
Train vs. Play: Evaluating the Effects of Gamified and Non-Gamified Wheelchair Skills Training Using Virtual Reality

 ,
,  and
and
Abstract
:
1. Introduction
2. Related Work
2.1. Environment Design of Wheelchair Skills Training in VR
2.2. Gamification in Training
3. Materials and Methods
3.1. Participants and Ethics
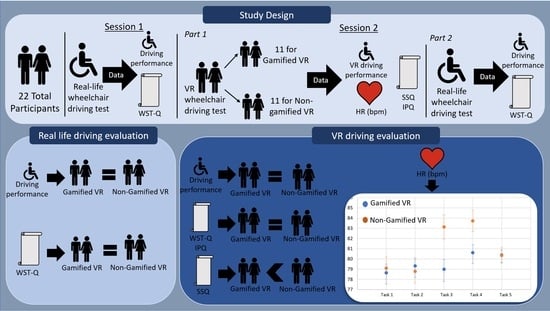
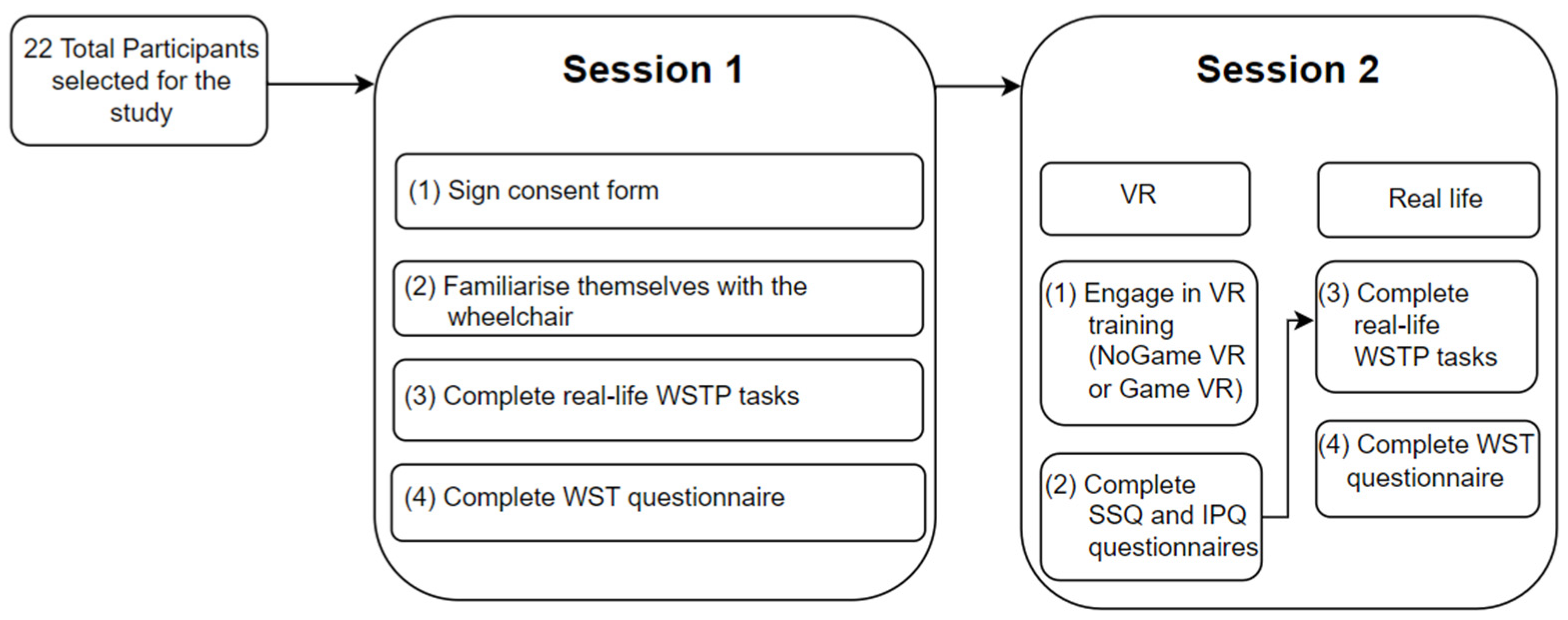
3.2. Setup of the Study
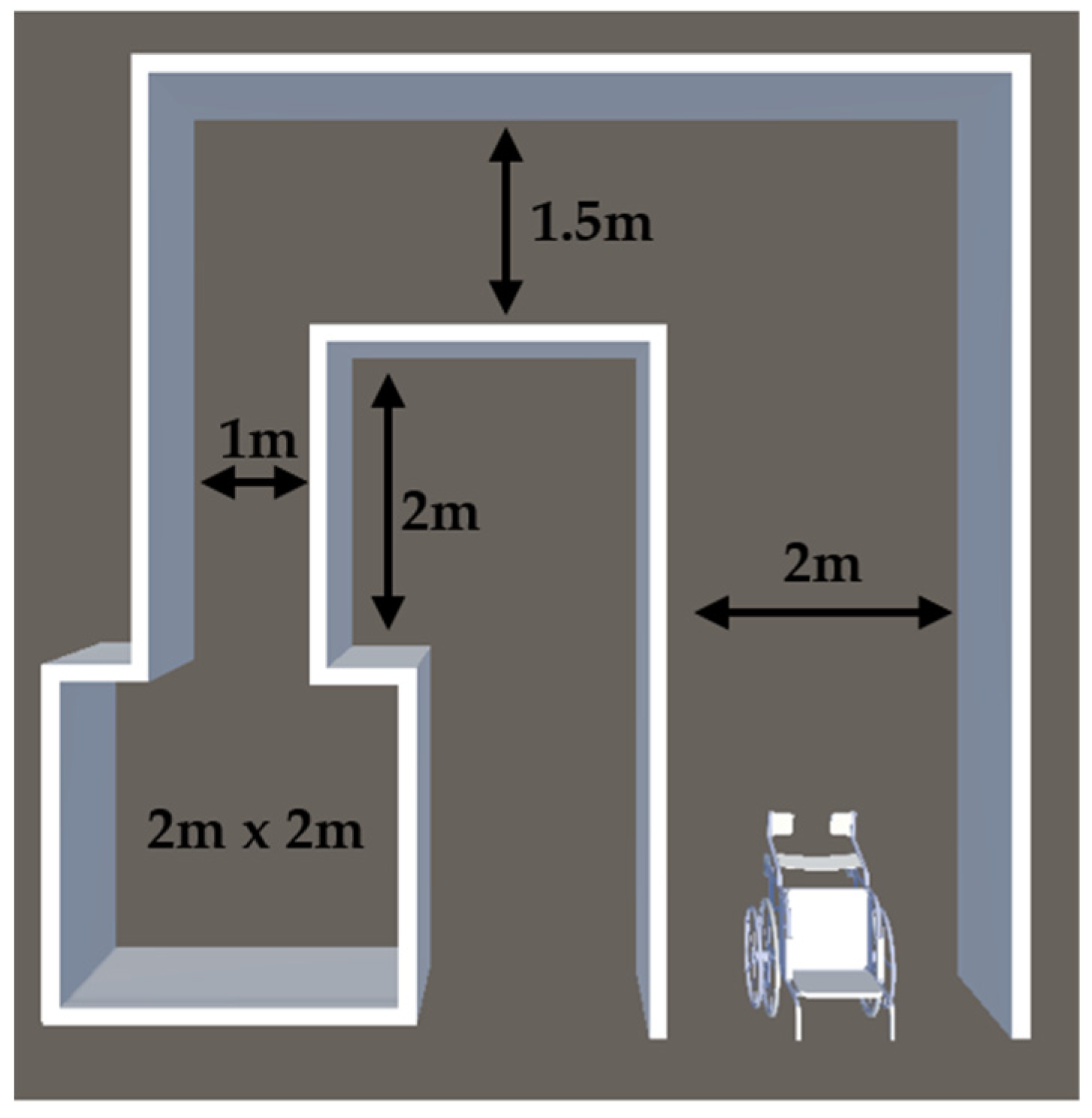
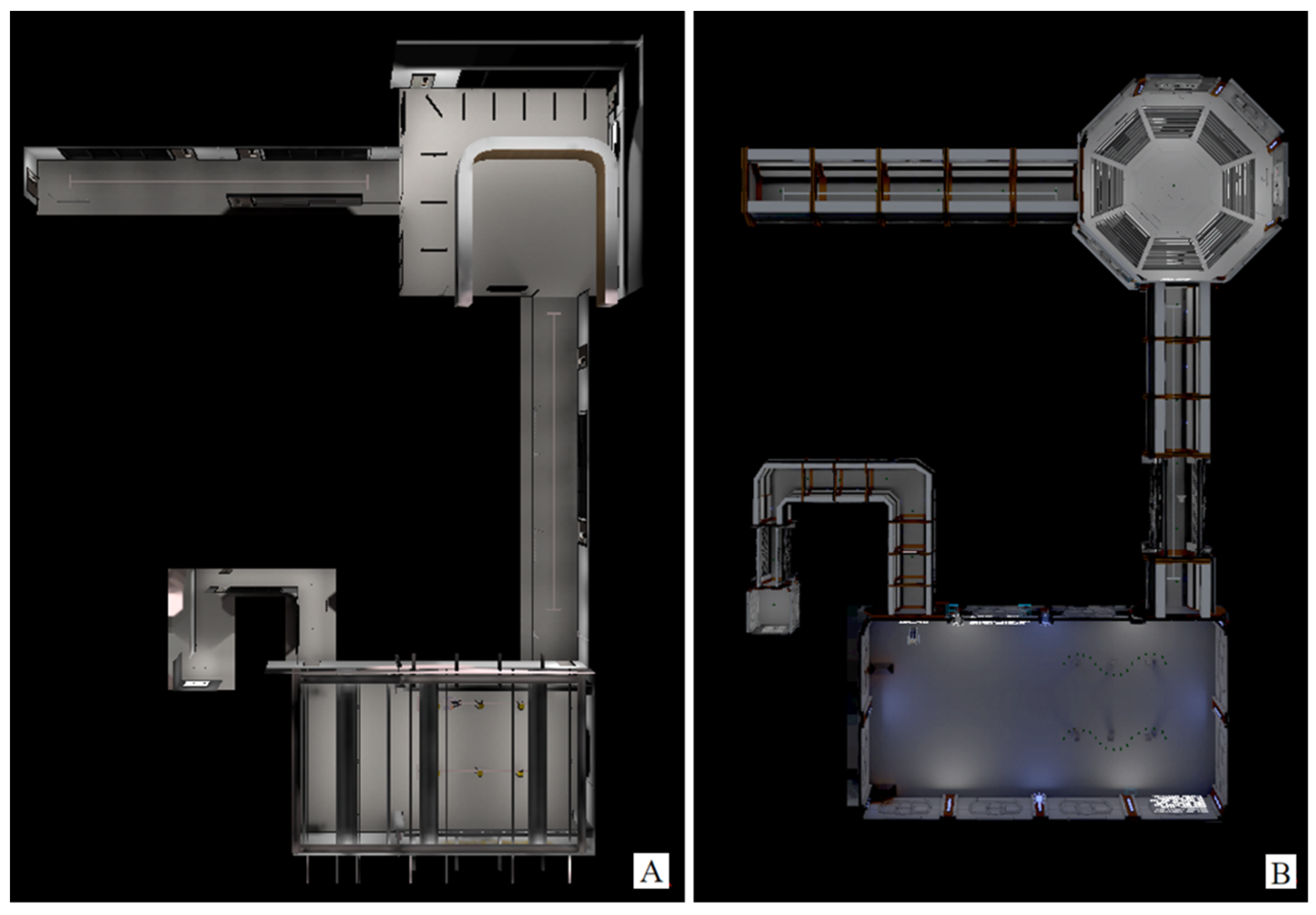
3.2.1. Real-Life Environment for Skills Evaluation
3.2.2. NoGame VR Training
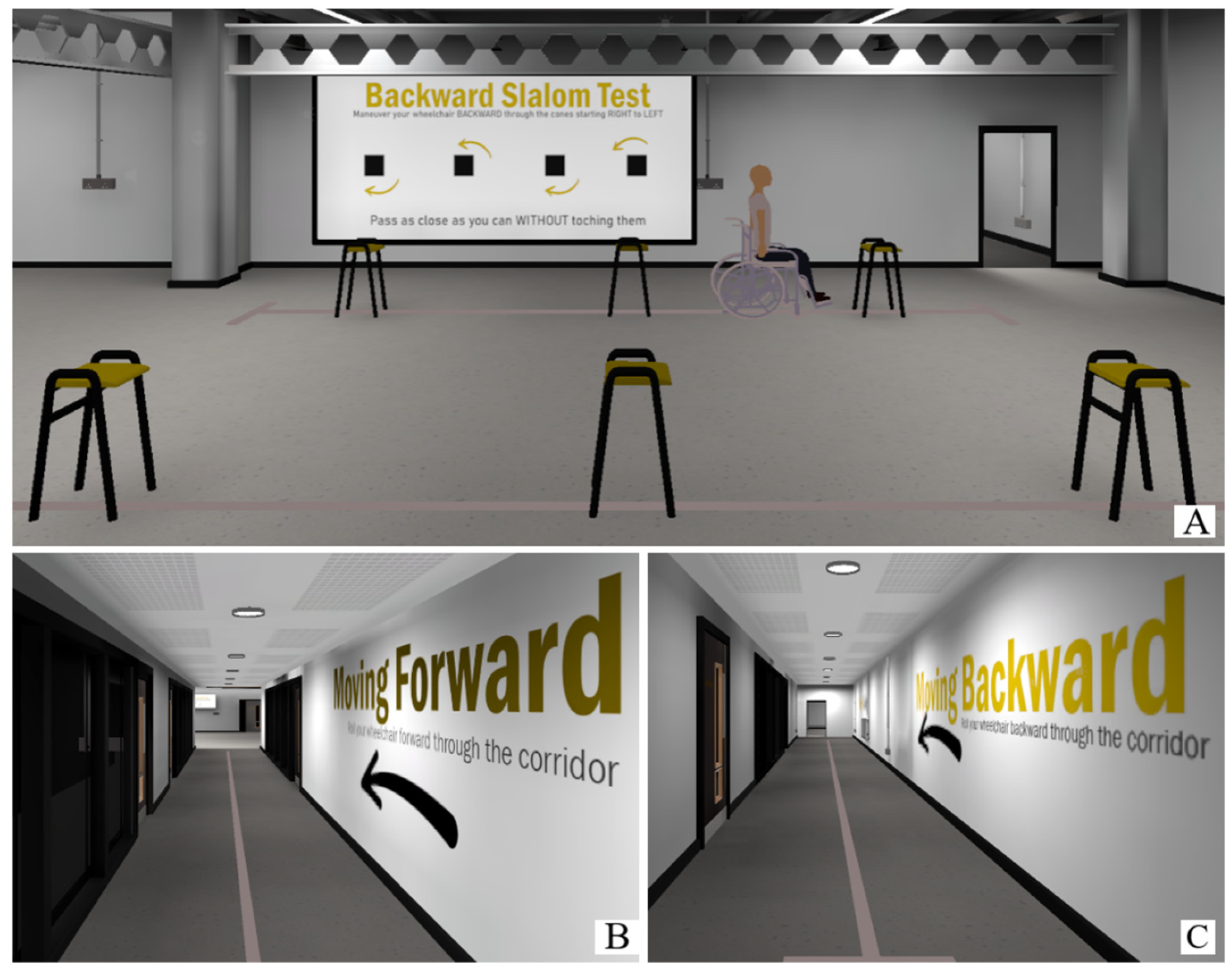
3.2.3. Game VR Training
3.3. Hardware of the System
3.3.1. Controller
3.4. Data Collection and Processing
3.4.1. Data Collected to Test H1: Real-Life Driving Performance after VR Training Will Differ Based on the Environment
Sum of Movement of the Joystick
Completion Time
Number of Collisions
WSTP-Style Questionnaire
3.4.2. Data Collected to test H2: The Levels of Involvement and Presence Will Vary Based on the Environment
Igroup Presence Questionnaire
