
The Use of Head-Mounted Display Systems for Upper Limb Kinematic Analysis in Post-Stroke Patients: A Perspective Review on Benefits, Challenges and Other Solutions

 , ,
, , 
Abstract
1. Introduction
Virtual Reality Head-Mounted Display (HMD-VR) Platforms
2. Kinematics of Upper Limb Movements in Post-Stroke Patients
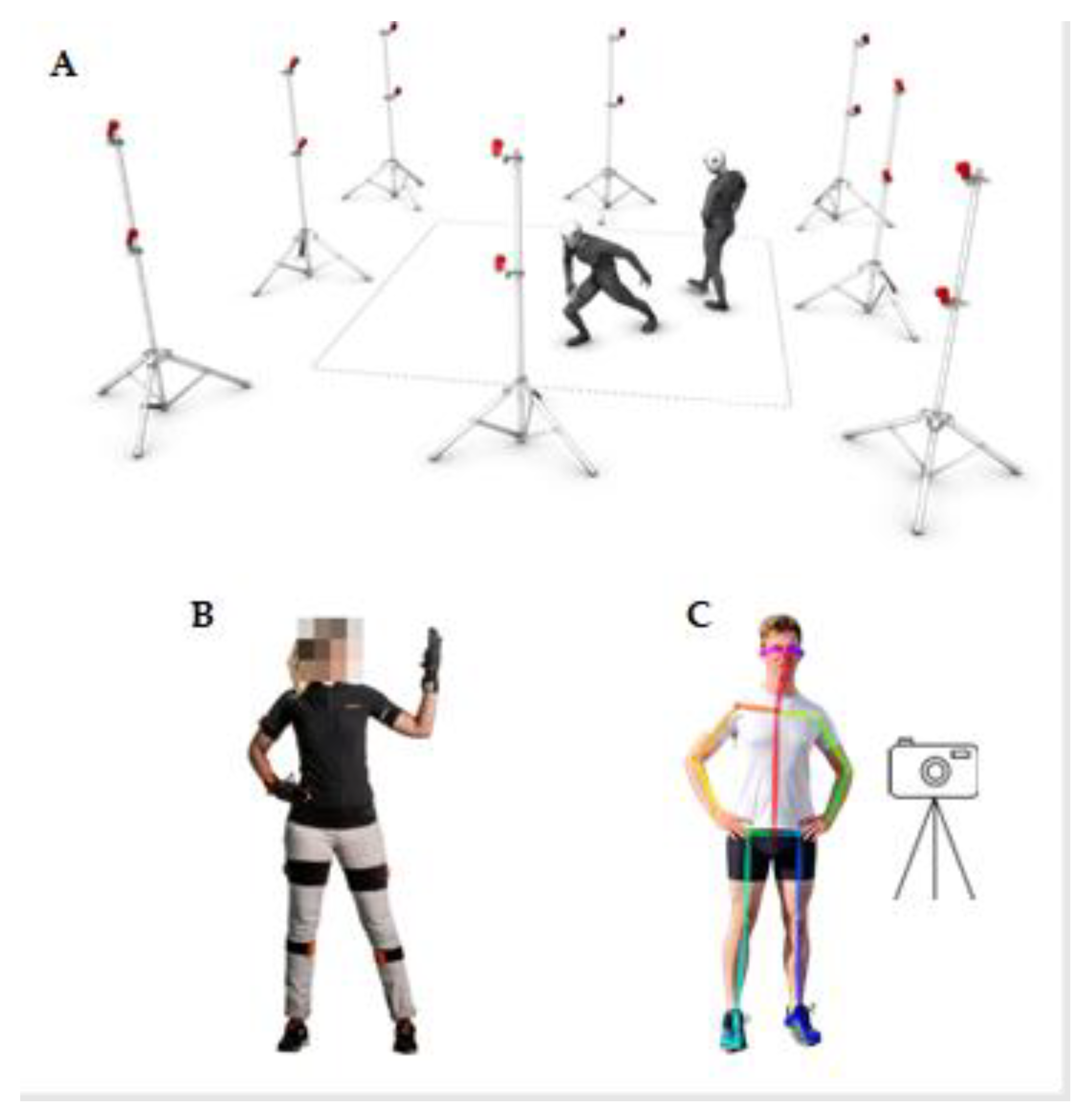
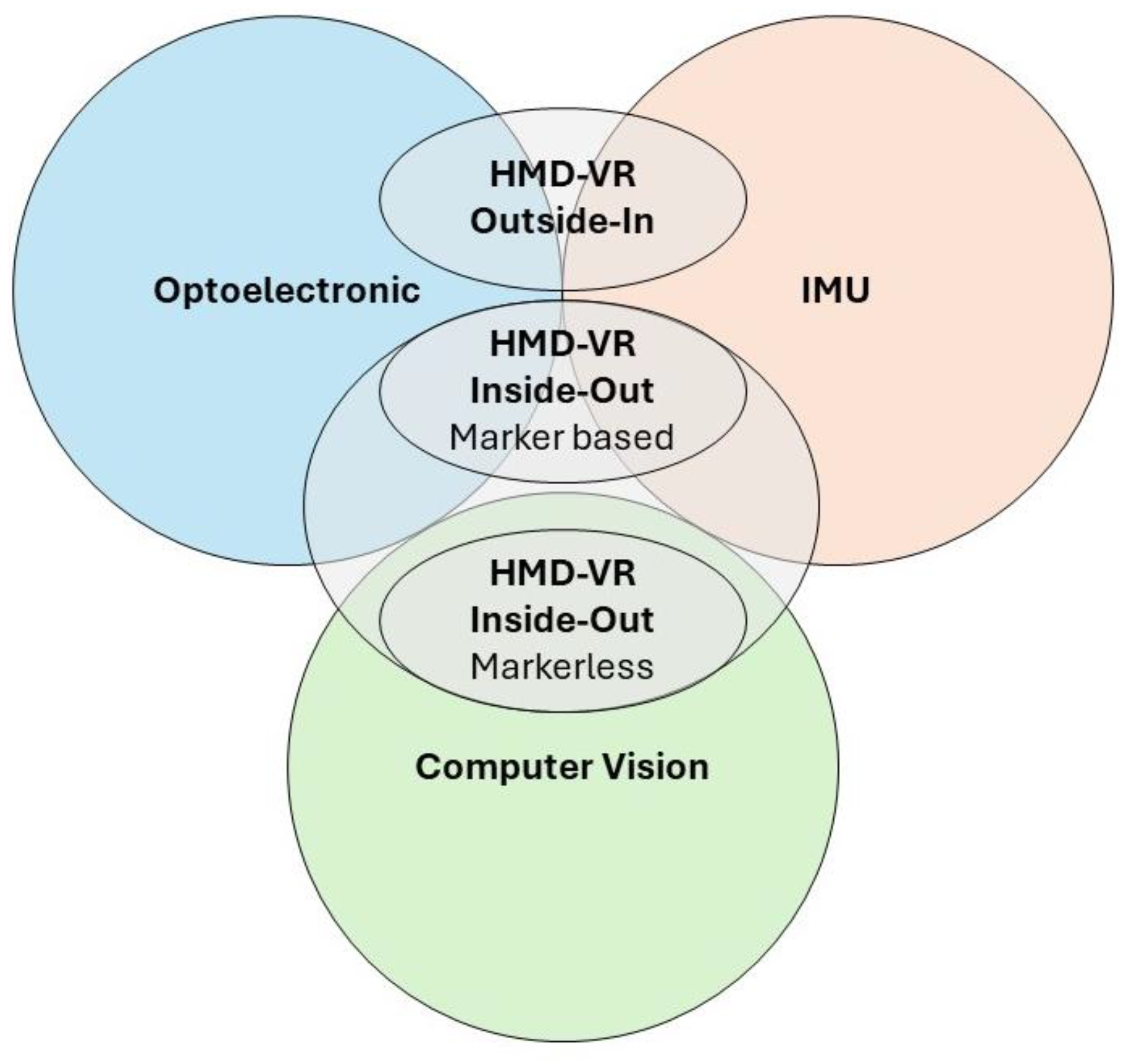
3. Technologies for Motion Capture: Optoelectronic, IMUs, and Vision-Based Motion Tracking and Other Solutions
Other Technologies for Motion Capture: Focus on Collaborative Robots
4. Benefits and Challenges of Virtual Reality Head-Mounted Display Platforms
5. Discussion
5.1. Benefits and Challenges of HMD-VR in a Neurorehabilitation Context
5.2. Reliability, Technical Features, and Limitations of HMD-VR
5.3. Clinical Perspectives and Future Directions
- A comparison between the different types and brands of HMD-VR platforms is still missing, intended as measurement and rehabilitation tools. In addition, among the studies that we have included in this review, there is no homogeneity in results regarding accuracy and precision analysis.
- According to the authors (Table 4), these systems are suitably accurate and reliable to be used as rehabilitation tools and MoCap systems.
- The selection of one device over another depends on its intended use and on the severity degree of the disease. Therefore, clinicians must consider the reliability and effectiveness of the instrument.
