

CT-Based Radiomics Enhance Respiratory Function Analysis for Lung SBRT

 , , , , ,
, , , , ,  ,
,  , , , ,
, , , , 
Abstract
1. Introduction
2. Patients and Methods
2.1. Clinical Dataset
2.2. Imaging Dataset and Segmentation
2.3. Feature Extraction
2.4. Statistical Analysis
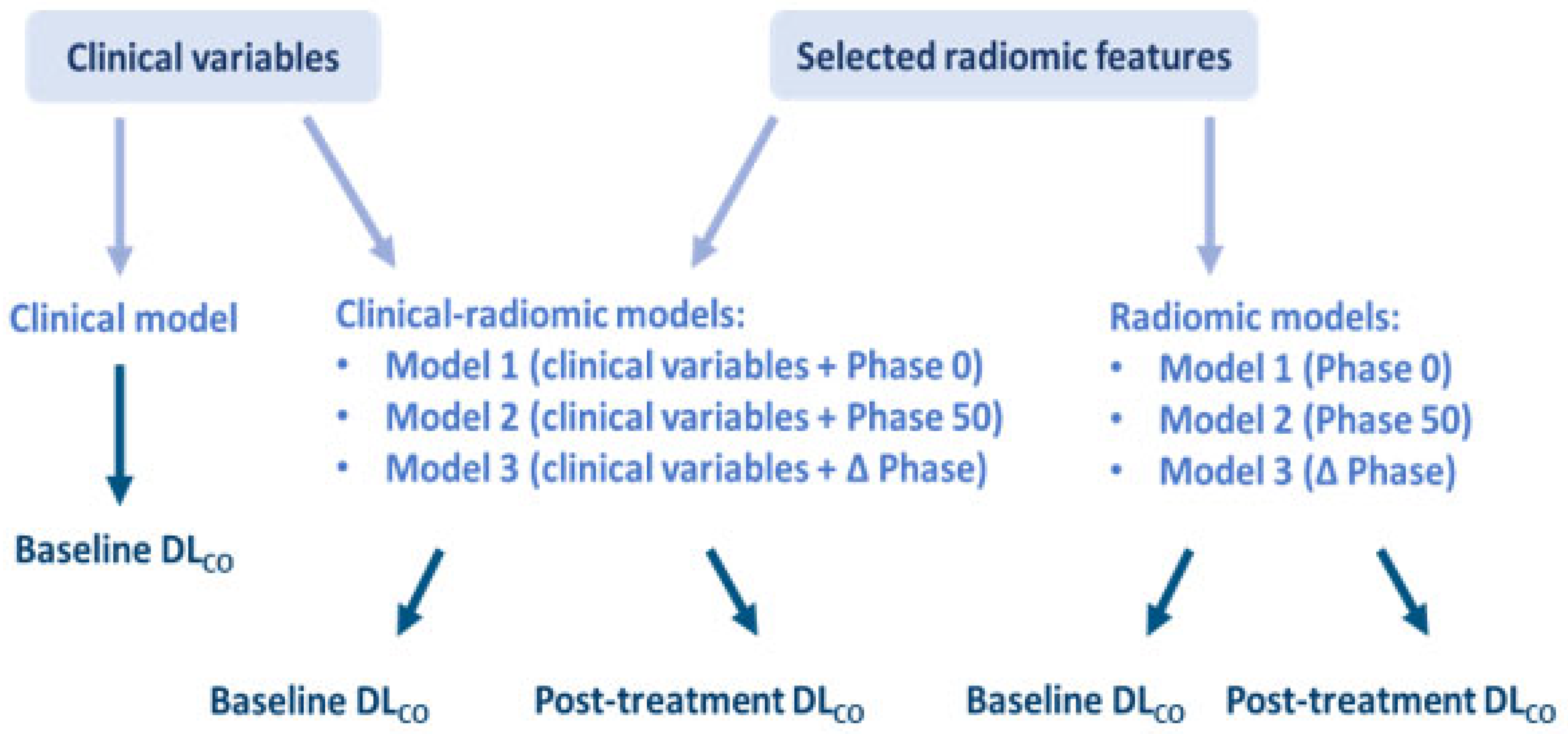
2.5. Model Building
- the first radiomic model (Model 1) was built considering the radiomic features selected from Phase 0, the second one (Model 2) the radiomic features selected from Phase 50, and the third one (Model 3) the radiomic features selected from those that were different between the two phases;
- the three clinical-radiomic models were built following the same criteria, but considering the clinical variable selected as exemplary in each model.
