New Functions of Classical Compounds against Orofacial Inflammatory Lesions



Abstract
1. Introduction
2. Stomatitis and Oral Mucosal Diseases
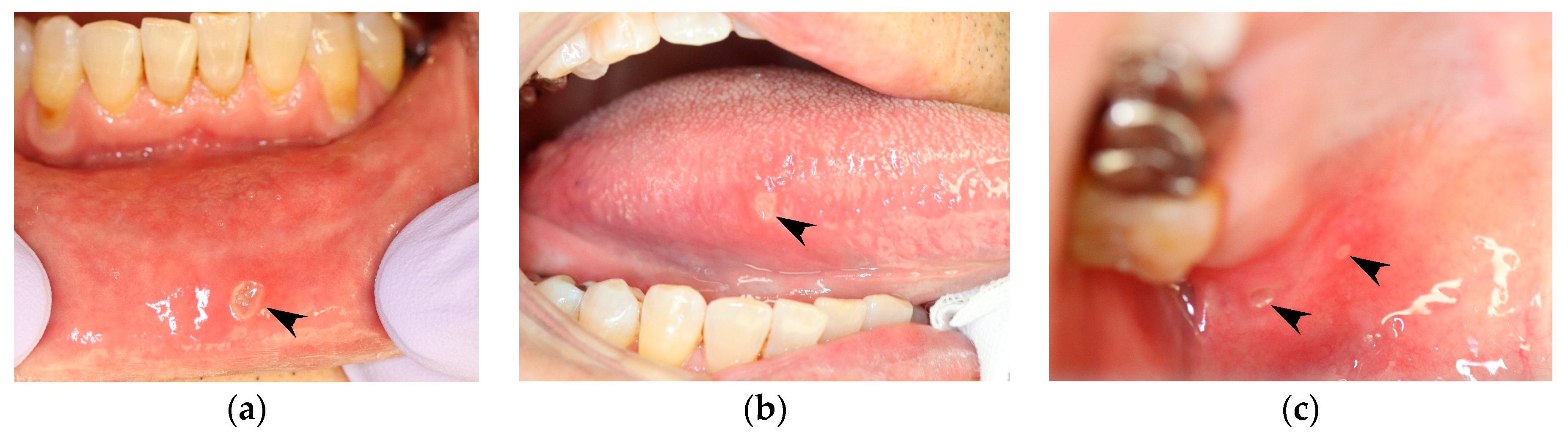
2.1. Recurrent Aphthous Stomatitis (RAS)
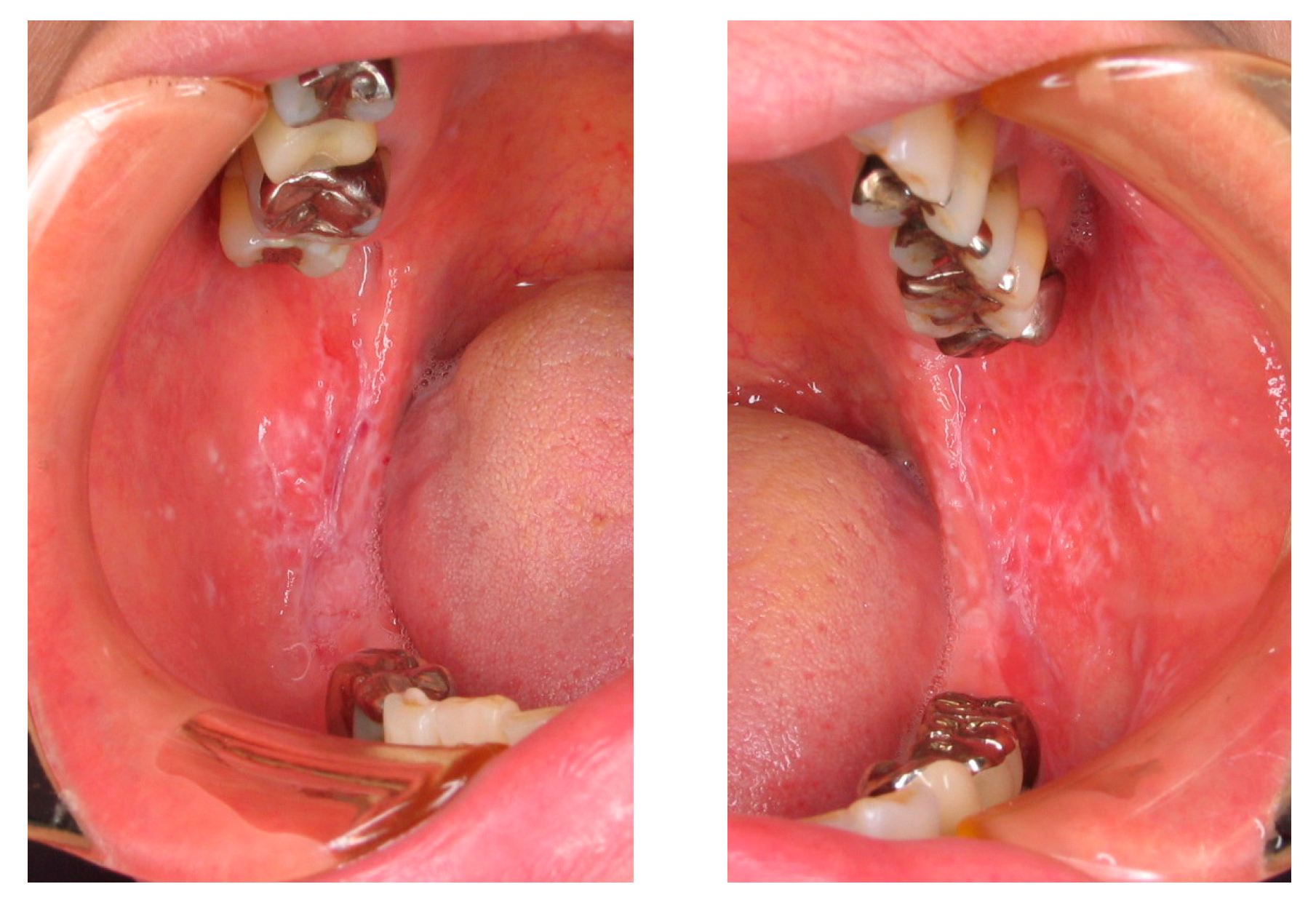
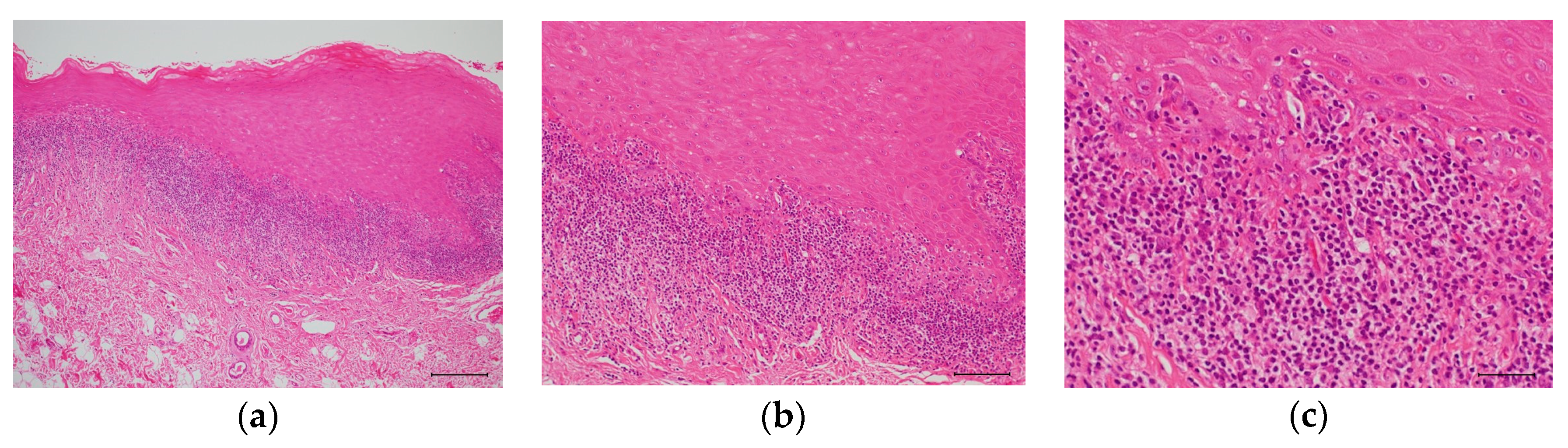
2.2. Oral Lichen Planus (OLP)
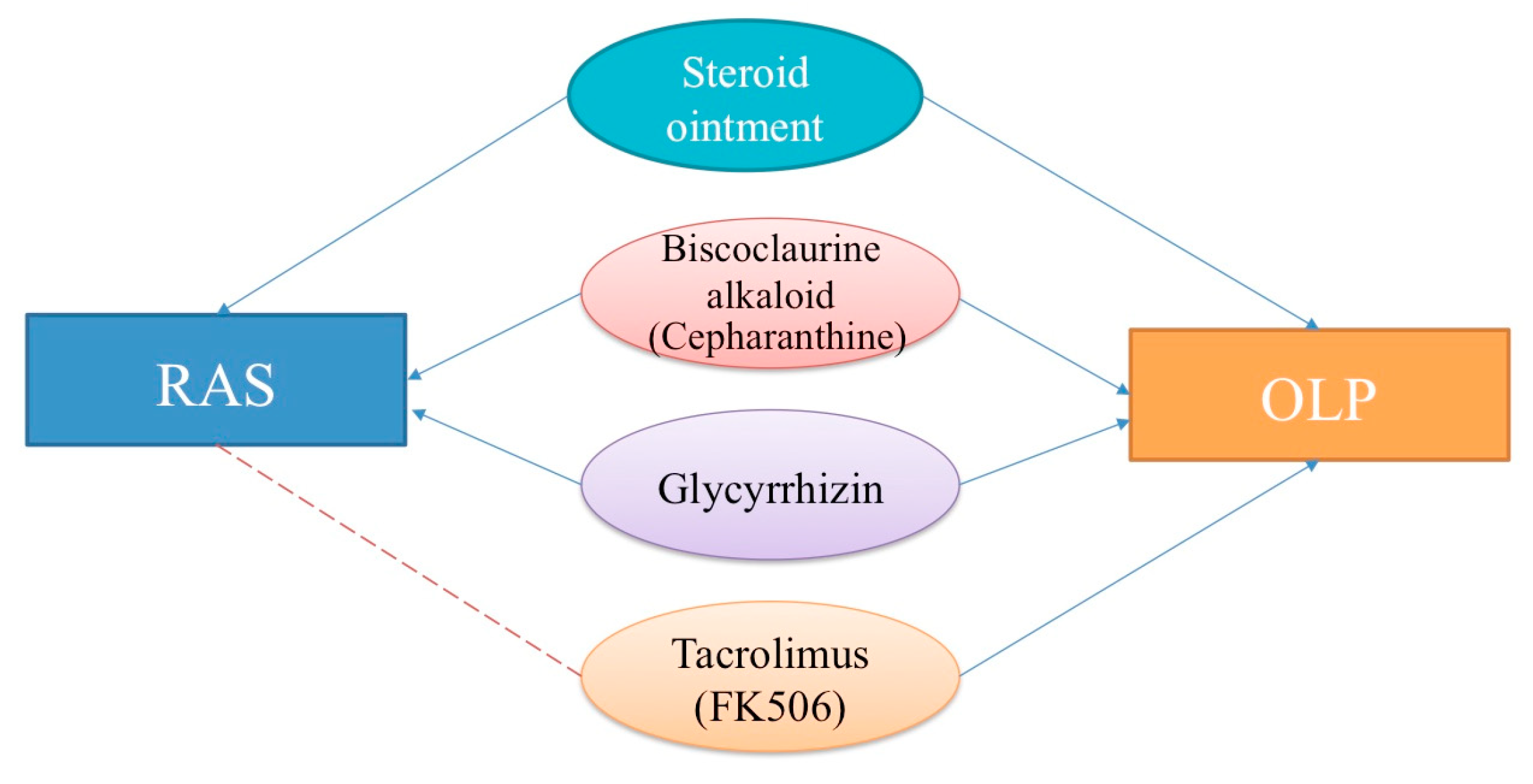
3. Topical or Systemic Therapeutic Agents for RAS and OLP
3.1. Glucocorticoids (Topical Use)
3.1.1. RAS
3.1.2. OLP
3.2. Biscoclaurine Alkaloid (BA) and Cepharanthine (CEP)
3.2.1. RAS
3.2.2. OLP
3.3. Glycyrrhizin (GL)
3.3.1. RAS
3.3.2. OLP
3.4. Tacrolimus (FK506: Topical Use)
3.5. Desiccants (Topical Use)
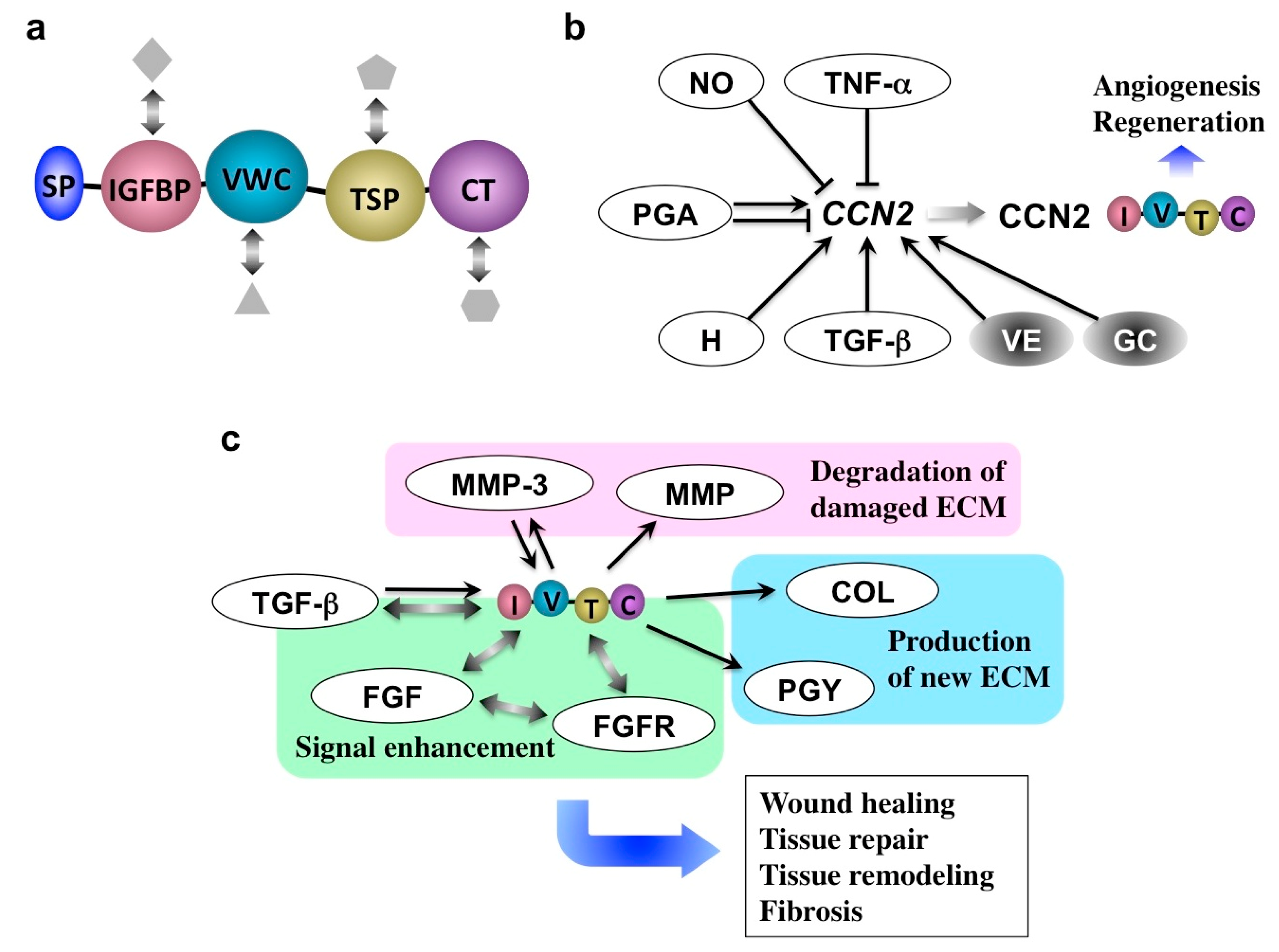
4. Role of CCN Family 2 (CCN2) in Inflammation
5. Novel Utility of Particular Glucocorticoid and Alkaloid in Orofacial Disorders
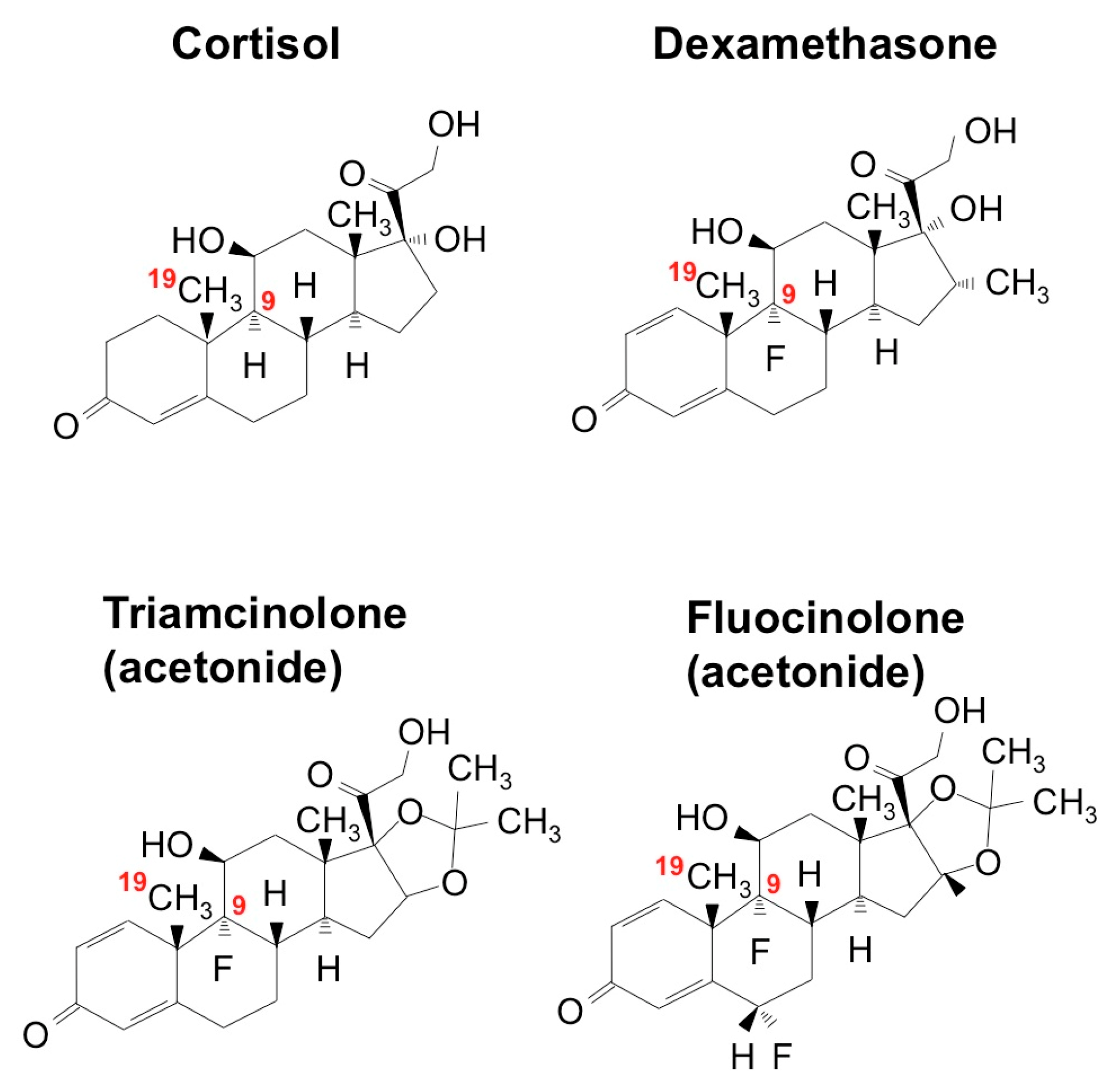
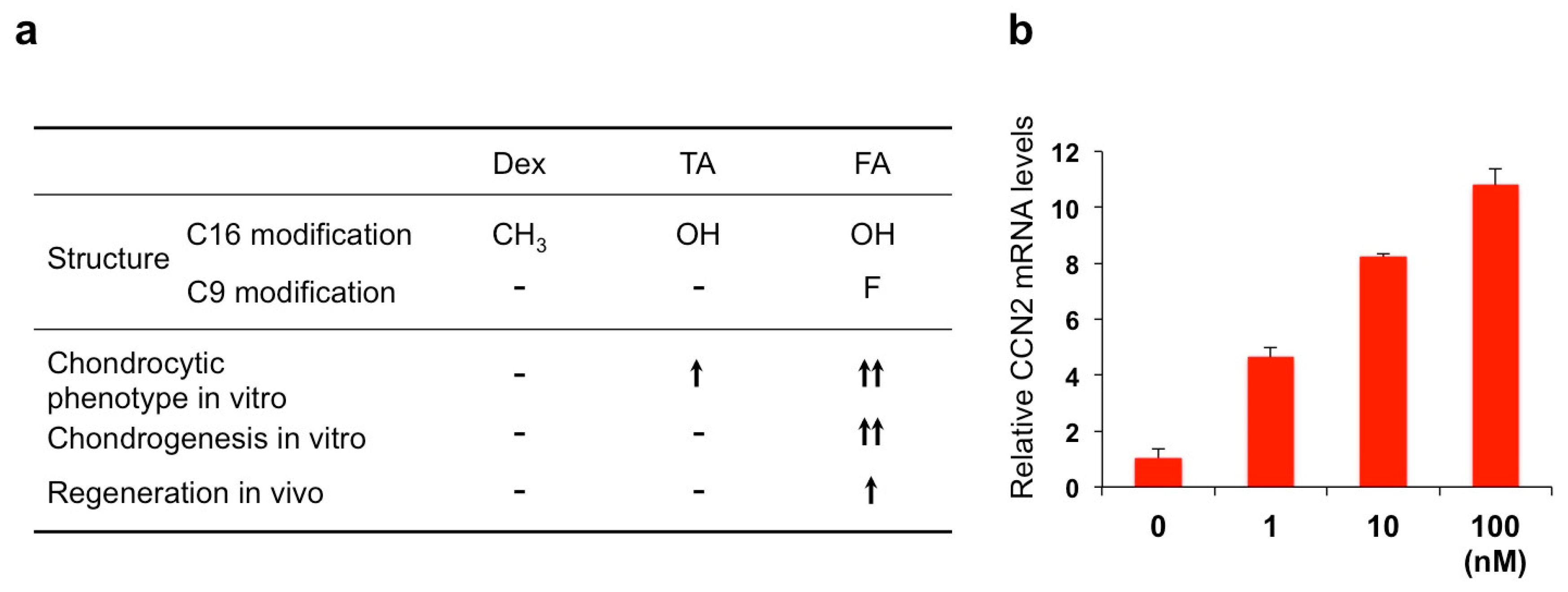
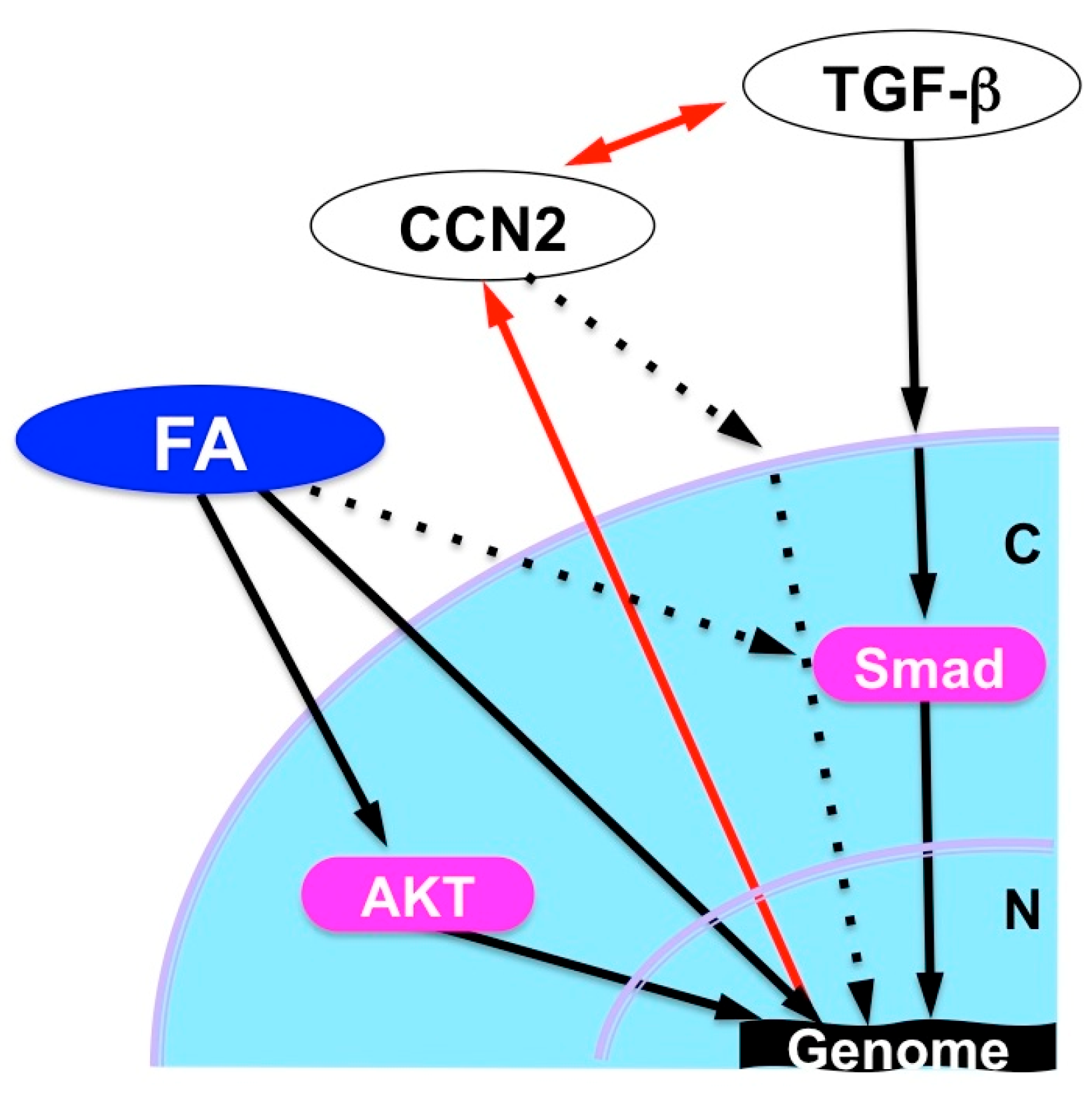
5.1. Fluocinolone Acetonide
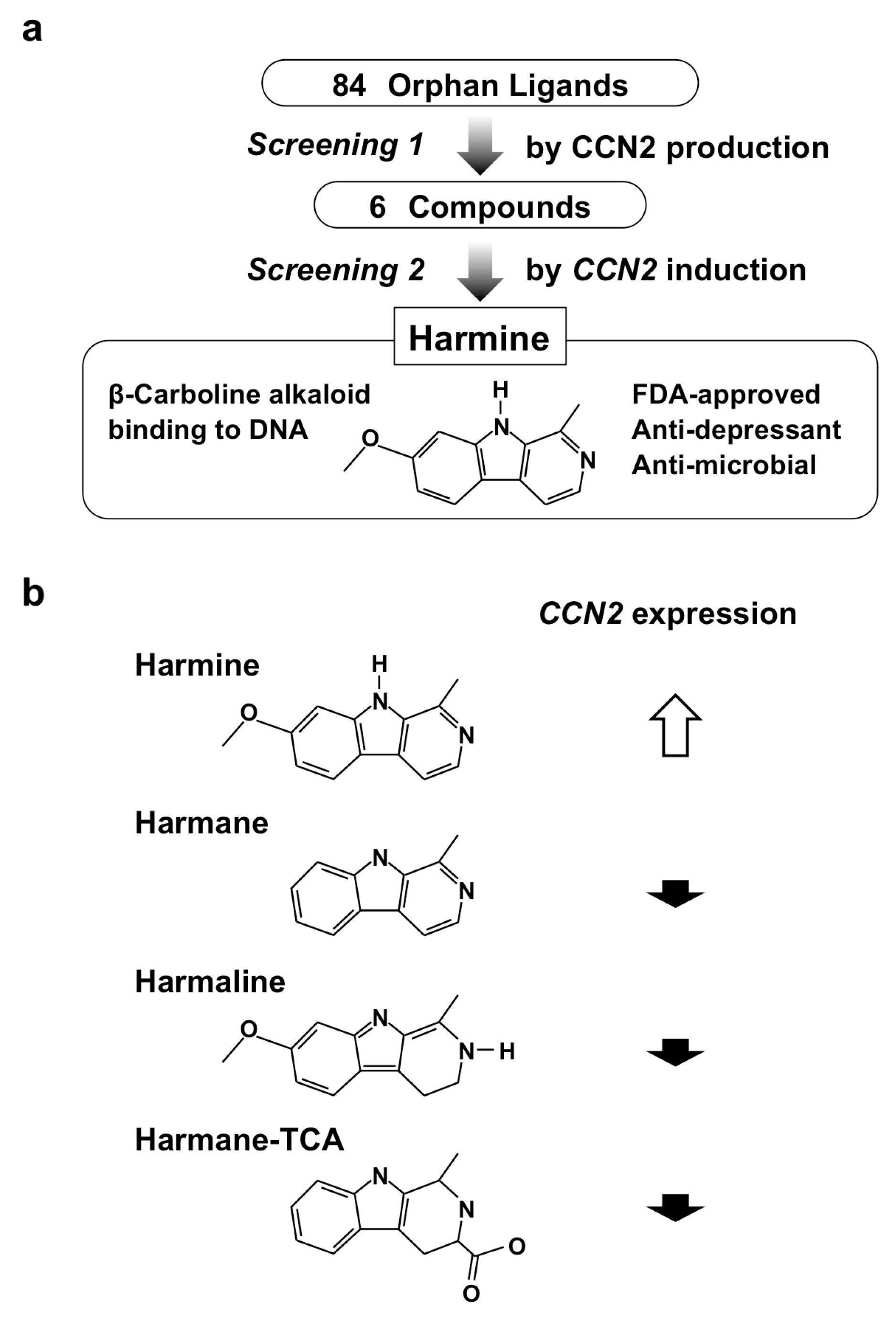
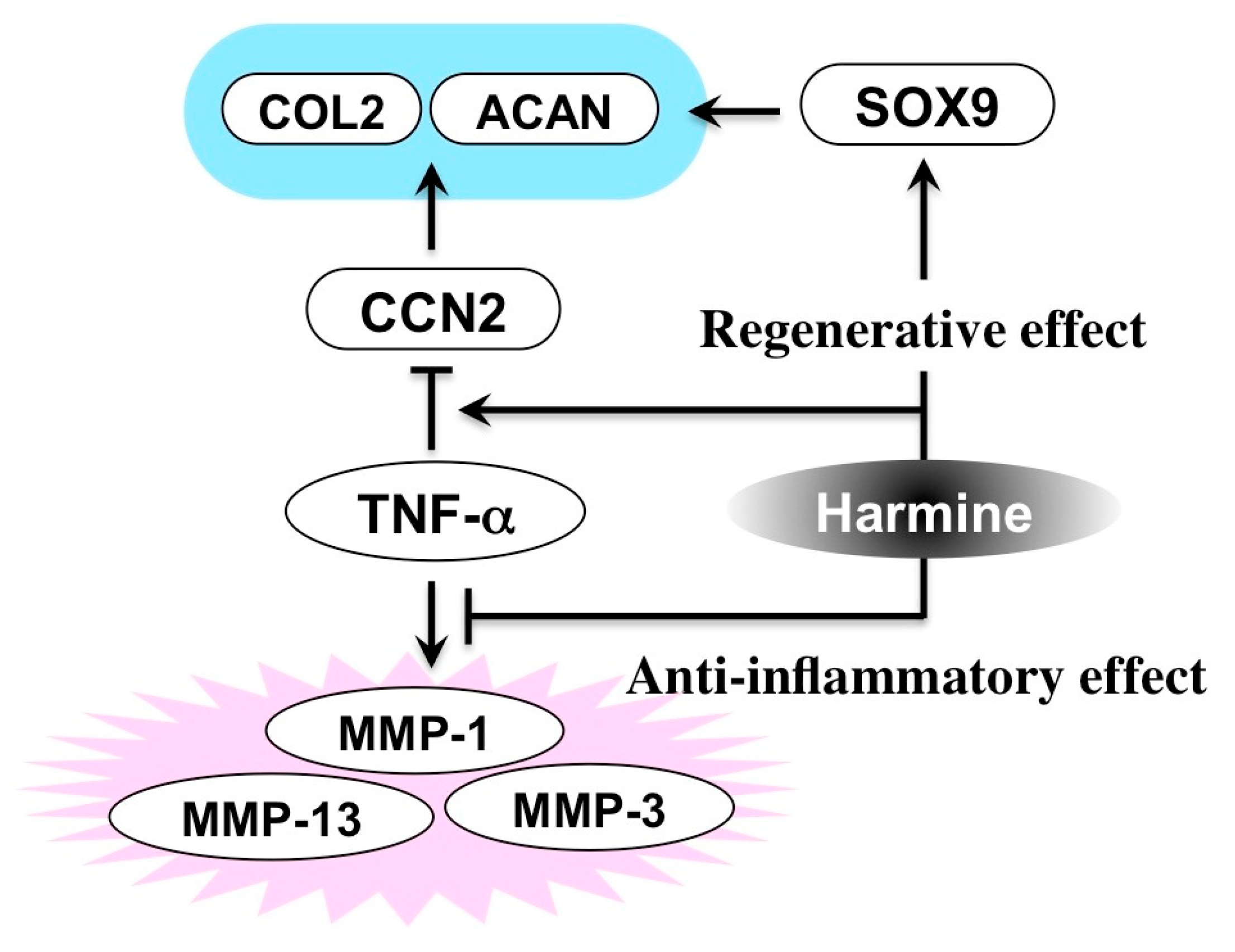
5.2. Harmine
6. Conclusive Remarks
Author Contributions
Funding
Conflicts of Interest
References
- Hayama, T.; Kamio, N.; Okabe, T.; Muromachi, K.; Matsushima, K. Kallikrein Promotes Inflammation in Human Dental Pulp Cells via Protease-Activated Receptor-1. J. Cell. Biochem. 2016, 117, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- Takashiba, S.; Naruishi, K.; Murayama, Y. Perspective of cytokine regulation for periodontal treatment: Fibroblast biology. J. Periodontol. 2003, 74, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Ugawa, Y.; Kawamura, M.; Yamashiro, K.; Kochi, S.; Ideguchi, H.; Takashiba, S. Modulation of microenvironment for controlling the fate of periodontal ligament cells: The role of Rho/ROCK signaling and cytoskeletal dynamics. J. Cell Commun. Signal. 2018, 12, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, G.; Williams, R.C.; Siciliano, V.I.; Alibrandi, A.; Cordasco, G.; Ramaglia, L. The effects of a desiccant agent in the treatment of chronic periodontitis: A randomized, controlled clinical trial. Clin. Oral Investig. 2018, 22, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, G.; Lo Giudice, G.; Briguglio, F.; Alibrandi, A.; Crupi, A.; Cordasco, G.; Ramaglia, L. A New Approach for the Treatment of Lateral Periodontal Cysts with an 810-nm Diode Laser. Int. J. Periodontics Restor. Dent. 2017, 37, e120–e129. [Google Scholar] [CrossRef] [PubMed]
