
Risk Assessment of Brucella Exposure Through Raw Milk Consumption in India: One Health Implications and Control Strategies


Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Model Parameters
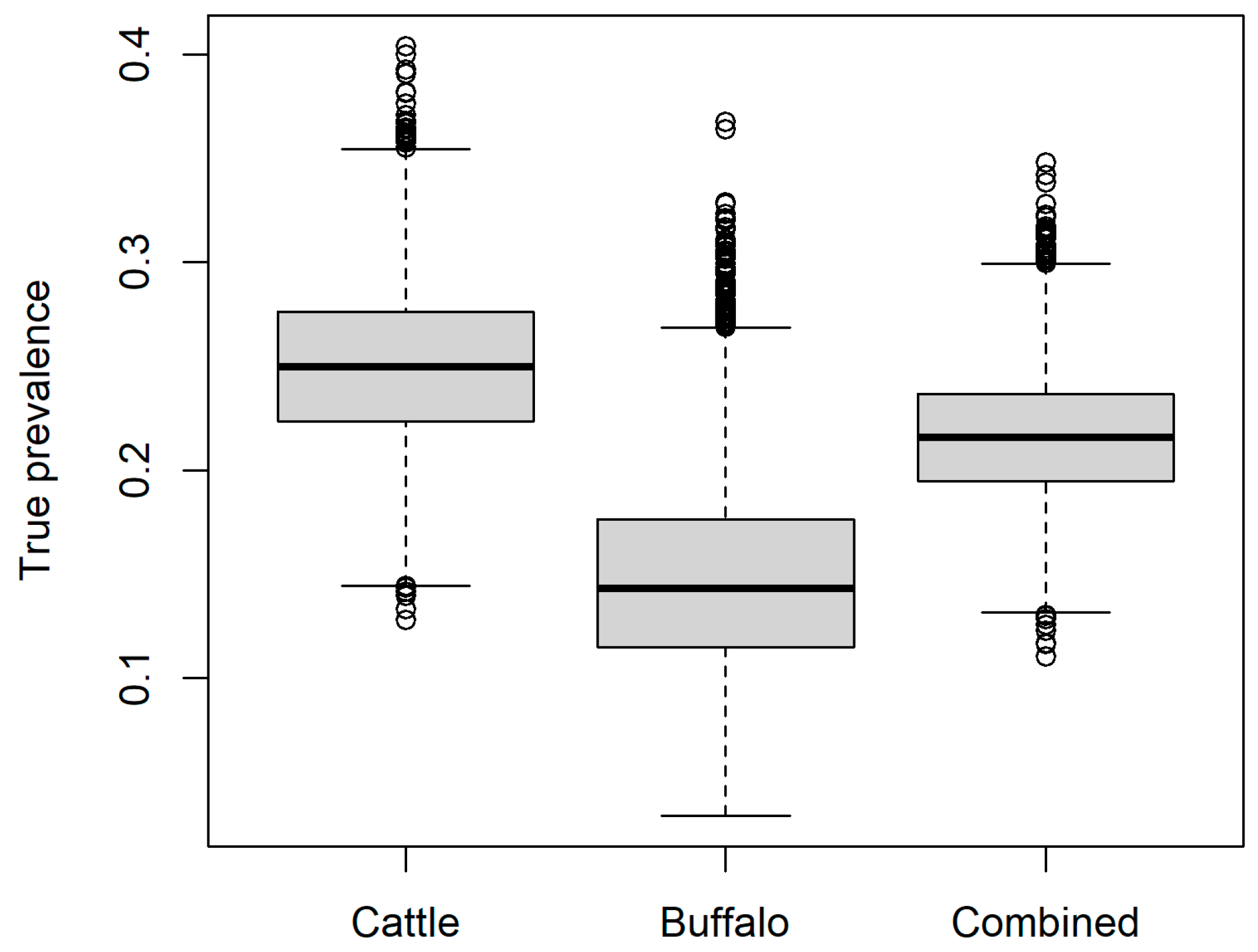
2.1.1. Brucella Seroprevalence in Lactating Cattle and Buffalo
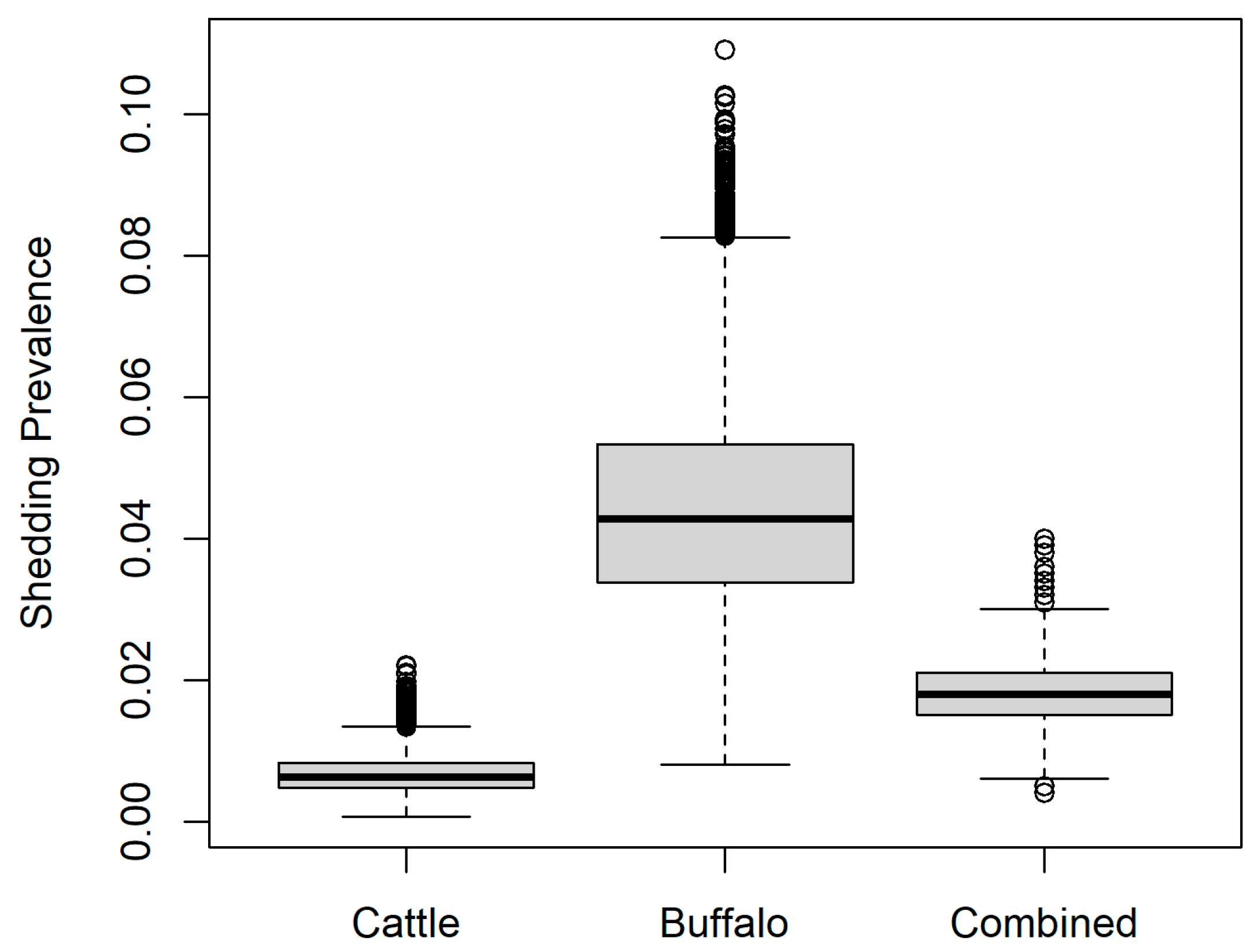
2.1.2. Probability of Brucella Abortus Shed in Milk of Seropositive Cattle and Buffalo
2.1.3. Number of B. abortus Colony Forming Units/mL Milk
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laine, C.G.; Johnson, V.E.; Scott, H.M.; Arenas-Gamboa, A.M. Global Estimate of Human Brucellosis Incidence. Emerg. Infect. Dis. 2023, 29, 1789–1797. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.P.; Mulder, M.; Gilman, R.H.; Smits, H.L. Human brucellosis. Lancet Infect. Dis. 2007, 7, 775–786. [Google Scholar] [CrossRef]
- Forbes, L.B.; Tessaro, S.V. Evaluation of cattle for experimental infection with and transmission of Brucella suis biovar 4. J. Am. Vet. Med. Assoc. 2003, 222, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Deka, R.P.; Magnusson, U.; Grace, D.; Lindahl, J.F. Bovine brucellosis: Prevalence, risk factors, economic cost and control options with particular reference to India- a review. Infect. Ecol. Epidemiol. 2018, 8, 1556548. [Google Scholar] [CrossRef]
- Jaismon, P.A.; Sushmitha, A.P.; Verma, M.R.; Singh, Y.P.; Borthakur, U.; Kumar, S.; Sharun, K.; Dhama, K. Prevalence of bovine brucellosis in India: A meta-analysis. Vet. Q. 2023, 43, 1–9. [Google Scholar] [CrossRef]
- Khurana, S.K.; Sehrawat, A.; Tiwari, R.; Prasad, M.; Gulati, B.; Shabbir, M.Z.; Chhabra, R.; Karthik, K.; Patel, S.K.; Pathak, M.; et al. Bovine brucellosis—A comprehensive review. Vet. Q. 2021, 41, 61–88. [Google Scholar] [CrossRef]
- Godfroid, J.; Nielsen, K.; Saegerman, C. Diagnosis of brucellosis in livestock and wildlife. Croat. Med. J. 2010, 51, 296–305. [Google Scholar] [CrossRef]
- Singh, B.; Dhand, N.K.; Gill, J. Economic losses occurring due to brucellosis in Indian livestock populations. Prev. Vet. Med. 2015, 119, 211–215. [Google Scholar] [CrossRef]
- Renukaradhya, G.; Isloor, S.; Rajasekhar, M. Epidemiology, zoonotic aspects, vaccination and control/eradication of brucellosis in India. Vet. Microbiol. 2002, 90, 183–195. [Google Scholar] [CrossRef]