- It is noteworthy that VR is not the only technology capable of providing an objective and quantitative assessment of movement as well as delivering rehabilitation treatment. In fact, robotic devices can be tailored to meet the patient’s needs, offering both precise movement evaluation and intensive, repetitive, and task-oriented treatment options.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anwer, S.; Waris, A.; Gilani, S.O.; Iqbal, J.; Shaikh, N.; Pujari, A.N.; Niazi, I.K. Rehabilitation of Upper Limb Motor Impairment in Stroke: A Narrative Review on the Prevalence, Risk Factors, and Economic Statistics of Stroke and State of the Art Therapies. Healthcare 2022, 10, 190. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.J.X.; Werring, D.J. Stroke: Causes and Clinical Features. Medicine 2020, 48, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Bhagubai, M.M.C.; Nies, S.H.G.; Held, J.P.O.; Veltink, P.H.; Buurke, J.H.; Luft, A.R. Characterization of Stroke-Related Upper Limb Motor Impairments across Various Upper Limb Activities by Use of Kinematic Core Set Measures. J. NeuroEngineering Rehabil. 2022, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, M.; Calabrò, R.S. Robot-Aided Motion Analysis in Neurorehabilitation: Benefits and Challenges. Diagnostics 2023, 13, 3561. [Google Scholar] [CrossRef] [PubMed]
- Chiriatti, G.; Bottiglione, A.; Palmieri, G. Manipulability Optimization of a Rehabilitative Collaborative Robotic System. Machines 2022, 10, 452. [Google Scholar] [CrossRef]
- Pan, B.; Huang, Z.; Jin, T.; Wu, J.; Zhang, Z.; Shen, Y. Motor Function Assessment of Upper Limb in Stroke Patients. J. Healthc. Eng. 2021, 2021, 6621950. [Google Scholar] [CrossRef] [PubMed]
- Gu, C.; Lin, W.; He, X.; Zhang, L.; Zhang, M. IMU-Based Motion Capture System for Rehabilitation Applications: A Systematic Review. Biomim. Intell. Robot. 2023, 3, 100097. [Google Scholar] [CrossRef]
- Topley, M.; Richards, J.G. A Comparison of Currently Available Optoelectronic Motion Capture Systems. J. Biomech. 2020, 106, 109820. [Google Scholar] [CrossRef]
- van Schaik, J.E.; Dominici, N. Chapter 5—Motion Tracking in Developmental Research: Methods, Considerations, and Applications. In Progress in Brain Research; Hunnius, S., Meyer, M., Eds.; New Perspectives on Early Social-cognitive Development; Elsevier: Amsterdam, The Netherlands, 2020; Volume 254, pp. 89–111. [Google Scholar]
- Zago, M.; Luzzago, M.; Marangoni, T.; De Cecco, M.; Tarabini, M.; Galli, M. 3D Tracking of Human Motion Using Visual Skeletonization and Stereoscopic Vision. Front. Bioeng. Biotechnol. 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Rubio, Á.; Alguacil-Diego, I.M.; Mallo-López, A.; Cuesta-Gómez, A. Use of the Leap Motion Controller® System in the Rehabilitation of the Upper Limb in Stroke. A Systematic Review. J. Stroke Cerebrovasc. Dis. 2022, 31, 106174. [Google Scholar] [CrossRef]
- Potter, M.V.; Cain, S.M.; Ojeda, L.V.; Gurchiek, R.D.; McGinnis, R.S.; Perkins, N.C. Evaluation of Error-State Kalman Filter Method for Estimating Human Lower-Limb Kinematics during Various Walking Gaits. Sensors 2022, 22, 8398. [Google Scholar] [CrossRef] [PubMed]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods Towards Developing a Markerless System. Sports Med. Open 2018, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, J.K.; Gillies, M.; Pan, X. A Comparison of the Effects of Haptic and Visual Feedback on Presence in Virtual Reality. Int. J. Hum. Comput. Stud. 2022, 157, 102717. [Google Scholar] [CrossRef]
- Lindeman, R.W.; Page, R.; Yanagida, Y.; Sibert, J.L. Towards Full-Body Haptic Feedback: The Design and Deployment of a Spatialized Vibrotactile Feedback System. In Proceedings of the ACM Symposium on Virtual Reality Software and Technology, Osaka, Japan, 8–10 December 2021. [Google Scholar]
- Pacchierotti, C.; Sinclair, S.; Solazzi, M.; Frisoli, A.; Hayward, V.; Prattichizzo, D. Wearable Haptic Systems for the Fingertip and the Hand: Taxonomy, Review, and Perspectives. IEEE Trans. Haptics 2017, 10, 580–600. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Chen, J.; Ye, G.; Dong, S.; Gao, Z.; Zhou, Y. Soft Robotic Glove with Sensing and Force Feedback for Rehabilitation in Virtual Reality. Biomimetics 2023, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Saldana, D.; Neureither, M.; Schmiesing, A.; Jahng, E.; Kysh, L.; Roll, S.C.; Liew, S.-L. Applications of Head-Mounted Displays for Virtual Reality in Adult Physical Rehabilitation: A Scoping Review. Am. J. Occup. Ther. 2020, 74, 7405205060p1–7405205060p15. [Google Scholar] [CrossRef] [PubMed]
- Trinidad-Fernández, M.; Bossavit, B.; Salgado-Fernández, J.; Abbate-Chica, S.; Fernández-Leiva, A.J.; Cuesta-Vargas, A.I. Head-Mounted Display for Clinical Evaluation of Neck Movement Validation with Meta Quest 2. Sensors 2023, 23, 3077. [Google Scholar] [CrossRef] [PubMed]
- Fregna, G.; Paoluzzi, C.; Baroni, A.; Cano-de-la-Cuerda, R.; Casile, A.; Straudi, S. Head-Mounted Displays for Upper Limb Stroke Rehabilitation: A Scoping Review. J. Clin. Med. 2023, 12, 7444. [Google Scholar] [CrossRef] [PubMed]
