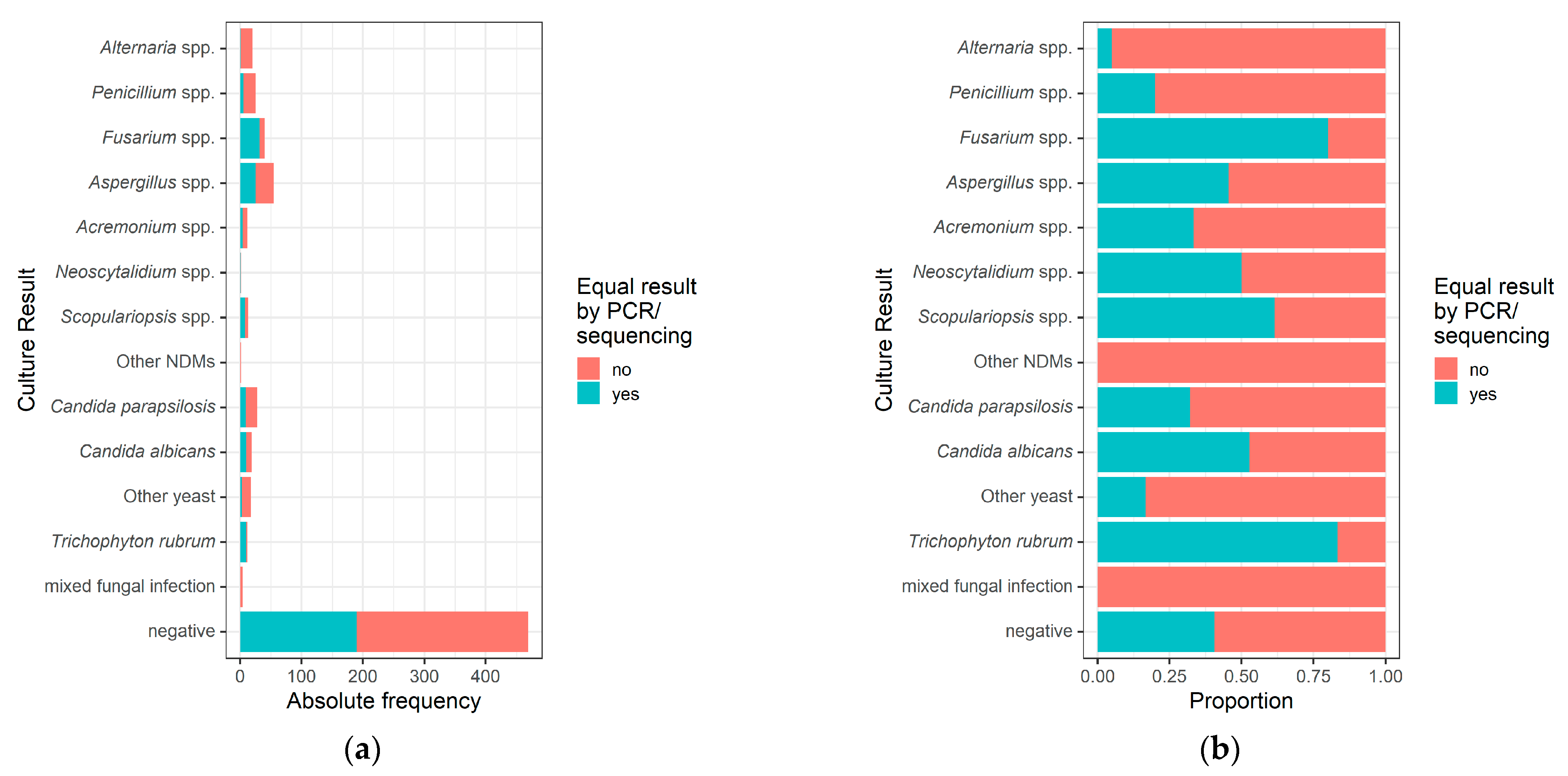
| Culture Result | Comparison With PCR/Sequencing | |||||
|---|---|---|---|---|---|---|
| Equal Result | Discordant Result | |||||
| NDM | Dermatophyte | Yeast | Negative | |||
| NDM n = 169 | Aspergillus spp. n = 55 | 25 (45%) | 2 (4%) | 1 (2%) | 2 (4%) | 25 (45%) |
| Fusarium spp. n = 40 | 32 (80%) | 0 (0%) | 3 (8%) | 0 (0%) | 5 (12%) | |
| Penicillium spp. n = 25 | 5 (20%) | 6 (24%) | 0 (0%) | 1 (4%) | 13 (52%) | |
| Alternaria spp. n = 20 | 1 (5%) | 5 (25%) | 0 (0%) | 0 (0%) | 14 (70%) | |
| Scopulariopsis spp. n = 13 | 8 (62%) | 0 (0%) | 0 (0%) | 0 (0%) | 5 (38%) | |
| Acremonium spp. n = 12 | 4 (33%) | 3 (25%) | 0 (0%) | 0 (0%) | 5 (42%) | |
| Neoscytalidium spp. n = 2 | 1 (50%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (50%) | |
| Other NDMs n = 2 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (100%) | |
| Yeast n = 65 | Candida parapsilosis n = 28 | 9 (32%) | 3 (11%) | 1 (4%) | 0 (0%) | 15 (54%) |
| Candida albicans n = 19 | 10 (53%) | 0 (0%) | 1 (5%) | 0 (0%) | 8 (42%) | |
| Other yeast n = 18 | 3 (17%) | 2 (11%) | 2 (11%) | 0 (0%) | 11 (61%) | |
| Dermatophytes n = 12 | Trichophyton rubrum n = 12 | 10 (83%) | 1 (8%) | 0 (0%) | 0 (0%) | 1 (8%) |
| Mixed fungal infection (NDM + yeast) n = 4 | 0 (0%) | 0 (0%) | 1 (25%) | 0 (0%) | 3 (75%) | |
| Contamination (NDM) n = 149 | 0 (0%) | 24 (16%) | 101 (68%) | 6 (4%) | 18 (12%) | |
| Contamination (yeast) n = 15 | 0 (0%) | 0 (0%) | 15 (100%) | 0 (0%) | 0 (0%) | |
| Contamination (bacteria) n = 265 | 0 (0%) | 39 (15%) | 120 (45%) | 3 (1%) | 103 (39%) | |
| Negative n = 469 | 190 (41%) | 67 (14%) | 207 (44%) | 5 (1%) | 0 (0%) | |