- Matarese, G.; Ramaglia, L.; Cicciù, M.; Cordasco, G.; Isola, G. The Effects of diode laser therapy as an adjunct to scaling and root planing in the treatment of aggressive periodontitis: A 1-Year randomized controlled clinical trial. Photomed. Laser Surg. 2017, 35, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Marheineke, N.; Scherer, U.; Rücker, M.; von See, C.; Rahlf, B.; Gellrich, N.C.; Stoetzer, M. Evaluation of accuracy in implant site preparation performed in single- or multi-step drilling procedures. Clin. Oral Investig. 2018, 22, 2057–2067. [Google Scholar] [CrossRef] [PubMed]
- Natah, S.S.; Konttinen, Y.T.; Enattah, N.S.; Ashammakhi, N.; Sharkey, K.A.; Hayrinen-Immonen, R. Recurrent aphthous ulcers today: A review of the growing knowledge. Int. J. Oral Maxillofac. Surg. 2004, 33, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Femiano, F.; Lanza, A.; Buonaiuto, C.; Gombos, F.; Nunziata, M.; Piccolo, S.; Cirillo, N. Guidelines for diagnosis and management of aphthous stomatitis. Pediatr. Infect. Dis. J. 2007, 26, 728–732. [Google Scholar] [CrossRef] [PubMed]
- Kular, L.; Pakradouni, J.; Kitabgi, P.; Laurent, M.; Martinerie, C. The CCN family: A new class of inflammation modulators? Biochimie 2011, 93, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Mat, M.C.; Sevim, A.; Fresko, I.; Tuzun, Y. Behcet’s disease as a systemic disease. Clin. Dermatol. 2014, 32, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Kovac-Kovacic, M.; Skaleric, U. The prevalence of oral mucosal lesions in a population in Ljubljana, Slovenia. J. Oral Pathol. Med. 2000, 29, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Pentenero, M.; Broccoletti, R.; Carbone, M.; Conrotto, D.; Gandolfo, S. The prevalence of oral mucosal lesions in adults from the Turin area. Oral Dis. 2008, 14, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.B.; Kumar, S.K.; Zain, R.B. Oral lichen planus and lichenoid reactions: Etiopathogenesis, diagnosis, management and malignant transformation. J. Oral Sci. 2007, 49, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jawanda, M.K. Oral Lichen Planus: An Update on Etiology, Pathogenesis, Clinical Presentation, Diagnosis and Management. Indian J. Dermatol. 