- Kiper, P.; Godart, N.; Cavalier, M.; Berard, C.; Cieślik, B.; Federico, S.; Kiper, A.; Pellicciari, L.; Meroni, R. Effects of Immersive Virtual Reality on Upper-Extremity Stroke Rehabilitation: A Systematic Review with Meta-Analysis. J. Clin. Med. 2024, 13, 146. [Google Scholar] [CrossRef]
- Amini Gougeh, R.; Falk, T.H. Head-Mounted Display-Based Virtual Reality and Physiological Computing for Stroke Rehabilitation: A Systematic Review. Front. Virtual Real. 2022, 3. [Google Scholar] [CrossRef]
- Marek, K.; Zubrycki, I.; Miller, E. Immersion Therapy with Head-Mounted Display for Rehabilitation of the Upper Limb after Stroke—Review. Sensors 2022, 22, 9962. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Van Wegen, E.; Burridge, J.H.; Winstein, C.J.; van Dokkum, L.; Alt Murphy, M.; Levin, M.F.; Krakauer, J.W. Standardized Measurement of Quality of Upper Limb Movement after Stroke: Consensus-Based Core Recommendations from the Second Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke 2019, 14, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Duprey, S.; Naaim, A.; Moissenet, F.; Begon, M.; Chèze, L. Kinematic Models of the Upper Limb Joints for Multibody Kinematics Optimisation: An Overview. J. Biomech. 2017, 62, 87–94. [Google Scholar] [CrossRef] [PubMed]
- De Baets, L.; Vanbrabant, S.; Dierickx, C.; van der Straaten, R.; Timmermans, A. Assessment of Scapulothoracic, Glenohumeral, and Elbow Motion in Adhesive Capsulitis by Means of Inertial Sensor Technology: A Within-Session, Intra-Operator and Inter-Operator Reliability and Agreement Study. Sensors 2020, 20, 876. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Bhagubai, M.M.C.; Wolterink, G.; Held, J.P.O.; Luft, A.R.; Veltink, P.H. Assessment of Upper Limb Movement Impairments after Stroke Using Wearable Inertial Sensing. Sensors 2020, 20, 4770. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Valtin, M.; Salchow, C.; Seel, T.; Laidig, D.; Schauer, T. Modular Finger and Hand Motion Capturing System Based on Inertial and Magnetic Sensors. Curr. Dir. Biomed. Eng. 2017, 3, 19–23. [Google Scholar] [CrossRef]
- Mesquita, I.A.; da Fonseca, P.F.P.; Pinheiro, A.R.V.; Velhote Correia, M.F.P.; da Silva, C.I.C. Methodological Considerations for Kinematic Analysis of Upper Limbs in Healthy and Poststroke Adults Part II: A Systematic Review of Motion Capture Systems and Kinematic Metrics. Top. Stroke Rehabil. 2019, 26, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, J.; Hayward, K.S.; Dancause, N.; Lannin, N.A.; Ward, N.S.; Nudo, R.J.; Farrin, A.; Churilov, L.; Boyd, L.A.; Jones, T.A.; et al. A Stroke Recovery Trial Development Framework: Consensus-Based Core Recommendations from the Second Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke 2019, 14, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Prange-Lasonder, G.B.; Alt Murphy, M.; Lamers, I.; Hughes, A.-M.; Buurke, J.H.; Feys, P.; Keller, T.; Klamroth-Marganska, V.; Tarkka, I.M.; Timmermans, A.; et al. European Evidence-Based Recommendations for Clinical Assessment of Upper Limb in Neurorehabilitation (CAULIN): Data Synthesis from Systematic Reviews, Clinical Practice Guidelines and Expert Consensus. J. NeuroEngineering Rehabil. 2021, 18, 162. [Google Scholar] [CrossRef] [PubMed]
- Johansson, G.M.; Grip, H.; Levin, M.F.; Häger, C.K. The Added Value of Kinematic Evaluation of the Timed Finger-to-Nose Test in Persons Post-Stroke. J. NeuroEngineering Rehabil. 2017, 14, 11. [Google Scholar] [CrossRef] [PubMed]
- van der Vliet, R.; Selles, R.W.; Andrinopoulou, E.-R.; Nijland, R.; Ribbers, G.M.; Frens, M.A.; Meskers, C.; Kwakkel, G. Predicting Upper Limb Motor Impairment Recovery after Stroke: A Mixture Model. Ann. Neurol. 2020, 87, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Liao, O.; Jiang, S.; Li, J.; Ma, X. Kinematic Analysis in Post-Stroke Patients with Moderate to Severe Upper Limb Paresis and Non-Disabled Controls. Clin. Biomech. 2024, 113, 106206. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Park, D.; Rha, D.-W.; Nam, H.S.; Jo, Y.J.; Kim, D.Y. Kinematic Analysis of Movement Patterns during a Reach-and-Grasp Task in Stroke Patients. Front. Neurol. 2023, 14, 1225425. [Google Scholar] [CrossRef] [PubMed]
- Guzik-Kopyto, A.; Nowakowska-Lipiec, K.; Krysiak, M.; Jochymczyk-Woźniak, K.; Jurkojć, J.; Wodarski, P.; Gzik, M.; Michnik, R. Selection of Kinematic and Temporal Input Parameters to Define a Novel Upper Body Index Indicator for the Evaluation of Upper Limb Pathology. Appl. Sci. 2022, 12, 11634. [Google Scholar] [CrossRef]
- Aprile, I.; Rabuffetti, M.; Padua, L.; Di Sipio, E.; Simbolotti, C.; Ferrarin, M. Kinematic Analysis of the Upper Limb Motor Strategies in Stroke Patients as a Tool towards Advanced Neurorehabilitation Strategies: A Preliminary Study. Biomed. Res. Int. 2014, 2014, 636123. [Google Scholar] [CrossRef] [PubMed]
- Flex 13-In Depth. Available online: http://optitrack.com/cameras/flex-13/index.html (accessed on 21 May 2024).
- MVN Awinda|Movella.Com. Available online: https://www.movella.com/products/motion-capture/xsens-mvn-awinda (accessed on 28 April 2024).
