Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Standard Echocardiography
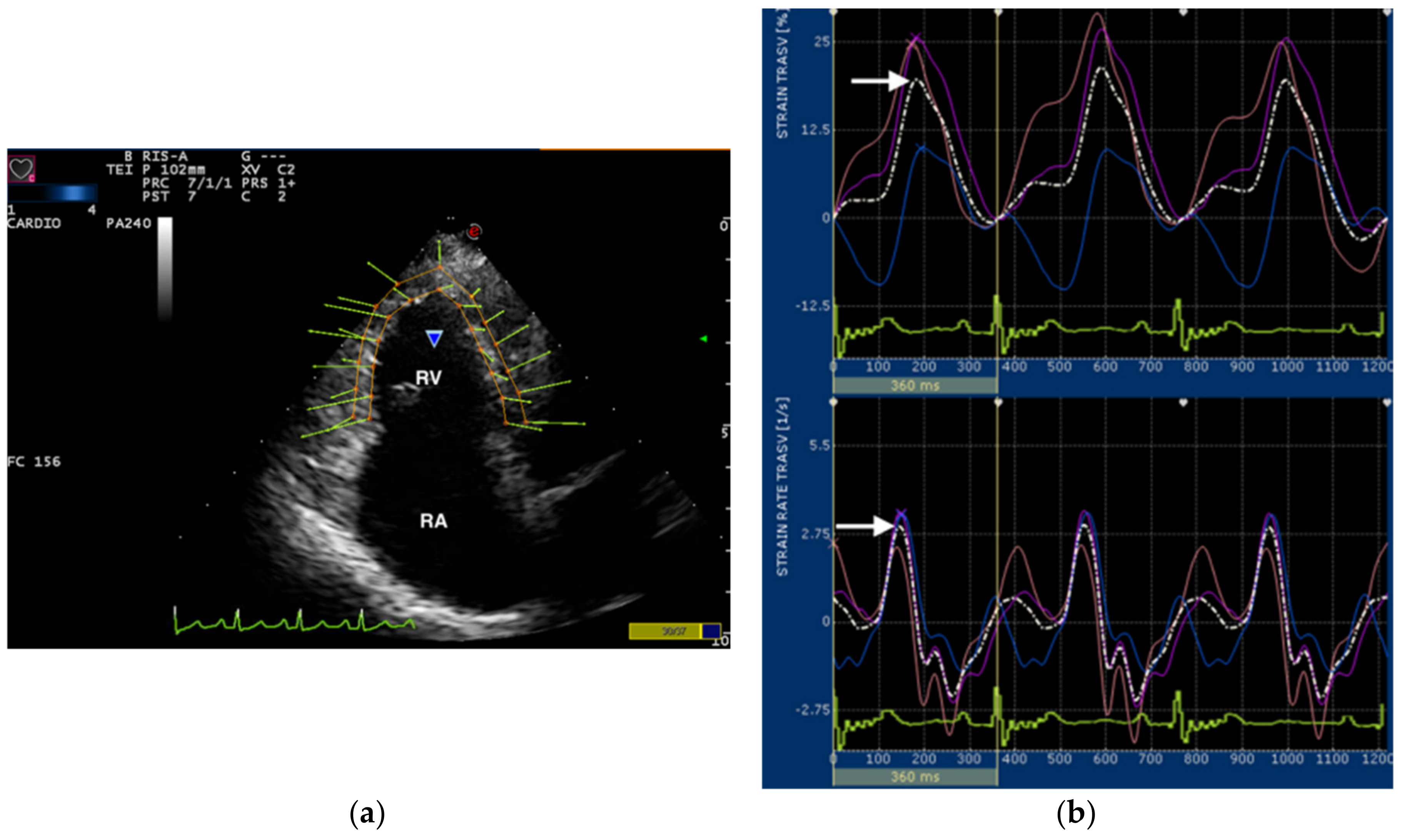
2.2. Speckle Tracking Echocardiography
2.3. Statistical Analysis
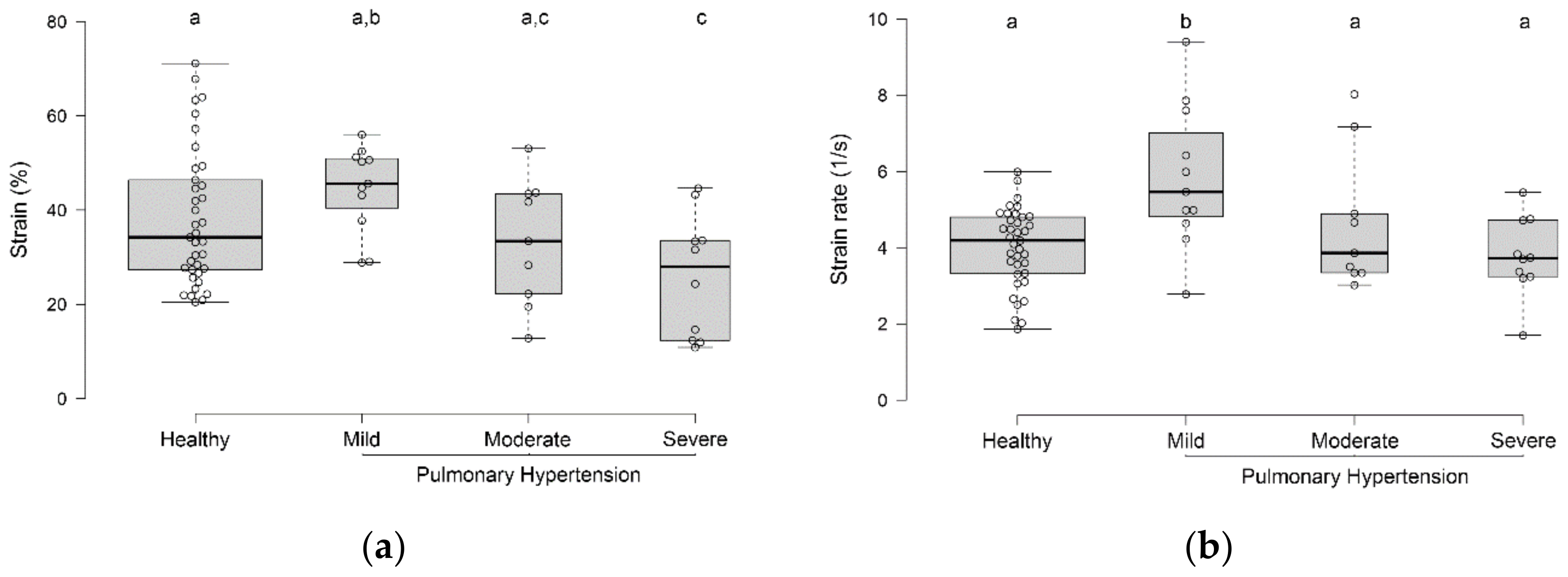
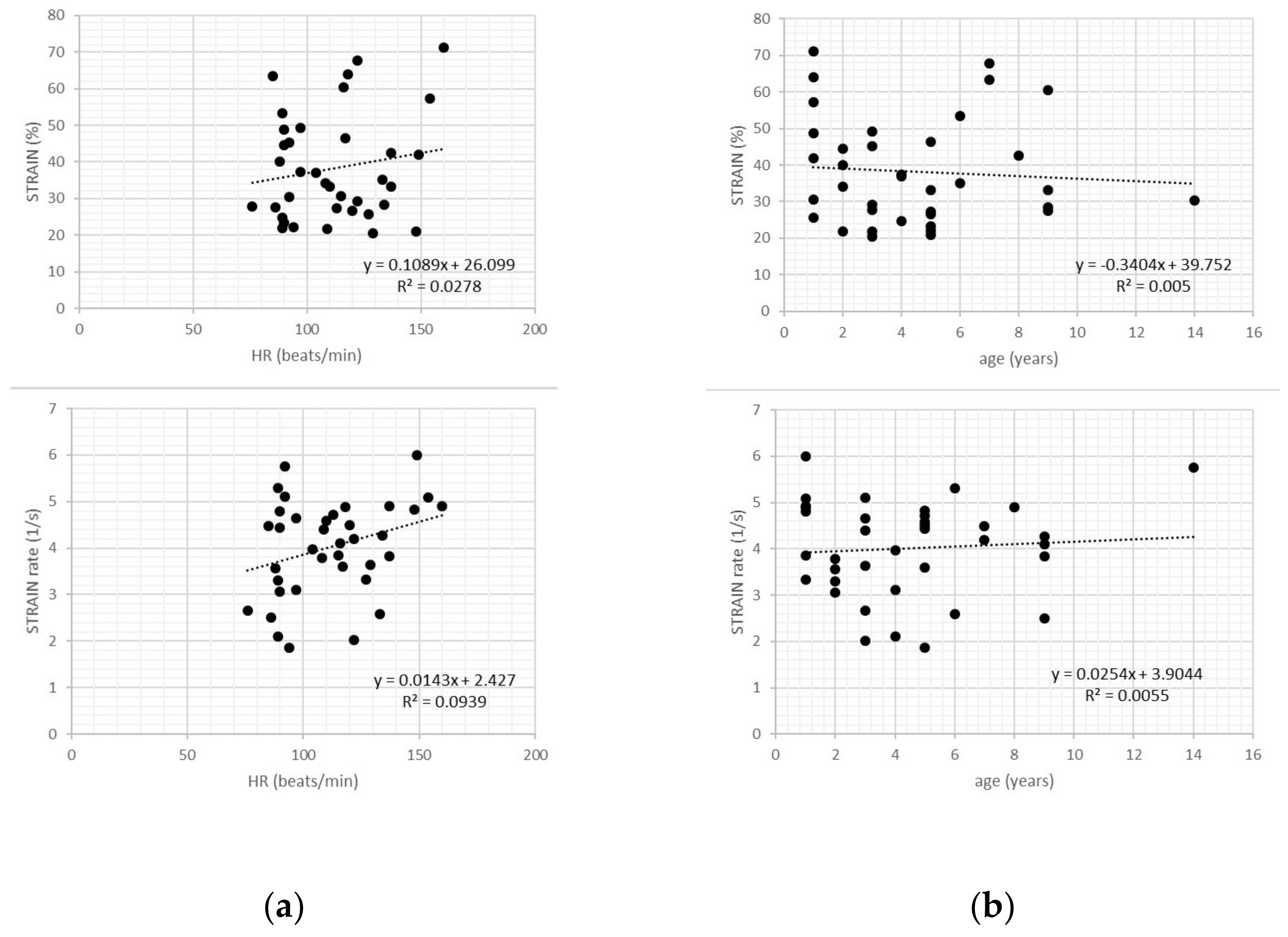
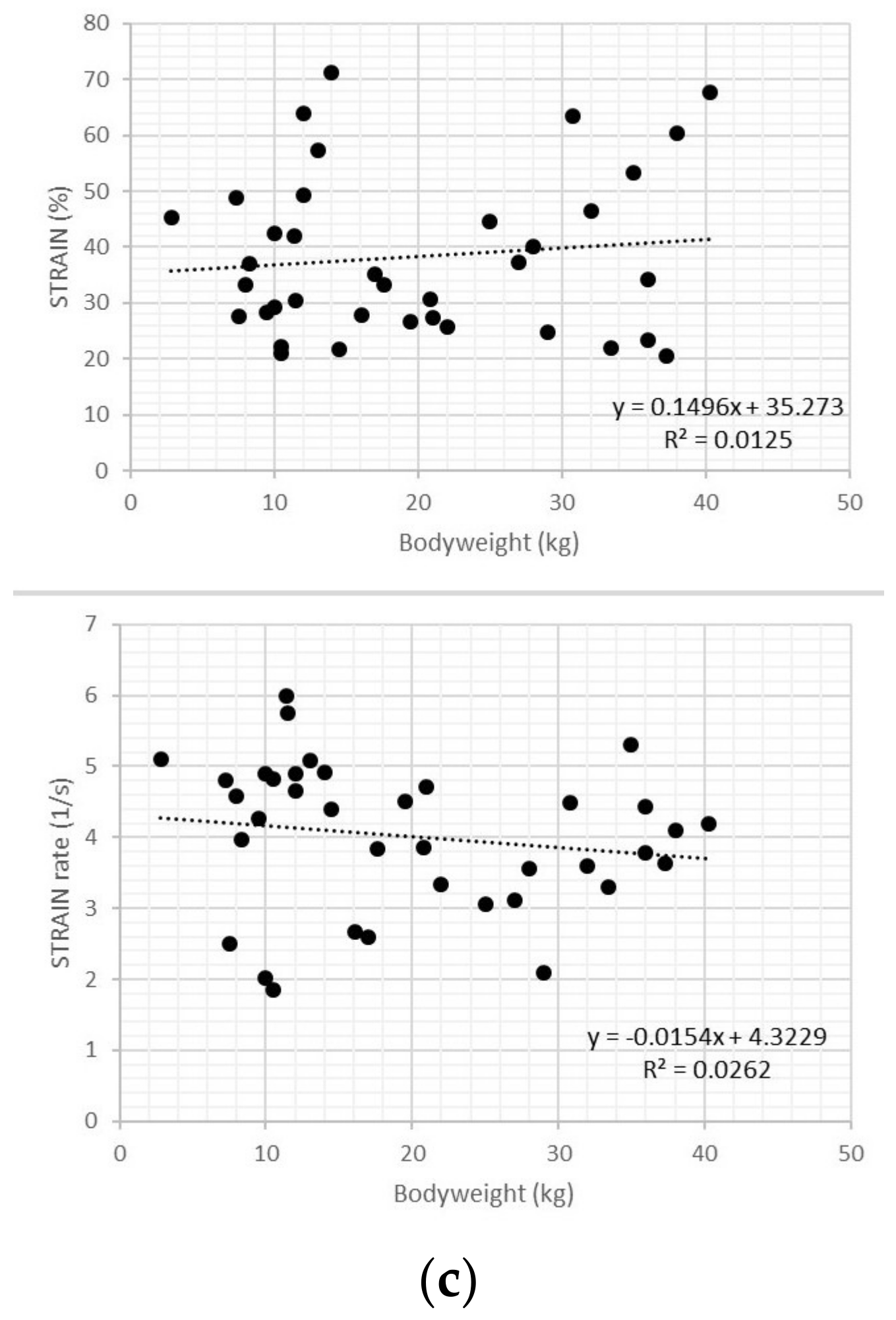
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Visser, L.C.; Scansen, B.A.; Schober, K.E.; Bonagura, J.D. Echocardiographic assessment of right ventricular systolic function in conscious healthy dogs: Repeatability and referenc intervals. J. Vet. Cardiol. 2015, 17, 83–96. [Google Scholar] [CrossRef]
- Gentile-Solomon, J.M.; Abbott, J.A. Conventional echocardiographic assessment of the canine right heart: Reference intervals and repeatability. J. Vet. Cardiol. 2016, 18, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Nakamura, K.; Osuga, T.; Lim, S.Y.; Yokoyama, N.; Morishita, K.; Ohta, H.; Takiguchi, M. Repeatability and reproducibility of right ventricular Tei index valves derived from three echocardiographic methods for evaluation of cardiac function in dogs. Am. J. Vet. Res. 2016, 77, 715–720. [Google Scholar] [CrossRef]
- Baron Toaldo, M.; Poser, H.; Menciotti, G.; Battaia, S.; Contiero, B.; Cipone, M.; Diana, A.; Mazzotta, E.; Guglielmini, C. Utility of tissue Doppler imaging in the echocardiographic evaluation of left and right ventricular function in dogs with myxomatous mitral valve disease with or without pulmonary hypertension. J. Vet. Intern. Med. 2016, 30, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Morita, T.; Osuga, T.; Morishita, K.; Sasaki, N.; Ohta, H.; Takiguchi, M. Prognostic value of