Regulation of the Ocular Cell/Tissue Response by Implantable Biomaterials and Drug Delivery Systems †



Abstract
1. Introduction
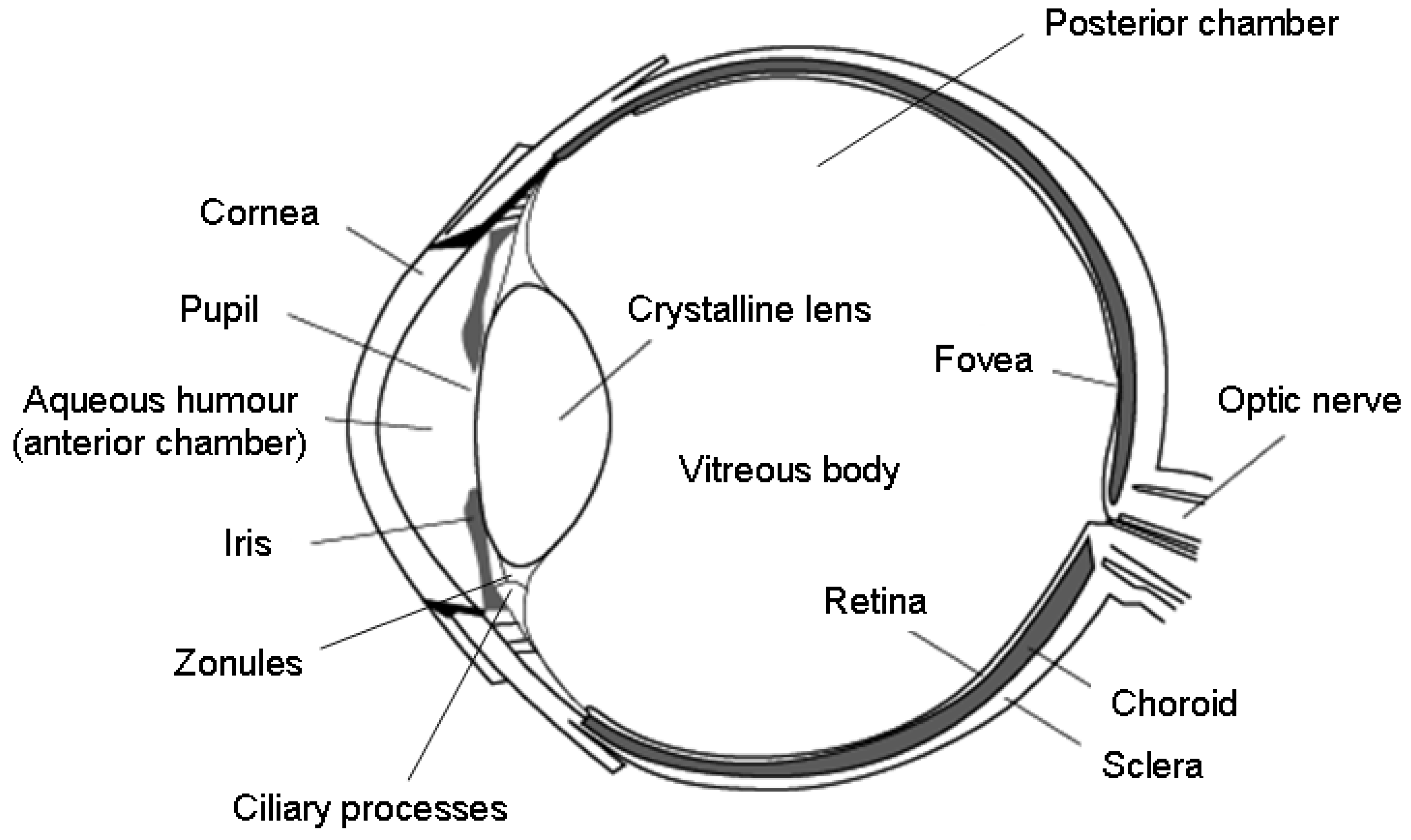
2. A Short Overview of Eye Anatomy
3. Strategies of Ocular Drug Administration
3.1. Topical Route
3.2. Intracameral Route
3.3. Transcleral/Periocular Route
3.4. Intravitreal Route
3.5. Sub-Retinal Route
3.6. Suprachoroidal Route
3.7. Systemic Route
4. Biomaterials and Implants for the Ocular Release of Therapeutics
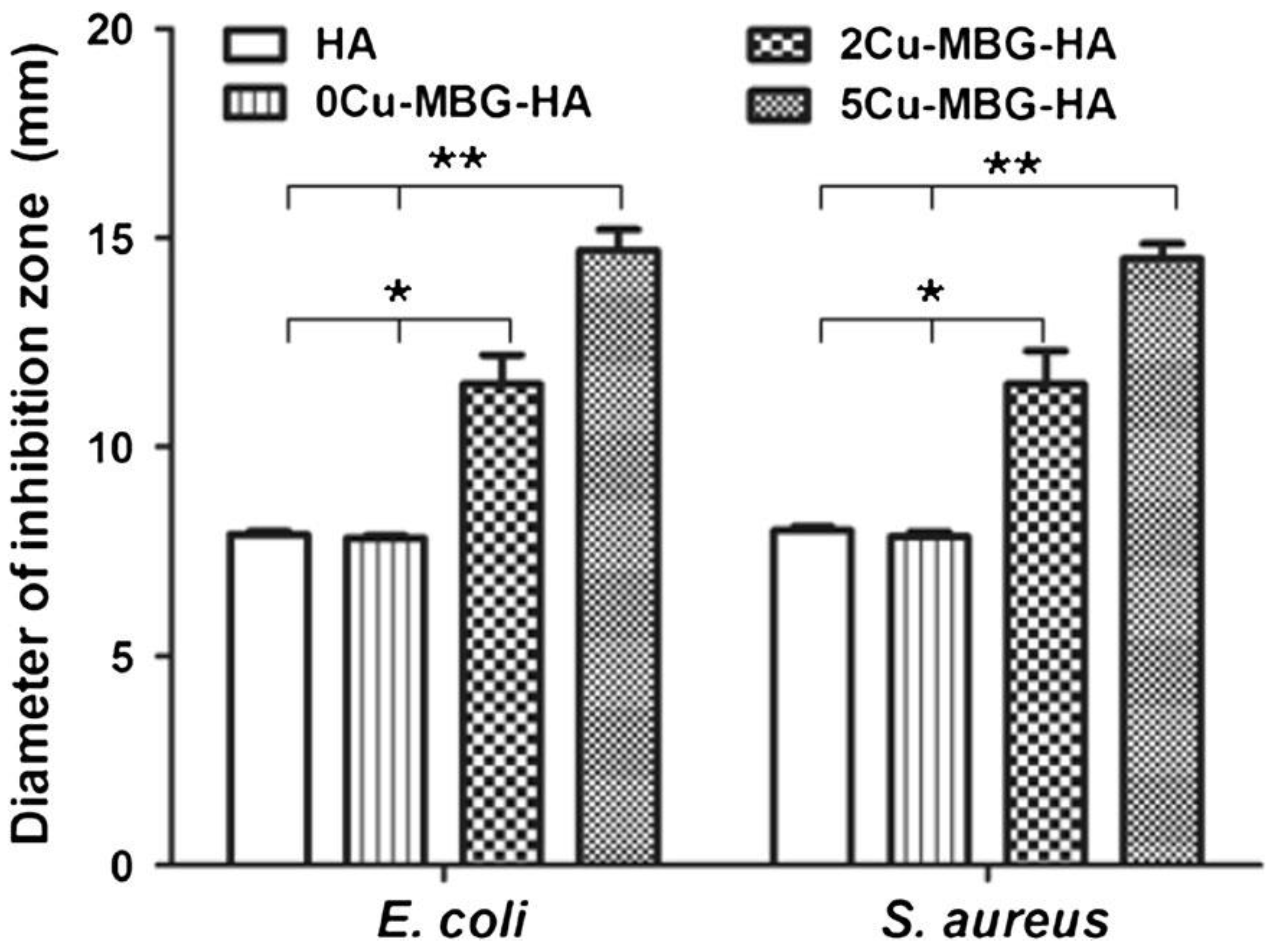
4.1. Therapeutic Ion Release from Orbital Implants and Ocular Prostheses
4.2. Microspheres and Nanospheres
4.2.1. Poly(lactic-co-glycolic) Acid
4.2.2. PLGA/Polyethylene Glycol (PEG) Copolymers
4.2.3. Copolymers with Gallic Acid
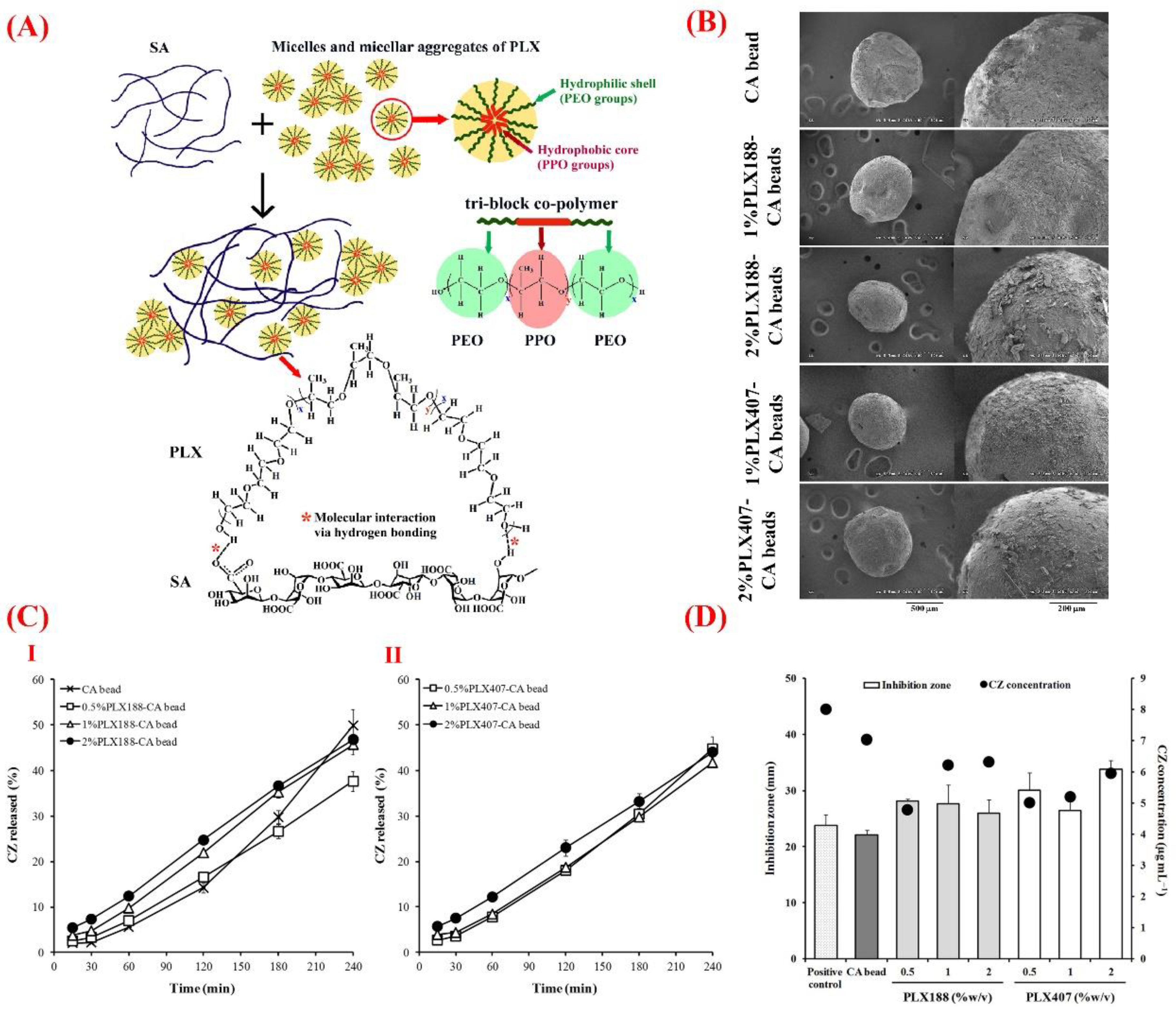
4.2.4. Copolymers with Polysaccharides
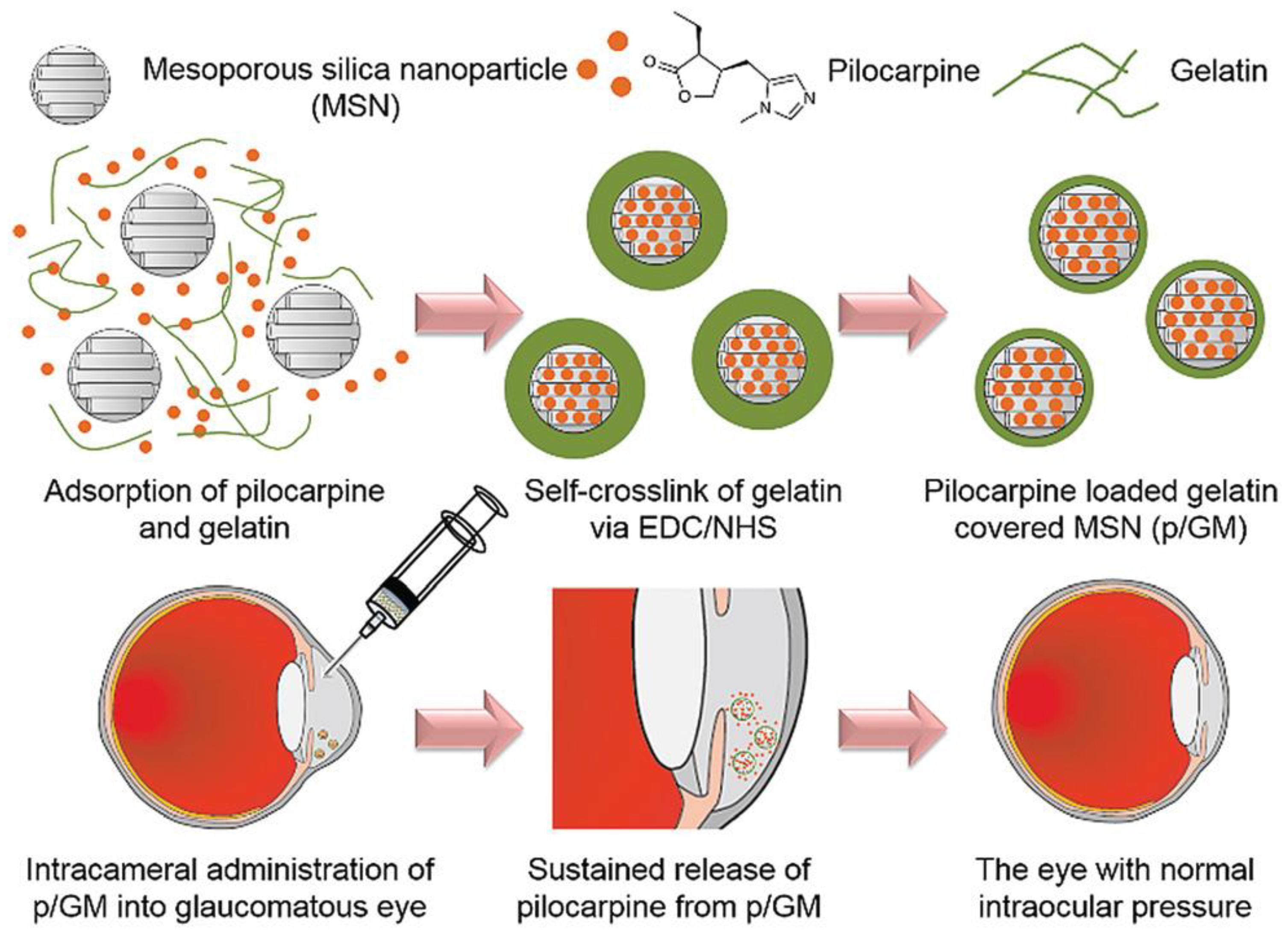
4.2.5. Gelatin
4.2.6. Chitosan
4.2.7. Other Polysaccharides
4.3. Liposomes
4.4. Hydrogels
4.4.1. Ionic Force-Sensitive Hydrogels in Topical Administration
4.4.2. Thermo-Reactive Hydrogels for Intravitreal Injection
4.4.3. Cell-Releasing Hydrogels
4.5. Combined Systems
5. Clinical Applications
5.1. Glaucoma
5.2. Corneal Transplantation
5.3. Macular Edema
5.4. Maculopathy
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bibliowicz, J.; Tittle, R.K.; Gross, J.M. Chapter 7—Toward a Better Understanding of Human Eye Disease: Insights from the Zebrafish, Danio rerio. In Progress in Molecular Biology and Translational Science; Chang, K.T., Min, K.-T., Eds.; Academic Press: Cambridge, MA, USA, 2011; Volume 100, pp. 287–330. [Google Scholar]
- Resnikoff, S.; Pascolini, D.; Etya’ale, D.; Kocur, I.; Pararajasegaram, R.; Pokharel, G.P.; Mariotti, S.P. Global data on visual impairment in the year 2002. Bull. World Health Organ. 2004, 82, 844–851. [Google Scholar]
- Flaxman, S.; Bourne, R.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.; Das, A.; Jonas, J.; Keeffe, J.; Kempen, J. Vision Loss Expert Group of the Global Burden of Disease Study Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef]
- Chen, H. Recent developments in ocular drug delivery. J. Drug Target. 2015, 23, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Samy, K.E.; Bernards, D.A.; Desai, T.A. Recent advances in intraocular sustained-release drug delivery devices. Drug Discov. Today 2019, 24, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Gilger, B.C.; Mandal, A.; Shah, S.; Mitra, A.K. Episcleral, Intrascleral, and Suprachoroidal Routes of Ocular Drug Delivery–Recent Research Advances and Patents. Recent Pat. Drug Deliv. Formul. 2014, 8, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular drug delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef]
- Mandal, A.; Gote, V.; Pal, D.; Ogundele, A.; Mitra, A.K. Ocular pharmacokinetics of a topical ophthalmic nanomicellar solution of cyclosporine (Cequa®) for dry eye disease. Pharm. Res. 2019, 36, 36. [Google Scholar] [CrossRef]
- Ahmed, I.; Patton, T. Importance of the noncorneal absorption route in topical ophthalmic drug delivery. Investig. Ophthalmol. Vis. Sci. 1985, 26, 584–587. [Google Scholar]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Alvarez-Lorenzo, C.; Anguiano-Igea, S.; Varela-García, A.; Vivero-Lopez, M.; Concheiro, A. Bioinspired hydrogels for drug-eluting contact lenses. Acta Biomater. 2019, 84, 49–62. [Google Scholar] [CrossRef]
- Gote, V.; Sikder, S.; Sicotte, J.; Pal, D. Ocular drug delivery: Present innovations and future challenges. J. Pharmacol. Exp. Ther. 2019, 370, 602–624. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.P.; Vaishya, R.; Pal, D.; Mitra, A.K. Novel pentablock copolymer-based nanoparticulate systems for sustained protein delivery. AAPS PharmSciTech 2015, 16, 327–343. [Google Scholar] [CrossRef] [PubMed]
