
Fearless in Physical Activity: The Implications of Community-Based Physical Activity Interventions on Children, Adolescents, and Adults with Congenital Heart Disease

 ,
,
Abstract
1. Introduction
2. Results
2.1. Participant Demographics
2.2. The Intrinsic Motivation Inventory
2.3. Perceived Competence Scale
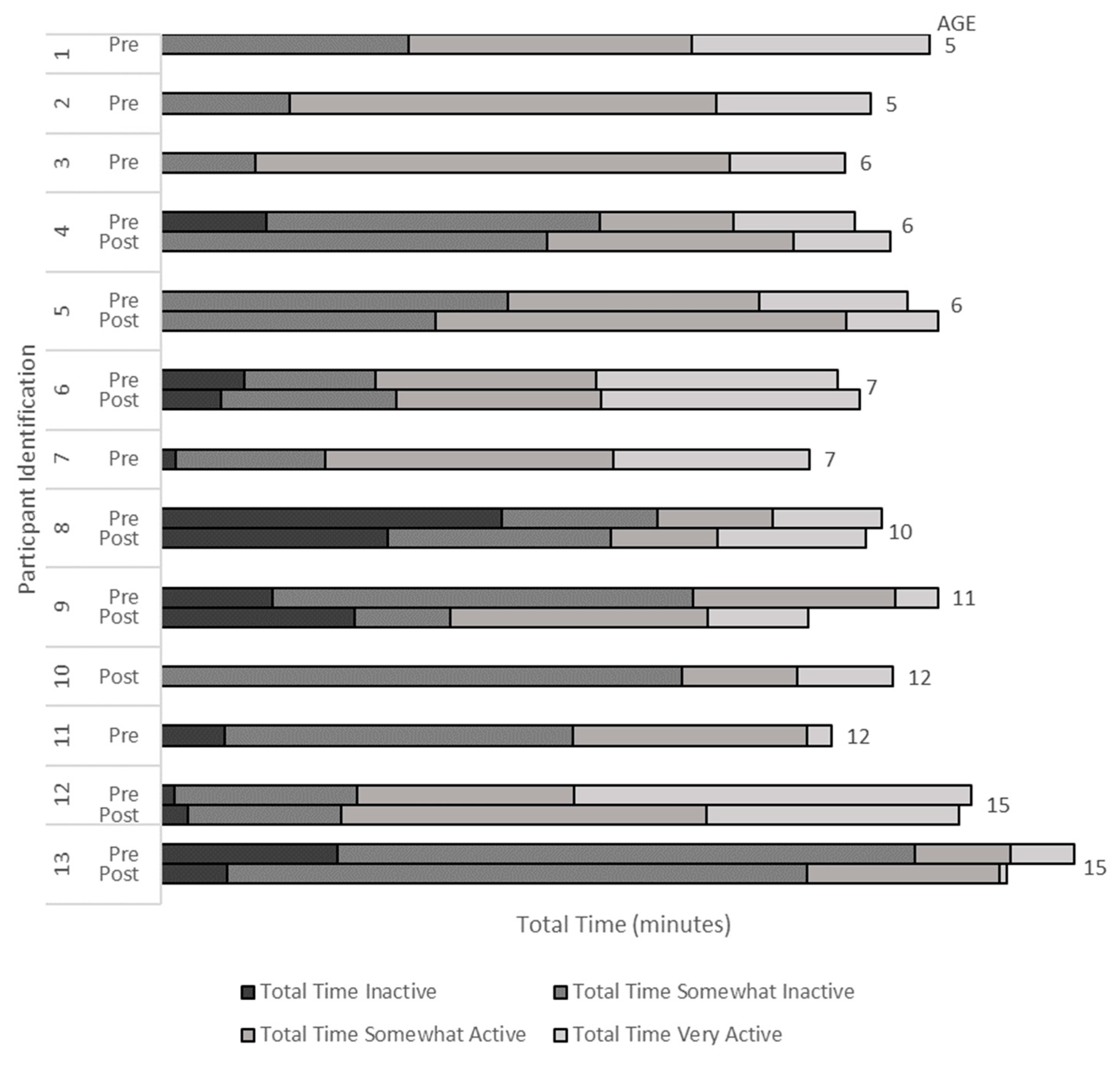
2.4. Habitual Activity Estimation Scale Total Physical Activity Levels
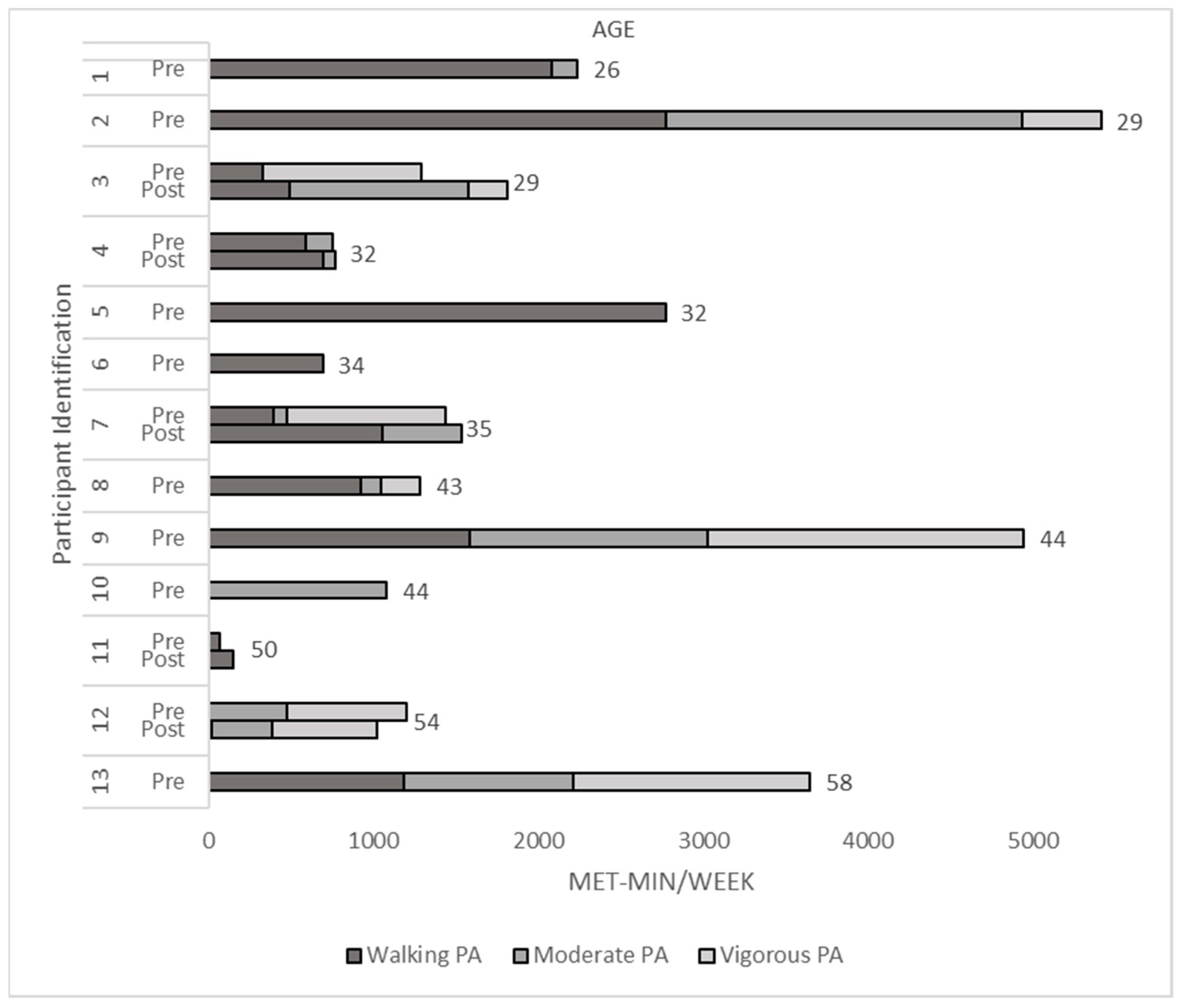
2.5. The International Physical Activity Questionnaire
2.6. Post-Event Feedback
3. Discussion
3.1. Fearless Impacts on Physical Activity Motivation and Perceived Competence
3.2. Fearless Impacts on Physical Activity Behaviour
3.3. Perceptions of the Fearless Physical Activity Intervention
3.4. Strengths and Limitations
4. Materials and Methods
4.1. Participants and Recruitment
4.2. Data Collection
4.2.1. Events
4.2.2. Recruitment
4.2.3. Assessments and Outcomes
4.3. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krasuski, R.A.; Bashore, T.M. Congenital Heart Disease Epidemiology in the United States: Blindly Feeling for the Charging Elephant. Circulation 2016, 134, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Mackie, A.S.; Tran, D.T.; Marelli, A.J.; Kaul, P. Cost of congenital heart disease hospitalizations in Canada: A population-based study. Can. J. Cardiol. 2017, 33, 792–798. [Google Scholar] [CrossRef]
- Mandalenakis, Z.; Giang, K.W.; Eriksson, P.; Liden, H.; Synnergren, M.; Wåhlander, H.; Fedchenko, M.; Rosengren, A.; Dellborg, M. Survival in Children with Congenital Heart Disease: Have We Reached a Peak at 97%? J. Am. Heart Assoc. 2020, 9, e017704. [Google Scholar] [CrossRef] [PubMed]
- Dua, J.S.; Cooper, A.R.; Fox, K.R.; Graham Stuart, A. Exercise training in adults with congenital heart disease: Feasibility and benefits. Int. J. Cardiol. 2010, 138, 196–205. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American heart association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Voss, C.; Duncombe, S.L.; Dean, P.H.; De Souza, A.M.; Harris, K.C. Physical activity and sedentary behavior in children with congenital heart disease. J. Am. Heart Assoc. 2017, 6, e004665. [Google Scholar] [CrossRef]
- Colley, R.C.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian children and youth: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011, 22, 15–23. [Google Scholar]