3. Results
3.1. Patient Characteristics
3.2. Associations
3.3. Selected Radiomic Features
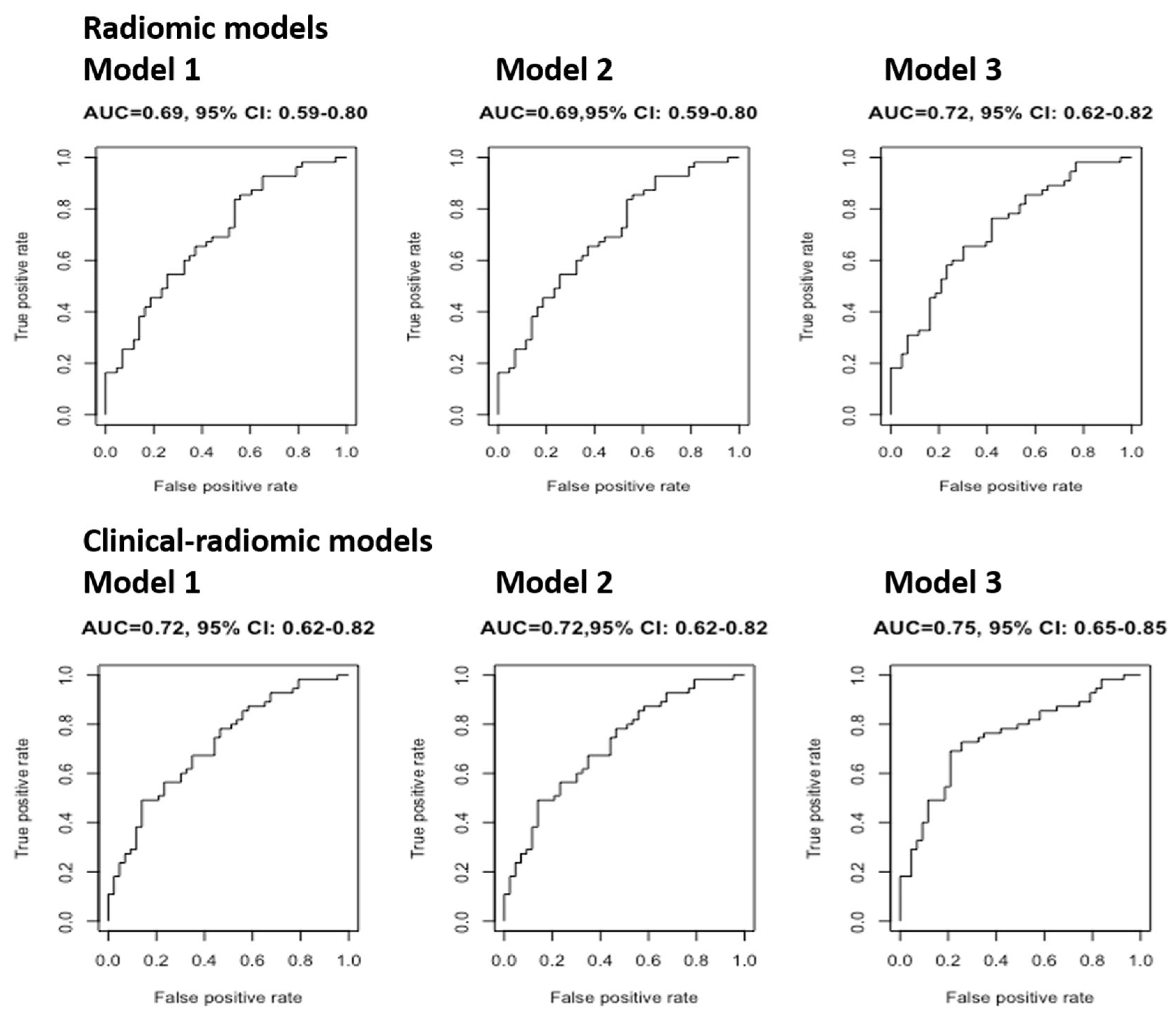
3.4. Model Performances
Baseline DLCO
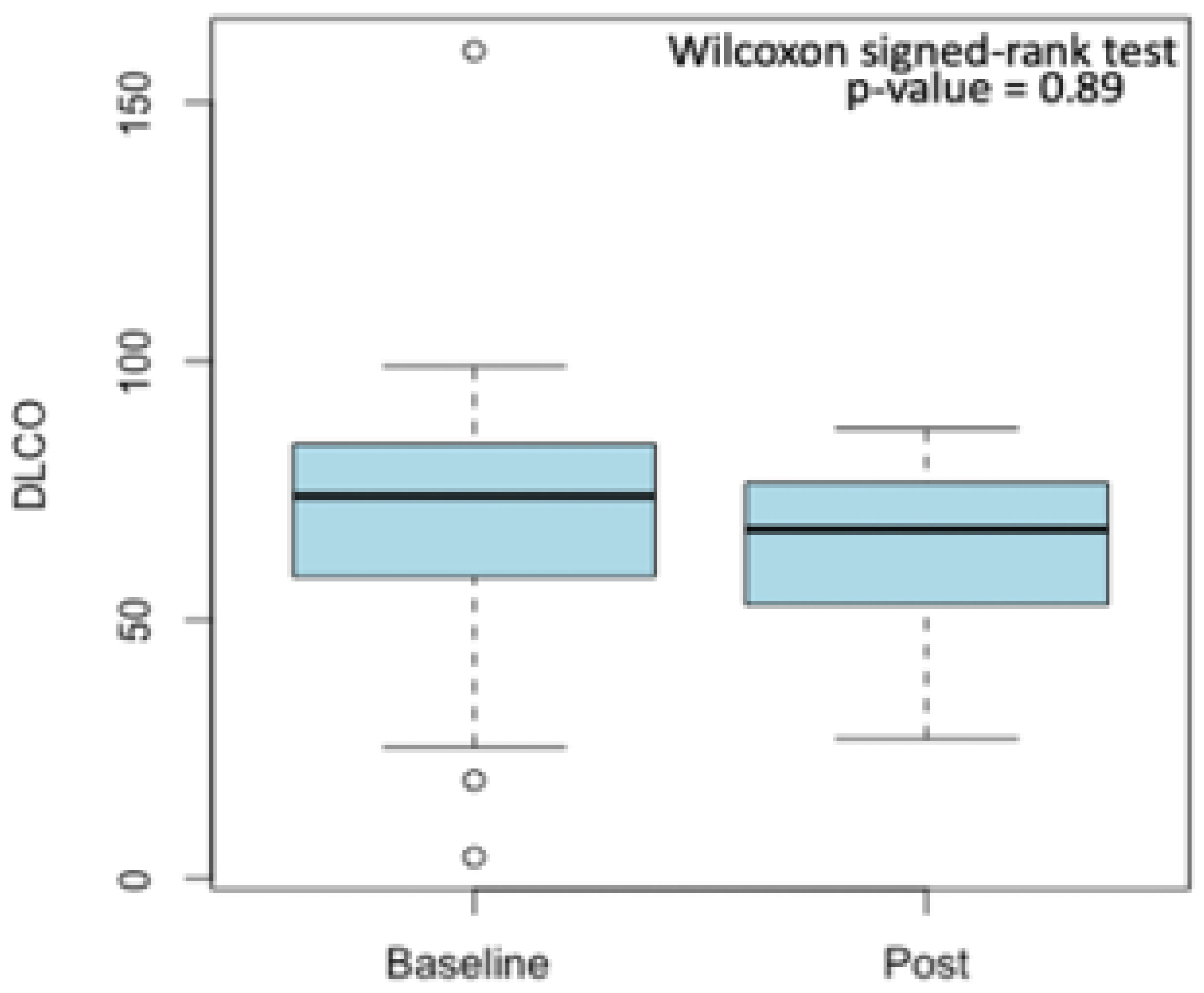
3.5. Post-Treatment DLCO
4. Discussion
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 4DCT | Four-Dimensional Computed Tomography |
| AUC | Area Under the Curve |
| CCI | Charlson Comorbidity Index |
| CI | Confidence Interval |
| COPD | Chronic Obstructive Pulmonary Disease |
| DLCO | Diffusing Capacity to Carbon Monoxide |
| ECIS | European Cancer Information System |
| ESMO | European Society for Medical Oncology |
| ES | Early stage |
| FEV1 | Forced Expiratory Volume 1 |
| GLCM | Gray Leve Co-Occurrence Matrix |
| GLDM | Gray Level Dependence Matrix |
| GLSZM | Gray Level Size Zone Matrix |
| FVC | Forced Vital Capacity |
| GTV | Gross Tumor Volume |
| LASSO | Least Absolute Shrinkage and Selection Operator |
| NSCLC | Non-Small Cell Lung Cancer |
| OMD | Oligometastatic Disease |
| PFTs | Pulmonary Function Tests |
| PMD | Polymetastatic Disease |
| ROI | Region of Interest |
| SBRT | Stereotactic Body Radiotherapy |
| VOI | Volume of Interest |
References
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef]
- Marvaso, G.; Mastroleo, F.; Corrao, G.; Zaffaroni, M.; Vincini, M.G.; Borghetti, P.; Cuccia, F.; Federico, M.; Montesi, G.; Pontoriero, A.; et al. A Bibliometric Analysis of the Oligometastatic State over the Last Two Decades: A Shifting Paradigm for Oncology? An AIRO Oligometastatic Study Group. Cancers 2023, 15, 3902. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, P.; All, S.; Berry, M.F.; Boike, T.P.; Bradfield, L.; Dingemans, A.-M.C.; Feldman, J.; Gomez, D.R.; Hesketh, P.J.; Jabbour, S.K.; et al. Treatment of Oligometastatic Non-Small Cell Lung Cancer: An ASTRO/ESTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2023, 13, 393–412. [Google Scholar] [CrossRef]