- Wade, L.; Needham, L.; McGuigan, P.; Bilzon, J. Applications and Limitations of Current Markerless Motion Capture Methods for Clinical Gait Biomechanics. PeerJ 2022, 10, e12995. [Google Scholar] [CrossRef] [PubMed]
- Boser, Q.A.; Valevicius, A.M.; Lavoie, E.B.; Chapman, C.S.; Pilarski, P.M.; Hebert, J.S.; Vette, A.H. Cluster-Based Upper Body Marker Models for Three-Dimensional Kinematic Analysis: Comparison with an Anatomical Model and Reliability Analysis. J. Biomech. 2018, 72, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Bodily, K.D.; Daniel, T.A.; Sturz, B.R. The Roles of Beaconing and Dead Reckoning in Human Virtual Navigation. Learn. Motiv. 2012, 43, 14–23. [Google Scholar] [CrossRef]
- Ponsiglione, A.M.; Ricciardi, C.; Amato, F.; Cesarelli, M.; Cesarelli, G.; D’Addio, G. Statistical Analysis and Kinematic Assessment of Upper Limb Reaching Task in Parkinson’s Disease. Sensors 2022, 22, 1708. [Google Scholar] [CrossRef] [PubMed]
- Held, J.P.O.; Klaassen, B.; Eenhoorn, A.; van Beijnum, B.-J.F.; Buurke, J.H.; Veltink, P.H.; Luft, A.R. Inertial Sensor Measurements of Upper-Limb Kinematics in Stroke Patients in Clinic and Home Environment. Front. Bioeng. Biotechnol. 2018, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Fischer, E.; Tunca, C.; Brahms, C.M.; Ersoy, C.; Granacher, U.; Arnrich, B. How We Found Our IMU: Guidelines to IMU Selection and a Comparison of Seven IMUs for Pervasive Healthcare Applications. Sensors 2020, 20, 4090. [Google Scholar] [CrossRef] [PubMed]
- Merlau, B.; Cormier, C.; Alaux, A.; Morin, M.; Montané, E.; Amarantini, D.; Gasq, D. Assessing Spatiotemporal and Quality Alterations in Paretic Upper Limb Movements after Stroke in Routine Care: Proposal and Validation of a Protocol Using IMUs versus MoCap. Sensors 2023, 23, 7427. [Google Scholar] [CrossRef]
- Unger, T.; de Sousa Ribeiro, R.; Mokni, M.; Weikert, T.; Pohl, J.; Schwarz, A.; Held, J.P.O.; Sauerzopf, L.; Kühnis, B.; Gavagnin, E.; et al. Upper Limb Movement Quality Measures: Comparing IMUs and Optical Motion Capture in Stroke Patients Performing a Drinking Task. Front. Digit. Health 2024, 6, 1359776. [Google Scholar] [CrossRef] [PubMed]
- Nie, J.Z.; Nie, J.W.; Hung, N.-T.; Cotton, R.J.; Slutzky, M.W. Portable, Open-Source Solutions for Estimating Wrist Position during Reaching in People with Stroke. Sci. Rep. 2021, 11, 22491. [Google Scholar] [CrossRef] [PubMed]
- GitHub-Google-Ai-Edge/Mediapipe: Cross-Platform, Customizable ML Solutions for Live and Streaming Media. Available online: https://github.com/google-ai-edge/mediapipe (accessed on 21 May 2024).
- MoveNet: Modello di Rilevamento Della Posa Ultra Veloce e Preciso. TensorFlow Hub. Available online: https://www.tensorflow.org/hub/tutorials/movenet?hl=it (accessed on 10 April 2024).
- CMU-Perceptual-Computing-Lab/Openpose: OpenPose: Real-Time Multi-Person Keypoint Detection Library for Body, Face, Hands, and Foot Estimation. Available online: https://github.com/CMU-Perceptual-Computing-Lab/openpose (accessed on 10 April 2024).
- Ceseracciu, E.; Sawacha, Z.; Cobelli, C. Comparison of Markerless and Marker-Based Motion Capture Technologies through Simultaneous Data Collection during Gait: Proof of Concept. PLoS ONE 2014, 9, e87640. [Google Scholar] [CrossRef]
- Faity, G.; Mottet, D.; Froger, J. Validity and Reliability of Kinect v2 for Quantifying Upper Body Kinematics during Seated Reaching. Sensors 2022, 22, 2735. [Google Scholar] [CrossRef] [PubMed]
- Galeoto, G.; Berardi, A.; Mangone, M.; Tufo, L.; Silvani, M.; González-Bernal, J.; Seco-Calvo, J. Assessment Capacity of the Armeo® Power: Cross-Sectional Study. Technologies 2023, 11, 125. [Google Scholar] [CrossRef]