- Joseph, M.; Trinh, H.M.; Cholkar, K.; Pal, D.; Mitra, A.K. Recent perspectives on the delivery of biologics to back of the eye. Expert Opin. Drug Deliv. 2017, 14, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Gaudana, R.; Mitra, A.K. A novel approach for antibody nanocarriers development through hydrophobic ion-pairing complexation. J. Microencapsul. 2014, 31, 542–550. [Google Scholar] [CrossRef]
- Vaishya, R.D.; Mandal, A.; Patel, S.; Mitra, A.K. Extended release microparticle-in-gel formulation of octreotide: Effect of polymer type on acylation of peptide during in vitro release. Int. J. Pharm. 2015, 496, 676–688. [Google Scholar] [CrossRef]
- Baino, F. The use of polymers in the treatment of retinal detachment: Current trends and future perspectives. Polymers 2010, 2, 286–322. [Google Scholar] [CrossRef]
- Bozukova, D.; Pagnoulle, C.; Jérôme, R.; Jérôme, C. Polymers in modern ophthalmic implants—Historical background and recent advances. Mater. Sci. Eng. R Rep. 2010, 69, 63–83. [Google Scholar] [CrossRef]
- Ghassemi, A.H.; van Steenbergen, M.J.; Barendregt, A.; Talsma, H.; Kok, R.J.; van Nostrum, C.F.; Crommelin, D.J.; Hennink, W.E. Controlled release of octreotide and assessment of peptide acylation from poly (D, L-lactide-co-hydroxymethyl glycolide) compared to PLGA microspheres. Pharm. Res. 2012, 29, 110–120. [Google Scholar] [CrossRef][Green Version]
- Patel, S.P.; Vaishya, R.; Patel, A.; Agrahari, V.; Pal, D.; Mitra, A.K. Optimization of novel pentablock copolymer based composite formulation for sustained delivery of peptide/protein in the treatment of ocular diseases. J. Microencapsul. 2016, 33, 103–113. [Google Scholar] [CrossRef]
- Kang-Mieler, J.J.; Osswald, C.R.; Mieler, W.F. Advances in ocular drug delivery: Emphasis on the posterior segment. Expert Opin. Drug Deliv. 2014, 11, 1647–1660. [Google Scholar] [CrossRef]
- Kang-Mieler, J.J.; Dosmar, E.; Liu, W.; Mieler, W.F. Extended ocular drug delivery systems for the anterior and posterior segments: Biomaterial options and applications. Expert Opin. Drug Deliv. 2017, 14, 611–620. [Google Scholar] [CrossRef]
- Lee, V.H.; Robinson, J.R. Topical ocular drug delivery: Recent developments and future challenges. J. Ocul. Pharmacol. Ther. 1986, 2, 67–108. [Google Scholar] [CrossRef] [PubMed]
- Barar, J.; Javadzadeh, A.R.; Omidi, Y. Ocular novel drug delivery: Impacts of membranes and barriers. Expert Opin. Drug Deliv. 2008, 5, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Bucolo, C.; Drago, F.; Salomone, S. Ocular drug delivery: A clue from nanotechnology. Front. Pharmacol. 2012, 3, 188. [Google Scholar] [CrossRef]
- Schultz, C.; Breaux, J.; Schentag, J.; Morck, D. Drug delivery to the posterior segment of the eye through hydrogel contact lenses. Clin. Exp. Optom. 2011, 94, 212–218. [Google Scholar] [CrossRef]
- Davis, B.M.; Normando, E.M.; Guo, L.; Turner, L.A.; Nizari, S.; O’Shea, P.; Moss, S.E.; Somavarapu, S.; Cordeiro, M.F. Topical Delivery of Avastin to the Posterior Segment of the Eye In Vivo Using Annexin A5-associated Liposomes. Small 2014, 10, 1575–1584. [Google Scholar] [CrossRef]
- Macha, S.; Hughes, P.M.; Mitra, A.K. Overview of ocular drug delivery. In Ophthalmic Drug Delivery Systems; CRC Press: Boca Raton, FL, USA, 2003; pp. 22–33. [Google Scholar]
- Group, E.E.S. Prophylaxis of postoperative endophthalmitis following cataract surgery: Results of the ESCRS multicenter study and identification of risk factors. J. Cataract Refract. Surg. 2007, 33, 978–988. [Google Scholar]
- Jamil, A.Z.; Ahmed, A.; Mirza, K.A. Effect of intracameral use of dexamethasone on corneal endothelial cells. J. Coll. Physicians Surg. Pak. 2014, 24, 245–248. [Google Scholar]
- Park, C.Y.; Lee, J.K.; Chuck, R.S. Toxic anterior segment syndrome-an updated review. BMC Ophthalmol. 2018, 18, 276. [Google Scholar] [CrossRef]
