



Identification of Adolescent Menarche Status Using Biplanar X-ray Images: A Deep Learning-Based Method

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
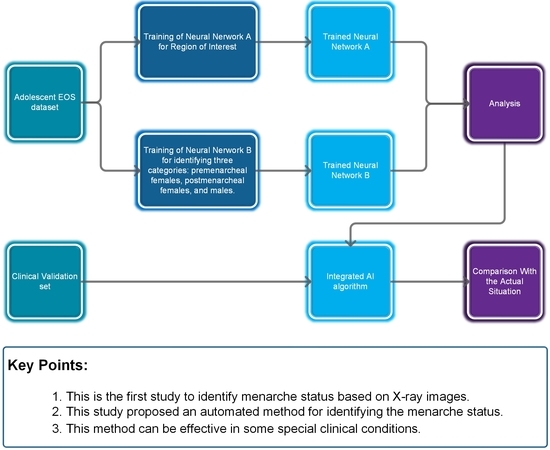
2.2. Neural Network A: Detection Network for ROI
2.3. Image Processing Module
2.4. Neural Network B: Classification Network
2.5. Integrated AI Program
2.6. Clinical Validation
2.7. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karapanou, O.; Papadimitriou, A. Determinants of menarche. Reprod. Biol. Endocrinol. 2010, 8, 115. [Google Scholar] [CrossRef]
- Bradley, S.H.; Lawrence, N.; Steele, C.; Mohamed, Z. Precocious puberty. BMJ 2020, 368, l6597. [Google Scholar] [CrossRef]
- Melmed, S.; Kaiser, U.B.; Lopes, M.B.; Bertherat, J.; Syro, L.V.; Raverot, G.; Reincke, M.; Johannsson, G.; Beckers, A.; Fleseriu, M.; et al. Clinical Biology of the Pituitary Adenoma. Endocr. Rev. 2022, 43, 1003–1037. [Google Scholar] [CrossRef]
- Klein, D.A.; Paradise, S.L.; Reeder, R.M. Amenorrhea: A Systematic Approach to Diagnosis and Management. Am. Fam. Physician 2019, 100, 39–48. [Google Scholar]
- Brown, R.; Goulder, P.; Matthews, P.C. Sexual Dimorphism in Chronic Hepatitis B Virus (HBV) Infection: Evidence to Inform Elimination Efforts. Wellcome Open Res. 2022, 7, 32. [Google Scholar] [CrossRef]
- Almeida, M.; Laurent, M.R.; Dubois, V.; Claessens, F.; O’Brien, C.A.; Bouillon, R.; Vanderschueren, D.; Manolagas, S.C. Estrogens and Androgens in Skeletal Physiology and Pathophysiology. Physiol. Rev. 2017, 97, 135–187. [Google Scholar] [CrossRef]
- Farr, J.N.; Khosla, S. Skeletal changes through the lifespan--from growth to senescence. Nat. Rev. Endocrinol. 2015, 11, 513–521. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Menarche, menopause, and breast cancer risk: Individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012, 13, 1141–1151. [Google Scholar] [CrossRef]
- Gong, T.T.; Wang, Y.L.; Ma, X.X. Age at menarche and endometrial cancer risk: A dose-response meta-analysis of prospective studies. Sci. Rep. 2015, 5, 14051. [Google Scholar] [CrossRef]
- Okoth, K.; Chandan, J.S.; Marshall, T.; Thangaratinam, S.; Thomas, G.N.; Nirantharakumar, K.; Adderley, N.J. Association between the reproductive health of young women and cardiovascular disease in later life: Umbrella review. BMJ 2020, 371, m3502. [Google Scholar] [CrossRef]
- Bubach, S.; De Mola, C.L.; Hardy, R.; Dreyfus, J.; Santos, A.C.; Horta, B.L. Early menarche and blood pressure in adulthood: Systematic review and meta-analysis. J. Public Health 2018, 40, 476–484. [Google Scholar] [CrossRef]
- Janghorbani, M.; Mansourian, M.; Hosseini, E. Systematic review and meta-analysis of age at menarche and risk of type 2 diabetes. Acta Diabetol. 2014, 51, 519–528. [Google Scholar] [CrossRef]
- Sommer, M.; Sutherland, C.; Chandra-Mouli, V. Putting menarche and girls into the global population health agenda. Reprod. Health 2015, 12, 24. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Berking, C.; Haferkamp, S.; Hauschild, A.; Weichenthal, M.; Klode, J.; Schadendorf, D.; Holland-Letz, T.; et al. Deep neural networks are superior to dermatologists in melanoma image classification. Eur. J. Cancer 2019, 119, 11–17. [Google Scholar] [CrossRef]
- Keenan, T.D.L.; Chen, Q.; Agron, E.; Tham, Y.C.; Goh, J.H.L.; Lei, X.; Ng, Y.P.; Liu, Y.; Xu, X.; Cheng, C.Y.; et al. DeepLensNet: Deep Learning Automated Diagnosis and Quantitative Classification of Cataract Type and Severity. Ophthalmology 2022, 129, 571–584. [Google Scholar] [CrossRef]