3.4.3. Data Collected to Test H3: The Perceived Cybersickness Will Vary Based on the Environment
Heart Rate
Simulator Sickness Questionnaire
4. Results
4.1. Results of the Data Collected to Test H1: Real-Life Driving Performance after VR Training Will Differ Based on the Environment
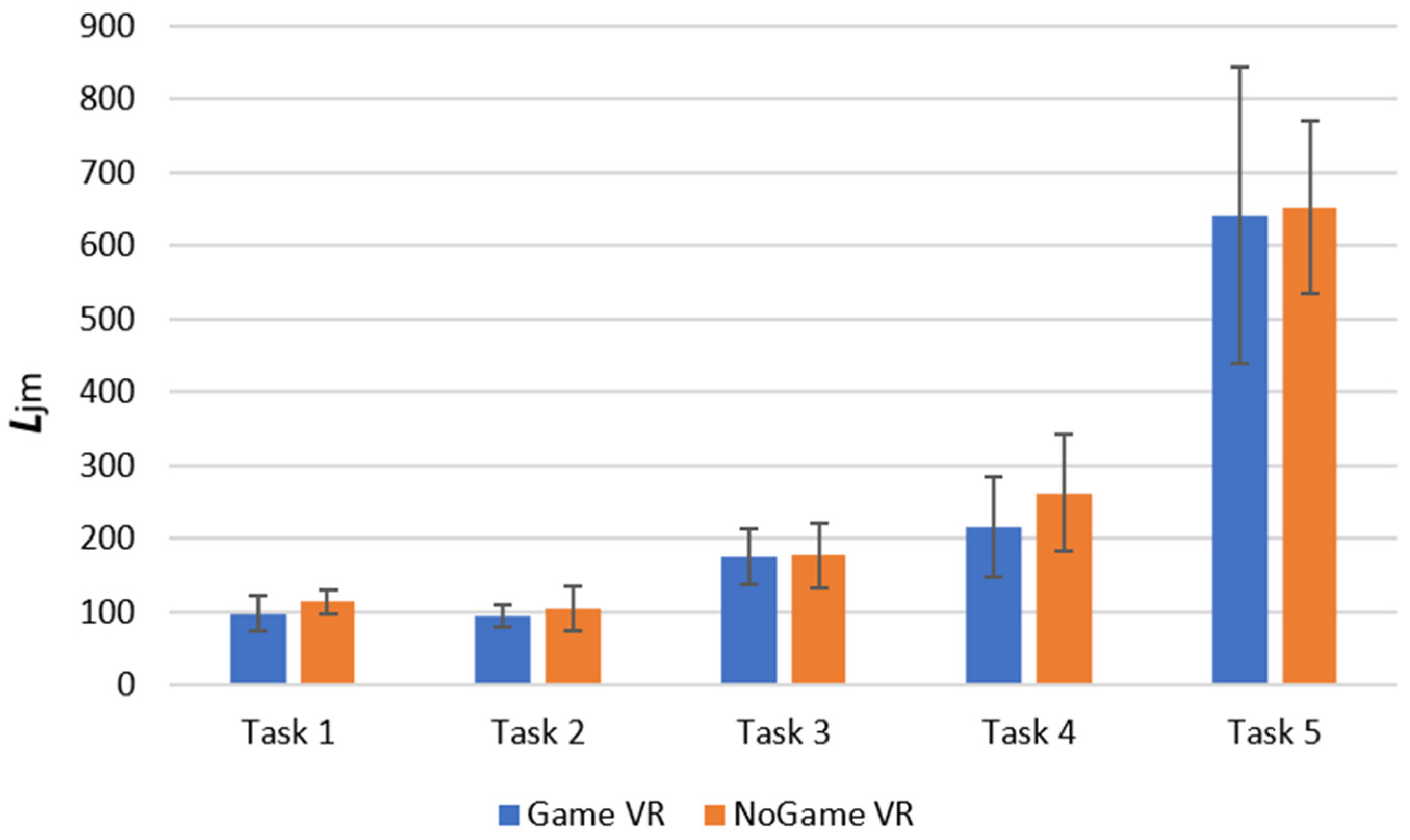
4.1.1. Proxy of the Sum of Joystick Movements, Ljm
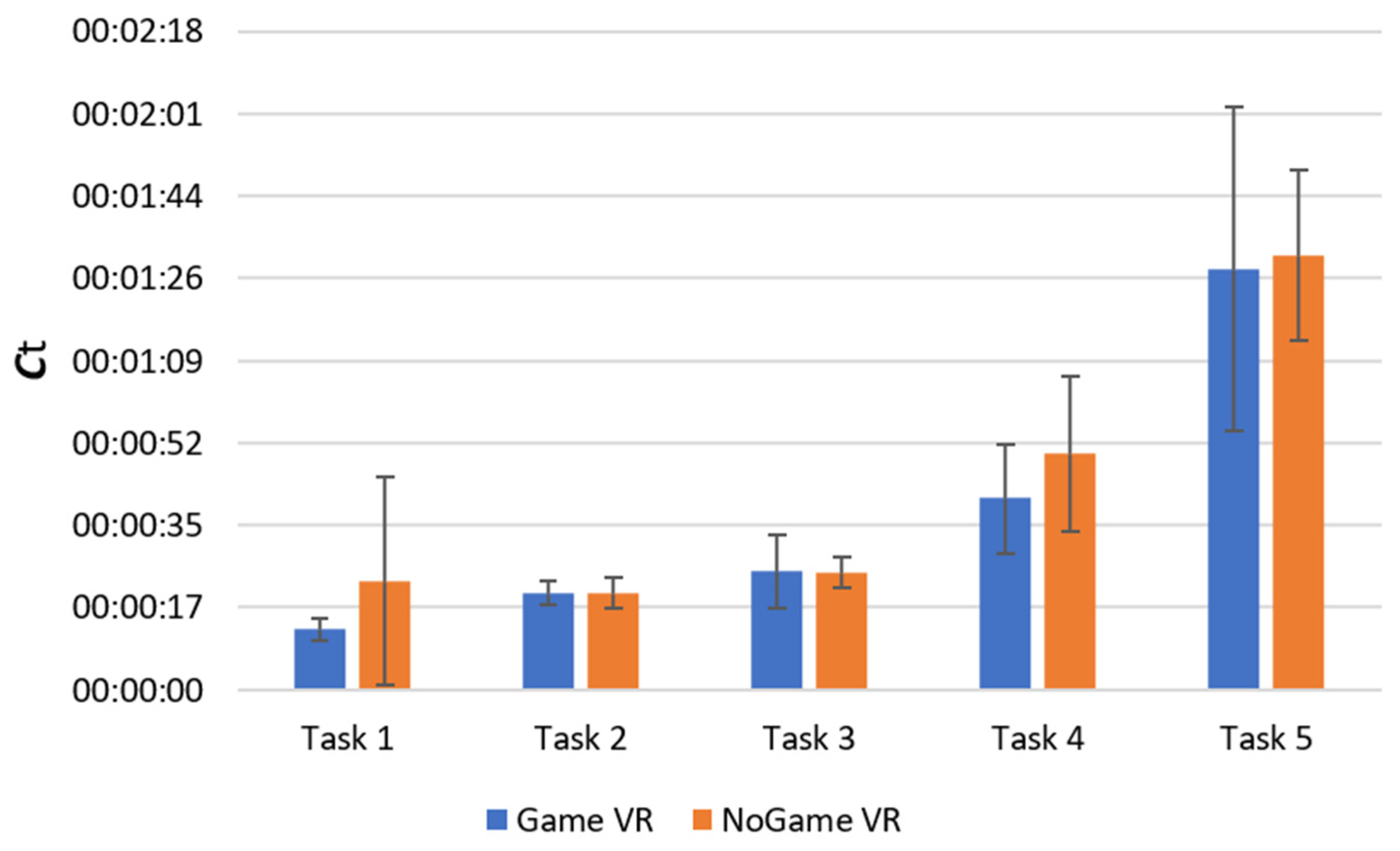
4.1.2. Completion Time
4.1.3. Number of Collisions
4.1.4. WSTP-Style Questionnaire
4.2. Results of the Data Collected to Test H2: The Levels of Involvement and Presence Will Vary Based on the Environment
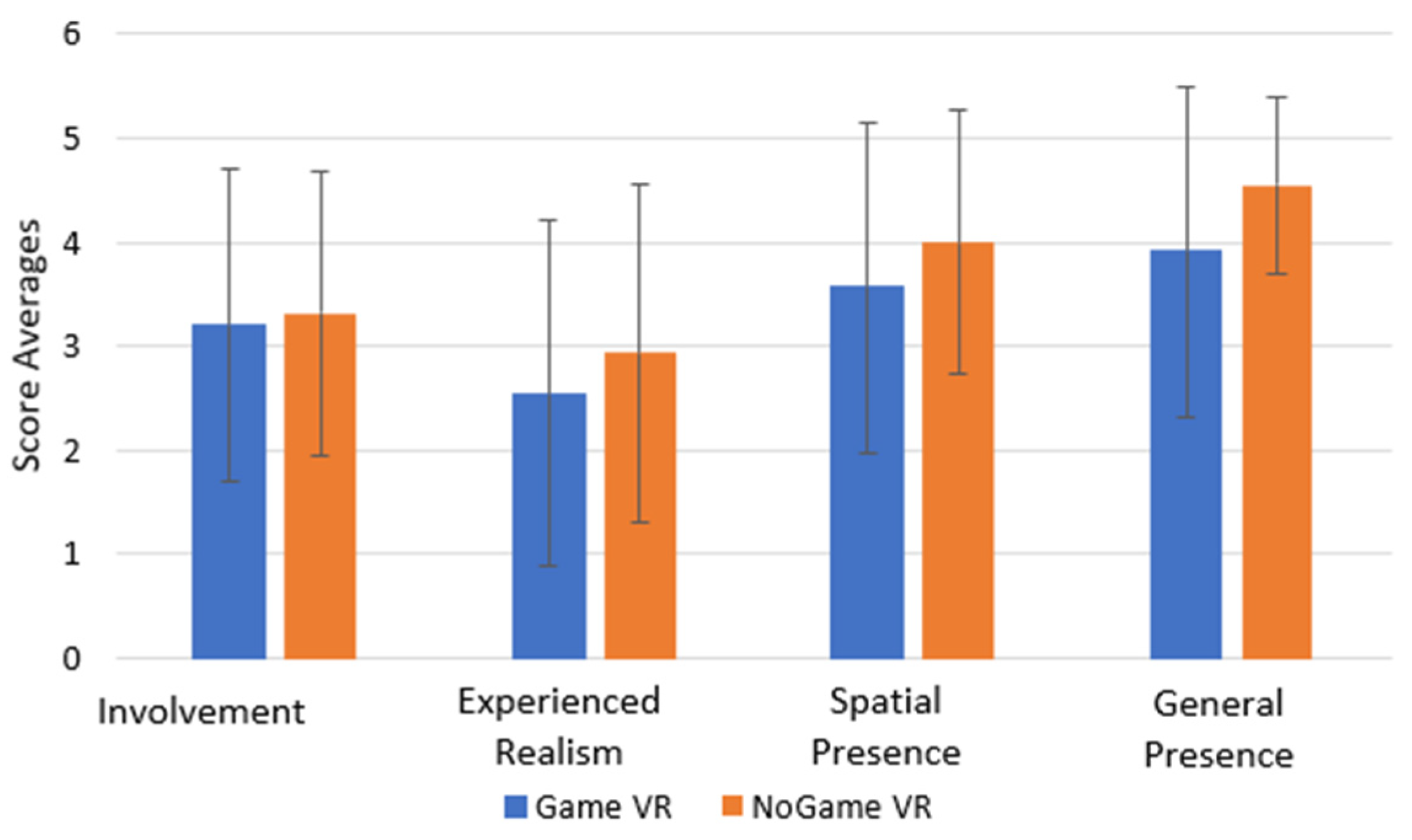
Igroup Presence Questionnaire
4.3. Results of the Data Collected to Test H3: The Perceived Cybersickness Will Vary Based on the Environment
4.3.1. Heart Rate
4.3.2. Simulator Sickness Questionnaire
5. Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| User ID: | |
| Adapted version of the Wheelchair Skills Test Questionnaire (WST-Q) Version 5.2 for Powered Wheelchairs | |
| Question | Answer |