- Tsai, C.J.; Yang, J.T.; Shaverdian, N.; Patel, J.; Shepherd, A.F.; Eng, J.; Guttmann, D.; Yeh, R.; Gelblum, D.Y.; Namakydoust, A.; et al. Standard-of-care systemic therapy with or without stereotactic body radiotherapy in patients with oligoprogressive breast cancer or non-small-cell lung cancer (Consolidative Use of Radiotherapy to Block [CURB] oligoprogression): An open-label, randomised, controlled, phase 2 study. Lancet 2024, 403, 171–182. [Google Scholar] [CrossRef]
- Virbel, G.; Le Fèvre, C.; Noël, G.; Antoni, D. Stereotactic Body Radiotherapy for Patients with Lung Oligometastatic Disease: A Five-Year Systematic Review. Cancers 2021, 13, 3623. [Google Scholar] [CrossRef]
- Gomez, D.R.; Blumenschein, G.R.; Lee, J.J.; Hernandez, M.; Ye, R.; Camidge, D.R.; Doebele, R.C.; Skoulidis, F.; Gaspar, L.E.; Gibbons, D.L.; et al. Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: A multicentre, randomised, controlled, phase 2 study. Lancet Oncol. 2016, 17, 1672–1682. [Google Scholar] [CrossRef]
- AlGhamdi, H.; Dhont, J.; Krayem, M.; De Bruyn, P.; Engels, B.; Van Gestel, D.; Van den Begin, R. The Road to Dissemination: The Concept of Oligometastases and the Barriers for Widespread Disease. Cancers 2022, 14, 2046. [Google Scholar] [CrossRef]
- Bergsma, D.P.; Salama, J.K.; Singh, D.P.; Chmura, S.J.; Milano, M.T. Radiotherapy for Oligometastatic Lung Cancer. Front. Oncol. 2017, 7, 210. [Google Scholar] [CrossRef]