right ventricular Tei Index in dogs with myxomatous mitral valvular heart disease. J. Vet. Intern. Med. 2016, 30, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Poser, H.; Berlanda, M.; Monacolli, M.; Contiero, B.; Coltro, A.; Guglielmini, C. Tricuspid annular plane systolic excursion in dogs with myxomatous mitral valve disease with and without pulmonary hypertension. J. Vet. Cardiol. 2017, 19, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Nakamura, K.; Osuga, T.; Yokoyama, N.; Khoirun, N.; Morishita, K.; Sasaki, N.; Ohta, H.; Takiguchi, M. The repeatability and characteristics of right ventricular longitudinal strain imaging by speckle-tracking echocardiography in healthy dogs. J. Vet. Cardiol. 2017, 19, 351–362. [Google Scholar] [CrossRef]
- Chapel, E.H.; Scansen, B.A.; Schober, K.E.; Bonagura, J.D. Echocardiographic estimates of right ventricular systolic function in dogs with myxomatous mitral valve disease. J. Vet. Intern. Med. 2018, 32, 64–71. [Google Scholar] [CrossRef]
- Caivano, D.; Dickson, D.; Pariaut, R.; Stillman, M.; Rishniw, M. Tricuspid annular plane systolic excursion-to-aortic ratio provides a bodyweight-independent measure of right ventricular systolic function in dogs. J. Vet. Cardiol. 2018, 20, 79–91. [Google Scholar] [CrossRef]
- Vezzosi, T.; Domenech, O.; Costa, G.; Marchesotti, F.; Venco, L.; Zini, E.; Del Palacio, M.J.F.; Tognetti, R. Echocardiographic evaluation of the right ventricular dimension and systolic function in dogs with pulmonary hypertension. J. Vet. Intern. Med. 2018, 32, 1541–1548. [Google Scholar] [CrossRef]