- Seleem, M.N.; Boyle, S.M.; Sriranganathan, N. Brucellosis: A re-emerging zoonosis. Vet. Microbiol. 2010, 140, 392–398. [Google Scholar] [CrossRef]
- Singh, B.B.; Khatkar, M.S.; Aulakh, R.S.; Gill, J.P.S.; Dhand, N.K. Estimation of the health and economic burden of human brucellosis in India. Prev. Vet. Med. 2018, 154, 148–155. [Google Scholar] [CrossRef] [PubMed]
- BAHS. Basic Animal Husbandry Statistics 2024; Department of Animal Husbandry and Dairying, Ministry of Fisheries, Animal Husbandry and Dairying: New Delhi, India, 2024; pp. 1–272. [Google Scholar]
- Food Safety and Standards Authority of India Expert Group on Milk and Milk Products. Base Working Paper on Strategy and Action Plan for Ensuring Safety of Milk and Milk Products; NDDB: Gujarat, India, 2009; pp. 1–46. [Google Scholar]
- Shi, J.-F.; Gong, Q.-L.; Zhao, B.; Ma, B.-Y.; Chen, Z.-Y.; Yang, Y.; Sun, Y.-H.; Wang, Q.; Leng, X.; Zong, Y.; et al. Seroprevalence of Brucellosis in Buffalo Worldwide and Associated Risk Factors: A Systematic Review and Meta-Analysis. Front. Vet. Sci. 2021, 8, 649252. [Google Scholar] [CrossRef]
- Makita, K.; Fèvre, E.M.; Waiswa, C.; Eisler, M.C.; Thrusfield, M.; Welburn, S.C. Herd prevalence of bovine brucellosis and analysis of risk factors in cattle in urban and peri-urban areas of the Kampala economic zone, Uganda. BMC Vet. Res. 2011, 7, 60. [Google Scholar] [CrossRef]
- Dos Santos Rocha, I.D.; Clementino, I.J.; Canuto de Sousa, D.L.; Alves, C.J.; de Sousa Américo Batista Santos, C.; de Azevedo, S.S. Distribution, seroprevalence and risk factors for bovine brucellosis in Brazil: Official data, systematic review and meta-analysis. Rev. Argent. Microbiol. 2024, 56, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.D.; Kelly, L.; England, T.; MacMillan, A.; Wooldridge, M. A quantitative risk assessment for the importation of brucellosis-infected breeding cattle into Great Britain from selected European countries. Prev. Vet. Med. 2004, 63, 51–61. [Google Scholar] [CrossRef]
- Mohammed, F.A.O.; Salman, A.M.A. Risk Assessment of Brucellosis in Dairy Cows in Bahri North Locality, Sudan. EAS J. Nutr. Food Sci. 2020, 2, 129–140. [Google Scholar]