- Myles, M.E.; Neumann, D.M.; Hill, J.M. Recent progress in ocular drug delivery for posterior segment disease: Emphasis on transscleral iontophoresis. Adv. Drug Deliv. Rev. 2005, 57, 2063–2079. [Google Scholar] [CrossRef]
- Peyman, G.A.; Lad, E.M.; Moshfeghi, D.M. Intravitreal injection of therapeutic agents. Retina 2009, 29, 875–912. [Google Scholar] [CrossRef]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Aiello, L.P.; Antoszyk, A.N.; Arnold-Bush, B.; Baker, C.W.; Bressler, N.M.; Browning, D.J. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N. Engl. J. Med. 2015, 372, 1193–1203. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Tang, L.; Zhou, Y. Subretinal injection: A review on the novel route of therapeutic delivery for vitreoretinal diseases. Ophthalmic Res. 2017, 58, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Mühlfriedel, R.; Michalakis, S.; Garrido, M.G.; Biel, M.; Seeliger, M.W. Optimized technique for subretinal injections in mice. In Retinal Degeneration; Springer: Berlin/Heidelberg, Germany, 2012; pp. 343–349. [Google Scholar]
- Johnson, C.J.; Berglin, L.; Chrenek, M.A.; Redmond, T.; Boatright, J.H.; Nickerson, J.M. Technical brief: Subretinal injection and electroporation into adult mouse eyes. Mol. Vis. 2008, 14, 2211. [Google Scholar]
- Qi, Y.; Dai, X.; Zhang, H.; He, Y.; Zhang, Y.; Han, J.; Zhu, P.; Zhang, Y.; Zheng, Q.; Li, X. Trans-corneal subretinal injection in mice and its effect on the function and morphology of the retina. PLoS ONE 2015, 10, e0136523. [Google Scholar] [CrossRef] [PubMed]
- Timmers, A.M.; Zhang, H.; Squitieri, A.; Gonzalez-Pola, C. Subretinal injections in rodent eyes: Effects on electrophysiology and histology of rat retina. Mol. Vis. 2001, 7, 131–137. [Google Scholar]
- Ehlers, J.P.; Petkovsek, D.S.; Yuan, A.; Singh, R.P.; Srivastava, S.K. Intrasurgical assessment of subretinal tPA injection for submacular hemorrhage in the PIONEER study utilizing intraoperative OCT. Ophthalmic Surg. Lasers Imaging Retin. 2015, 46, 327–332. [Google Scholar] [CrossRef]
- Schlichtenbrede, F.C.; da Cruz, L.; Stephens, C.; Smith, A.J.; Georgiadis, A.; Thrasher, A.J.; Bainbridge, J.W.; Seeliger, M.W.; Ali, R.R. Long-term evaluation of retinal function in Prph2Rd2/Rd2 mice following AAV-mediated gene replacement therapy. J. Gene Med. 2003, 5, 757–764. [Google Scholar] [CrossRef]
- Pfeffer, B.; Wiggert, B.; Lee, L.; Zonnenberg, B.; Newsome, D.; Chader, G. The presence of a soluble interphotoreceptor retinol-binding protein (IRBP) in the retinal interphotoreceptor space. J. Cell. Physiol. 1983, 117, 333–341. [Google Scholar] [CrossRef]
- Parikh, S.; Le, A.; Davenport, J.; Gorin, M.B.; Nusinowitz, S.; Matynia, A. An alternative and validated injection method for accessing the subretinal space via a transcleral posterior approach. JoVE J. Vis. Exp. 2016, e54808. [Google Scholar] [CrossRef]
- Gerding, H. A new approach towards a minimal invasive retina implant. J. Neural Eng. 2007, 4, S30. [Google Scholar] [CrossRef]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Koerber, N.; Kearney, J.R.; Shingleton, B.J.; Samuelson, T.W. Canaloplasty: Circumferential viscodilation and tensioning of Schlemm canal using a flexible microcatheter for the treatment of open-angle glaucoma in adults: Two-year interim clinical study results. J. Cataract Refract. Surg. 2009, 35, 814–824. [Google Scholar] [CrossRef]
- Patel, S.R.; Lin, A.S.; Edelhauser, H.F.; Prausnitz, M.R. Suprachoroidal drug delivery to the back of the eye using hollow microneedles. Pharm. Res. 2011, 28, 166–176. [Google Scholar] [CrossRef]
- Safety Study of Suprachoroidal Triamcinolone Acetonide via Microneedle to Treat Uveitis. Clearside Biomedical Inc., 2013. Available online: https://ClinicalTrials.gov/show/NCT01789320 (accessed on 10 June 2020).