- Wang, Y.M.; Li, Y.; Cheng, Y.S.; He, Z.Y.; Yang, J.M.; Xu, J.H.; Chi, Z.C.; Chi, F.L.; Ren, D.D. Deep Learning in Automated Region Proposal and Diagnosis of Chronic Otitis Media Based on Computed Tomography. Ear Hear. 2020, 41, 669–677. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.; van Ginneken, B.; Sanchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef]
- Ge, Z.; Liu, S.; Wang, F.; Li, Z.; Sun, J.J. YOLOX: Exceeding YOLO Series in 2021. arXiv 2021, arXiv:2107.08430. [Google Scholar] [CrossRef]
- Melhem, E.; Assi, A.; El Rachkidi, R.; Ghanem, I. EOS® biplanar X-ray imaging: Concept, developments, benefits, and limitations. J. Child. Orthop. 2016, 10, 1–14. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q.V.J. EfficientNetV2: Smaller Models and Faster Training. arXiv 2021, arXiv:2104.00298. [Google Scholar] [CrossRef]
- Loshchilov, I.; Hutter, F.J. Decoupled Weight Decay Regularization. arXiv 2017, arXiv:1711.05101. [Google Scholar] [CrossRef]
- Nahiduzzaman, M.; Islam, M.R.; Hassan, R. ChestX-Ray6: Prediction of multiple diseases including COVID-19 from chest X-ray images using convolutional neural network. Expert Syst. Appl. 2023, 211, 118576. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Huo, Y.; Deng, R.; Liu, Q.; Fogo, A.B.; Yang, H. AI applications in renal pathology. Kidney Int. 2021, 99, 1309–1320. [Google Scholar] [CrossRef]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.M.; Larochelle, H. Brain tumor segmentation with Deep Neural Networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef]
- Livovsky, D.M.; Veikherman, D.; Golany, T.; Aides, A.; Dashinsky, V.; Rabani, N.; Ben Shimol, D.; Blau, Y.; Katzir, L.; Shimshoni, I.; et al. Detection of elusive polyps using a large-scale artificial intelligence system (with videos). Gastrointest. Endosc. 2021, 94, 1099–1109.e10. [Google Scholar] [CrossRef]
- Seo, H.; Badiei Khuzani, M.; Vasudevan, V.; Huang, C.; Ren, H.; Xiao, R.; Jia, X.; Xing, L. Machine learning techniques for biomedical image segmentation: An overview of technical aspects and introduction to state-of-art applications. Med. Phys. 2020, 47, e148–e167. [Google Scholar] [CrossRef]
- Lu, Y.; Li, K.; Pu, B.; Tan, Y.; Zhu, N. A YOLOX-based Deep Instance Segmentation Neural Network for Cardiac Anatomical Structures in Fetal Ultrasound Images. IEEE/ACM Trans Comput. Biol. Bioinform. 2022. [Google Scholar] [CrossRef]
- Teng, C.; Kylili, K.; Hadjistassou, C. Deploying deep learning to estimate the abundance of marine debris from video footage. Mar. Pollut. Bull. 2022, 183, 114049. [Google Scholar] [CrossRef]
- Wang, A.; Peng, T.; Cao, H.; Xu, Y.; Wei, X.; Cui, B. TIA-YOLOv5: An improved YOLOv5 network for real-time detection of crop and weed in the field. Front. Plant Sci. 2022, 13, 1091655. [Google Scholar] [CrossRef]
- Sizonenko, P.C. Physiology of puberty. J. Endocrinol. Investig. 1989, 12, 59–63. [Google Scholar]
- Huang, M.L.; Liao, Y.C. Stacking Ensemble and ECA-EfficientNetV2 Convolutional Neural Networks on Classification of Multiple Chest Diseases Including COVID-19. Acad. Radiol. 2022, in press. [Google Scholar] [CrossRef]
- Lee, M.J.; Yang, M.K.; Khwarg, S.I.; Oh, E.K.; Choi, Y.J.; Kim, N.; Choung, H.; Seo, C.W.; Ha, Y.J.; Cho, M.H.; et al. Differentiating malignant and benign eyelid lesions using deep learning. Sci. Rep. 2023, 13, 4103. [Google Scholar] [CrossRef]