| How experienced are you in driving a wheelchair? | □ 1 □ 2 □ 3 □ 4 □ 5 |
| How experienced are you with gaming? | □ 1 □ 2 □ 3 □ 4 □ 5 |
| How experienced are you with VR? | □ 1 □ 2 □ 3 □ 4 □ 5 |
| How realistic did the VR joystick feel? | □ 1 □ 2 □ 3 □ 4 □ 5 |
| What is your age range? | □ 18–23 □ 24–28 □ 29–33 □ 34–38 □ 39–43 □ 44–48 □ 49–53 □ 54–58 □ 59–63 □ 63+ |
| To which gender do you most identify? | □ Male □ Female □ Other: ……………… □ Prefer not say |
| Introduction to the questionnaire | |
| • Copies of this questionnaire can be downloaded from www.wheelchairskillsprogram.ca/eng/wstq.php (accessed on 25 December 2022). | |
| • More details about the questionnaire can be found there in the WSP Manual. | |
| • In this questionnaire, you will be asked questions about different skills that you might do in your wheelchair. These skills range from ones that are more basic at the beginning to those that are more advanced at the end. | |
| • There are no “right” or “wrong” answers. The purpose of the questionnaire is simply to help us understand how you use your wheelchair. | |
| • It will probably take about 10 min to complete the questionnaire, but please take as much time as you need. | |
| • If you have any comments, you will be able to record them at the end of the questionnaire. | |
| • For each specific skill, beginning on page 3. The questions and the possible answers are shown below. | |
| # | Skill Description | ||
| 1 | Moving the wheelchair forward, for example along a hallway. | □ Yes, very well □ Yes, but not well □ Yes, with help □ No | □ Very confident □ Somewhat confident □ Somewhat unconfident □ Very unconfident |
| 2 | Moving the wheelchair backward, for example to back away from a table. | □ Yes, very well □ Yes, but not well □ Yes, with help □ No | □ Very confident □ Somewhat confident □ Somewhat unconfident □ Very unconfident |
| 3 | Turning the wheelchair around in a small space so that it is facing in the opposite direction. | □ Yes, very well □ Yes, but not well □ Yes, with help □ No | □ Very confident □ Somewhat confident □ Somewhat unconfident □ Very unconfident |
| 4 | Turning the wheelchair around obstacles while moving forward. | □ Yes, very well □ Yes, but not well □ Yes, with help □ No | □ Very confident □ Somewhat confident □ Somewhat unconfident □ Very unconfident |
| 5 | Turning the wheelchair around obstacles while moving backward. | □ Yes, very well □ Yes, but not well □ Yes, with help □ No | □ Very confident □ Somewhat confident □ Somewhat unconfident □ Very unconfident |
| 6 | Moving the wheelchair sideways in a small space, for example to get the side of your wheelchair next to a kitchen counter, and then back to where you started. | □ Yes, very well □ Yes, but not well □ Yes, with help □ No | □ Very confident □ Somewhat confident □ Somewhat unconfident □ Very unconfident |
| If you have any general comments about the questions that you have answered above, please record them in the space available below. |
| This is the end of the questionnaire. Thank you for completing it. |
References
- World Health Organization Wheelchair Publications—An Overview. Available online: https://www.who.int/news-room/articles-detail/wheelchair_publications%E2%80%93an_overview (accessed on 19 September 2022).