- Rieber, J.; Abbassi-Senger, N.; Adebahr, S.; Andratschke, N.; Blanck, O.; Duma, M.; Eble, M.J.; Ernst, I.; Flentje, M.; Gerum, S.; et al. Influence of Institutional Experience and Technological Advances on Outcome of Stereotactic Body Radiation Therapy for Oligometastatic Lung Disease. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Jereczek-Fossa, B.A.; Kowalczyk, A.; D’Onofrio, A.; Catalano, G.; Garibaldi, C.; Boboc, G.; Vitolo, V.; Leonardi, M.C.; Cambria, R.; Orecchia, R. Three-dimensional conformal or stereotactic reirradiation of recurrent, metastatic or new primary tumors: Analysis of 108 patients. Strahlenther. Onkol. 2008, 184, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Wegner, R.E.; Abel, S.; Hasan, S.; Schumacher, L.Y.; Colonias, A. Stereotactic Body Radiotherapy (SBRT) for Oligometastatic Lung Nodules: A Single Institution Series. Front. Oncol. 2019, 9, 334. [Google Scholar] [CrossRef] [PubMed]
- Navarria, P.; Baldaccini, D.; Clerici, E.; Marini, B.; Cozzi, L.; Franceschini, D.; Bertuzzi, A.F.; Quagliuolo, V.; Torri, V.; Colombo, P.; et al. Stereotactic Body Radiation Therapy for Lung Metastases from Sarcoma in Oligometastatic Patients: A Phase 2 Study. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 762–770. [Google Scholar] [CrossRef]
- Jereczek-Fossa, B.A.; Bossi-Zanetti, I.; Mauro, R.; Beltramo, G.; Fariselli, L.; Bianchi, L.C.; Fodor, C.; Fossati, P.; Baroni, G.; Orecchia, R. CyberKnife robotic image-guided stereotactic radiotherapy for oligometastic cancer: A prospective evaluation of 95 patients/118 lesions. Strahlenther. Onkol. 2013, 189, 448–455. [Google Scholar] [CrossRef]
- Mikolasch, T.A.; Garthwaite, H.S.; Porter, J.C. Update in diagnosis and management of interstitial lung disease. Clin. Med. 2017, 17, 146–153. [Google Scholar] [CrossRef]