- Merlo, A.; Longhi, M.; Giannotti, E.; Prati, P.; Giacobbi, M.; Ruscelli, E.; Mancini, A.; Ottaviani, M.; Montanari, L.; Mazzoli, D. Upper Limb Evaluation with Robotic Exoskeleton. Normative Values for Indices of Accuracy, Speed and Smoothness. NeuroRehabilitation 2013, 33, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Longhi, M.; Merlo, A.; Prati, P.; Giacobbi, M.; Mazzoli, D. Instrumental Indices for Upper Limb Function Assessment in Stroke Patients: A Validation Study. J. NeuroEng. Rehabil. 2016, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Schweighofer, N.; Choi, Y.; Winstein, C.; Gordon, J. Task-Oriented Rehabilitation Robotics. Am. J. Phys. Med. Rehabil. 2012, 91, S270–S279. [Google Scholar] [CrossRef] [PubMed]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A Survey on Robotic Devices for Upper Limb Rehabilitation. J. NeuroEngineering Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Wagner, T.H.; Lo, A.C.; Peduzzi, P.; Bravata, D.M.; Huang, G.D.; Krebs, H.I.; Ringer, R.J.; Federman, D.G.; Richards, L.G.; Haselkorn, J.K.; et al. An Economic Analysis of Robot-Assisted Therapy for Long-Term Upper-Limb Impairment after Stroke. Stroke 2011, 42, 2630–2632. [Google Scholar] [CrossRef]
- Cherubini, A.; Navarro-Alarcon, D. Sensor-Based Control for Collaborative Robots: Fundamentals, Challenges, and Opportunities. Front. Neurorobot. 2021, 14, 576846. [Google Scholar] [CrossRef] [PubMed]
- Kyrkjebø, E.; Johan Laastad, M.; Stavdahl, Ø. Feasibility of the UR5 Industrial Robot for Robotic Rehabilitation of the Upper Limbs After Stroke. In Proceedings of the 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Madrid, Spain, 1–5 October 2018; pp. 1–6. [Google Scholar]
- Reinkensmeyer, D.J.; Wolbrecht, E.T.; Chan, V.; Chou, C.; Cramer, S.C.; Bobrow, J.E. Comparison of 3D, Assist-as-Needed Robotic Arm/Hand Movement Training Provided with Pneu-WREX to Conventional Table Top Therapy Following Chronic Stroke. Am. J. Phys. Med. Rehabil. 2012, 91, S232–S241. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.C.; Menezes, P.; Restivo, M.T. An Augmented Reality Interface to Control a Collaborative Robot in Rehab: A Preliminary Usability Evaluation. Front. Digit. Health 2023, 5, 1078511. [Google Scholar] [CrossRef] [PubMed]
- Caserman, P.; Garcia-Agundez, A.; Konrad, R.; Göbel, S.; Steinmetz, R. Real-Time Body Tracking in Virtual Reality Using a Vive Tracker. Virtual Real. 2019, 23, 155–168. [Google Scholar] [CrossRef]
- Pandita, S.; Stevenson Won, A. Chapter 7—Clinical Applications of Virtual Reality in Patient-Centered Care. In Technology and Health; Kim, J., Song, H., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 129–148. ISBN 978-0-12-816958-2. [Google Scholar]
- Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients. Sensors 2022, 22, 3302. [Google Scholar] [CrossRef] [PubMed]
- Varela-Aldás, J.; Palacios-Navarro, G.; Amariglio, R.; García-Magariño, I. Head-Mounted Display-Based Application for Cognitive Training. Sensors 2020, 20, 6552. [Google Scholar] [CrossRef] [PubMed]
- Memmesheimer, V.M.; Ebert, A. Scalable Extended Reality: A Future Research Agenda. Big Data Cogn. Comput. 2022, 6, 12. [Google Scholar] [CrossRef]
- Rojo, A.; Cortina, J.; Sánchez, C.; Urendes, E.; García-Carmona, R.; Raya, R. Accuracy Study of the Oculus Touch v2 versus Inertial Sensor for a Single-Axis Rotation Simulating the Elbow’s Range of Motion. Virtual Real. 2022, 26, 1651–1662. [Google Scholar] [CrossRef]
- Casile, A.; Fregna, G.; Boarini, V.; Paoluzzi, C.; Manfredini, F.; Lamberti, N.; Baroni, A.; Straudi, S. Quantitative Comparison of Hand Kinematics Measured with a Markerless Commercial Head-Mounted Display and a Marker-Based Motion Capture System in Stroke Survivors. Sensors 2023, 23, 7906. [Google Scholar] [CrossRef] [PubMed]
- Unity Real-Time Development Platform|3D, 2D, VR & AR Engine. Available online: https://unity.com/ (accessed on 20 May 2024).
- Downloads-Meta XR Core SDK (UPM). Available online: https://developer.oculus.com/downloads/package/meta-xr-core-sdk/ (accessed on 20 May 2024).
- Monica, R.; Aleotti, J. Evaluation of the Oculus Rift S Tracking System in Room Scale Virtual Reality. Virtual Real. 2022, 26, 1335–1345. [Google Scholar] [CrossRef]
- Pereira, D.; Oliveira, V.; Vilaça, J.L.; Carvalho, V.; Duque, D. Measuring the Precision of the Oculus Quest 2′s Handheld Controllers. Actuators 2023, 12, 257. [Google Scholar] [CrossRef]
- Kharoub, H.; Lataifeh, M.; Ahmed, N. 3D User Interface Design and Usability for Immersive VR. Appl. Sci. 2019, 9, 4861. [Google Scholar] [CrossRef]
- SteamVR su Steam. Available online: https://store.steampowered.com/app/250820/SteamVR/ (accessed on 20 May 2024).