- Caivano, D.; Rishniw, M.; Birettoni, F.; Patata, V.; Giorgi, M.E.; Dei, K.; Porciello, F. Right ventricular outflow tract fractional shortening: An echocardiographic index of right ventricular systolic function in dogs with pulmonary hypertension. J. Vet. Cardiol. 2018, 20, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of theright heart in adults: A report from the American society of echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European association of cardiovascular imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Mondillo, S.; Galderisi, M.; Mele, D.; Cameli, M.; Lomoriello, V.S.; Zaca‘, V.; Ballo, P.; D’Andrea, A.; Muraru, D.; Losi, M.; et al. Speckle tracking echocardiography: A new technique for assessing myocardial function. J. Ultrasound Med. 2011, 30, 71–83. [Google Scholar] [CrossRef]
- Moceri, P.; Bouvier, P.; Baudouy, D.; Dimopoulos, K.; Cerboni, P.; Wort, S.J.; Doyen, D.; Schouver, E.D.; Gibelin, P.; Senior, R.; et al. Cardiac remodelling amongst adults with various aetiologies of pulmonary arterial hypertension including Eisenmenger syndrome-implications on survival and the role of right ventricular transverse strain. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1262–1270. [Google Scholar] [CrossRef]
- Di Salvo, G.; Pacileo, G.; Rea, A.; Limongelli, G.; Baldini, L.; D’Andrea, A.; D’Alto, M.; Sarubbi, B.; Russo, M.G.; Calabrò, R. Transverse strain predicts exercise capacity in systemic right ventricle patients. Int. J. Cardiol. 2010, 145, 193–196. [Google Scholar] [CrossRef]
- Caivano, D.; Rishniw, M.; Birettoni, F.; Petrescu, V.F.; Porciello, F. Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension. In Proceedings of the 30th ECVIM-CA Congress, Milan, Italy, 19–21 September 2019. [Google Scholar]