2015, 60, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Alrashdan, M.S.; Cirillo, N.; McCullough, M. Oral lichen planus: A literature review and update. Arch. Dermatol. Res. 2016, 308, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Schäcke, H.; Schottelius, A.; Döcke, W.D.; Strehlke, P.; Jaroch, S.; Schmees, N.; Rehwinkel, H.; Hennekes, H.; Asadullah, K. Dissociation of transactivation from transrepression by a selective glucocorticoid receptor agonist leads to separation of therapeutic effects from side effects. Proc. Natl. Acad. Sci. USA 2004, 101, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Lowenberg, M.; Stahn, C.; Hommes, D.W.; Buttgereit, F. Novel insights into mechanisms of glucocorticoid action and the development of new glucocorticoid receptor ligands. Steroids 2008, 73, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Stahn, C.; Lowenberg, M.; Hommes, D.W.; Buttgereit, F. Molecular mechanisms of glucocorticoid action and selective glucocorticoid receptor agonists. Mol. Cell. Endocrinol. 2007, 275, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Ueta, E.; Umazume, M.; Yamamoto, T.; Osaki, T. Leukocyte dysfunction in oral mucous membrane diseases. J. Oral Pathol. Med. 1993, 22, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Thongprasom, K.; Dhanuthai, K. Steriods in the treatment of lichen planus: A review. J. Oral Sci. 2008, 50, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Rogosnitzky, M.; Danks, R. Therapeutic potential of the biscoclaurine alkaloid, cepharanthine, for a range of clinical conditions. Pharmacol. Rep. 2011, 63, 337–347. [Google Scholar] [CrossRef]
- Akamatsu, H.; Komura, J.; Asada, Y.; Niwa, Y. Effects of cepharanthin on neutrophil chemotaxis, phagocytosis, and reactive oxygen species generation. J. Dermatol. 1991, 18, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Harada, T.; Kingetsu, A.; Nariai, Y.; Yoshimura, H. Effects of biscoclaurine alkaloids on clinical symptoms and superoxide anion generation from peripheral blood neutrophils in patients with oral lichen planus. Asian J. Oral Maxillofac. Surg. 2001, 13, 117–124. [Google Scholar]