- Mirzaei, B.; Nezamabadi-pour, H.; Raoof, A.; Derakhshani, R. Small Object Detection and Tracking: A Comprehensive Review. Sensors 2023, 23, 6887. [Google Scholar] [CrossRef] [PubMed]
- Fregna, G.; Schincaglia, N.; Baroni, A.; Straudi, S.; Casile, A. A Novel Immersive Virtual Reality Environment for the Motor Rehabilitation of Stroke Patients: A Feasibility Study. Front. Robot. AI 2022, 9, 906424. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, A.; Mannocchi, I.; Sassi, M.S.H.; Carli, M.; De Luca, G.; Longo, U.G.; Denaro, V.; Schena, E. Virtual Reality for Shoulder Rehabilitation: Accuracy Evaluation of Oculus Quest 2. Sensors 2022, 22, 5511. [Google Scholar] [CrossRef] [PubMed]
- Jost, T.A.; Nelson, B.; Rylander, J. Quantitative Analysis of the Oculus Rift S in Controlled Movement. Disabil. Rehabil. Assist. Technol. 2021, 16, 632–636. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Müller-Eising, C.; Diliberti, M.L.; Manuli, A.; Parrinello, F.; Rao, G.; Barone, V.; Civello, T. Who Will Pay for Robotic Rehabilitation? The Growing Need for a Cost-Effectiveness Analysis. Innov. Clin. Neurosci. 2020, 17, 14–16. [Google Scholar] [PubMed]
- Arias, P.; Robles-García, V.; Sanmartín, G.; Flores, J.; Cudeiro, J. Virtual Reality as a Tool for Evaluation of Repetitive Rhythmic Movements in the Elderly and Parkinson’s Disease Patients. PLoS ONE 2012, 7, e30021. [Google Scholar] [CrossRef] [PubMed]
- Aderinto, N.; Olatunji, G.; Abdulbasit, M.O.; Edun, M.; Aboderin, G.; Egbunu, E. Exploring the Efficacy of Virtual Reality-Based Rehabilitation in Stroke: A Narrative Review of Current Evidence. Ann. Med. 2023, 55, 2285907. [Google Scholar] [CrossRef] [PubMed]
- Demeco, A.; Zola, L.; Frizziero, A.; Martini, C.; Palumbo, A.; Foresti, R.; Buccino, G.; Costantino, C. Immersive Virtual Reality in Post-Stroke Rehabilitation: A Systematic Review. Sensors 2023, 23, 1712. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Liu, F.; Lin, S.; Yu, L.; Lin, R. Effects of Virtual Reality Rehabilitation Training on Cognitive Function and Activities of Daily Living of Patients With Poststroke Cognitive Impairment: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2022, 103, 1422–1435. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, R.; Fortini, A.; Aghilarre, F.; Gentili, F.; Morone, G.; Antonucci, G.; Vetrano, M.; Tieri, G.; Iosa, M. Virtual Art Therapy: Application of Michelangelo Effect to Neurorehabilitation of Patients with Stroke. J. Clin. Med. 2023, 12, 2590. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.F.V.; Vega, M.F.M.; Cardona, J.E.M.; Lopez, D.; Quiñones, L.; Gallo, O.A.H.; Lopez, J.F. Design of Virtual Reality Exergames for Upper Limb Stroke Rehabilitation Following Iterative Design Methods: Usability Study. JMIR Serious Games 2024, 12, e48900. [Google Scholar] [CrossRef] [PubMed]
- Pilacinski, A.; Pinto, A.; Oliveira, S.; Araújo, E.; Carvalho, C.; Silva, P.A.; Matias, R.; Menezes, P.; Sousa, S. The Robot Eyes Don’t Have It. The Presence of Eyes on Collaborative Robots Yields Marginally Higher User Trust but Lower Performance. Heliyon 2023, 9, e18164. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, G. Full-Immersion Virtual Reality: Adverse Effects Related to Static Balance. Neurosci. Lett. 2020, 733, 134974. [Google Scholar] [CrossRef] [PubMed]
- De Luca, R.; Manuli, A.; De Domenico, C.; Lo Voi, E.; Buda, A.; Maresca, G.; Bramanti, A.; Calabrò, R.S. Improving Neuropsychiatric Symptoms Following Stroke Using Virtual Reality. Medicine 2019, 98, e15236. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Bonanno, M.; Torregrossa, W.; Cacciante, L.; Celesti, A.; Rifici, C.; Tonin, P.; De Luca, R.; Quartarone, A. Benefits of Telerehabilitation for Patients With Severe Acquired Brain Injury: Promising Results From a Multicenter Randomized Controlled Trial Using Nonimmersive Virtual Reality. J. Med. Internet Res. 2023, 25, e45458. [Google Scholar] [CrossRef] [PubMed]
- Choukou, M.-A.; He, E.; Moslenko, K. Feasibility of a Virtual-Reality-Enabled At-Home Telerehabilitation Program for Stroke Survivors: A Case Study. J. Pers. Med. 2023, 13, 1230. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Kinematic Features | Description |
|---|---|
| Path length ratio | Path length ratio (PLR) in upper limb kinematic analysis is a quantitative measure used to assess movement efficiency. It is calculated by dividing the actual path length travelled by a specific point or segment of the upper limb during a movement task by the shortest possible path length for the same movement. Higher PLR indicates less efficient movement patterns. |
| Joint excursion | Joint excursion consists of the angular RoM experienced by a specific joint during a movement task. It is typically measured in degrees or radians and provides insight into the flexibility, mobility, and coordination of the joint during the execution of a motor task. |
| Smoothness | Smoothness in upper limb kinematic analysis is a quantitative measure used to assess movement quality during reaching. There are several methods to measure movement smoothness. One of these is calculated as the number of peaks detected in the velocity profile. |