| Total n = 1148 | 298 (26%) | 152 (13%) | 452 (39%) | 17 (2%) | 229 (20%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pospischil, I.; Reinhardt, C.; Bontems, O.; Salamin, K.; Fratti, M.; Blanchard, G.; Chang, Y.-T.; Wagner, H.; Hermann, P.; Monod, M.; et al. Identification of Dermatophyte and Non-Dermatophyte Agents in Onychomycosis by PCR and DNA Sequencing—A Retrospective Comparison of Diagnostic Tools. J. Fungi 2022, 8, 1019. https://doi.org/10.3390/jof8101019
Pospischil I, Reinhardt C, Bontems O, Salamin K, Fratti M, Blanchard G, Chang Y-T, Wagner H, Hermann P, Monod M, et al. Identification of Dermatophyte and Non-Dermatophyte Agents in Onychomycosis by PCR and DNA Sequencing—A Retrospective Comparison of Diagnostic Tools. Journal of Fungi. 2022; 8(10):1019. https://doi.org/10.3390/jof8101019
Chicago/Turabian StylePospischil, Isabella, Charlotte Reinhardt, Olympia Bontems, Karine Salamin, Marina Fratti, Gabriela Blanchard, Yun-Tsan Chang, Helga Wagner, Philipp Hermann, Michel Monod, and et al. 2022. "Identification of Dermatophyte and Non-Dermatophyte Agents in Onychomycosis by PCR and DNA Sequencing—A Retrospective Comparison of Diagnostic Tools" Journal of Fungi 8, no. 10: 1019. https://doi.org/10.3390/jof8101019
APA StylePospischil, I., Reinhardt, C., Bontems, O., Salamin, K., Fratti, M., Blanchard, G., Chang, Y.-T., Wagner, H., Hermann, P., Monod, M., Hoetzenecker, W., & Guenova, E. (2022). Identification of Dermatophyte and Non-Dermatophyte Agents in Onychomycosis by PCR and DNA Sequencing—A Retrospective Comparison of Diagnostic Tools. Journal of Fungi, 8(10), 1019. https://doi.org/10.3390/jof8101019