- Johnson, L.; Boon, J.; Orton, E.C. Clinical characteristics of 53 dogs with Doppler-derived evidence of pulmonary hypertension: 1992–1996. J. Vet. Intern. Med. 1999, 13, 440–447. [Google Scholar]
- Thomas, W.P.; Gaber, C.E.; Jacobs, G.J.; Kaplan, P.M.; Lombard, C.W.; Moise, N.S.; Moses, B.L. Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. Echocardiography Committee of the Specialty of Cardiology, American College of Veterinary Internal Medicine. J. Vet. Intern. Med. 1993, 7, 247–252. [Google Scholar] [CrossRef]
- Abbott, J.A.; MacLean, H.N. Comparison of Doppler-derived peak aortic velocities obtained from subcostal and apical transducer sites in healthy dogs. Vet. Radiol. Ultrasound 2003, 44, 695–698. [Google Scholar] [CrossRef]
- Cornell, C.C.; Kittleson, M.D.; Della Torre, P.; Haggstrom, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric scaling of M-mode cardiac measurements in normal adult dogs. J. Vet. Intern. Med. 2004, 18, 311–321. [Google Scholar] [CrossRef]
- Dickson, D.; Caivano, D.; Patteson, M.; Rishniw, M. The times they are a-changin’: Two-dimensional aortic valve measurements differ throughout diastole. J. Vet. Cardiol. 2016, 18, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Rishniw, M.; Caivano, D.; Dickson, D.; Vatne, L.; Harris, J.; Matos, J.N. Two-dimensional echocardiographic left- atrial-to-aortic ratio in healthy adult dogs: A reexamination of reference intervals. J. Vet. Cardiol. 2019, 26, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Caivano, D.; Rishniw, M.; Patata, V.; Giorgi, M.E.; Birettoni, F.; Porciello, F. Left atrial deformation and phasic function determined by 2-dimensional speckle tracking echocardiography in healthy dogs. J. Vet. Cardiol. 