- Takemoto, S.; Shibamoto, Y.; Hashizume, C.; Miyakawa, A.; Murai, T.; Yanagi, T.; Sugie, C.; Nagai, A. Changes in pulmonary function and their correlation with dose–volume parameters in patients undergoing stereotactic body radiotherapy for lung cancer. J. Radiat. Res. 2021, 62, 338–345. [Google Scholar] [CrossRef]
- Berg, J.; Ramberg, C.; Haugstvedt, J.O.S.; Bengtson, M.-B.; Gabrielsen, A.-M.; Brustugun, O.T.; Halvorsen, A.R.; Helland, Å. Lung Function After Stereotactic Body Radiation Therapy for Early-Stage Non-Small Cell Lung Cancer, Changes and Predictive Markers. Front. Oncol. 2021, 11, 674731. [Google Scholar] [CrossRef]
- Miller, A.; Enright, P.L. PFT interpretive strategies: American Thoracic Society/ European Respiratory Society 2005 guideline gaps. Respir. Care 2012, 57, 127–133; discussion 133–135. [Google Scholar] [CrossRef]
- Volpe, S.; Mastroleo, F.; Krengli, M.; Jereczek-Fossa, B.A. Quo vadis Radiomics? Bibliometric analysis of 10-year Radiomics journey. Eur. Radiol. 2023, 33, 6736–6745. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Meyers, S.M.; Kisling, K.; Atwood, T.F.; Ray, X. A standardized workflow for respiratory-gated motion management decision-making. J. Appl. Clin. Med. Phys. 2022, 23, e13705. [Google Scholar] [CrossRef] [PubMed]
- Patient Contouring and Plan Evaluation in RayStation. RaySearch Laboratories. Available online: https://www.raysearchlabs.com/contouring-organs-at-risk_raystation/ (accessed on 17 May 2024).
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Pulmonary Function Test. Physiopedia. Available online: https://www.physio-pedia.com/Pulmonary_Function_Test (accessed on 22 May 2024).
