
Biplanar High-Speed Fluoroscopy of Pony Superficial Digital Flexor Tendon (SDFT)—An In Vivo Pilot Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Animal
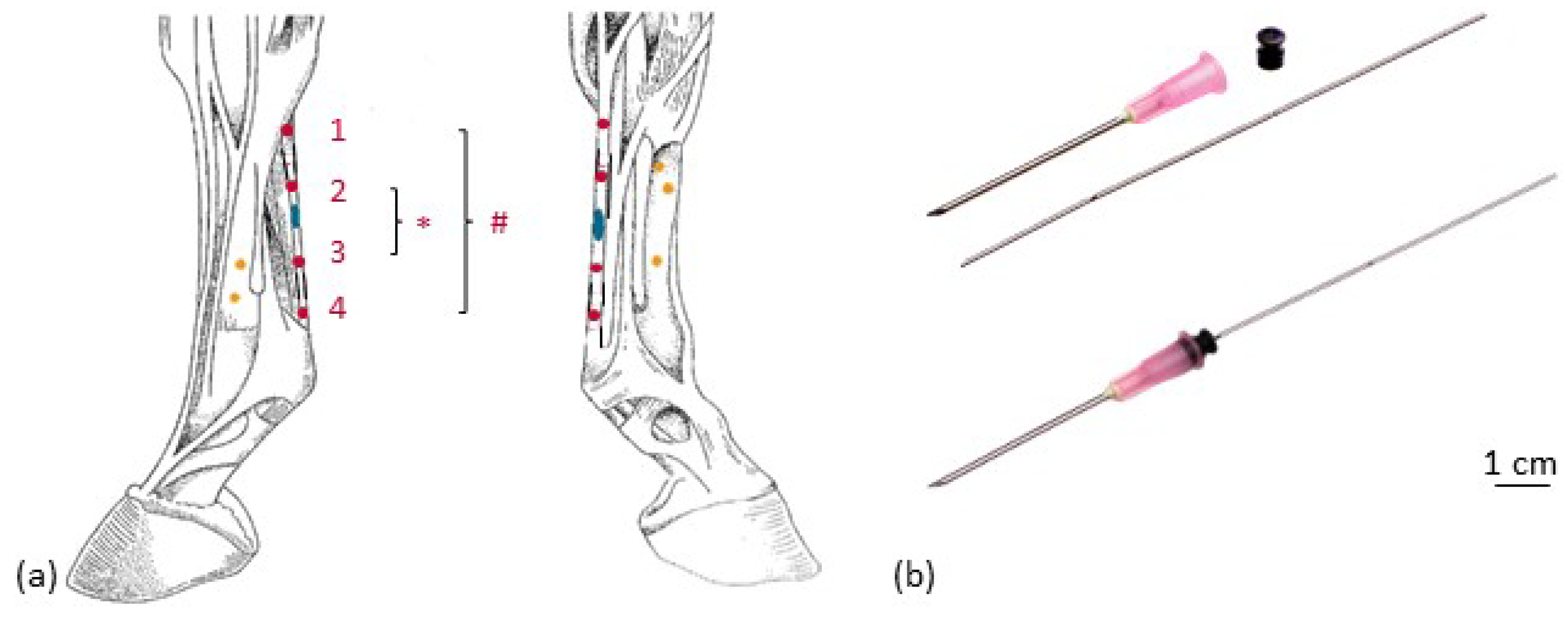
2.2. Implantation of Markers
2.3. Injection of Collagenase
2.4. Examinations and Treatment
2.5. Biplanar High-Speed Fluoroscopy
3. Results
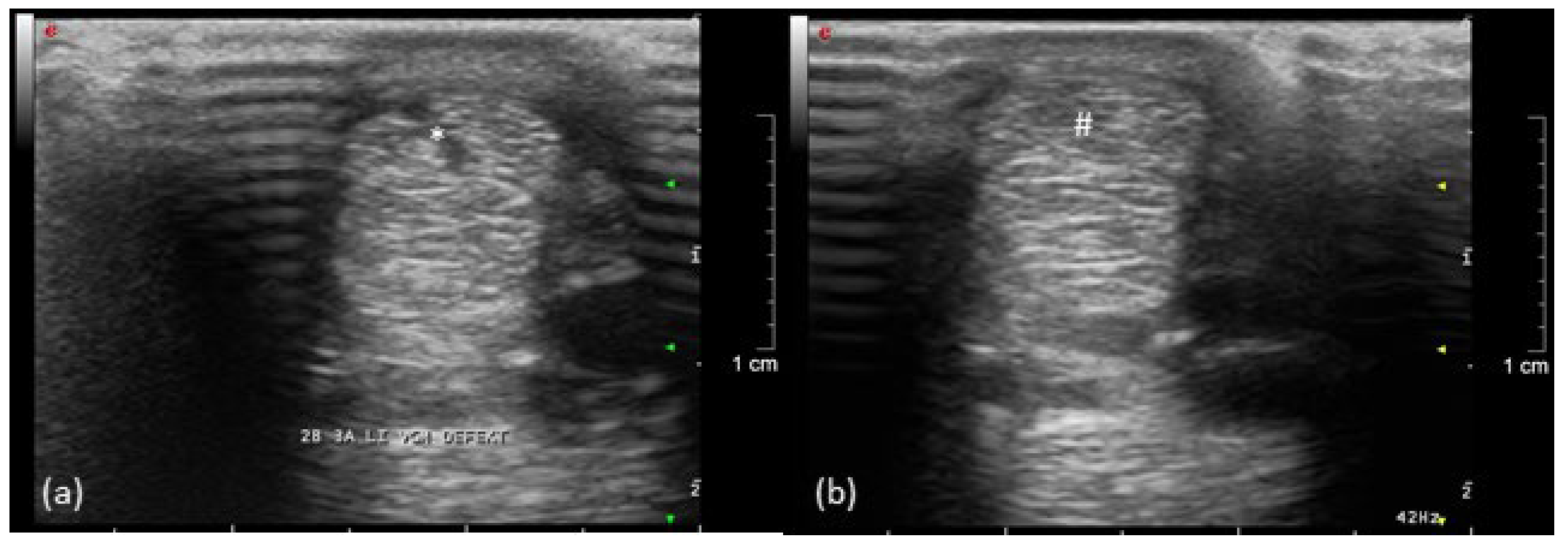
3.1. Clinical Examination Including Ultrasound and Computed Tomography
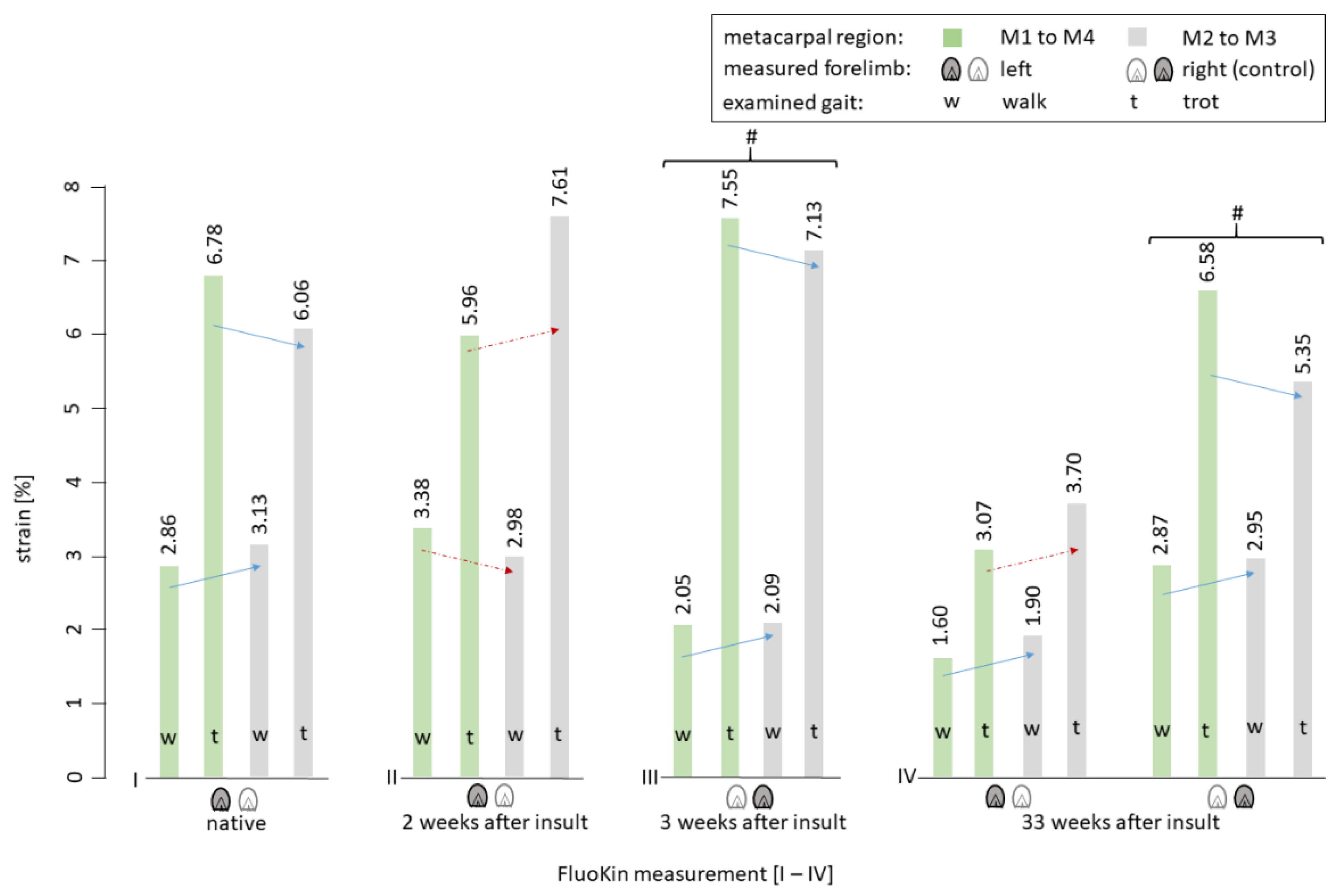
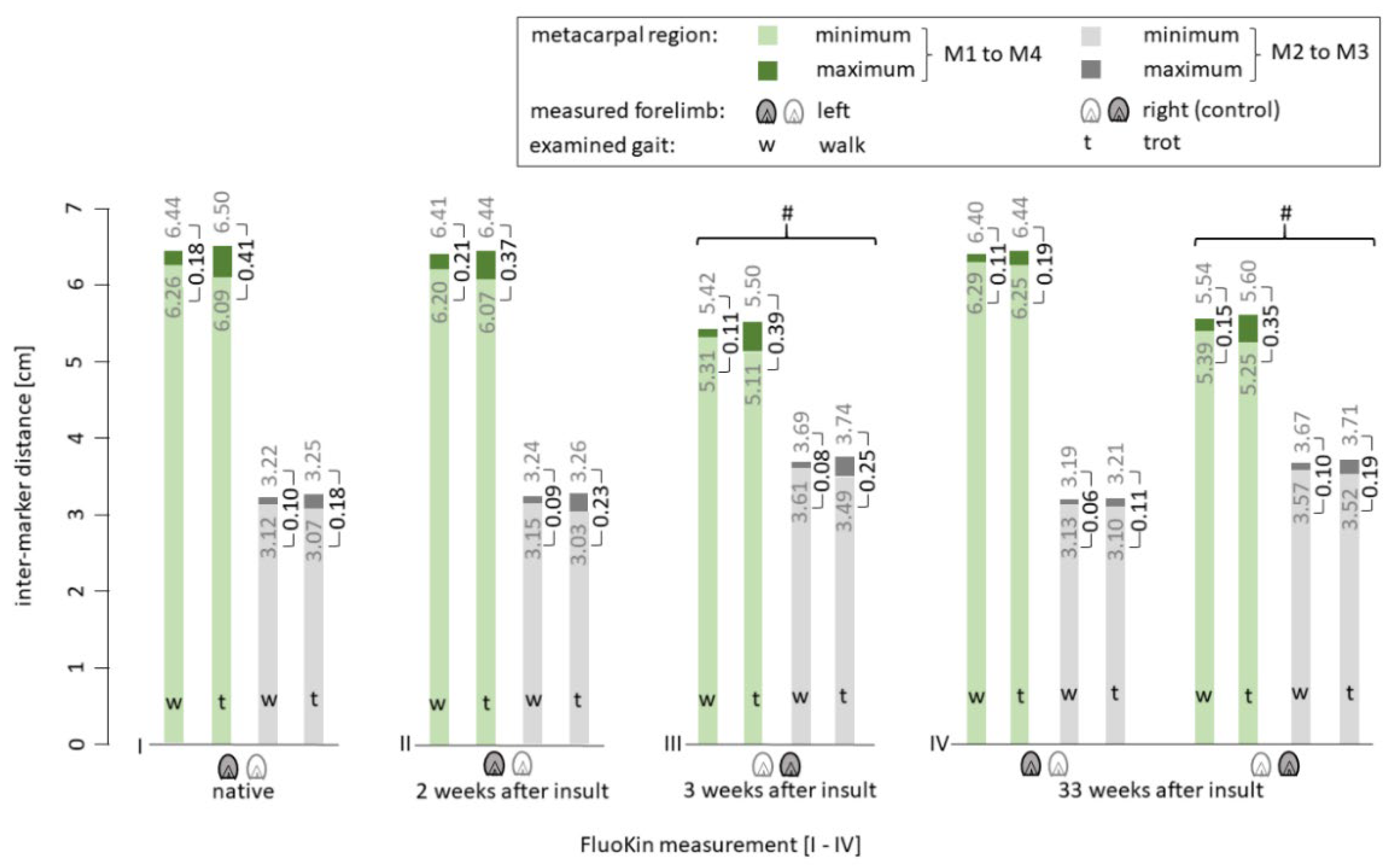
3.2. Biplanar High-Speed Fluoroscopy
4. Discussion
4.1. Clinical Examination
4.2. Ultrasound Examination
4.3. Biplanar High-Speed Fluoroscopy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, R.B.; Harkins, L.S.; Hammond, C.J.; Wood, J.L. Racehorse injuries, clinical problems and fatalities recorded on British racecourses from flat racing and National Hunt racing during 1996, 1997 and 1998. Equine Vet. J. 2001, 33, 478–486. [Google Scholar] [CrossRef]
- Smith, R.K.W.; Birch, H.L.; Goodman, S.; Heinegård, D.; Goodship, A.E. The influence of ageing and exercise on tendon growth and degeneration–Hypotheses for the initiation and prevention of strain-induced tendinopathies. Comp. Biochem. Physiol. Part. A Mol. Integr. Physiol. 2002, 133, 1039–1050. [Google Scholar] [CrossRef]
- Butcher, M.T.; Hermanson, J.W.; Ducharme, N.G.; Mitchell, L.M.; Soderholm, L.V.; Bertram, J.E.A. Superficial digital flexor tendon lesions in racehorses as a sequela to muscle fatigue: A preliminary study. Equine Vet. J. 2007, 39, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Patterson-Kane, J.C.; Firth, E.C. The pathobiology of exercise-induced superficial digital flexor tendon injury in Thoroughbred racehorses. Vet. J. 2009, 181, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Wollenman, P.; McMahon, P.J.; Knapp, S.; Ross, M.W. Lameness in the Polo Pony. In Diagnosis and Management of Lameness in the Horse, 2nd ed.; Ross, M.W., Dyson, S.J., Eds.; Elsevier/Saunders: St. Louis, MO, USA, 2011; pp. 1149–1164. [Google Scholar]
- Davis, C.S.; Smith, R.K.W. Diseases of tendon and ligament disorders. In Equine Surgery, 3rd ed.; Auer, J.A., Stick, J.A., Eds.; W.B. Saunders: St. Louis, MO, USA, 2006. [Google Scholar]
- Dyson, S.J. Medical management of superficial digital flexor tendonitis: A comparative study in 219 horses (1992–2000). Equine Vet. J. 2004, 36, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, C.T.; Clegg, P.D.; Birch, H.L. A review of tendon injury: Why is the equine superficial digital flexor tendon most at risk? Equine Vet. J. 2010, 42, 174–180. [Google Scholar] [CrossRef]
- Patterson-Kane, J.C.; Becker, D.L.; Rich, T. The pathogenesis of tendon microdamage in athletes: The horse as a natural model for basic cellular research. J. Comp. Pathol. 2012, 147, 227–247. [Google Scholar] [CrossRef]