2016, 18, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Caivano, D.; Rishniw, M.; Birettoni, F.; Patata, V.; Giorgi, M.E.; Porciello, F. Left atrial deformation and phasic function determined by two-dimensional speckle-tracking echocardiography in dogs with myxomatous mitral valve disease. J. Vet. Cardiol. 2018, 20, 102–114. [Google Scholar] [CrossRef]
- Visser, L.C. Right Ventricular Function: Imaging Techniques. Vet. Clin. N. Am. Small Anim. Pract. 2017, 47, 989–1003. [Google Scholar] [CrossRef]
- Sanchez-Quintana, D.; Anderson, R.H.; Ho, S.Y. Ventricular myoarchitecture in tetralogy of Fallot. Heart 1996, 76, 280–286. [Google Scholar] [CrossRef]
- Pettersen, E.; Helle-Valle, T.; Edvardsen, T.; Lindberg, H.; Smith, H.J.; Smevik, B.; Smiseth, O.A.; Andersen, K. Contraction pattern of the systemic right ventricle shift from longitudinal to circumferential shortening and absent global ventricular torsion. J. Am. Coll. Cardiol. 2007, 49, 2450–2456. [Google Scholar] [CrossRef]
- Kind, T.; Mauritz, G.J.; Marcus, J.T.; van de Veerdonk, M.; Westerhof, N.; Vonk-Noordegraaf, A. Right ventricular ejection fraction is better reflected by transverse rather than longitudinal wall motion in pulmonary hypertension. J. Cardiovasc. Magn. Reson. 2010, 12, 35. [Google Scholar] [CrossRef]
- Kind, T.; Marcus, J.T.; Westerhof, N.; Vonk-Noordegraaf, A. Longitudinal and transverse movements of the right ventricle: Both are important in pulmonary arterial hypertension. Chest 2011, 140, 556–557. [Google Scholar] [CrossRef]