- Volpe, S.; Gaeta, A.; Colombo, F.; Zaffaroni, M.; Mastroleo, F.; Vincini, M.G.; Pepa, M.; Isaksson, L.J.; Turturici, I.; Marvaso, G.; et al. Blood- and Imaging-Derived Biomarkers for Oncological Outcome Modelling in Oropharyngeal Cancer: Exploring the Low-Hanging Fruit. Cancers 2023, 15, 2022. [Google Scholar] [CrossRef]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: Epidemiology, molecular biology and clinical management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef]
- Sawayanagi, S.; Yamashita, H.; Nozawa, Y.; Takenaka, R.; Miki, Y.; Morishima, K.; Ueno, H.; Ohta, T.; Katano, A. Establishment of a Prediction Model for Overall Survival after Stereotactic Body Radiation Therapy for Primary Non-Small Cell Lung Cancer Using Radiomics Analysis. Cancers 2022, 14, 3859. [Google Scholar] [CrossRef]
- Ryan, S.M.; Fingerlin, T.E.; Mroz, M.; Barkes, B.; Hamzeh, N.; Maier, L.A.; Carlson, N.E. Radiomic measures from chest high-resolution computed tomography associated with lung function in sarcoidosis. Eur. Respir. J. 2019, 54, 1900371. [Google Scholar] [CrossRef]
- Yang, K.; Yang, Y.; Kang, Y.; Liang, Z.; Wang, F.; Li, Q.; Xu, J.; Tang, G.; Chen, R. The value of radiomic features in chronic obstructive pulmonary disease assessment: A prospective study. Clin. Radiol. 2022, 77, e466–e472. [Google Scholar] [CrossRef]
- Yun, J.; Cho, Y.H.; Lee, S.M.; Hwang, J.; Lee, J.S.; Oh, Y.-M.; Lee, S.-D.; Loh, L.-C.; Ong, C.-K.; Seo, J.B.; et al. Deep radiomics-based survival prediction in patients with chronic obstructive pulmonary disease. Sci. Rep. 2021, 11, 15144. [Google Scholar] [CrossRef]
- Lafata, K.J.; Zhou, Z.; Liu, J.-G.; Hong, J.; Kelsey, C.R.; Yin, F.-F. An Exploratory Radiomics Approach to Quantifying Pulmonary Function in CT Images. Sci. Rep. 2019, 9, 11509. [Google Scholar] [CrossRef]
- Zhou, T.-H.; Zhou, X.-X.; Ni, J.; Ma, Y.-Q.; Xu, F.-Y.; Fan, B.; Guan, Y.; Jiang, X.-A.; Lin, X.-Q.; Li, J.; et al. CT whole lung radiomic nomogram: A potential biomarker for lung function evaluation and identification of COPD. Mil. Med. Res. 2024, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Ponce-Bobadilla, A.V.; Schmitt, V.; Maier, C.S.; Mensing, S.; Stodtmann, S. Practical guide to SHAP analysis: Explaining supervised machine learning model predictions in drug development. Clin. Transl. Sci. 2024, 17, e70056. [Google Scholar] [CrossRef]
- Marvaso, G.; Isaksson, L.J.; Zaffaroni, M.; Vincini, M.G.; Summers, P.E.; Pepa, M.; Corrao, G.; Mazzola, G.C.; Rotondi, M.; Mastroleo, F.; et al. Can we predict pathology without surgery? Weighing the added value of multiparametric MRI and whole prostate radiomics in integrative machine learning models. Eur. Radiol. 2024, 34, 6241–6253. [Google Scholar] [CrossRef]
- Yue, X.; Cui, J.; Huang, S.; Liu, W.; Qi, J.; He, K.; Li, T. An interpretable radiomics-based machine learning model for predicting reverse left ventricular remodeling in STEMI patients using late gadolinium enhancement of myocardial scar. Eur. Radiol. 2025. [Google Scholar] [CrossRef]
- Zhan, Y.; Song, F.; Zhang, W.; Gong, T.; Zhao, S.; Lv, F. Prediction of benign and malignant pulmonary nodules using preoperative CT features: Using PNI-GARS as a predictor. Front. Immunol. 2024, 15, 1446511. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | p-Value 1 | |
|---|---|---|
| Baseline | Sex | >0.9 |