- McCullagh, K.G.; Goodship, A.E.; Silver, I.A. Tendon injuries and their treatment in the horse. Vet. Rec. 1979, 105, 54–57. [Google Scholar] [CrossRef]
- Goodship, A.E.; Birch, H.L.; Wilson, A.M. The pathobiology and repair of tendon and ligament injury. Vet. Clin. N. Am. Equine Pract 1994, 10, 323–349. [Google Scholar] [CrossRef]
- Patterson-Kane, J.C.; Wilson, A.M.; Firth, E.C.; Parry, D.A.; Goodship, A.E. Exercise-related alterations in crimp morphology in the central regions of superficial digital flexor tendons from young thoroughbreds: A controlled study. Equine Vet. J. 1998, 30, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Dowling, B.A.; Dart, A.J.; Hodgson, D.R.; Smith, R.K. Superficial digital flexor tendonitis in the horse. Equine Vet. J. 2000, 32, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Stephens, P.R.; Nunamaker, D.M.; Butterweck, D.M. Application of a Hall-effect transducer for measurement of tendon strains in horses. Am. J. Vet. Res. 1989, 50, 1089–1095. [Google Scholar] [PubMed]
- Riemersma, D.J.; van den Bogert, A.J.; Jansen, M.O.; Schamhardt, H.C. Tendon strain in the forelimbs as a function of gait and ground characteristics and in vitro limb loading in ponies. Equine Vet. J. 1996, 28, 133–138. [Google Scholar] [CrossRef]
- Pourcelot, P.; Defontaine, M.; Ravary, B.; Lemâtre, M.; Crevier-Denoix, N. A non-invasive method of tendon force measurement. J. Biomech. 2005, 38, 2124–2129. [Google Scholar] [CrossRef] [PubMed]
- Duenwald, S.; Kobayashi, H.; Frisch, K.; Lakes, R.; Vanderby, R., Jr. Ultrasound echo is related to stress and strain in tendon. J. Biomech. 2011, 44, 424–429. [Google Scholar] [CrossRef]
- Vergari, C.; Ravary-Plumioën, B.; Evrard, D.; Laugier, P.; Mitton, D.; Pourcelot, P.; Crevier-Denoix, N. Axial speed of sound is related to tendon’s nonlinear elasticity. J. Biomech. 2012, 45, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Ellison, M.E.; Duenwald-Kuehl, S.E.; Forrest, L.J.; Vanderby, R., Jr.; Brounts, S.H. Reproducibility and feasibility of acoustoelastography in the superficial digital flexor tendons of clinically normal horses. Am. J. Vet. Res. 2014, 75, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Meershoek, L.S.; Lanovaz, J.L. Sensitivity analysis and application to trotting of a noninvasive method to calculate flexor tendon forces in the equine forelimb. Am. J. Vet. Res. 2001, 62, 1594–1598. [Google Scholar] [CrossRef] [PubMed]
- Crevier-Denoix, N.; Ruel, Y.; Dardillat, C.; Jerbi, H.; Sanaa, M.; Collobert-Laugier, C.; Ribot, X.; Denoix, J.M.; Pourcelot, P. Correlations between mean echogenicity and material properties of normal and diseased equine superficial digital flexor tendons: An in vitro segmental approach. J. Biomech. 2005, 38, 2212–2220. [Google Scholar] [CrossRef]