- Makita, K.; Fèvre, E.M.; Waiswa, C.; Eisler, M.C.; Welburn, S.C. How Human Brucellosis Incidence in Urban Kampala Can Be Reduced Most Efficiently? A Stochastic Risk Assessment of Informally-Marketed Milk. PLoS ONE 2010, 5, e14188. [Google Scholar] [CrossRef] [PubMed]
- Corbel, M.J. Microbiology of the genus Brucella. In Brucellosis; CRC Press: Boca Raton, FL, USA, 2020; pp. 53–72. [Google Scholar]
- Rahman, A.K.M.A.; Smit, S.; Devleesschauwer, B.; Kostoulas, P.; Abatih, E.; Saegerman, C.; Shamsuddin, M.; Berkvens, D.; Dhand, N.K.; Ward, M.P. Bayesian evaluation of three serological tests for the diagnosis of bovine brucellosis in Bangladesh. Epidemiol. Infect. 2019, 147, e73. [Google Scholar] [CrossRef]
- Rogan, W.J.; Gladen, B. Estimating prevalence from the results of a screening test. Am. J. Epidemiol. 1978, 107, 71–76. [Google Scholar] [CrossRef]
- Capparelli, R.; Parlato, M.; Iannaccone, M.; Roperto, S.; Marabelli, R.; Roperto, F.; Iannelli, D. Heterogeneous shedding of Brucella abortus in milk and its effect on the control of animal brucellosis. J. Appl. Microbiol. 2009, 106, 2041–2047. [Google Scholar] [CrossRef]
- Abnaroodheleh, F.; Emadi, A.; Dashtipour, S.; Jamil, T.; Khaneghah, A.M.; Dadar, M. Shedding rate of Brucella spp. in the milk of seropositive and seronegative dairy cattle. Heliyon 2023, 9, e15085. [Google Scholar] [CrossRef]
- Kaden, R.; Ferrari, S.; Jinnerot, T.; Lindberg, M.; Wahab, T.; Lavander, M. Brucella abortus: Determination of survival times and evaluation of methods for detection in several matrices. BMC Infect. Dis. 2018, 18, 259. [Google Scholar] [CrossRef]
- Panchasara, H.; Patel, J.; Patel, P. Economic implications of brucellosis in bovine. Indian J. Vet. Sci. Biotechnol. 2012, 8, 19–21. [Google Scholar]
- Iooss, B.; Da Veiga, S.; Janon, A.; Pujol, G. Sensitivity: Global Sensitivity Analysis of Model Outputs and Importance Measures; R Package Version 1.30.1. 2024. Available online: https://CRAN.R-project.org/package=sensitivity (accessed on 28 April 2025).
- Ndaki, M. A quantitative risk assessment of humans exposure to brucellosis through the consumption of raw cow milk in Arusha, Tanzania. J. Agric. Biomed. Sci. 2022, 6, 1–20. [Google Scholar] [CrossRef]