| Age at diagnosis | 0.2 | |
| Comorbidity | 0.01 | |
| CCI | 0.014 | |
| Arterial hypertension | 0.046 | |
| Cardiopathy | 0.075 | |
| Diabetes | 0.4 | |
| COPD | 0.003 | |
| Smoking habit | 0.05 | |
| Hb | 0.4 | |
| CRP | 0.9 | |
| Oxygen Therapy | >0.9 | |
| SpO2 basal | <0.001 | |
| PRIM/M+ | <0.001 | |
| M+ origin | 0.11 | |
| Histology | 0.01 | |
| Histological type | >0.9 | |
| Number of lesions | 0.3 | |
| Side of the lesions | 0.6 | |
| Central/peripheral lesion | 0.2 | |
| Shape | 0.13 | |
| Margin | 0.7 | |
| Diam max (mm) | 0.2 | |
| Systemic concomitant therapy | 0.7 | |
| Type of systemic therapy | >0.9 | |
| RE-RT | 0.7 | |
| Number of fractions | 0.004 | |
| Dose/fraction | 0.008 | |
| Total prescribed dose | 0.1 | |
| Baseline spirometry data | VC | 0.2 |
| FEV1 | 0.009 | |
| PEF | 0.057 | |
| VC% | <0.001 | |
| FEV1% | <0.001 | |
| Post-treatment spirometry data | VC | >0.9 |
| FEV1 | 0.2 | |
| PEF | 0.9 | |
| VC% | 0.035 | |
| FEV1% | <0.001 | |
| Follow-up | Status | 0.2 |
| Radiomic Features | Coefficient | |
|---|---|---|
| Phase 0 | wavelet-HHH GLCM Correlation | −39.20 |
| wavelet-LLL GLDM Low Gray Level Emphasis | 57.85 | |
| Phase 50 | wavelet-HHH GLCM Correlation | −38.56 |
| wavelet-LLL GLDM Low Gray Level Emphasis | 54.49 | |
| ∆ Phase | Gradient GLSZM Size Zone Non Uniformity Normalized | 0.346 |
| log-sigma-2-0-mm-3D First Order Maximum | 0.00023 | |
| wavelet-HLL First Order Maximum | 2.35 | |
| wavelet-HHL First Order Median | 0.14 | |
| wavelet-HHH GLCM Correlation | 1.21 | |
| wavelet-HHH GLCM Imc1 | −2.61 |
| Repeated Cross-Validation of AUC (Median, IQR) | ||
|---|---|---|
| Radiomic Models | Model 1 | 0.69 (0.67–0.71) |
| Model 2 | 0.69 (0.67–0.71) | |
| Model 3 | 0.72 (0.71–0.74) | |
| Clinical- Radiomic Models | Model 1 | 0.71 (0.69–0.73) |
| Model 2 | 0.71 (0.69–0.73) | |
| Model 3 | 0.74 (0.71–0.76) | |
| Clinical Model | 0.65 (0.63–0.67) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porazzi, A.; Zaffaroni, M.; Pierini, V.E.; Vincini, M.G.; Gaeta, A.; Raimondi, S.; Berton, L.; Isaksson, L.J.; Mastroleo, F.; Gandini, S.; et al. CT-Based Radiomics Enhance Respiratory Function Analysis for Lung SBRT. Bioengineering 2025, 12, 800. https://doi.org/10.3390/bioengineering12080800
Porazzi A, Zaffaroni M, Pierini VE, Vincini MG, Gaeta A, Raimondi S, Berton L, Isaksson LJ, Mastroleo F, Gandini S, et al. CT-Based Radiomics Enhance Respiratory Function Analysis for Lung SBRT. Bioengineering. 2025; 12(8):800. https://doi.org/10.3390/bioengineering12080800
Chicago/Turabian StylePorazzi, Alice, Mattia Zaffaroni, Vanessa Eleonora Pierini, Maria Giulia Vincini, Aurora Gaeta, Sara Raimondi, Lucrezia Berton, Lars Johannes Isaksson, Federico Mastroleo, Sara Gandini, and et al. 2025. "CT-Based Radiomics Enhance Respiratory Function Analysis for Lung SBRT" Bioengineering 12, no. 8: 800. https://doi.org/10.3390/bioengineering12080800
APA StylePorazzi, A., Zaffaroni, M., Pierini, V. E., Vincini, M. G., Gaeta, A., Raimondi, S., Berton, L., Isaksson, L. J., Mastroleo, F., Gandini, S., Casiraghi, M., Piperno, G., Spaggiari, L., Guarize, J., Donghi, S. M., Kuncman, Ł., Orecchia, R., Volpe, S., & Jereczek-Fossa, B. A. (2025). CT-Based Radiomics Enhance Respiratory Function Analysis for Lung SBRT. Bioengineering, 12(8), 800. https://doi.org/10.3390/bioengineering12080800