- Brainerd, E.L.; Baier, D.B.; Gatesy, S.M.; Hedrick, T.L.; Metzger, K.A.; Gilbert, S.L.; Crisco, J.J. X-ray reconstruction of moving morphology (XROMM): Precision, accuracy and applications in comparative biomechanics research. J. Exp. Zool. A Ecol. Genet. Physiol. 2010, 313, 262–279. [Google Scholar] [CrossRef]
- Friden, T.; Ryd, L.; Lindstrand, A. Laxity and graft fixation after reconstruction of the anterior cruciate ligament. A roentgen stereophotogrammetric analysis of 11 patients. Acta Orthop. Scand. 1992, 63, 80–84. [Google Scholar] [CrossRef]
- Schepull, T.; Kvist, J.; Andersson, C.; Aspenberg, P. Mechanical properties during healing of Achilles tendon ruptures to predict final outcome: A pilot Roentgen stereophotogrammetric analysis in 10 patients. BMC Musculoskelet. Disord. 2007, 8, 116. [Google Scholar] [CrossRef]
- Cashman, P.M.M.; Baring, T.; Reilly, P.; Emery, R.J.H.; Amis, A.A. Measurement of migration of soft tissue by modified Roentgen stereophotogrammetric analysis (RSA): Validation of a new technique to monitor rotator cuff tears. J. Med. Eng. Technol. 2010, 34, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.E.; Keller, R.A.; Okoroha, K.; Guest, J.M.; Yu, C.; Muh, S.; Moutzouros, V. Radiostereometric Evaluation of Tendon Elongation After Distal Biceps Repair. Orthop. J. Sports Med. 2016, 4, 2325967116672620. [Google Scholar] [CrossRef] [PubMed]
- Wagner, F.C.; Reese, S.; Gerlach, K.; Böttcher, P.; Mülling, C.K.W. Cyclic tensile tests of Shetland pony superficial digital flexor tendon with an optimized cryo-clamp combined with biplanar high-speed fluoroscopy. BMC Vet. Res. 2021. accepted. [Google Scholar]
- Bussières, G.; Jacques, C.; Lainay, O.; Beauchamp, G.; Leblond, A.; Cadore, J.L.; Desmaizieres, L.M.; Cuvelliez, S.G.; Troncy, E. Development of a composite orthopaedic pain scale in horses. Res. Vet. Sci. 2008, 85, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.K.W.; McIlwraith, C.W. Consensus on equine tendon disease: Building on the 2007 Havemeyer symposium. Equine Vet. J. 2012, 44, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Dalla Costa, E.; Minero, M.; Lebelt, D.; Stucke, D.; Canali, E.; Leach, M.C. Development of the horse grimace scale (HGS) as a pain assessment tool in horses undergoing routine castration. PLoS ONE 2014, 9, e92281. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.; Reich, E.; Grund, S.; Mülling, C.K.W.; Geiger, S.M. Validation of 2 noninvasive, markerless reconstruction techniques in biplane high-speed fluoroscopy for 3-dimensional research of bovine distal limb kinematics. J. Dairy Sci. 2017, 100, 8372–8384. [Google Scholar] [CrossRef] [PubMed]