- Lam, J.F.; Gosselin, L.; Rushton, P.W. Use of Virtual Technology as an Intervention for Wheelchair Skills Training: A Systematic Review. Arch. Phys. Med. Rehabil. 2018, 99, 2313–2341. [Google Scholar] [CrossRef] [PubMed]
- Bigras, C.; Owonuwa, D.D.; Miller, W.C.; Archambault, P.S. A Scoping Review of Powered Wheelchair Driving Tasks and Performance-Based Outcomes. Disabil. Rehabil. Assist. Technol. 2020, 15, 76–91. [Google Scholar] [CrossRef] [PubMed]
- Best, K.L.; Routhier, F.; Miller, W.C. A Description of Manual Wheelchair Skills Training: Current Practices in Canadian Rehabilitation Centers. Disabil. Rehabil. Assist. Technol. 2014, 10, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Arlati, S.; Colombo, V.; Ferrigno, G.; Sacchetti, R.; Sacco, M. Virtual Reality-Based Wheelchair Simulators: A Scoping Review. Assist. Technol. 2020, 32, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Nunnerley, J.; Gupta, S.; Snell, D.; King, M. Training Wheelchair Navigation in Immersive Virtual Environments for Patients with Spinal Cord Injury–End-User Input to Design an Effective System. Disabil. Rehabil. Assist. Technol. 2017, 12, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.; Derwent, G.; Enticknap, A.; Attree, E.A.; Rose, F.D. The Role of Virtual Reality Technology in the Assessment and Training of Inexperienced Powered Wheelchair Users. Disabil. Rehabil. 2009, 24, 599–606. [Google Scholar] [CrossRef]
- John, N.W.; Pop, S.R.; Day, T.W.; Ritsos, P.D.; Headleand, C.J. The Implementation and Validation of a Virtual Environment for Training Powered Wheelchair Manoeuvres. IEEE Trans. Vis. Comput. Graph. 2018, 24, 1867–1878. [Google Scholar] [CrossRef]
- Débora, D.; Salgado, P.; Flynn, R.; Lázaro, E.; Martins, L.; Murray, N. A Questionnaire-Based and Physiology-Inspired Quality of Experience Evaluation of an Immersive Multisensory Wheelchair Simulator. In Proceedings of the 13th ACM Multimedia Systems Conference, Athlone, Ireland, 14–17 June 2022. [Google Scholar]
- Alshaer, A.; Regenbrecht, H.; O’Hare, D. Immersion Factors Affecting Perception and Behaviour in a Virtual Reality Power Wheelchair Simulator. Appl. Erg. 2017, 58, 1–12. [Google Scholar] [CrossRef]
- Palumbo, A.; Gramigna, V.; Calabrese, B.; Ielpo, N. Motor-Imagery EEG-Based BCIs in Wheelchair Movement and Control: A Systematic Literature Review. Sensors 2021, 21, 6285. [Google Scholar] [CrossRef] [PubMed]
- Younis, H.; Ramzan, F.; Khan, J.; Ghani Khan, M.U. Wheelchair Training Virtual Environment for People with Physical and Cognitive Disabilities. In Proceedings of the 15th International Conference on Emerging Technologies, ICET 2019, Peshawar, Pakistan, 2–3 December 2019; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2019. [Google Scholar]
- Hernandez-Ossa, K.A.; Montenegro-Couto, E.H.; Longo, B.; Bissoli, A.; Sime, M.M.; Lessa, H.M.; Enriquez, I.R.; Frizera-Neto, A.; Bastos-Filho, T. Simulation System of Electric-Powered Wheelchairs for Training Purposes. Sensors 2020, 20, 3565. [Google Scholar] [CrossRef] [PubMed]
- Salgado, D.P.; Flynn, R.; Naves, E.L.M.; Murray, N. The Impact of Jerk on Quality of Experience and Cybersickness in an Immersive Wheelchair Application. In Proceedings of the Twelfth International Conference on Quality of Multimedia Experience (QoMEX), Athlone, Ireland, 26–28 May 2020. [Google Scholar]
- Li, W.; Talavera, J.; Gomez Samayoa, A.; Lien Lap-Fai Yu, J.-M. Automatic Synthesis of Virtual Wheelchair Training Scenarios. In Proceedings of the IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Atlanta, GA, USA, 22–26 March 2020. [Google Scholar]
- Zorzi, C.; Tabbaa, L.; Covaci, A.; Sirlantzis, K.; Marcelli, G. A Standardised and Cost-Effective VR Approach for Powered Wheelchair Training. IEEE Access 2023, 11, 66921–66933. [Google Scholar] [CrossRef]
- The Chartered Society of Physiotherapy NIHR: WSTP Structured Training Improves Wheelchair Skills|The Chartered Society of Physiotherapy. Available online: https://www.csp.org.uk/frontline/article/nihr-wstp-structured-training-improves-wheelchair-skills (accessed on 10 May 2022).
- Wheelchair Skills Program. Available online: https://wheelchairskillsprogram.ca/en/ (accessed on 25 December 2022).
- Palmas, F.; Labode, D.; Plecher, D.A.; Klinker, G. Comparison of a Gamified and Non-Gamified Virtual Reality Training Assembly Task. In Proceedings of the 11th International Conference on Virtual Worlds and Games for Serious Applications (VS-Games), Vienna, Austria, 4–6 September 2019. [Google Scholar]
- Wheelchair Skills Test Questionnaire (WST-Q) Version 5.3 for Powered Wheelchairs. Available online: https://wheelchairskillsprogram.ca/en/skills- (accessed on 25 December 2022).