| Movement time | Movement time refers to the duration taken to complete a specific movement task. It is a crucial measure in assessing motor control, coordination, and efficiency of upper limb movements. |
| Movement velocity | Movement velocity is calculated by dividing the displacement of the point or segment by the time taken to complete the movement. It provides information about the speed or pace of movement execution, and it can be used to understand motor performance, coordination dynamics, and task difficulty. |
| Peak velocity | Peak velocity refers to the maximum instantaneous velocity achieved by a specific point or segment of the upper limb during a movement task. It represents the highest speed attained during the movement. |
| Number of velocity peaks | The number of velocity peaks refers to the count of distinct instances where the velocity of a specific point or segment of the upper limb reaches a local maximum during a movement task. Each velocity peak corresponds to a moment of rapid acceleration or deceleration within the movement profile. |
| MoCap System | Portability | Markerless | Easy-to-Use | Tele-Monitoring | Untethered | Rehabilitation | Cost |
|---|---|---|---|---|---|---|---|
| Optoelectronic | No | No | No | No | No | No | High |
| IMU | Yes | No | Yes | Yes | No | No | Medium |
| Vision-based | Yes | Yes | Yes | Yes | No | No | Low |
| Robot | No | Yes | No | No | No | Yes | High |
| HMD-VR | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Features | Outside-In | Inside-Out (Marker-Based) | Inside-Out (Markerless) |
|---|---|---|---|
| Portability | ✗ | ✓ | ✓ |
| Untethered | ✗ | ✓ | ✓ |
| Hand gesture | ✗ | ✗ | ✓ |
| HMD field of view tracking | ✓ | ✓ | ✓ |
| External field of view tracking | ✓ | ✗ | ✗ |
| Study Reference | MoCap Systems Comparison | Performed Task | Parameters of Precision/Accuracy | Kinematic Assessment |
|---|---|---|---|---|
| HMD Outside-In | ||||
| [50] | IMUs and HMD VR sensor (Vive) compared with Optoelectronic system (Vicon) | Wrist position, during reaching tasks, with respect to the shoulder | Compared to a traditional optical tracking system, both methods accurately tracked the wrist during reaching, with mean signed errors of 0.09 ± 1.81 cm and 0.48 ± 1.58 cm for the IMUs and Vive, respectively. | Normalised mean endpoint speed (Smoothness) |
| [66] | HTC Vive HMD and Vive tracker | Reaching tasks | HTC Vive headset and Vive Trackers showed that both can track joint rotation and position with reasonable accuracy and a very low end to latency of 6.71 ± 0.80 ms. | Joint rotation and position |
| HMD Inside-Out Marker-based | ||||
| [81] | HMD (Oculus Quest 2) compared with Qualysis optical capture system | Upper limb rotational and translational movements | The results showed a mean absolute error of 13.52 ± 6.57 mm at a distance of 500 mm from the HMD along the x-direction. The maximum mean absolute error for rotational displacements was found to be 1.11 ± 0.37° for a rotation of 40° around the z-axis. | Translational and rotational movement |
| [71] | HMD (Oculus Touch v2) controller compared with IMU | Flexion–extension movement of the forearm. | The level of agreement between the measurements of these devices was 0.999 with a 95% confidence interval (ranged from 0.996 to 1.000). The accuracy degrades at flexion values between 70° and 110°, peaking at 90°. | Range of motion of elbow in the sagittal plane |
| HMD Inside-Out Marker-less | ||||
| [72] | HMD (Oculus Quest 2, Meta) compared with Optoelectronic system (Optitrack). | Reaching | Maximum distance: mean slope = 0.94 ± 0.1; peak velocity: mean slope = 1.06 ± 0.12). | Peak velocity and hand position |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Pasquale, P.; Bonanno, M.; Mojdehdehbaher, S.; Quartarone, A.; Calabrò, R.S. The Use of Head-Mounted Display Systems for Upper Limb Kinematic Analysis in Post-Stroke Patients: A Perspective Review on Benefits, Challenges and Other Solutions. Bioengineering 2024, 11, 538. https://doi.org/10.3390/bioengineering11060538
De Pasquale P, Bonanno M, Mojdehdehbaher S, Quartarone A, Calabrò RS. The Use of Head-Mounted Display Systems for Upper Limb Kinematic Analysis in Post-Stroke Patients: A Perspective Review on Benefits, Challenges and Other Solutions. Bioengineering. 2024; 11(6):538. https://doi.org/10.3390/bioengineering11060538
Chicago/Turabian StyleDe Pasquale, Paolo, Mirjam Bonanno, Sepehr Mojdehdehbaher, Angelo Quartarone, and Rocco Salvatore Calabrò. 2024. "The Use of Head-Mounted Display Systems for Upper Limb Kinematic Analysis in Post-Stroke Patients: A Perspective Review on Benefits, Challenges and Other Solutions" Bioengineering 11, no. 6: 538. https://doi.org/10.3390/bioengineering11060538
APA StyleDe Pasquale, P., Bonanno, M., Mojdehdehbaher, S., Quartarone, A., & Calabrò, R. S. (2024). The Use of Head-Mounted Display Systems for Upper Limb Kinematic Analysis in Post-Stroke Patients: A Perspective Review on Benefits, Challenges and Other Solutions. Bioengineering, 11(6), 538. https://doi.org/10.3390/bioengineering11060538