- Hughes, P.M.; Olejnik, O.; Chang-Lin, J.-E.; Wilson, C.G. Topical and systemic drug delivery to the posterior segments. Adv. Drug Deliv. Rev. 2005, 57, 2010–2032. [Google Scholar] [CrossRef]
- Gaudana, R.; Jwala, J.; Boddu, S.H.; Mitra, A.K. Recent perspectives in ocular drug delivery. Pharm. Res. 2009, 26, 1197. [Google Scholar] [CrossRef]
- Agrahari, V.; Mandal, A.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Ray, A.; Hadji, H.; Mitra, R.; Pal, D.; Mitra, A.K. A comprehensive insight on ocular pharmacokinetics. Drug Deliv. Transl. Res. 2016, 6, 735–754. [Google Scholar] [CrossRef]
- Moshfeghi, D.M.; Moshfeghi, A.A.; Finger, P.T. Enucleation. Surv. Ophthalmol. 2000, 44, 277–301. [Google Scholar] [CrossRef]
- Chalasani, R.; Poole-Warren, L.; Conway, R.M.; Ben-Nissan, B. Porous orbital implants in enucleation: A systematic review. Surv. Ophthalmol. 2007, 52, 145–155. [Google Scholar] [CrossRef]
- Baino, F.; Vitale-Brovarone, C. Bioceramics in ophthalmology. Acta Biomater. 2014, 10, 3372–3397. [Google Scholar] [CrossRef]
- Baino, F.; Perero, S.; Ferraris, S.; Miola, M.; Balagna, C.; Verné, E.; Vitale-Brovarone, C.; Coggiola, A.; Dolcino, D.; Ferraris, M. Biomaterials for orbital implants and ocular prostheses: Overview and future prospects. Acta Biomater. 2014, 10, 1064–1087. [Google Scholar] [CrossRef]
- Baino, F.; Potestio, I. Orbital implants: State-of-the-art review with emphasis on biomaterials and recent advances. Mater. Sci. Eng. C 2016, 69, 1410–1428. [Google Scholar] [CrossRef]
- Baino, F.; Ferraris, S.; Miola, M.; Perero, S.; Verné, E.; Coggiola, A.; Dolcino, D.; Ferraris, M. Novel antibacterial ocular prostheses: Proof of concept and physico-chemical characterization. Mater. Sci. Eng. C 2016, 60, 467–474. [Google Scholar] [CrossRef]
- Ye, J.; He, J.; Wang, C.; Yao, K.; Gou, Z. Copper-containing mesoporous bioactive glass coatings on orbital implants for improving drug delivery capacity and antibacterial activity. Biotechnol. Lett. 2014, 36, 961–968. [Google Scholar] [CrossRef]
- Chatterjee, A.K.; Chakraborty, R.; Basu, T. Mechanism of antibacterial activity of copper nanoparticles. Nanotechnology 2014, 25, 135101. [Google Scholar] [CrossRef]
- Giacomelli, C.; Trincavelli, M.L.; Satriano, C.; Hansson, Ö.; La Mendola, D.; Rizzarelli, E.; Martini, C. Copper (II) ions modulate Angiogenin activity in human endothelial cells. Int. J. Biochem. Cell Biol. 2015, 60, 185–196. [Google Scholar] [CrossRef]
- Urso, E.; Maffia, M. Behind the link between copper and angiogenesis: Established mechanisms and an overview on the role of vascular copper transport systems. J. Vasc. Res. 2015, 52, 172–196. [Google Scholar] [CrossRef]
- Mavria, G.; Vercoulen, Y.; Yeo, M.; Paterson, H.; Karasarides, M.; Marais, R.; Bird, D.; Marshall, C.J. ERK-MAPK signaling opposes Rho-kinase to promote endothelial cell survival and sprouting during angiogenesis. Cancer Cell 2006, 9, 33–44. [Google Scholar] [CrossRef]
- Baino, F. How can bioactive glasses be useful in ocular surgery? J. Biomed. Mater. Res. Part A 2015, 103, 1259–1275. [Google Scholar] [CrossRef]
- Wang, C.; Jin, K.; He, J.; Wang, J.; Yang, X.; Yao, C.; Dai, X.; Gao, C.; Gou, Z.; Ye, J. Synergistic Effect of Copper-Containing Mesoporous Bioactive Glass Coating on Stimulating Vascularization of Porous Hydroxyapatite Orbital Implants in Rabbits. J. Biomed. Nanotechnol. 2018, 14, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Baino, F.; Potestio, I.; Vitale-Brovarone, C. Production and physicochemical characterization of Cu-doped silicate bioceramic scaffolds. Materials 2018, 11, 1524. [Google Scholar] [CrossRef]
- Varde, N.K.; Pack, D.W. Microspheres for controlled release drug delivery. Expert Opin. Biol. Ther. 2004, 4, 35–51. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, S. A review of in vitro drug release test methods for nano-sized dosage forms. Adv. Pharm. 2014, 2014, 304757. [Google Scholar]
- Mi, F.-L.; Lin, Y.-M.; Wu, Y.-B.; Shyu, S.-S.; Tsai, Y.-H. Chitin/PLGA blend microspheres as a biodegradable drug-delivery system: Phase-separation, degradation and release behavior. Biomaterials 2002, 23, 3257–3267. [Google Scholar] [CrossRef]
- Hans, M.L.; Lowman, A.M. Biodegradable nanoparticles for drug delivery and targeting. Curr. Opin. Solid State Mater. Sci. 2002, 6, 319–327. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An overview of poly (lactic-co-glycolic) acid (PLGA)-based biomaterials for bone tissue engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Astete, C.E.; Sabliov, C.M. Synthesis and characterization of PLGA nanoparticles. J. Biomater. Sci. Polym. Ed. 2006, 17, 247–289. [Google Scholar] [CrossRef]
- Xie, H.; Smith, J.W. Fabrication of PLGA nanoparticles with a fluidic nanoprecipitation system. J. Nanobiotechnol. 2010, 8, 18. [Google Scholar] [CrossRef]
- Mi, F.-L.; Shyu, S.-S.; Lin, Y.-M.; Wu, Y.-B.; Peng, C.-K.; Tsai, Y.-H. Chitin/PLGA blend microspheres as a biodegradable drug delivery system: A new delivery system for protein. Biomaterials 2003, 24, 5023–5036. [Google Scholar] [CrossRef]
- Makadia, H.K.; Siegel, S.J. Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef]
- Siegel, S.J.; Kahn, J.B.; Metzger, K.; Winey, K.I.; Werner, K.; Dan, N. Effect of drug type on the degradation rate of PLGA matrices. Eur. J. Pharm. Biopharm. 2006, 64, 287–293. [Google Scholar] [CrossRef]
- Keles, H.; Naylor, A.; Clegg, F.; Sammon, C. Investigation of factors influencing the hydrolytic degradation of single PLGA microparticles. Polym. Degrad. Stab. 2015, 119, 228–241. [Google Scholar] [CrossRef]
- Zheng, C.; Liang, W. A one-step modified method to reduce the burst initial release from PLGA microspheres. Drug Deliv. 2010, 17, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Yeo, Y.; Park, K. Control of encapsulation efficiency and initial burst in polymeric microparticle systems. Arch. Pharm. Res. 2004, 27, 1. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.-H.; Gao, J.-Q.; Zhang, Y.-P.; Liang, W.-Q. A protein delivery system: Biodegradable alginate–chitosan–poly (lactic-co-glycolic acid) composite microspheres. Biochem. Biophys. Res. Commun. 2004, 323, 1321–1327. [Google Scholar] [CrossRef]
- Ghassemi, A.H.; van Steenbergen, M.J.; Talsma, H.; van Nostrum, C.F.; Crommelin, D.J.; Hennink, W.E. Hydrophilic polyester microspheres: Effect of molecular weight and copolymer composition on release of BSA. Pharm. Res. 2010, 27, 2008–2017. [Google Scholar] [CrossRef]
- Manoharan, C.; Singh, J. Insulin loaded PLGA microspheres: Effect of zinc salts on encapsulation, release, and stability. J. Pharm. Sci. 2009, 98, 529–542. [Google Scholar] [CrossRef]
- French, A.C.; Thompson, A.L.; Davis, B.G. High-Purity Discrete PEG-Oligomer Crystals Allow Structural Insight. Angew. Chem. Int. Ed. 2009, 48, 1248–1252. [Google Scholar] [CrossRef]
- Chou, S.-F.; Luo, L.-J.; Lai, J.-Y. Gallic acid grafting effect on delivery performance and antiglaucoma efficacy of antioxidant-functionalized intracameral pilocarpine carriers. Acta Biomater. 2016, 38, 116–128. [Google Scholar] [CrossRef]
- Curcio, M.; Puoci, F.; Iemma, F.; Parisi, O.I.; Cirillo, G.; Spizzirri, U.G.; Picci, N. Covalent insertion of antioxidant molecules on chitosan by a free radical grafting procedure. J. Agric. Food Chem. 2009, 57, 5933–5938. [Google Scholar] [CrossRef]
- Yang, L.; Cui, F.; Cun, D.; Tao, A.; Shi, K.; Lin, W. Preparation, characterization and biodistribution of the lactone form of 10-hydroxycamptothecin (HCPT)-loaded bovine serum albumin (BSA) nanoparticles. Int. J. Pharm. 2007, 340, 163–172. [Google Scholar] [CrossRef]
- Zhai, P.; Chen, X.; Schreyer, D.J. PLGA/alginate composite microspheres for hydrophilic protein delivery. Mater. Sci. Eng. C 2015, 56, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Jay, S.M.; Saltzman, W.M. Controlled delivery of VEGF via modulation of alginate microparticle ionic crosslinking. J. Control. Release 2009, 134, 26–34. [Google Scholar] [CrossRef]
- Li, L.; Lu, C.; Wang, L.; Chen, M.; White, J.; Hao, X.; McLean, K.M.; Chen, H.; Hughes, T.C. Gelatin-based photocurable hydrogels for corneal wound repair. ACS Appl. Mater. Interfaces 2018, 10, 13283–13292. [Google Scholar] [CrossRef]
- Jumelle, C.; Gholizadeh, S.; Annabi, N.; Dana, R. Advances and limitations of drug delivery systems formulated as eye drops. J. Control. Release 2020, 321, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-L.; Chen, K.-H.; Su, W.-Y.; Lee, Y.-H.; Wu, C.-C.; Lin, F.-H. Cationic Gelatin Nanoparticles for Drug Delivery to the Ocular Surface: In Vitro and In Vivo Evaluation. J. Nanomater. 2013, 2013, 238351. [Google Scholar] [CrossRef]