- Bull, F.; Saad Al-Ansari, S.; Biddle, S.; Borodulin, K.; Buman, M.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Longmuir, P.E.; Russell, J.L.; Corey, M.; Faulkner, G.; McCrindle, B.W. Factors associated with the physical activity level of children who have the Fontan procedure. Am. Heart J. 2011, 161, 411–417. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Brothers, J.A.; De Ferranti, S.D.; Hayman, L.L.; Van Hare, G.F.; Matherne, G.P.; Davis, C.K.; Joy, E.A.; McCrindle, B.W. Promotion of physical activity for children and adults with congenital heart disease: A scientific statement from the American Heart Association. Circulation 2013, 127, 2147–2159. [Google Scholar] [CrossRef]
- Takken, T.; Giardini, A.; Reybrouck, T.; Gewillig, M.; Hövels-Gürich, H.H.H.; Longmuir, P.E.; McCrindle, B.W.; Paridon, S.M.; Hager, A. Recommendations for physical activity, recreation sport, and exercise training in paediatric patients with congenital heart disease: A report from the Exercise, Basic & Translational Research Section of the European Association of Cardiovascular Preve. Eur. J. Prev. Cardiol. 2012, 19, 1034–1065. [Google Scholar] [PubMed]
- Tran, D.; Maiorana, A.; Ayer, J.; Lubans, D.R.; Davis, G.M.; Celermajer, D.S.; d’Udekem, Y.; Cordina, R. Recommendations for exercise in adolescents and adults with congenital heart disease. Prog. Cardiovasc. Dis. 2020, 63, 350–366. [Google Scholar] [CrossRef] [PubMed]
- Lunt, D.; Briffa, T.; Briffa, N.K.; Ramsay, J. Physical activity levels of adolescents with congenital heart disease. Aust. J. Physiother. 2003, 49, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Swan, L.; Hillis, W.S. Exercise prescription in adults with congenital heart disease: A long way to go. Heart 2000, 83, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Chaix, M.-A.; Marcotte, F.; Dore, A.; Mongeon, F.-P.; Mondésert, B.; Mercier, L.-A.; Khairy, P. Risks and Benefits of Exercise Training in Adults With Congenital Heart Disease. Can. J. Cardiol. 2016, 32, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Dua, J.S.; Cooper, A.R.; Fox, K.R.; Graham Stuart, A. Physical activity levels in adults with congenital heart disease. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 287–293. [Google Scholar] [CrossRef]