- Kouamé-Sina, S.M.; Makita, K.; Costard, S.; Grace, D.; Dadié, A.; Dje, M.; Bonfoh, B. Hazard identification and exposure assessment for bacterial risk assessment of informally marketed milk in Abidjan, Côte d’Ivoire. Food Nutr. Bull. 2012, 33, 223–234. [Google Scholar] [CrossRef]
- Hundal, J.S.; Sodhi, S.S.; Gupta, A.; Singh, J.; Chahal, U.S. Awareness, knowledge, and risks of zoonotic diseases among livestock farmers in Punjab. Vet. World 2016, 9, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, R.; Swaminathan, S.; Webb, P.; Kurpad, A.V.; Thomas, T. Evidence on Milk Consumption and Production Linkages from Rural Bihar, India. Curr. Dev. Nutr. 2024, 8, 102122. [Google Scholar] [CrossRef]
- Dadar, M.; Fakhri, Y.; Shahali, Y.; Mousavi Khaneghah, A. Contamination of milk and dairy products by Brucella species: A global systematic review and meta-analysis. Food Res. Int. 2020, 128, 108775. [Google Scholar] [CrossRef]
- Spickler, A.R. Brucellosis: Brucella abortus; Center for Food Security and Public Health, USDA: Des Moines, IA, USA, 2018; Available online: http://www.cfsph.iastate.edu/DiseaseInfo/factsheets.php (accessed on 28 April 2025).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | RBPT Positive (%) | I-ELISA Positive (%) | Both RBPT and I-ELISA Positive (%) | Total Tested |
|---|---|---|---|---|
| Cattle | 35 (19.3) | 45 (24.9) | 33 (18.2) | 181 |
| Buffalo | 11 (13.8) | 13 (16.3) | 8 (10.0) | 80 |
| Total | 46 (17.6) | 58 (22.2) | 41 (15.7) | 261 |
| Parameter | Name | Value | Distribution | References |
|---|---|---|---|---|
| Apparent seroprevalence of Brucella abortus in lactating cattle and buffalo | Seroprevalenceapparent | mean 0.16 (95% range 0.12–0.21) | beta (42, 221) | Field data (current study) |
| Apparent seroprevalence of Brucella abortus in lactating cattle | Seroprevalenceapparent | mean 0.19 (95% range 0.13–0.25) | beta (34, 149) | Field data (current study) |
| Apparent seroprevalence of Brucella abortus in lactating buffalo | Seroprevalenceapparent | mean 0.11 (95% range 0.05–0.19) | beta (9, 73) | Field data (current study) |
| Probability of Brucella sp. shed in milk of seropositive cattle and buffalo—least conservative scenario (buffalo) | Pshed | mean 0.30 (95% CI 0.25–0.35) | beta (102, 237) | [23] |