- Hathout, R.M.; Omran, M.K. Gelatin-based particulate systems in ocular drug delivery. Pharm. Dev. Technol. 2016, 21, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Mahor, A.; Prajapati, S.K.; Verma, A.; Gupta, R.; Iyer, A.K.; Kesharwani, P. Moxifloxacin loaded gelatin nanoparticles for ocular delivery: Formulation and in-vitro, in-vivo evaluation. J. Colloid Interface Sci. 2016, 483, 132–138. [Google Scholar] [CrossRef]
- El-Feky, G.S.; Zayed, G.M.; Elshaier, Y.A.; Alsharif, F.M. Chitosan-gelatin hydrogel crosslinked with oxidized sucrose for the ocular delivery of timolol maleate. J. Pharm. Sci. 2018, 107, 3098–3104. [Google Scholar] [CrossRef]
- Esteban-Pérez, S.; Andrés-Guerrero, V.; López-Cano, J.J.; Molina-Martínez, I.; Herrero-Vanrell, R.; Bravo-Osuna, I. Gelatin Nanoparticles-HPMC Hybrid System for Effective Ocular Topical Administration of Antihypertensive Agents. Pharmaceutics 2020, 12, 306. [Google Scholar] [CrossRef]
- Liao, Y.-T.; Lee, C.-H.; Chen, S.-T.; Lai, J.-Y.; Wu, K.C.-W. Gelatin-functionalized mesoporous silica nanoparticles with sustained release properties for intracameral pharmacotherapy of glaucoma. J. Mater. Chem. B 2017, 5, 7008–7013. [Google Scholar] [CrossRef]
- Mohebbi, S.; Nezhad, M.N.; Zarrintaj, P.; Jafari, S.H.; Gholizadeh, S.S.; Saeb, M.R.; Mozafari, M. Chitosan in biomedical engineering: A critical review. Curr. Stem Cell Res. Ther. 2019, 14, 93–116. [Google Scholar] [CrossRef] [PubMed]
- Alonso, M.J.; Sánchez, A. The potential of chitosan in ocular drug delivery. J. Pharm. Pharmacol. 2003, 55, 1451–1463. [Google Scholar] [CrossRef] [PubMed]
- Qiao, X.; Peng, X.; Qiao, J.; Jiang, Z.; Han, B.; Yang, C.; Liu, W. Evaluation of a photocrosslinkable hydroxyethyl chitosan hydrogel as a potential drug release system for glaucoma surgery. J. Mater. Sci. Mater. Med. 2017, 28, 149. [Google Scholar] [CrossRef] [PubMed]
- Intini, C.; Elviri, L.; Cabral, J.; Mros, S.; Bergonzi, C.; Bianchera, A.; Flammini, L.; Govoni, P.; Barocelli, E.; Bettini, R. 3D-printed chitosan-based scaffolds: An in vitro study of human skin cell growth and an in-vivo wound healing evaluation in experimental diabetes in rats. Carbohydr. Polym. 2018, 199, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Neamnark, A.; Sanchavanakit, N.; Pavasant, P.; Rujiravanit, R.; Supaphol, P. In vitro biocompatibility of electrospun hexanoyl chitosan fibrous scaffolds towards human keratinocytes and fibroblasts. Eur. Polym. J. 2008, 44, 2060–2067. [Google Scholar] [CrossRef]
- Abilova, G.K.; Kaldybekov, D.B.; Ozhmukhametova, E.K.; Saimova, A.Z.; Kazybayeva, D.S.; Irmukhametova, G.S.; Khutoryanskiy, V.V. Chitosan/poly (2-ethyl-2-oxazoline) films for ocular drug delivery: Formulation, miscibility, in vitro and in vivo studies. Eur. Polym. J. 2019, 116, 311–320. [Google Scholar] [CrossRef]
- Franca, J.R.; Fuscaldi, L.L.; Ribeiro, T.G.; Foureaux, G.; Cesar, A.L.; Castilho, R.O.; Cronemberger, S.; Ferreira, A.J.; Fernandes, S.O.; Cardoso, V.N. Use of chitosan as pharmaceutical excipient in ocular drug delivery systems: Sterilization and pharmacokinetics. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 2227–2237. [Google Scholar] [CrossRef]
- Shinde, U.A.; Joshi, P.N.; Jain, D.D.; Singh, K. Preparation and evaluation of N-trimethyl chitosan nanoparticles of flurbiprofen for ocular delivery. Curr. Eye Res. 2019, 44, 575–582. [Google Scholar] [CrossRef]
- Pakzad, Y.; Fathi, M.; Omidi, Y.; Mozafari, M.; Zamanian, A. Synthesis and characterization of timolol maleate-loaded quaternized chitosan-based thermosensitive hydrogel: A transparent topical ocular delivery system for the treatment of glaucoma. Int. J. Biol. Macromol. 2020, 159, 117–128. [Google Scholar] [CrossRef]
- Imam, S.S.; Abbas Bukhari, S.N.; Ahmad, J.; Ali, A. Formulation and optimization of levofloxacin loaded chitosan nanoparticle for ocular delivery: In-vitro characterization, ocular tolerance and antibacterial activity. Int. J. Biol. Macromol. 2018, 108, 650–659. [Google Scholar] [CrossRef]
- Li, J.; Jin, X.; Yang, Y.; Zhang, L.; Liu, R.; Li, Z. Trimethyl chitosan nanoparticles for ocular baicalein delivery: Preparation, optimization, in vitro evaluation, in vivo pharmacokinetic study and molecular dynamics simulation. Int. J. Biol. Macromol. 2020, 156, 749–761. [Google Scholar] [CrossRef]
- Elsaid, N.; Jackson, T.L.; Elsaid, Z.; Alqathama, A.; Somavarapu, S. PLGA microparticles entrapping chitosan-based nanoparticles for the ocular delivery of ranibizumab. Mol. Pharm. 2016, 13, 2923–2940. [Google Scholar] [CrossRef]
- Kalam, M.A. Development of chitosan nanoparticles coated with hyaluronic acid for topical ocular delivery of dexamethasone. Int. J. Biol. Macromol. 2016, 89, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Nagarwal, R.C.; Kumar, R.; Pandit, J. Chitosan coated sodium alginate–chitosan nanoparticles loaded with 5-FU for ocular delivery: In vitro characterization and in vivo study in rabbit eye. Eur. J. Pharm. Sci. 2012, 47, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Liu, X.; Hu, W.; Bai, Y.; Zhang, L. Preparation and evaluation of naringenin-loaded sulfobutylether-β-cyclodextrin/chitosan nanoparticles for ocular drug delivery. Carbohydr. Polym. 2016, 149, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Chaiyasan, W.; Srinivas, S.P.; Tiyaboonchai, W. Mucoadhesive chitosan–dextran sulfate nanoparticles for sustained drug delivery to the ocular surface. J. Ocul. Pharmacol. Ther. 2013, 29, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Bhatta, R.; Chandasana, H.; Chhonker, Y.; Rathi, C.; Kumar, D.; Mitra, K.; Shukla, P. Mucoadhesive nanoparticles for prolonged ocular delivery of natamycin: In vitro and pharmacokinetics studies. Int. J. Pharm. 2012, 432, 105–112. [Google Scholar] [CrossRef]
- Dubashynskaya, N.; Poshina, D.; Raik, S.; Urtti, A.; Skorik, Y.A. Polysaccharides in Ocular Drug Delivery. Pharmaceutics 2020, 12, 22. [Google Scholar] [CrossRef]
- Patchan, M.; Graham, J.; Xia, Z.; Maranchi, J.; McCally, R.; Schein, O.; Elisseeff, J.H.; Trexler, M. Synthesis and properties of regenerated cellulose-based hydrogels with high strength and transparency for potential use as an ocular bandage. Mater. Sci. Eng. C 2013, 33, 3069–3076. [Google Scholar] [CrossRef]
- Yusufu, M.; Liu, X.; Zheng, T.; Fan, F.; Xu, J.; Luo, Y. Hydroxypropyl methylcellulose 2% for dry eye prevention during phacoemulsification in senile and diabetic patients. Int. Ophthalmol. 2018, 38, 1261–1273. [Google Scholar] [CrossRef]
- Wallerstein, A.; Jackson, W.B.; Chambers, J.; Moezzi, A.M.; Lin, H.; Simmons, P.A. Management of post-LASIK dry eye: A multicenter randomized comparison of a new multi-ingredient artificial tear to carboxymethylcellulose. Clin. Ophthalmol. 2018, 12, 839. [Google Scholar] [CrossRef] [PubMed]
- Labetoulle, M.; Chiambaretta, F.; Shirlaw, A.; Leaback, R.; Baudouin, C. Osmoprotectants, carboxymethylcellulose and hyaluronic acid multi-ingredient eye drop: A randomised controlled trial in moderate to severe dry eye. Eye 2017, 31, 1409–1416. [Google Scholar] [CrossRef]
- Mu, H.; Wang, Y.; Wei, H.; Lu, H.; Feng, Z.; Yu, H.; Xing, Y.; Wang, H. Collagen peptide modified carboxymethyl cellulose as both antioxidant drug and carrier for drug delivery against retinal ischaemia/reperfusion injury. J. Cell. Mol. Med. 2018, 22, 5008–5019. [Google Scholar] [CrossRef] [PubMed]
- Mohan, E.C.; Kandukuri, J.M.; Allenki, V. Preparation and evaluation of in-situ-gels for ocular drug delivery. J. Pharm. Res. 2009, 2, 1089–1094. [Google Scholar]
- Orasugh, J.T.; Sarkar, G.; Saha, N.R.; Das, B.; Bhattacharyya, A.; Das, S.; Mishra, R.; Roy, I.; Chattoapadhyay, A.; Ghosh, S.K.; et al. Effect of cellulose nanocrystals on the performance of drug loaded in situ gelling thermo-responsive ophthalmic formulations. Int. J. Biol. Macromol. 2019, 124, 235–245. [Google Scholar] [CrossRef]
- Xuan, F.; Rong, J.; Liang, M.; Zhang, X.; Sun, J.; Zhao, L.; Li, Y.; Liu, D.; Li, F.; Wang, X. Biocompatibility and effectiveness evaluation of a new hemostatic embolization agent: Thrombin loaded alginate calcium microsphere. BioMed Res. Int. 2017, 2017, 1875258. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; He, S.; Chen, B. Retinoic acid-loaded alginate microspheres as a slow release drug delivery carrier for intravitreal treatment. Biomed. Pharmacother. 2018, 97, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Toragall, V.; Jayapala, N.; Muthukumar, S.; Baskaran, V. Biodegradable chitosan-sodium alginate-oleic acid nanocarrier promotes bioavailability and target delivery of lutein in rat model with no toxicity. Food Chem. 2020, 330, 127195. [Google Scholar] [CrossRef]