- Moola, F.; McCrindle, B.W.; Longmuir, P.E. Physical activity participation in youth with surgically corrected congenital heart disease: Devising guidelines so Johnny can participate. Paediatr. Child Health 2009, 14, 167–170. [Google Scholar] [CrossRef]
- Budts, W.; Börjesson, M.; Chessa, M.; Van Buuren, F.; Trigo Trindade, P.; Corrado, D.; Heidbuchel, H.; Webb, G.; Holm, J.; Papadakis, M. Physical activity in adolescents and adults with congenital heart defects: Individualized exercise prescription. Eur. Heart J. 2013, 34, 3669–3674. [Google Scholar] [CrossRef]
- Williams, C.A.; Wadey, C.; Pieles, G.; Stuart, G.; Taylor, R.S.; Long, L. Physical activity interventions for people with congenital heart disease. Cochrane Database Syst. Rev. 2020, 10, CD013400. [Google Scholar] [CrossRef][Green Version]
- Duppen, N.; Takken, T.; Hopman, M.T.E.; Ten Harkel, A.D.J.; Dulfer, K.; Utens, E.M.; Helbing, W.A. Systematic review of the effects of physical exercise training programmes in children and young adults with congenital heart disease. Int. J. Cardiol. 2013, 168, 1779–1787. [Google Scholar] [CrossRef]
- Berghammer, M.C.; Mattsson, E.; Johansson, B.; Moons, P.; Dellborg, M. Comparison of participants and non-participants in patient-reported outcome surveys: The case of Assessment of Patterns of Patient-Reported Outcomes in Adults with Congenital Heart disease—International Study. Cardiol. Young 2017, 27, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Babic, M.J.; Morgan, P.J.; Plotnikoff, R.C.; Lonsdale, C.; White, R.L.; Lubans, D.R. Physical Activity and Physical Self-Concept in Youth: Systematic Review and Meta-Analysis. Sport Med. 2014, 44, 1589–1601. [Google Scholar] [CrossRef] [PubMed]
- Havitz, M.E.; Kaczynski, A.T.; Mannell, R.C. Exploring Relationships Between Physical Activity, Leisure Involvement, Self-Efficacy, and Motivation via Participant Segmentation. Leis. Sci. 2013, 35, 45–62. [Google Scholar] [CrossRef]
- Banks, L.; Rosenthal, S.; Manlhiot, C.; Fan, C.P.; McKillop, A.; Longmuir, P.E.; McCrindle, B.W. Exercise Capacity and Self-Efficacy are Associated with Moderate-to-Vigorous Intensity Physical Activity in Children with Congenital Heart Disease. Pediatr. Cardiol. 2017, 38, 1206–1214. [Google Scholar] [CrossRef]
- Huitt, W.; Hummel, J. Piaget’s theory of cognitive development. Educ. Psychol. Interact. 2003, 3, 1–5. [Google Scholar]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel. In A Guide to Designing Interventions, 1st ed.; Silverback Publishing: London, UK, 2014; pp. 1003–1010. [Google Scholar]