- Liu, Y.; Tong, Y.; Wan, Y.; Xia, Z.; Yao, G.; Shang, X.; Huang, Y.; Chen, L.; Chen, D.Q.; Liu, B. Identification and diagnosis of mammographic malignant architectural distortion using a deep learning based mask regional convolutional neural network. Front. Oncol. 2023, 13, 1119743. [Google Scholar] [CrossRef]
- Song, Y.; Ma, J.; Agardh, A.; Lau, P.W.; Hu, P.; Zhang, B. Secular trends in age at menarche among Chinese girls from 24 ethnic minorities, 1985 to 2010. Glob. Health Action 2015, 8, 26929. [Google Scholar] [CrossRef]
- Feng, T.; Zhai, Y.; Yang, J.; Liang, J.; Fan, D.P.; Zhang, J.; Shao, L.; Tao, D. IC9600: A Benchmark Dataset for Automatic Image Complexity Assessment. IEEE Trans Pattern Anal. Mach. Intell. 2022, 45, 8577–8593. [Google Scholar] [CrossRef]
- Luo, Z.; Branchaud-Charron, F.; Lemaire, C.; Konrad, J.; Li, S.; Mishra, A.; Achkar, A.; Eichel, J.; Jodoin, P.M. MIO-TCD: A new benchmark dataset for vehicle classification and localization. IEEE Trans. Image Process. 2018, 27, 5129–5141. [Google Scholar] [CrossRef]
- Verma, R.; Kumar, N.; Patil, A.; Kurian, N.C.; Rane, S.; Graham, S.; Vu, Q.D.; Zwager, M.; Raza, S.E.A.; Rajpoot, N.; et al. MoNuSAC2020: A Multi-Organ Nuclei Segmentation and Classification Challenge. IEEE Trans. Med. Imaging 2021, 40, 3413–3423. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | Total | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-menarche | Post-menarche | |||||||||||||||||
| P25 | Median | P75 | Count | P25 | Median | P75 | Count | P25 | Median | P75 | Count | P25 | Median | P75 | Count | |||
| Subsets | 1 | Age (years) | 9.9 | 10.7 | 11.8 | 34 | 13.8 | 14.6 | 16.5 | 41 | 11.2 | 13.9 | 15.8 | 72 | 11.1 | 13.6 | 15.7 | 147 |
| 2 | Age (years) | 9.8 | 10.8 | 11.6 | 32 | 13.3 | 14.8 | 16.2 | 45 | 11.3 | 13.6 | 15.6 | 70 | 11.1 | 13.4 | 15.4 | 147 | |
| 3 | Age (years) | 9.7 | 10.9 | 11.8 | 24 | 13.8 | 15.1 | 16.4 | 49 | 11.1 | 12.7 | 15.7 | 74 | 11.2 | 13.4 | 15.5 | 147 | |
| 4 | Age (years) | 10.1 | 10.9 | 11.6 | 29 | 14 | 15.5 | 16.4 | 43 | 11.3 | 13 | 15.3 | 75 | 11.2 | 13.2 | 15.6 | 147 | |
| 5 | Age (years) | 9.5 | 10.7 | 11.8 | 23 | 13.8 | 15.6 | 16.7 | 49 | 10.8 | 13.3 | 16.3 | 78 | 11.3 | 13.8 | 16.3 | 150 | |
| Total | Age (years) | 9.8 | 10.8 | 11.8 | 142 | 13.8 | 15.1 | 16.4 | 227 | 11.1 | 13.5 | 15.7 | 369 | 11.2 | 13.5 | 15.7 | 738 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, L.; Ge, T.; Xiao, B.; Han, X.; Zhang, Q.; Xu, Z.; He, D.; Tian, W. Identification of Adolescent Menarche Status Using Biplanar X-ray Images: A Deep Learning-Based Method. Bioengineering 2023, 10, 769. https://doi.org/10.3390/bioengineering10070769
Xie L, Ge T, Xiao B, Han X, Zhang Q, Xu Z, He D, Tian W. Identification of Adolescent Menarche Status Using Biplanar X-ray Images: A Deep Learning-Based Method. Bioengineering. 2023; 10(7):769. https://doi.org/10.3390/bioengineering10070769
Chicago/Turabian StyleXie, Linzhen, Tenghui Ge, Bin Xiao, Xiaoguang Han, Qi Zhang, Zhongning Xu, Da He, and Wei Tian. 2023. "Identification of Adolescent Menarche Status Using Biplanar X-ray Images: A Deep Learning-Based Method" Bioengineering 10, no. 7: 769. https://doi.org/10.3390/bioengineering10070769
APA StyleXie, L., Ge, T., Xiao, B., Han, X., Zhang, Q., Xu, Z., He, D., & Tian, W. (2023). Identification of Adolescent Menarche Status Using Biplanar X-ray Images: A Deep Learning-Based Method. Bioengineering, 10(7), 769. https://doi.org/10.3390/bioengineering10070769