- Geiger, S.M.; Reich, E.; Böttcher, P.; Grund, S.; Hagen, J. Validation of biplane high-speed fluoroscopy combined with two different noninvasive tracking methodologies for measuring in vivo distal limb kinematics of the horse. Equine Vet. J. 2018, 50, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Knoerlein, B.J.; Baier, D.B.; Gatesy, S.M.; Laurence-Chasen, J.D.; Brainerd, E.L. Validation of XMALab software for marker-based XROMM. J. Exp. Biol. 2016, 219, 3701–3711. [Google Scholar] [CrossRef]
- De Grauw, J.C.; van Loon, J.P.A.M. Systematic pain assessment in horses. Vet. J. 2016, 209, 14–22. [Google Scholar] [CrossRef]
- Van Loon, J.P.A.M.; van Dierendonck, M.C. Pain assessment in horses after orthopaedic surgery and with orthopaedic trauma. Vet. J. 2019, 246, 85–91. [Google Scholar] [CrossRef]
- Khan, K.M.; Cook, J.L.; Bonar, F.; Harcourt, P.; Astrom, M. Histopathology of common tendinopathies. Update and implications for clinical management. Sports Med. 1999, 27, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Sugg, K.B.; Lubardic, J.; Gumucio, J.P.; Mendias, C.L. Changes in macrophage phenotype and induction of epithelial-to-mesenchymal transition genes following acute Achilles tenotomy and repair. J. Orthop. Res. 2014, 32, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Killian, M.L.; Cavinatto, L.; Galatz, L.M.; Thomopoulos, S. The role of mechanobiology in tendon healing. J. Shoulder Elbow Surg. 2012, 21, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Alberius, P. Bone reactions to tantalum markers. A scanning electron microscopic study. Acta Anat. 1983, 115, 310–318. [Google Scholar] [CrossRef]
- Aronson, A.S.; Jonsson, N.; Alberius, P. Tantalum markers in radiography. An assessment of tissue reactions. Skeletal Radiol. 1985, 14, 207–211. [Google Scholar] [CrossRef]
- Roos, P.J.; Hull, M.L.; Howell, S.M. How cyclic loading affects the migration of radio-opaque markers attached to tendon grafts using a new method: A study using roentgen stereophotogrammetric analysis (RSA). J. Biomech. Eng. 2004, 126, 62–69. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Goldin, B.; Block, W.D.; Pearson, J.R. Wound healing of tendon–I. Physical, mechanical and metabolic changes. J. Biomech. 1980, 13, 241–256. [Google Scholar] [CrossRef]
- Silver, I.A.; Brown, P.N.; Goodship, A.E.; Lanyon, L.E.; McCullagh, K.G.; Perry, G.C.; Williams, I.F. A clinical and experimental study of tendon injury, healing and treatment in the horse. Equine Vet. J. Suppl. 1983, 1, 1–43. [Google Scholar]