- Stone, N.; Obeid, J.; Dillenburg, R.; Milenkovic, J.; MacDonald, M.J.; Timmons, B.W. Objectively measured physical activity levels of young children with congenital heart disease. Cardiol. Young 2015, 25, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Dighero, R.; Torres-Castro, R.; Rodríguez-Núñez, I.; Rosales-Fuentes, J.; Vilaró, J.; Fregonezi, G.; Lopetegui, B. Physical activity assessments in children with congenital heart disease: A systematic review. Acta Paediatr. 2020, 109, 2479–2490. [Google Scholar] [CrossRef]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e698–e800. [Google Scholar]
- Müller, J.; Amberger, T.; Berg, A.; Goeder, D.; Remmele, J.; Oberhoffer, R.; Ewert, P.; Hager, A. Physical activity in adults with congenital heart disease and associations with functional outcomes. Heart 2017, 103, 1117–1121. [Google Scholar] [CrossRef]
- Morrison, M.L.; Sands, A.J.; McCusker, C.G.; McKeown, P.P.; McMahon, M.; Gordon, J.; Casey, F.A. Exercise training improves activity in adolescents with congenital heart disease. Heart 2013, 99, 1122–1128. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Shmotkin, D.; Goldberg, S. Predictors of Longitudinal Changes in Older Adults’ Physical Activity Engagement. J. Aging Phys. Act. 2010, 18, 141–157. [Google Scholar] [CrossRef] [PubMed]
- Giannakoulas, G.; Dimopoulos, K. Exercise training in congenital heart disease: Should we follow the heart failure paradigm? Int. J. Cardiol. 2010, 138, 109–111. [Google Scholar] [CrossRef] [PubMed]
- McKillop, A.; McCrindle, B.W.; Dimitropoulos, G.; Kovacs, A.H. Physical activity perceptions and behaviors among young adults with congenital heart disease: A mixed-methods study. Congenit. Heart Dis. 2018, 13, 232–240. [Google Scholar] [CrossRef]
- Moola, F.; Faulkner, G.E.J.; Kirsh, J.A.; Kilburn, J. Physical activity and sport participation in youth with congenital heart disease: Perceptions of children and parents. Adapt. Phys. Activ. Q. 2008, 25, 49–70. [Google Scholar] [CrossRef] [PubMed]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Los Angeles, CA, USA, 2014. [Google Scholar]