- Szekalska, M.; Puciłowska, A.; Szymańska, E.; Ciosek, P.; Winnicka, K. Alginate: Current use and future perspectives in pharmaceutical and biomedical applications. Int. J. Polym. Sci. 2016, 2016, 7697031. [Google Scholar] [CrossRef]
- Silva, D.; Pinto, L.F.; Bozukova, D.; Santos, L.F.; Serro, A.P.; Saramago, B. Chitosan/alginate based multilayers to control drug release from ophthalmic lens. Colloids Surf. B Biointerfaces 2016, 147, 81–89. [Google Scholar] [CrossRef]
- Khlibsuwan, R.; Khunkitti, W.; Pongjanyakul, T. Alginate-poloxamer beads for clotrimazole delivery: Molecular interactions, mechanical properties, and anticandidal activity. Int. J. Biol. Macromol. 2020, 148, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Pandey, P.; Parashar, S. Pectin as Natural Polymer: An overview. Res. J. Pharm. Technol. 2017, 10, 1225–1229. [Google Scholar] [CrossRef]
- Pereira, R.F.; Barrias, C.C.; Bártolo, P.J.; Granja, P.L. Cell-instructive pectin hydrogels crosslinked via thiol-norbornene photo-click chemistry for skin tissue engineering. Acta Biomater. 2018, 66, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Hussien, N.A.; Işıklan, N.; Türk, M. Pectin-conjugated magnetic graphene oxide nanohybrid as a novel drug carrier for paclitaxel delivery. Artif. Cells Nanomed. Biotechnol. 2018, 46, 264–273. [Google Scholar] [CrossRef]
- Chan, S.Y.; Chan, B.Q.Y.; Liu, Z.; Parikh, B.H.; Zhang, K.; Lin, Q.; Su, X.; Kai, D.; Choo, W.S.; Young, D.J. Electrospun pectin-polyhydroxybutyrate nanofibers for retinal tissue engineering. ACS Omega 2017, 2, 8959–8968. [Google Scholar] [CrossRef]
- Sharma, R.; Ahuja, M.; Kaur, H. Thiolated pectin nanoparticles: Preparation, characterization and ex vivo corneal permeation study. Carbohydr. Polym. 2012, 87, 1606–1610. [Google Scholar] [CrossRef]
- Dubey, V.; Mohan, P.; Dangi, J.S.; Kesavan, K. Brinzolamide loaded chitosan-pectin mucoadhesive nanocapsules for management of glaucoma: Formulation, characterization and pharmacodynamic study. Int. J. Biol. Macromol. 2019, 152, 1224–1232. [Google Scholar] [CrossRef]
- Smistad, G.; Bøyum, S.; Alund, S.J.; Samuelsen, A.B.C.; Hiorth, M. The potential of pectin as a stabilizer for liposomal drug delivery systems. Carbohydr. Polym. 2012, 90, 1337–1344. [Google Scholar] [CrossRef]
- Hamcerencu, M.; Popa, M.; Riess, G.; Desbrieres, J. Chemically modified xanthan and gellan for preparation of biomaterials for ophthalmic applications. Polym. Int. 2019. [Google Scholar] [CrossRef]
- Montani, G.; Blanco, A.R.; Mazzone, M.G. Xanthan gum 0.2% lubricant eyedrop used in contact lens wearers increase stability of pre lens tear film and improve the optical quality of the eye. Contact Lens Anterior Eye 2018, 41, S71. [Google Scholar] [CrossRef]
- Bhowmik, M.; Kumari, P.; Sarkar, G.; Bain, M.K.; Bhowmick, B.; Mollick, M.M.R.; Mondal, D.; Maity, D.; Rana, D.; Bhattacharjee, D. Effect of xanthan gum and guar gum on in situ gelling ophthalmic drug delivery system based on poloxamer-407. Int. J. Biol. Macromol. 2013, 62, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Rubio, A.Y.; Baiza-Durán, L.; Olvera-Montaño, O.; Miranda-Robles, M.; Bonilla-García, J.; Mercado-Sesma, A. Histopathological changes on the ocular surface of New Zealand white rabbits after instillation of a fixed combination of 0.09% xanthan gum and 0.1% chondroitin sulfate. Int. Ophthalmol. 2016, 36, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Amico, C.; Tornetta, T.; Scifo, C.; Blanco, A.R. Antioxidant effect of 0.2% xanthan gum in ocular surface corneal epithelial cells. Curr. Eye Res. 2015, 40, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Allison, S.D. Liposomal drug delivery. J. Infus. Nurs. 2007, 30, 89–95. [Google Scholar] [CrossRef]
- Kaur, I.P.; Garg, A.; Singla, A.K.; Aggarwal, D. Vesicular systems in ocular drug delivery: An overview. Int. J. Pharm. 2004, 269, 1–14. [Google Scholar] [CrossRef]
- Natarajan, J.V.; Ang, M.; Darwitan, A.; Chattopadhyay, S.; Wong, T.T.; Venkatraman, S.S. Nanomedicine for glaucoma: Liposomes provide sustained release of latanoprost in the eye. Int. J. Nanomed. 2012, 7, 123. [Google Scholar]
- Fahmy, H.M.; Saad, E.A.E.-M.S.; Sabra, N.M.; El-Gohary, A.A.; Mohamed, F.F.; Gaber, M.H. Treatment merits of latanoprost/thymoquinone–encapsulated liposome for glaucomatus rabbits. Int. J. Pharm. 2018, 548, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Bressler, N.M.; Arnold, J.; Benchaboune, M.; Blumenkranz, M.S.; Fish, G.E.; Gragoudas, E.S.; Lewis, H.; Schmidt-Erfurth, U.; Slakter, J.S.; Bressler, S.B. Verteporfin therapy of subfoveal choroidal neovascularization in patients with age-related macular degeneration: Additional information regarding baseline lesion composition’s impact on vision outcomes-TAP report No. 3. Arch. Ophthalmol. 2002, 120, 1443–1454. [Google Scholar]
- Bressler, N. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: Two-year results of 2 randomized clinical trials-tap report 2. Arch. Ophthalmol. 2001, 119, 198–207. [Google Scholar]
- Fenton, C.; Perry, C.M. Verteporfin. Drugs Aging 2006, 23, 421–445. [Google Scholar] [CrossRef]
- Lajavardi, L.; Bochot, A.; Camelo, S.; Goldenberg, B.; Naud, M.-C.; Behar-Cohen, F.; Fattal, E.; de Kozak, Y. Downregulation of endotoxin-induced uveitis by intravitreal injection of vasoactive intestinal peptide encapsulated in liposomes. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3230–3238. [Google Scholar] [CrossRef] [PubMed]
- Kang-Mieler, J.J.; Rudeen, K.M.; Liu, W.; Mieler, W.F. Advances in ocular drug delivery systems. Eye 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.S. Hydrogels for biomedical applications. Adv. Drug Deliv. Rev. 2012, 64, 18–23. [Google Scholar] [CrossRef]
- Mahinroosta, M.; Farsangi, Z.J.; Allahverdi, A.; Shakoori, Z. Hydrogels as intelligent materials: A brief review of synthesis, properties and applications. Mater. Today Chem. 2018, 8, 42–55. [Google Scholar] [CrossRef]
- Kanjickal, D.; Lopina, S.; Evancho-Chapman, M.M.; Schmidt, S.; Donovan, D. Effects of sterilization on poly (ethylene glycol) hydrogels. J. Biomed. Mater. Res. Part A 2008, 87, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Karajanagi, S.S.; Yoganathan, R.; Mammucari, R.; Park, H.; Cox, J.; Zeitels, S.M.; Langer, R.; Foster, N.R. Application of a dense gas technique for sterilizing soft biomaterials. Biotechnol. Bioeng. 2011, 108, 1716–1725. [Google Scholar] [CrossRef]
- Hammer, N.; Brandl, F.P.; Kirchhof, S.; Messmann, V.; Goepferich, A.M. Protein compatibility of selected cross-linking reactions for hydrogels. Macromol. Biosci. 2015, 15, 405–413. [Google Scholar] [CrossRef]
- Moreau, M.F.; Chappard, D.; Lesourd, M.; Monthéard, J.P.; Baslé, M.F. Free radicals and side products released during methylmethacrylate polymerization are cytotoxic for osteoblastic cells. J. Biomed. Mater. Res. 1998, 40, 124–131. [Google Scholar] [CrossRef]
- Kirchhof, S.; Goepferich, A.M.; Brandl, F.P. Hydrogels in ophthalmic applications. Eur. J. Pharm. Biopharm. 2015, 95, 227–238. [Google Scholar] [CrossRef]
- Ribeiro, A.; Veiga, F.; Santos, D.; Torres-Labandeira, J.J.; Concheiro, A.; Alvarez-Lorenzo, C. Bioinspired Imprinted PHEMA-Hydrogels for Ocular Delivery of Carbonic Anhydrase Inhibitor Drugs. Biomacromolecules 2011, 12, 701–709. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Lakdawala, D.H.; Shaikh, A.A.; Desai, A.R.; Choksi, H.H.; Vaidya, R.J.; Ranch, K.M.; Koli, A.R.; Vyas, B.A.; Shah, D.O. In vitro and in vivo evaluation of novel implantation technology in hydrogel contact lenses for controlled drug delivery. J. Control. Release 2016, 226, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Janga, K.Y.; Tatke, A.; Balguri, S.P.; Lamichanne, S.P.; Ibrahim, M.M.; Maria, D.N.; Jablonski, M.M.; Majumdar, S. Ion-sensitive in situ hydrogels of natamycin bilosomes for enhanced and prolonged ocular pharmacotherapy: In vitro permeability, cytotoxicity and in vivo evaluation. Artif. Cells Nanomed. Biotechnol. 2018, 46, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.K.; Das, M.; Jain, S. In situ gel systems as ‘smart’ carriers for sustained ocular drug delivery. Expert Opin. Drug Deliv. 2012, 9, 383–402. [Google Scholar] [CrossRef]
- Kesavan, K.; Kant, S.; Pandit, J.K. Therapeutic effectiveness in the treatment of experimental bacterial keratitis with ion-activated mucoadhesive hydrogel. Ocul. Immunol. Inflamm. 2016, 24, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Ranch, K.; Patel, H.; Chavda, L.; Koli, A.; Maulvi, F.; Parikh, R.K. Development of in situ ophthalmic gel of dexamethasone sodium phosphate and chloramphenicol: A viable alternative to conventional eye drops. J. Appl. Pharm. Sci. 2017, 7, 101–108. [Google Scholar]