- Chetboul, V.; Serres, F.; Gouni, V.; Tissier, R.; Pouchelon, J.L. Radial strain and strain rate by two-dimensional speckle tracking echocardiography and the tissue velocity based technique in the dog. J. Vet. Cardiol. 2007, 9, 69–81. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Dogs | Dogs with PH | |
|---|---|---|
| Number of dogs (male) | 37 (20) | 30 (16) |
| Age (years) | 4 (1–14) | 12 (5–17) |
| Body weight (kg) | 17 (2.8–40.3) | 9.4 (2.2–31) |
| Heart rate (bpm) LA: Ao | 110 (76–160) 1.44 (1.1–1.68) | 137 (86–208) 2.0 (1.0–3.3) |
| TR velocity (m/Section) Transverse RV Strain (%) Transverse RV Strain rate (1/s) | – 34.2 (20.5–71.1) 4.2 (1.9–6.0) | 3.7 (3.1–6.2) 35.7 (10.9–56.0) 4.6 (1.7–9.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caivano, D.; Rishniw, M.; Birettoni, F.; Petrescu, V.-F.; Porciello, F. Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension. Vet. Sci. 2020, 7, 19. https://doi.org/10.3390/vetsci7010019
Caivano D, Rishniw M, Birettoni F, Petrescu V-F, Porciello F. Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension. Veterinary Sciences. 2020; 7(1):19. https://doi.org/10.3390/vetsci7010019
Chicago/Turabian StyleCaivano, Domenico, Mark Rishniw, Francesco Birettoni, Vasilica-Flory Petrescu, and Francesco Porciello. 2020. "Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension" Veterinary Sciences 7, no. 1: 19. https://doi.org/10.3390/vetsci7010019
APA StyleCaivano, D., Rishniw, M., Birettoni, F., Petrescu, V.-F., & Porciello, F. (2020). Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension. Veterinary Sciences, 7(1), 19. https://doi.org/10.3390/vetsci7010019