| Probability of Brucella sp. shed in milk of seropositive cattle and buffalo—most conservative scenario (cattle) | Pshed | mean 0.03 (95% CI 0.01–0.05) | beta (7, 255) | [24] |
| Probability and shedding range (Brucella sp. CFU/mL) in low-shedding cattle and buffalo | PLowShed; RLowShed | mean 0.83 (95% range 0.75–0.9); 0–103 CFU/mL | beta (86, 17); uniform (0, 1000) | [23] |
| Probability and shedding range (Brucella sp. CFU/mL) in high-shedding cattle and buffalo | 1 − PLowShed; RHighShed | mean 0.17 (95% range 0.10–0.24); 1 × 104–4 × 104 | 1 − PLowShed; uniform (1 × 104, 4 × 104) | [23] |
| Population | Scenario | Median Single Consumption Risk (95% Predicted Interval [PI]) | Absolute Risk Reduction (Single Consumption) | Median Annual Risk (95% PI) | Absolute Risk Reduction (Annual) |
|---|---|---|---|---|---|
| Cattle | With high shedders | 0.02 (0–0.96) | NA | 0.23 (0–1) | NA |
| Buffalo | 0.72 (0.06–0.99) | NA | 1.00 (0.55–1) | NA | |
| Combined | 0.09 (0.01–0.98) | NA | 0.69 (0.10–1) | NA | |
| Cattle | Only low shedders | 0.02 (0–0.91) | 0.2% | 0.20 (0–0.68) | 2.8% |
| Buffalo | 0.18 (0.05–0.33) | 54.4% | 0.90 (0.46–0.99) | 9.8% | |
| Combined | 0.08 (0.01–0.16) | 1.5% | 0.62 (0.07–0.88) | 6.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, V.; Singh, B.B.; Brookes, V.J. Risk Assessment of Brucella Exposure Through Raw Milk Consumption in India: One Health Implications and Control Strategies. Vet. Sci. 2025, 12, 465. https://doi.org/10.3390/vetsci12050465
Sharma V, Singh BB, Brookes VJ. Risk Assessment of Brucella Exposure Through Raw Milk Consumption in India: One Health Implications and Control Strategies. Veterinary Sciences. 2025; 12(5):465. https://doi.org/10.3390/vetsci12050465
Chicago/Turabian StyleSharma, Vijay, Balbir B. Singh, and Victoria J. Brookes. 2025. "Risk Assessment of Brucella Exposure Through Raw Milk Consumption in India: One Health Implications and Control Strategies" Veterinary Sciences 12, no. 5: 465. https://doi.org/10.3390/vetsci12050465
APA StyleSharma, V., Singh, B. B., & Brookes, V. J. (2025). Risk Assessment of Brucella Exposure Through Raw Milk Consumption in India: One Health Implications and Control Strategies. Veterinary Sciences, 12(5), 465. https://doi.org/10.3390/vetsci12050465