- Peppas, N.; Bures, P.; Leobandung, W.; Ichikawa, H. Hydrogels in pharmaceutical formulations. Eur. J. Pharm. Biopharm. 2000, 50, 27–46. [Google Scholar] [CrossRef]
- Kushwaha, S.K.; Saxena, P.; Rai, A. Stimuli sensitive hydrogels for ophthalmic drug delivery: A review. Int. J. Pharm. Investig. 2012, 2, 54. [Google Scholar] [CrossRef]
- Hu, C.-C.; Chaw, J.-R.; Chen, C.-F.; Liu, H.-W. Controlled release bevacizumab in thermoresponsive hydrogel found to inhibit angiogenesis. Bio Med. Mater. Eng. 2014, 24, 1941–1950. [Google Scholar] [CrossRef]
- Rauck, B.M.; Friberg, T.R.; Medina Mendez, C.A.; Park, D.; Shah, V.; Bilonick, R.A.; Wang, Y. Biocompatible Reverse Thermal Gel Sustains the Release of Intravitreal Bevacizumab In Vivo. Investig. Ophthalmol. Vis. Sci. 2014, 55, 469–476. [Google Scholar] [CrossRef]
- Derwent, J.J.K.; Mieler, W.F. Thermoresponsive hydrogels as a new ocular drug delivery platform to the posterior segment of the eye. Trans. Am. Ophthalmol. Soc. 2008, 106, 206. [Google Scholar]
- Klouda, L. Thermoresponsive hydrogels in biomedical applications: A seven-year update. Eur. J. Pharm. Biopharm. 2015, 97, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Turturro, S.B.; Guthrie, M.J.; Appel, A.A.; Drapala, P.W.; Brey, E.M.; Pérez-Luna, V.H.; Mieler, W.F.; Kang-Mieler, J.J. The effects of cross-linked thermo-responsive PNIPAAm-based hydrogel injection on retinal function. Biomaterials 2011, 32, 3620–3626. [Google Scholar] [CrossRef] [PubMed]
- Kang-Mieler, J.J.; Mieler, W.F. Thermo-responsive hydrogels for ocular drug delivery. In Retinal Pharmacotherapeutics; Karger Publishers: Basel, Switzerland, 2016; Volume 55, pp. 104–111. [Google Scholar]
- Drapala, P.W.; Jiang, B.; Chiu, Y.-C.; Mieler, W.F.; Brey, E.M.; Kang-Mieler, J.J.; Pérez-Luna, V.H. The effect of glutathione as chain transfer agent in PNIPAAm-based thermo-responsive hydrogels for controlled release of proteins. Pharm. Res. 2014, 31, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Jin, L.; Luo, Z.; Yu, J.; Shi, S.; Zhang, Z.; Shen, M.; Chen, H.; Li, X.; Song, Z. An injectable thermosensitive polymeric hydrogel for sustained release of Avastin® to treat posterior segment disease. Int. J. Pharm. 2015, 490, 375–383. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, R.; Zarembinski, T.I.; Doty, N.; Jiang, C.; Regatieri, C.; Zhang, X.; Young, M.J. The application of hyaluronic acid hydrogels to retinal progenitor cell transplantation. Tissue Eng. Part A 2013, 19, 135–142. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Shin, J.-M.; Yeum, C.E.; Chae, G.T.; Chun, M.-H.; Oh, S.-J. Intravitreal delivery of mesenchymal stem cells loaded onto hydrogel affects the regulatory expression of endogenous NGF and BDNF in ischemic rat retina. Tissue Eng. Regen. Med. 2012, 9, 249–258. [Google Scholar] [CrossRef]
- Ballios, B.G.; Cooke, M.J.; van der Kooy, D.; Shoichet, M.S. A hydrogel-based stem cell delivery system to treat retinal degenerative diseases. Biomaterials 2010, 31, 2555–2564. [Google Scholar] [CrossRef]
- Burdick, J.A.; Ward, M.; Liang, E.; Young, M.J.; Langer, R. Stimulation of neurite outgrowth by neurotrophins delivered from degradable hydrogels. Biomaterials 2006, 27, 452–459. [Google Scholar] [CrossRef]
- Lajavardi, L.; Camelo, S.; Agnely, F.; Luo, W.; Goldenberg, B.; Naud, M.-C.; Behar-Cohen, F.; de Kozak, Y.; Bochot, A. New formulation of vasoactive intestinal peptide using liposomes in hyaluronic acid gel for uveitis. J. Control. Release 2009, 139, 22–30. [Google Scholar] [CrossRef]
- Osswald, C.R.; Kang-Mieler, J.J. Controlled and extended in vitro release of bioactive anti-vascular endothelial growth factors from a microsphere-hydrogel drug delivery system. Curr. Eye Res. 2016, 41, 1216–1222. [Google Scholar] [CrossRef]
- Osswald, C.R.; Kang-Mieler, J.J. Controlled and extended release of a model protein from a microsphere-hydrogel drug delivery system. Ann. Biomed. Eng. 2015, 43, 2609–2617. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, M.J.; Osswald, C.R.; Valio, N.L.; Mieler, W.F.; Kang-Mieler, J.J. Objective area measurement technique for choroidal neovascularization from fluorescein angiography. Microvasc. Res. 2014, 91, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Aung, T.; Bourne, R.R.; Bron, A.M.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 390, 2183–2193. [Google Scholar] [CrossRef]
- Hong, C.-H.; Arosemena, A.; Zurakowski, D.; Ayyala, R.S. Glaucoma drainage devices: A systematic literature review and current controversies. Surv. Ophthalmol. 2005, 50, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Ayyala, R.S.; Harman, L.E.; Michelini-Norris, B.; Ondrovic, L.E.; Haller, E.; Margo, C.E.; Stevens, S.X. Comparison of different biomaterials for glaucoma drainage devices. Arch. Ophthalmol. 1999, 117, 233–236. [Google Scholar] [CrossRef]
- Ayyala, R.S.; Michelini-Norris, B.; Flores, A.; Haller, E.; Margo, C.E. Comparison of different biomaterials for glaucoma drainage devices: Part 2. Arch. Ophthalmol. 2000, 118, 1081–1084. [Google Scholar] [CrossRef]
- Blake, D.A.; Sahiner, N.; John, V.T.; Clinton, A.D.; Galler, K.E.; Walsh, M.; Arosemena, A.; Johnson, P.Y.; Ayyala, R.S. Inhibition of cell proliferation by mitomycin C incorporated into P (HEMA) hydrogels. J. Glaucoma 2006, 15, 291–298. [Google Scholar] [CrossRef]
- Sahiner, N.; Kravitz, D.J.; Qadir, R.; Blake, D.A.; Haque, S.; John, V.T.; Margo, C.E.; Ayyala, R.S. Creation of a drug-coated glaucoma drainage device using polymer technology: In vitro and in vivo studies. Arch. Ophthalmol. 2009, 127, 448–453. [Google Scholar] [CrossRef][Green Version]
- Hovakimyan, M.; Siewert, S.; Schmidt, W.; Sternberg, K.; Reske, T.; Stachs, O.; Guthoff, R.; Wree, A.; Witt, M.; Schmitz, K.-P. Development of an experimental drug eluting suprachoroidal microstent as glaucoma drainage device. Transl. Vis. Sci. Technol. 2015, 4, 14. [Google Scholar] [CrossRef]
- Ishida, K.; Netland, P.A.; Costa, V.P.; Shiroma, L.; Khan, B.; Ahmed, I.I.K. Comparison of polypropylene and silicone Ahmed glaucoma valves. Ophthalmology 2006, 113, 1320–1326. [Google Scholar] [CrossRef]
- Hinkle, D.; Zurakowski, D.; Ayyala, R. A comparison of the polypropylene plate Ahmed™ glaucoma valve to the silicone plate Ahmed™ glaucoma flexible valve. Eur. J. Ophthalmol. 2007, 17, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Cantor, L.; Burgoyne, J.; Sanders, S.; Bhavnani, V.; Hoop, J.; Brizendine, E. The effect of mitomycin C on Molteno implant surgery: A 1-year randomized, masked, prospective study. J. Glaucoma 1998, 7, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, J.A.; Hollander, D.A.; Juster, R.P.; Lee, L.C. Ahmed valve implantation with adjunctive mitomycin C and 5-fluorouracil: Long-term outcomes. Am. J. Ophthalmol. 2008, 146, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Bi, X.-Z.; Pan, W.-H.; Yu, X.-P.; Song, Z.-M.; Ren, Z.-J.; Sun, M.; Li, C.-H.; Nan, K.-H. Application of 5-Fluorouracil-Polycaprolactone Sustained-Release Film in Ahmed Glaucoma Valve Implantation Inhibits Postoperative Bleb Scarring in Rabbit Eyes. PLoS ONE 2015, 10, e0141467. [Google Scholar] [CrossRef] [PubMed]
- Alice, L.Y.; Kaiser, M.; Schaumberger, M.; Messmer, E.; Kook, D.; Welge-Lussen, U. Donor-related risk factors and preoperative recipient-related risk factors for graft failure. Cornea 2014, 33, 1149–1156. [Google Scholar]
- Larkin, D.; Calder, V.; Lightman, S. Identification and characterization of cells infiltrating the graft and aqueous humour in rat corneal allograft rejection. Clin. Exp. Immunol. 1997, 107, 381–391. [Google Scholar] [CrossRef]
- Nicholls, S.M.; Banerjee, S.; Figueiredo, F.C.; Crome, S.; Mistry, S.; Easty, D.L.; Dick, A.D. Differences in leukocyte phenotype and interferon-γ expression in stroma and endothelium during corneal graft rejection. Exp. Eye Res. 2006, 83, 339–347. [Google Scholar] [CrossRef]
- Shi, W.; Chen, M.; Xie, L.; Liu, M.; Gao, H.; Wang, T.; Wu, X.; Zhao, J. A novel cyclosporine a drug-delivery system for prevention of human corneal rejection after high-risk keratoplasty: A clinical study. Ophthalmology 2013, 120, 695–702. [Google Scholar] [CrossRef]
- Zhang, T.; Li, Z.; Liu, T.; Li, S.; Gao, H.; Wei, C.; Shi, W. Cyclosporine a drug-delivery system for high-risk penetrating keratoplasty: Stabilizing the intraocular immune microenvironment. PLoS ONE 2018, 13, e0196571. [Google Scholar] [CrossRef]
- Banerjee, S. A review of developments in the management of retinal diseases. J. R. Soc. Med. 2006, 99, 125–127. [Google Scholar] [CrossRef]