- Igroup Presence Questionnaire (IPQ) Item Download|Igroup.Org—Project Consortium. Available online: http://www.igroup.org/pq/ipq/download.php (accessed on 25 December 2022).
- Palumbo, A. Microsoft HoloLens 2 in Medical and Healthcare Context: State of the Art and Future Prospects. Sensors 2022, 22, 7709. [Google Scholar] [CrossRef] [PubMed]
- Garrido, L.E.; Frías-Hiciano, M.; Moreno-Jiménez, M.; Cruz, G.N.; García-Batista, Z.E.; Guerra-Peña, K.; Medrano, L.A. Focusing on Cybersickness: Pervasiveness, Latent Trajectories, Susceptibility, and Effects on the Virtual Reality Experience. Virtual Real 2022, 26, 3. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Kim, Y.S.; Won, J.H.; Jang, S.W.; Ko, J. Effects of Cybersickness Caused by Head-Mounted Display–Based Virtual Reality on Physiological Responses: Cross-Sectional Study. JMIR Serious Games 2022, 10, e37938. [Google Scholar] [CrossRef]
- Torkia, C.; Ryan, S.E.; Reid, D.; Boissy, P.; Lemay, M.; Routhier, F.; Contardo, R.; Woodhouse, J.; Archambault, P.S. Virtual Community Centre for Power Wheelchair Training: Experience of Children and Clinicians. Disabil. Rehabil. Assist. Technol. 2019, 14, 46–55. [Google Scholar] [CrossRef]
- Rodriguez, N. Identifying Accessibility Conditions for Children with Multiple Disabilities: A Virtual Reality Wheelchair Simulator. In Proceedings of the Adjunct Proceedings—2018 IEEE International Symposium on Mixed and Augmented Reality, ISMAR-Adjunct 2018, Munichi, Germany, 16–20 October 2018; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2018; pp. 370–372. [Google Scholar]
- Gefen, N.; Rigbi, A.; Archambault, P.S.; Weiss, P.L. Comparing Children’s Driving Abilities in Physical and Virtual Environments. Disabil. Rehabil. Assist. Technol. 2019, 16, 653–660. [Google Scholar] [CrossRef]
- Ota, T.; Nakamura, T.; Kuzuoka, H. Effects of Gamification and Communication in Virtual Reality Frozen Shoulder Rehabilitation for Enhanced Rehabilitation Continuity. IEEE Access 2023, 11, 50841–50850. [Google Scholar] [CrossRef]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From Game Design Elements to Gamefulness: Defining “Gamification”. In Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, Tampere, Finland, 28–30 September 2011. [Google Scholar]
- Francisco-Aparicio, A.; Gutierrez-Vela, F.L.; Isla-Montes, J.L.; Gonzalez Sanchez, J.L. Chapter 9 Gamification: Analysis and Application; Penichet, V.M.R., Peñalver, A., Gallud, J.A., Eds.; Human–Computer Interaction Series; Springer: London, UK, 2013; ISBN 978-1-4471-5444-0. [Google Scholar]
- Kern, F.; Winter, C.; Gall, D.; Kathner, I.; Pauli, P.; Latoschik, M.E. Immersive Virtual Reality and Gamification within Procedurally Generated Environments to Increase Motivation during Gait Rehabilitation. In Proceedings of the 26th IEEE Conference on Virtual Reality and 3D User Interfaces, VR 2019—Proceedings, Osaka, Japan, 23–27 March 2019; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2019; pp. 500–509. [Google Scholar]
- Putze, F.; Tidoni, E.; Zewdie, E.T.; Škola, F.; Tinková, S.; Liarokapis, F. Progressive Training for Motor Imagery Brain-Computer Interfaces Using Gamification and Virtual Reality Embodiment. Front. Hum. Neurosci. 2019, 13, 329. [Google Scholar] [CrossRef]
- Ulmer, J.; Braun, S.; Cheng, C.T.; Dowey, S.; Wollert, J. Gamification of Virtual Reality Assembly Training: Effects of a Combined Point and Level System on Motivation and Training Results. Int. J. Hum. Comput. Stud. 2022, 165, 102854. [Google Scholar] [CrossRef]
- Yan, W.; Pang, J.; Cheng, L. Acceptance of Gamified Virtual Reality Environments by Older Adults. Educ. Gerontol. 2023, 49, 830–841. [Google Scholar] [CrossRef]
- Maya Software|Get Prices & Buy Official Maya 2024|Autodesk. Available online: https://www.autodesk.com/products/maya/overview?term=1-YEAR&tab=subscription (accessed on 16 September 2023).
- Unity Real-Time Development Platform|3D, 2D VR & AR Engine. Available online: https://unity.com/ (accessed on 26 December 2022).
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being Self-Determination Theory. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Polar H10 Heart Rate Sensor System. Available online: www.polar.com (accessed on 26 December 2022).