- Shinnoki, S.; Morita, N.; Sumiyoshi, M.; Kawashima, N.; Wada, T.; Miyata, K.; Sakamoto, T. Effect of Cepharanthin on intractable oral mucosal disease (oral lichen planus, recurrent aphthous stomatitis). Dent. Outlook 1992, 80, 1223–1234. [Google Scholar]
- Harada, T.; Mishima, K.; Obara, S.; Yoshimura, Y. Effects of radiation therapy on superoxide anion generation from peripheral blood neutrophils in oromaxillary cancer patients: A preliminary report of radiation-induced oral mucositis. Asian J. Oral Maxillofac. Surg. 1996, 8, 9–14. [Google Scholar]
- Harada, T.; Nariai, Y.; Yoshimura, Y. Effects of biscoclaurine alkaloids (Cepharanthin) on patients with oral lichen planus. Study on superoxide anion generation from peripheral blood neutrophils and plasma cytokine levels in patients. Oral. Ther. Pharm. 2004, 23, 46–53. [Google Scholar]
- Asano, M.; Ohkubo, C.; Sasaki, A.; Sawanobori, K.; Nagano, H. Vasodilator effects of cepharanthine, a biscoclaurine alkaloid, on cutaneous microcirculation in the rabbit. J. Ethnopharmacol. 1987, 20, 107–120. [Google Scholar] [PubMed]
- Abe, N.; Ebina, T.; Ishida, N. Interferon induction by glycyrrhizin and glycyrrhetinic acid in mice. Microbiol. Immunol. 1982, 26, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Pompei, R.; Laconi, S.; Ingianni, A. Antiviral properties of glycyrrhizic acid and its semisynthetic derivatives. Mini Rev. Med. Chem. 2009, 9, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Patrick, L. Hepatitis C: Epidemiology and review of complementary/alternative medicine treatments. Altern. Med. Rev. 1999, 4, 220–238. [Google Scholar] [PubMed]
- Ohtsuki, K. The anti-inflammatory molecular mechanism of glycyrrhizin. Minophagen Med. Rev. 2010, 55, 95–118. [Google Scholar]
- Messier, C.; Epifano, F.; Genovese, S.; Grenier, D. Licorice and its potential beneficial effects in common oro-dental diseases. Oral Dis. 2012, 18, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Moghadamnia, A.A.; Motallebnejad, M.; Khanian, M. The efficacy of the bioadhesive patches containing licorice extract in the management of recurrent aphthous stomatitis. Phytother. Res. 2009, 23, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.D.; Sherman, J.; van der Ven, P.; Burgess, J. A controlled trial of a dissolving oral patch concerning glycyrrhiza (licorice) herbal extract for the treatment of aphthous ulcers. Gen. Dent. 2008, 56, 206–210. [Google Scholar] [PubMed]