- Enwemeka, C.S. Inflammation, cellularity, and fibrillogenesis in regenerating tendon: Implications for tendon rehabilitation. Phys. Ther. 1989, 69, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Denoix, J.M. Functional anatomy of tendons and ligaments in the distal limbs (manus and pes). Vet. Clin. N. Am. Equine Pract. 1994, 10, 273–322. [Google Scholar] [CrossRef]
- Watkins, J.P.; Auer, J.A.; Gay, S.; Morgan, S.J. Healing of surgically created defects in the equine superficial digital flexor tendon: Collagen-type transformation and tissue morphologic reorganization. Am. J. Vet. Res. 1985, 46, 2091–2096. [Google Scholar]
- Van den Boom, R.; Wilmink, J.M.; O’Kane, S.; Wood, J.; Ferguson, M.W.J. Transforming growth factor-beta levels during second- intention healing are related to the different course of wound contraction in horses and ponies. Wound Repair Regen. 2002, 10, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Wilmink, J.M.; van Herten, J.; van Weeren, P.R.; Barneveld, A. Retrospective study of primary intention healing and sequestrum formation in horses compared to ponies under clinical circumstances. Equine Vet. J. 2002, 34, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Pickersgill, C.H.; Marr, C.M.; Reid, S.W. Repeatability of diagnostic ultrasonography in the assessment of the equine superficial digital flexor tendon. Equine Vet. J. 2001, 33, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Karlin, W.M.; Stewart, A.A.; Durgam, S.S.; Naughton, J.F.; O’Dell-Anderson, K.J.; Stewart, M.C. Evaluation of experimentally induced injury to the superficial digital flexor tendon in horses by use of low-field magnetic resonance imaging and ultrasonography. Am. J. Vet. Res. 2011, 72, 791–798. [Google Scholar] [CrossRef]
- Dakin, S.G.; Jespers, K.; Warner, S.; O’Hara, L.K.; Dudhia, J.; Goodship, A.E.; Wilson, A.M.; Smith, R.K.W. The relationship between in vivo limb and in vitro tendon mechanics after injury: A potential novel clinical tool for monitoring tendon repair. Equine Vet. J. 2011, 43, 418–423. [Google Scholar] [CrossRef]
- Crevier, N.; Pourcelot, P.; Denoix, J.-M.; Geiger, D.; Bortolussi, C.; Ribot, X.; Sanaa, M. Segmental variations of in vitro mechanical properties in equine superficial digital flexor tendons. Am. J. Vet. Res. 1996, 57, 1111–1117. [Google Scholar]
- Solomon, L.B.; Callary, S.A. Emerging ideas: Soft tissue applications of radiostereometric analysis. Clin. Orthop. Relat. Res. 2011, 469, 1512–1516. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.K.; Hull, M.L.; Howell, S.M. Migration of radio-opaque markers injected into tendon grafts: A study using roentgen stereophotogrammetric analysis (RSA). J. Biomech. Eng. 2005, 127, 887–890. [Google Scholar] [CrossRef][Green Version]