- Haghjou, N.; Soheilian, M.; Abdekhodaie, M.J. Sustained release intraocular drug delivery devices for treatment of uveitis. J. Ophthalmic Vis. Res. 2011, 6, 317. [Google Scholar] [PubMed]
- De Oliveira Dias, J.R.; Nunes, R.P.; Goldhardt, R. New drugs and new posterior delivery methods in CME. Curr. Ophthalmol. Rep. 2017, 5, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Castro-Navarro, V.; Cervera-Taulet, E.; Navarro-Palop, C.; Monferrer-Adsuara, C.; Hernández-Bel, L.; Montero-Hernández, J. Intravitreal dexamethasone implant Ozurdex® in naïve and refractory patients with different subtypes of diabetic macular edema. BMC Ophthalmol. 2019, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Mello Filho, P.; Andrade, G.; Maia, A.; Maia, M.; Neto, L.B.; Neto, A.M.; Brasil, O.M.; Minelli, E.; Dalloul, C.; Iglicki, M. Effectiveness and safety of intravitreal dexamethasone implant (Ozurdex) in patients with diabetic macular edema: A real-world experience. Ophthalmologica 2019, 241, 9–16. [Google Scholar] [CrossRef]
- Soubrane, G.; Behar-Cohen, F. Micro-implant d’acétonide de fluocinolone (ILUVIEN®) pour l’œdème maculaire diabétique chronique. J. Fr. Ophtalmol. 2015, 38, 159–167. [Google Scholar] [CrossRef][Green Version]
- Massa, H.; Nagar, A.M.; Vergados, A.; Dadoukis, P.; Patra, S.; Panos, G.D. Intravitreal fluocinolone acetonide implant (ILUVIEN®) for diabetic macular oedema: A literature review. J. Int. Med. Res. 2019, 47, 31–43. [Google Scholar] [CrossRef]
- Prata, A.I.; Coimbra, P.; Pina, M.E. Preparation of dexamethasone ophthalmic implants: A comparative study of in vitro release profiles. Pharm. Dev. Technol. 2018, 23, 218–224. [Google Scholar] [CrossRef]
- Fialho, S.L.; Behar-Cohen, F.; Silva-Cunha, A. Dexamethasone-loaded poly (ε-caprolactone) intravitreal implants: A pilot study. Eur. J. Pharm. Biopharm. 2008, 68, 637–646. [Google Scholar] [CrossRef]
- Mandal, A.; Pal, D.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Mitra, A.K. Ocular delivery of proteins and peptides: Challenges and novel formulation approaches. Adv. Drug Deliv. Rev. 2018, 126, 67–95. [Google Scholar] [CrossRef]
- Tyagi, P.; Barros, M.; Stansbury, J.W.; Kompella, U.B. Light-activated, in situ forming gel for sustained suprachoroidal delivery of bevacizumab. Mol. Pharm. 2013, 10, 2858–2867. [Google Scholar] [CrossRef]
- Wang, C.-H.; Hwang, Y.-S.; Chiang, P.-R.; Shen, C.-R.; Hong, W.-H.; Hsiue, G.-H. Extended release of bevacizumab by thermosensitive biodegradable and biocompatible hydrogel. Biomacromolecules 2012, 13, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Sheshala, R.; Hong, G.C.; Yee, W.P.; Meka, V.S.; Thakur, R.R.S. In situ forming phase-inversion implants for sustained ocular delivery of triamcinolone acetonide. Drug Deliv. Transl. Res. 2019, 9, 534–542. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Function |
|---|---|
| Cornea | The anterior, transparent part of the eye that covers the pupil and iris. It provides most of the eye’s focusing power (about 2/3). |
| Ocular chambers | Two compartments that are filled with aqueous fluid. The anterior chamber is the space between the cornea and the iris, whereas the smaller posterior chamber is between the iris and the lens. |
| Iris | The pigmented membrane that gives the eye its color; it lies between the cornea and the crystalline lens and separates the anterior chamber from the posterior chamber. Its main purpose is to block excess light from entering the eye and to control the iris opening or “pupil” for differing amounts of ambient light. |
| Aqueous humor | A transparent fluid filling the anterior and posterior chambers. It provides nutrition to the areas lacking blood vessels (i.e., the crystalline lens and the cornea). |
| Crystalline lens | Transparent, biconvex structure located behind the iris; it is responsible for additional power for focusing light onto the retina. |
| Tenon’s capsule | External to the sclera, it is a membranous structure that envelopes the extraocular eye muscles, as well as the eyeball and optic nerve. |
| Sclera | Opaque, fibrous outer tunic of the eye mainly composed of collagen. It holds together the contents of the eye and contains openings and canals for the vessels and nerves entering and exiting the eye. |
| Vitreous humor | Gel-like substance located in the posterior portion of the eye, filling in the area between the lens and the retina. |
| Choroid | Rich in blood vessels, provides nutrition to the retina. |
| Retina | Multilayered sensory tissue of the posterior eyeball onto which light entering the eye is focused, forming a reversed and inverted image. It contains photosensitive receptor cells, the rods and cones, which are capable of converting light into nerve impulses that are conducted and further relayed to the brain via the optic nerve. |
| Optic nerve | Structure at the back of the eye responsible for carrying nerve impulses from the retina to different areas of the brain. |
| Conjunctiva | The mucous membrane covering the anterior sclera and the posterior aspect of the eyelids. |
| Extraocular muscles (EOMs) | Six muscles which control the movement of the eye and are responsible for movements along three different axes: horizontal, vertical, and torsional. Horizontal movements are controlled entirely by the medial and lateral rectus muscles. Vertical movements require the coordinated action of the superior and inferior rectus muscles, as well as the oblique muscles. The oblique muscles are also primarily responsible for torsional movements. |
| Brand Name | Material | Active Ingredient | Dosage Form | Indication |
|---|---|---|---|---|
| Vitrasert® | PVA, EVA | Ganciclovir | Intravitreal implant | AIDS-related CMV retinitis |
| Retisert® | PVA, silicone | Fluocinolone acetonide | Intravitreal implant | Noninfectious uveitis, posterior uveitis |
| Ozurdex® | PLGA | Dexamethasone | Intravitreal implant | - DME - CRVO - BRVO - Posterior uveitis |
| Iluvien® | Polyimide | Fluocinolone acetonide | Intravitreal implant | - DME - Wet AMD |
| Yutiq® | Polyimide | Fluocinolone acetonide | Intravitreal implant | Chronic noninfectious uveitis |
| DEXYCU® | Acetyl triethyl citrate | Dexamethasone | Intraocular implant | Postoperative inflammation |
| OTX-TKI/IVT | Hydrogel | TKIs; anti-VEGF | Intravitreal implants | AMD |
| PDS | Undisclosed polymer | Ranibizumab | Intravitreal implants | Wet AMD |
| Brimo PS DDS® | PLGA | Brimonidine tartrate | Intravitreal implants | - Pars plana vitrectomy AMD - Retinal detachment - Geographic atrophy MD |
| Rysmon® TG | Methylcellulose | Timolol maleate | Eye drop | Glaucoma |
| Betoptic S® | Amberlite® IRP-69 | Betaxolol | Eye drop | Glaucoma |
| Timoptic-XE® | Gellan gum | Timolol maleate | Eye drop | Glaucoma |
| AzaSite® | Polycarbophil | Azithromycin | Eye drop | Bacterial conjunctivitis |
| AzaSite Plus™ | Polycarbophil | Azithromycin/Dexamethasone (ISV-502) | Eye drop | Blepharoconjunctivitis |
| Lumitect™ | Silicone matrix | Cyclosporin | Episcleral implant | GVHD and corneal allograft rejection |
| I-vation™ TA | PMMA/EVA | Triamcinolone acetonide | Intravitreal implants | DME |
| Visudyne® | Liposome | Verteporfin | Intravenous injection | Wet AMD |
| Durezol™ | Emulsion | Difluprednate | Eye drop | DME |
| Cortiject® | Emulsion | Corticosteroid prodrug (NOVA-63035) | Intravitreal injection | DME |
| Surodex™ | PLGA, HPMC | Dexamethasone | Subconjunctival implants | Postoperative inflammation following cataract surgery |
| Lacrisert® | HPC | HPC | Cul-de-sac implants | Moderate to severe dry eye syndrome, including keratitis sicca |
| Murocel® | Methylcellulose (MC) | PEG, PVA, Povidone | Eye drop | Dried eyes |
| Celluvisc® | CMC sodium | Carmellose sodium | Eye drop | Dried eyes |
| Ultra Tears® | HPMC | PEG, PVA, Povidone | Eye drop | Dried and irritated eyes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baino, F.; Kargozar, S. Regulation of the Ocular Cell/Tissue Response by Implantable Biomaterials and Drug Delivery Systems. Bioengineering 2020, 7, 65. https://doi.org/10.3390/bioengineering7030065
Baino F, Kargozar S. Regulation of the Ocular Cell/Tissue Response by Implantable Biomaterials and Drug Delivery Systems. Bioengineering. 2020; 7(3):65. https://doi.org/10.3390/bioengineering7030065
Chicago/Turabian StyleBaino, Francesco, and Saeid Kargozar. 2020. "Regulation of the Ocular Cell/Tissue Response by Implantable Biomaterials and Drug Delivery Systems" Bioengineering 7, no. 3: 65. https://doi.org/10.3390/bioengineering7030065
APA StyleBaino, F., & Kargozar, S. (2020). Regulation of the Ocular Cell/Tissue Response by Implantable Biomaterials and Drug Delivery Systems. Bioengineering, 7(3), 65. https://doi.org/10.3390/bioengineering7030065