- Das, S.K.; Das, V.; Gulati, A.K.; Singh, V.P. Deglycyrrhizinated liquorice in aphthous ulcers. J. Assoc. Phys. India 1989, 37, 647. [Google Scholar]
- Hashizume, K. A case of the oral lichen planus with alcoholic chronic hepatitis patients improved by glycyron tablets. Minophagen Med. Rev. 2007, 52, 352–354. [Google Scholar]
- Nagao, Y.; Sata, M.; Suzuki, H.; Tanikawa, K.; Itoh, K.; Kameyama, T. Effectiveness of glycyrrhizin for oral lichen planus in patients with chronic HCV infection. J. Gastroenterol. 1996, 31, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Graef, I.A.; Mermelstein, P.G.; Stankunas, K.; Neilson, J.R.; Deisseroth, K.; Tsien, R.W.; Crabtree, G.R. L-type calcium channels and GSK-3 regulate the activity of NF-ATc4 in hippocampal neurons. Nature 1999, 401, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Shichinohe, R.; Shibaki, A.; Nishie, W.; Tateishi, Y.; Shimizu, H. Successful treatment of severe recalcitrant erosive oral lichen planus with topical tacrolimus. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Morita, M.; Asoda, S.; Tsunoda, K.; Soma, T.; Nakagawa, T.; Shirakawa, M.; Shoji, H.; Yagishita, H.; Nishikawa, T.; Kawana, H. The onset risk of carcinoma in patients continuing tacrolimus topical treatment for oral lichen planus: A case report. Odontology 2017, 105, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.I.; Lau, L.F. Taking aim at the extracellular matrix: CCN proteins as emerging therapeutic targets. Nat. Rev. Drug Discov. 2011, 10, 945–963. [Google Scholar] [CrossRef] [PubMed]
- Kubota, S.; Takigawa, M. The CCN family acting throughout the body: Recent research developments. Biomol. Concepts 2013, 4, 477–494. [Google Scholar] [CrossRef] [PubMed]