- Rohwedder, T.; Fischer, M.S.; Böttcher, P. In vivo fluoroscopic kinematography of dynamic radio-ulnar incongruence in dogs. Open Vet. J. 2017, 7, 221–228. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rohwedder, T.; Fischer, M.S.; Böttcher, P. In vivo axial humero-ulnar rotation in normal and dysplastic canine elbow joints. Tierarztl. Prax. Ausg. K Kleintiere. Heimtiere. 2018, 46, 83–89. [Google Scholar] [CrossRef]
- Flanigan, P.; Kshettry, V.R.; Benzel, E.C. World War II, tantalum, and the evolution of modern cranioplasty technique. Neurosurg. Focus 2014, 36, E22. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.M.; Whitton, R.C.; Kawcak, C.E.; Stover, S.M.; Pandy, M.G. Relationship between muscle forces, joint loading and utilization of elastic strain energy in equine locomotion. J. Exp. Biol 2010, 213, 3998–4009. [Google Scholar] [CrossRef] [PubMed]
- Williams, I.F.; McCullagh, K.G.; Goodship, A.E.; Silver, I.A. Studies on the pathogenesis of equine tendonitis following collagenase injury. Res. Vet. Sci. 1984, 36, 326–338. [Google Scholar] [CrossRef]
- Wilmink, J.; Wilson, A.M.; Goodship, A.E. Functional significance of the morphology and micromechanics of collagen fibres in relation to partial rupture of the superficial digital flexor tendon in racehorses. Res. Vet. Sci. 1992, 53, 354–359. [Google Scholar] [CrossRef]
- Nabeshima, Y.; Grood, E.S.; Sakurai, A.; Herman, J.H. Uniaxial tension inhibits tendon collagen degradation by collagenase in vitro. J. Orthop. Res. 1996, 14, 123–130. [Google Scholar] [CrossRef]
- Oloumi, M.M.; Vosough, D.; Derakhshanfar, A.; Nematollahi, M.H. The healing potential of plantago lanceolata ointment on collagenase-induced tendinitis in burros (Equus asinus). J. Equine Vet. Sci. 2011, 31, 470–474. [Google Scholar] [CrossRef]
- Clayton, H.M.; Schamhardt, H.C.; Willemen, M.A.; Lanovaz, J.L.; Colborne, G.R. Kinematics and ground reaction forces in horses with superficial digital flexor tendinitis. Am. J. Vet. Res. 2000, 61, 191–196. [Google Scholar] [CrossRef]
- Clayton, H.M.; Schamhardt, H.C.; Willemen, M.A.; Lanovaz, J.L.; Colborne, G.R. Net joint moments and joint powers in horses with superficial digital flexor tendinitis. Am. J. Vet. Res. 2000, 61, 197–201. [Google Scholar] [CrossRef]
- Clayton, H.M.; Willemen, M.A.; Lanovaz, J.L.; Schamhardt, H.C. Effects of a Heel Wedge in Horses with Superficial Digital Flexor Tendinitis. Vet. Comp. Orthop. Traumatol. 2000, 13, 1–8. [Google Scholar] [CrossRef]
- Meershoek, L.S.; Lanovaz, J.L.; Schamhardt, H.C.; Clayton, H.M. Calculated forelimb flexor tendon forces in horses with experimentally induced superficial digital flexor tendinitis and the effects of application of heel wedges. Am. J. Vet. Res. 2002, 63, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Lustgarten, M.; Redding, W.R.; Labens, R.; Davis, W.; Daniel, T.M.; Griffith, E.; Seiler, G.S. Elastographic evaluation of naturally occuring tendon and ligament injuries of the equine distal limb. Vet. Radiol. Ultrasound 2015, 56, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Bukowiecki, C.F.; Bramlage, L.R.; Gabel, A.A. In vitro strength of the suspensory apparatus in training and resting horses. Vet. Surg. 1987, 16, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.C. Mechanobiology of tendon. J. Biomech. 