- Marasso, D.; Lupo, C.; Collura, S.; Rainoldi, A.; Brustio, P.R. Subjective versus Objective Measure of Physical Activity: A Systematic Review and Meta-Analysis of the Convergent Validity of the Physical Activity Questionnaire for Children (PAQ-C). Int. J. Environ. Res. Public Health 2021, 18, 3413. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Langendorfer, S.J.; Goodway, J.D.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- McAuley, E.D.; Duncan, T.; Tammen, V.V. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: A confirmatory factor analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef]
- Hay, J.A.; Cairney, J. Development of the Habitual Activity Estimation Scale for clinical research: A systematic approach. Pediatr. Exerc. Sci. 2006, 18, 193–202. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Braun, V.; Clark, V. Using Thematic Analysis Psychology. Qual. Res. Psychol. 2006, 3, 7–9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participant Demographics | Intrinsic Motivation | Perceived Competence Scale | Habitual Activity Estimation Score 1 | International Physical Activity Questionnaire | ||
|---|---|---|---|---|---|---|
| Youth | Pre and Post | n = x Age Sex | n = 8 10.25 ± 3.7 5M, 3F | n = 9 10.44 ± 3.5 5M, 4F | n = 7 10.00 ± 3.92 4M, 3F | |
| Pre only | n = x Age Sex | n = 8 7.50 ± 3.2 4M, 4F | n = 7 6.85 ± 2.79 4M, 3F | n = 6 7.83 ± 3.31 3M, 3F | ||
| Adult | Pre and Post | n = x Age Sex | n = 7 43.14 ± 11.4 0M, 7F | n = 8 42.00 ± 11.0 0M, 8F | n = 5 40.00 ± 11.24 0M, 5F | |
| Pre only | n = x Age Sex | n = 9 38.56 ± 8.75 2M, 7F | n = 8 39.13 ± 9.17 2M, 6F | n = 8 38.75 ± 10.48 2M, 6F |
| Age Group | Pre- and/or Post-Event 1 | Data Reported | Intrinsic Motivation Inventory | Perceived Competence Scale |
|---|---|---|---|---|
| Youth | Pre-event all | n = x Mean and SD Sex | n = 8 5.32 ± 1.10 4M; 4F | n = 9 5.47 ± 1.35 5M; 4F |
| Post-event all | n = x Mean and SD | n = 8 5.00 ± 0.89 | n = 9 5.66 ± 1.27 | |
| Pre- vs. Post-event | p-value Cohen’s d | 0.19 0.31 | 0.62 0.14 | |
| Pre-event only | n = x Mean and SD Sex | n = 8 5.71 ± 0.69 4M; 4F | n = 7 6.63 ± 0.33 4M; 3F | |
| Pre- only vs. Pre-event all | p-value Cohen’s d | 0.49 0.42 | 0.03 1.18 | |
| Adult | Pre-event all | n = x Mean and SD | n = 7 5.06 ± 0.99 | n = 8 4.18 ± 1.93 |
| Post-event all | n = x Mean and SD | n = 7 5.00 ± 0.81 | n = 8 4.43 ± 1.50 | |
| Pre- vs. Post-event | p-value Cohen’s d | 0.60 0.06 | 0.33 0.14 | |
| Pre-event only | n = x Mean and SD Sex | n = 9 4.68 ± 1.38 2M; 7F | n = 8 4.78 ± 2.23 0M; 7F | |