- Perbal, B. The concept of the CCN protein family revisited: A centralized coordination network. J. Cell Commun. Signal. 2018, 12, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kubota, S.; Takigawa, M. The role of CCN2 in cartilage and bone development. J. Cell Commun. Signal. 2011, 5, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Abd El Kader, T.; Kubota, S.; Nishida, T.; Hattori, T.; Aoyama, E.; Janune, D.; Hara, E.S.; Ono, M.; Tabata, Y.; Kuboki, T.; et al. The regenerative effects of CCN2 independent modules on chondrocytes in vitro and osteoarthritis models in vivo. Bone 2014, 59, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues-Díez, R.; Rodrigues-Díez, R.R.; Rayego-Mateos, S.; Suarez-Alvarez, B.; Lavoz, C.; Stark Aroeira, L.; Sánchez-López, E.; Orejudo, M.; Alique, M.; Lopez-Larrea, C.; et al. The C-terminal module IV of connective tissue growth factor is a novel immune modulator of the Th17 response. Lab. Investig. 2013, 93, 812–824. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, T.; Kubota, S.; Kawata, K.; Mukudai, Y.; Uehara, J.; Ohgawara, T.; Ibaragi, S.; Sasaki, A.; Kuboki, T.; Takigawa, M. Novel transcription-factor-like function of human matrix metalloproteinase 3 regulating the CTGF/CCN2 gene. Mol. Cell. Biol. 2008, 28, 2391–2413. [Google Scholar] [CrossRef] [PubMed]
- Muromachi, K.; Kamio, N.; Narita, T.; Annen-Kamio, M.; Sugiya, H.; Matsushima, K. MMP-3 provokes CTGF/CCN2 production independently of protease activity and dependently on dynamin-related endocytosis, which contributes to human dental pulp cell migration. J. Cell. Biochem. 2012, 113, 1348–1358. [Google Scholar] [CrossRef] [PubMed]
- Leask, A. CCN2: A bona fide target for anti-fibrotic drug intervention. J. Cell Commun. Signal. 2011, 5, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Abd El Kader, T.; Kubota, S.; Janune, D.; Nishida, T.; Hattori, T.; Aoyama, E.; Perbal, B.; Kuboki, T.; Takigawa, M. Anti-fibrotic effect of CCN3 accompanied by altered gene expression profile of the CCN family. J. Cell Commun. Signal. 2013, 7, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kubota, S.; Takigawa, M. Cellular and molecular actions of CCN2/CTGF and its role under physiological and pathological conditions. Clin. Sci. 2015, 128, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Toda, N.; Mori, K.; Kasahara, M.; Koga, K.; Ishii, A.; Mori, K.P.; Osaki, K.; Mukoyama, M.; Yanagita, M.; Yokoi, H. Deletion of connective tissue growth factor ameliorates peritoneal fibrosis by inhibiting angiogenesis and inflammation. Nephrol. Dial. Transplant. 