2006, 39, 1563–1582. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.K.W.; Goodship, A.E. The effect of early training and the adaptation and conditioning of skeletal tissues. Vet. Clin. N. Am. Equine Pract 2008, 24, 37–51. [Google Scholar] [CrossRef]
- Narici, M.V.; Maganaris, C.N. Adaptability of elderly human muscles and tendons to increased loading. J. Anat. 2006, 208, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Fouré, A.; Nordez, A.; Cornu, C. Plyometric training effects on Achilles tendon stiffness and dissipative properties. J. Appl. Physiol. 2010, 109, 849–854. [Google Scholar] [CrossRef]
- Kubo, K.; Ikebukuro, T.; Maki, A.; Yata, H.; Tsunoda, N. Time course of changes in the human Achilles tendon properties and metabolism during training and detraining in vivo. Eur. J. Appl. Physiol. 2012, 112, 2679–2691. [Google Scholar] [CrossRef] [PubMed]
- Lochner, F.K.; Milne, D.W.; Mills, E.J.; Groom, J.J. In vivo and in vitro measurement of tendon strain in the horse. Am. J. Vet. Res. 1980, 41, 1929–1937. [Google Scholar] [PubMed]
- Johnson, G.A.; Livesay, G.A.; Woo, S.L.; Rajagopal, K.R. A single integral finite strain viscoelastic model of ligaments and tendons. J. Biomech. Eng. 1996, 118, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Williams, I.F.; Heaton, A.; McCullagh, K.G. Cell morphology and collagen types in equine tendon scar. Res. Vet. Sci 1980, 28, 302–310. [Google Scholar] [CrossRef]
- Parry, D.A.; Barnes, G.R.; Craig, A.S. A comparison of the size distribution of collagen fibrils in connective tissues as a function of age and a possible relation between fibril size distribution and mechanical properties. Proc. R Soc. Lond. B Biol. Sci. 1978, 203, 305–321. [Google Scholar] [CrossRef]
- Diamant, J.; Keller, A.; Baer, E.; Litt, M.; Arridge, R.G. Collagen; ultrastructure and its relation to mechanical properties as a function of ageing. Proc. R Soc. Lond. B Biol. Sci. 1972, 180, 293–315. [Google Scholar] [CrossRef] [PubMed]
- Stashak, T.S.; Theoret, C. Equine Wound Management; Veterinary Wound Management Society/V.W.M.S.: Ames, IA, USA, 2008; ISBN 978-0813812236. [Google Scholar]
- Crevier-Denoix, N.; Collobert, C.; Pourcelot, P.; Denoix, J.M.; Sanaa, M.; Geiger, D.; Bernard, N.; Ribot, X.; Bortolussi, C.; Bousseau, B. Mechanical properties of pathological equine superficial digital flexor tendons. Equine Vet. J. Suppl. 1997, 23–26. [Google Scholar] [CrossRef]