- Farago, P.; Groza, R.; Hintea, S. High Precision Activity Tracker Based on the Correlation of Accelerometer and EMG Data. In Proceedings of the 2019 42nd International Conference on Telecommunications and Signal Processing (TSP), Budapest, Hungary, 1–3 July 2019; pp. 428–431. [Google Scholar] [CrossRef]
- Magaña, V.C.; Scherz, W.D.; Seepold, R.; Madrid, N.M.; Pañeda, X.G.; Garcia, R. The Effects of the Driver’s Mental State and Passenger Compartment Conditions on Driving Performance and Driving Stress. Sensors 2020, 20, 5274. [Google Scholar] [CrossRef] [PubMed]
- Schwind, V.; Knierim, P.; Haas, N.; Henze, N. Using Presence Questionnaires in Virtual Reality. In Proceedings of the Conference on Human Factors in Computing Systems—Proceedings, Scotland, UK, 4–9 May 2019; Association for Computing Machinery: New York, NY, USA, 2019. [Google Scholar]
- Gibbs, J.K.; Gillies, M.; Pan, X. A Comparison of the Effects of Haptic and Visual Feedback on Presence in Virtual Reality. Int. J. Hum. Comput. Stud. 2021, 157, 102717. [Google Scholar] [CrossRef]
- Riecke, B.E.; Org Schulte-Pelkum, J. Moving Sounds Enhance the Visually-Induced Self-Motion Illusion (Circular Vection) in Virtual Reality. ACM Trans. Appl. Percept. 2009, 6, 1–27. [Google Scholar] [CrossRef]
- Adhanom, I.B.; Al-Zayer, M.; Macneilage, P.; Folmer, E. Field-of-View Restriction to Reduce VR Sickness Does Not Impede Spatial Learning in Women. ACM Trans. Appl. Percept. 2021, 18, 1–17. [Google Scholar] [CrossRef]
- Groth, C.; Tauscher, J.-P.; Heesen, N.; Castillo, S.; Magnor, M. Visual Techniques to Reduce Cybersickness in Virtual Reality. In Proceedings of the IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), Lisbon, Portugal, 27 March–1 April 2021. [Google Scholar]
- Lim, K.; Lee, J.; Won, K.; Nupur, K.; Lee, T. A Novel Method for VR Sickness Reduction Based on Dynamic Field of View Processing. Virtual Real 2021, 25, 331–340. [Google Scholar] [CrossRef]
- Teixeira, J.; Palmisano, S. Effects of Dynamic Field-of-View Restriction on Cybersickness and Presence in HMD-Based Virtual Reality. Virtual Real 2020, 25, 433–445. [Google Scholar] [CrossRef]
- Ho Yip, S.; Allen Saunders, J. Restricting the Distribution of Visual Attention Reduces Cybersickness. Cogn. Res. Princ. Implic. 2023, 8, 18. [Google Scholar] [CrossRef]
- Keshavarz, B.; Hecht, H. Pleasant Music as a Countermeasure against Visually Induced Motion Sickness. Appl. Erg. 2014, 45, 521–527. [Google Scholar] [CrossRef]
- Widyanti, A.; Hafizhah, H.N. The Influence of Personality, Sound, and Content Difficulty on Virtual Reality Sickness. Virtual Real 2022, 26, 3. [Google Scholar] [CrossRef]
- Nalivaiko, E.; Davis, S.L.; Blackmore, K.L.; Vakulin, A.; Nesbitt, K. V Cybersickness Provoked by Head-Mounted Display Affects Cutaneous Vascular Tone, Heart Rate and Reaction Time; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar] [CrossRef]
- Magaki, T.; Vallance, M. Seeking Accessible Physiological Metrics to Detect Cybersickness in VR. Int. J. Virtual Augment. Real. 2020, 4, 1–18. [Google Scholar] [CrossRef]
- Chardonnet, J.R.; Mirzaei, M.A.; Mérienne, F. Using Cybersickness Indicators to Adapt Navigation in Virtual Reality: A Pre-Study. Int J Hum Comput Interact 2017, 33, 771–785. [Google Scholar] [CrossRef]
- Yildirim, C. Cybersickness during VR Gaming Undermines Game Enjoyment: A Mediation Model; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Battery Type | CR 2025 |
| Battery Sealing Ring | O-ring 20.0 × 0.90 Material Silicone |
| Battery Lifetime | 400 h |
| Sampling Rate | 1 Hz |
| Operating Temperature | −10 °C to +50 °C/14 °F to 122 °F |
| Connector Material | ABS, ABS + GF, PC, Stainless steel |
| Strap Material | 38% Polyamide, 29% Polyurethane, 20% Elastane, 13% Polyester, Silicone prints |
| Mean | SD | |
|---|---|---|
| Involvement | 3.32 | 1.36 |
| Experienced Realism | 2.93 | 1.63 |
| Spatial Presence | 4 | 1.27 |
| General Presence | 4.55 | 0.85 |
| Mean | SD | |
|---|---|---|
| Involvement | 3.2 | 1.50 |
| Experienced Realism | 2.5 | 1.66 |
| Spatial Presence | 3.56 | 1.58 |
| General Presence | 3.91 | 1.58 |
| Nausea | Oculomotor | Disorientation | Total | |
|---|---|---|---|---|
| Mean | 82.39 | 58.57 | 112.63 | 91.46 |
| SD | 24.24 | 35.24 | 56.18 | 37.45 |
| Min | 38.16 | 0 | 27.84 | 22.44 |
| Max | 114.48 | 113.7 | 208.8 | 145.86 |
| Nausea | Oculomotor | Disorientation | Total | |
|---|---|---|---|---|
| Mean | 42.5 | 33.08 | 67.07 | 51 |
| SD | 31.46 | 28.82 | 52.02 | 36.23 |
| Min | 0 | 0 | 0 | 0 |
| Max | 95.4 | 83.38 | 139.2 | 97.24 |
| Nausea | Oculomotor | Disorientation | Total | |
|---|---|---|---|---|
| None | 0 | 0 | 0 | 0 |
| Slight | 66.8 | 53.1 | 97.4 | 40.2 |
| Moderate | 133.6 | 106.1 | 194.9 | 80.4 |
| Severe | 200.3 | 159.2 | 292.3 | 120.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zorzi, C.; Tabbaa, L.; Covaci, A.; Sirlantzis, K.; Marcelli, G. Train vs. Play: Evaluating the Effects of Gamified and Non-Gamified Wheelchair Skills Training Using Virtual Reality. Bioengineering 2023, 10, 1269. https://doi.org/10.3390/bioengineering10111269
Zorzi C, Tabbaa L, Covaci A, Sirlantzis K, Marcelli G. Train vs. Play: Evaluating the Effects of Gamified and Non-Gamified Wheelchair Skills Training Using Virtual Reality. Bioengineering. 2023; 10(11):1269. https://doi.org/10.3390/bioengineering10111269
Chicago/Turabian StyleZorzi, Chantal, Luma Tabbaa, Alexandra Covaci, Konstantinos Sirlantzis, and Gianluca Marcelli. 2023. "Train vs. Play: Evaluating the Effects of Gamified and Non-Gamified Wheelchair Skills Training Using Virtual Reality" Bioengineering 10, no. 11: 1269. https://doi.org/10.3390/bioengineering10111269
APA StyleZorzi, C., Tabbaa, L., Covaci, A., Sirlantzis, K., & Marcelli, G. (2023). Train vs. Play: Evaluating the Effects of Gamified and Non-Gamified Wheelchair Skills Training Using Virtual Reality. Bioengineering, 10(11), 1269. https://doi.org/10.3390/bioengineering10111269