2018, 33, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Buajeeb, W.; Pobrurksa, C.; Kraivaphan, P. Efficacy of fluocinolone acetonide gel in the treatment of oral lichen planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2000, 89, 42–45. [Google Scholar] [CrossRef]
- Hara, E.S.; Ono, M.; Pham, H.T.; Sonoyama, W.; Kubota, S.; Takigawa, M.; Matsumoto, T.; Young, M.F.; Olsen, B.R.; Kuboki, T. Fluocinolone Acetonide Is a Potent Synergistic Factor of TGF-β3-Associated Chondrogenesis of Bone Marrow-Derived Mesenchymal Stem Cells for Articular Surface Regeneration. J. Bone Miner. Res. 2015, 30, 1585–1596. [Google Scholar] [CrossRef] [PubMed]
- Moloudizargari, M.; Mikaili, P.; Aghajanshakeri, S.; Asghari, M.H.; Shayegh, J. Pharmacological and therapeutic effects of Peganum harmala and its main alkaloids. Pharmacogn. Rev. 2013, 7, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Hara, E.S.; Ono, M.; Kubota, S.; Sonoyama, W.; Oida, Y.; Hattori, T.; Nishida, T.; Furumatsu, T.; Ozaki, T.; Takigawa, M.; et al. Novel chondrogenic and chondroprotective effects of the natural compound harmine. Biochimie 2013, 95, 374–381. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Names |
|---|
| aphthous stomatitis |
| recurrent aphthous stomatitis (RAS) (synonym: recurrent aphthous ulcer) |
| herpetic stomatitis |
| catarrhal stomatitis |
| drug-induced stomatitis |
| radiation-induced stomatitis |
| gangrenous stomatitis |
| nicotinic stomatitis |
| angular stomatitis (synonym: angular cheilitis) |
| denture-related stomatitis |
| Major Symptoms | Diseases |
|---|---|
| bulla/vesicle | herpetic stomatitis, herpes zoster, pemphigus, pemphigoid, epidermolysis bullosa hereditaria |
| erythema, erosion | erythroplakia, drug-induced stomatitis, radiation-induced stomatitis, angular stomatitis, oral candidiasis, OLP |
| ulcer | RAS, Behçet’s disease, gangrenous stomatitis, denture-related stomatitis |
| white spot/patch | leukoplakia, OLP, nicotinic stomatitis |
| pigmentation | Peutz–Jeghers syndrome, melanin pigmentation |