| Pre only vs. Pre-event all | p-value Cohen’s d | 0.53 0.32 | 0.42 0.34 |
| Spring | Summer | Fall | Winter | |
|---|---|---|---|---|
| Fearless Event Schedule (no seasonal changes) | Introduction/Icebreaker Physical Activity #1 Education Session#1 Break—Snack/Rest Physical Activity #2 Education Session #2 Physical Activity #3 1 End of Session Discussion/Feedback | |||
| Physical Activity Opportunities | Yoga Frisbee Bocce Nature Walk Cooperative Games Yoga Frisbee Bocce Nature Walk Cooperative Games 2 | Tai Chi Zumba Cooperative Games 2 | Badminton Outdoor Low Ropes Course Cooperative Games 2 | Capoeira Pickleball (select locations) Cooperative Games 2 |
| Educational Sessions | Self-Awareness 24 h Movement Guidelines | Physical Activity Communication Body Awareness | Self-Monitoring Breathing Community Resources for Physical Activity | Creating Connections Goal Setting |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chubbs-Payne, A.; Yaraskavitch, J.; Lai, L.; Graham, J.; DesClouds, P.; Longmuir, P.E. Fearless in Physical Activity: The Implications of Community-Based Physical Activity Interventions on Children, Adolescents, and Adults with Congenital Heart Disease. J. Cardiovasc. Dev. Dis. 2023, 10, 11. https://doi.org/10.3390/jcdd10010011
Chubbs-Payne A, Yaraskavitch J, Lai L, Graham J, DesClouds P, Longmuir PE. Fearless in Physical Activity: The Implications of Community-Based Physical Activity Interventions on Children, Adolescents, and Adults with Congenital Heart Disease. Journal of Cardiovascular Development and Disease. 2023; 10(1):11. https://doi.org/10.3390/jcdd10010011
Chicago/Turabian StyleChubbs-Payne, Adam, Jenna Yaraskavitch, Lillian Lai, Jennifer Graham, Poppy DesClouds, and Patricia E. Longmuir. 2023. "Fearless in Physical Activity: The Implications of Community-Based Physical Activity Interventions on Children, Adolescents, and Adults with Congenital Heart Disease" Journal of Cardiovascular Development and Disease 10, no. 1: 11. https://doi.org/10.3390/jcdd10010011
APA StyleChubbs-Payne, A., Yaraskavitch, J., Lai, L., Graham, J., DesClouds, P., & Longmuir, P. E. (2023). Fearless in Physical Activity: The Implications of Community-Based Physical Activity Interventions on Children, Adolescents, and Adults with Congenital Heart Disease. Journal of Cardiovascular Development and Disease, 10(1), 11. https://doi.org/10.3390/jcdd10010011