- Buchner, H.H.; Savelberg, H.H.; Schamhardt, H.C.; Merkens, H.W.; Barneveld, A. Kinematics of treadmill versus overground locomotion in horses. Vet. Q. 1994, 16 (Suppl. S2), S87–S90. [Google Scholar] [CrossRef]
- Back, W.; Schamhardt, H.C.; van Weeren, P.R.; Barneveld, A. A comparison between the trot of pony and horse foals to characterize equine locomotion at young age. Equine Vet. J. Suppl. 1999, 31, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Crevier-Denoix, N.; Ravary-Plumiöen, B.; Vergari, C.; Camus, M.; Holden-Douilly, L.; Falala, S.; Jerbi, H.; Desquilbet, L.; Chateau, H.; Denoix, J.M.; et al. Comparison of superficial digital flexor tendon loading on asphalt and sand in horses at the walk and trot. Vet. J. 2013, 198 (Suppl. S1), e130–e136. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animal | Specimen | Strain | |||
|---|---|---|---|---|---|
| During Walk | During Trot | Rupture | |||
| Riemersma et al. 1985 | ponies | whole SDFT | 1.74% | ||
| Riemersma et al. 1988 | ponies | whole SDFT | 2.3% | ||
| Stephens et al. 1989 | horses | whole SDFT | 3.3% | ||
| Jansen et al. 1993 | ponies | whole SDFT | 3.5% | ||
| Crevier et al. 1996 | horses | metacarpal segments | proximal 4.78%, mid 5.05%, distal 4.43% | ||
| Riemersma et al. 1996 | ponies | whole SDFT | 2.19% | 4.15% | |
| Butcher et al. 2007 | horses | whole SDFT | 3.6% | 5.6% | |
| Lawson et al. 2007 | horses | whole SDFT | 6.71% | 8.46% | |
| This study | pony | metacarpal region of the SDFT | 2.86% mid: 3.13% | 6.78% mid: 6.06% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, F.C.; Gerlach, K.; Geiger, S.M.; Gittel, C.; Böttcher, P.; Mülling, C.K.W. Biplanar High-Speed Fluoroscopy of Pony Superficial Digital Flexor Tendon (SDFT)—An In Vivo Pilot Study. Vet. Sci. 2021, 8, 92. https://doi.org/10.3390/vetsci8060092
Wagner FC, Gerlach K, Geiger SM, Gittel C, Böttcher P, Mülling CKW. Biplanar High-Speed Fluoroscopy of Pony Superficial Digital Flexor Tendon (SDFT)—An In Vivo Pilot Study. Veterinary Sciences. 2021; 8(6):92. https://doi.org/10.3390/vetsci8060092
Chicago/Turabian StyleWagner, Franziska C., Kerstin Gerlach, Sandra M. Geiger, Claudia Gittel, Peter Böttcher, and Christoph K. W. Mülling. 2021. "Biplanar High-Speed Fluoroscopy of Pony Superficial Digital Flexor Tendon (SDFT)—An In Vivo Pilot Study" Veterinary Sciences 8, no. 6: 92. https://doi.org/10.3390/vetsci8060092
APA StyleWagner, F. C., Gerlach, K., Geiger, S. M., Gittel, C., Böttcher, P., & Mülling, C. K. W. (2021). Biplanar High-Speed Fluoroscopy of Pony Superficial Digital Flexor Tendon (SDFT)—An In Vivo Pilot Study. Veterinary Sciences, 8(6), 92. https://doi.org/10.3390/vetsci8060092