| atrophic disease | glossitis with anemia (e.g., Hunter’s glossitis) |
| Etiology | Diseases |
|---|---|
| Congenital or developmental anomalies | epidermolysis bullosa hereditaria, Peutz–Jeghers syndrome |
| Physical or chemical cause | drug-induced stomatitis, radiation-induced stomatitis, nicotinic stomatitis, denture-related stomatitis |
| Bacterial infection | angular stomatitis, gangrenous stomatitis |
| Mycotic infection | oral candidiasis, angular stomatitis |
| Viral infection | herpetic stomatitis, herpes zoster |
| Allergic disease | drug-induced stomatitis, Quincke’s edema |
| Autoimmune disease | pemphigus, pemphigoid |
| Precancerous lesion | erythroplakia, leukoplakia |
| Unidentified or complex cause | RAS, Behçet’s disease, OLP |
| Heredity/Genetic Factor |
| Local trauma such as sharp food and tooth-brushing |
| Adverse effect of drugs |
| Deficiency such as iron, zinc, vitamin B12, and folate |
| Smoking |
| Virus |
| Bacteria |
| Allergy |
| Hormonal change |
| Stress |
| Inflammatory digestive system disease |
| Immunological abnormality |
| Cardinal symptom of Behçet’s disease |
| Food hypersensitivity |
| Adverse Drug Reaction |
| Intraoral dental metal and filler |
| Intraoral cosmetics including preservatives, aromatic substances |
| Overwork and stress |
| Smoking |
| Hepatitis (hepatitis C in particular) |
| Oral candidiasis |
| Herpetic infection |
| Immunological abnormality |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moritani, N.H.; Hara, E.S.; Kubota, S. New Functions of Classical Compounds against Orofacial Inflammatory Lesions. Medicines 2018, 5, 118. https://doi.org/10.3390/medicines5040118
Moritani NH, Hara ES, Kubota S. New Functions of Classical Compounds against Orofacial Inflammatory Lesions. Medicines. 2018; 5(4):118. https://doi.org/10.3390/medicines5040118
Chicago/Turabian StyleMoritani, Norifumi H., Emilio Satoshi Hara, and Satoshi Kubota. 2018. "New Functions of Classical Compounds against Orofacial Inflammatory Lesions" Medicines 5, no. 4: 118. https://doi.org/10.3390/medicines5040118
APA StyleMoritani, N. H., Hara, E. S., & Kubota, S. (2018). New Functions of Classical Compounds against Orofacial Inflammatory Lesions. Medicines, 5(4), 118. https://doi.org/10.3390/medicines5040118