
Effects of Maternal Cigarette Smoking on Trace Element Levels and Steroidogenesis in the Maternal–Placental–Fetal Unit

 , , , , ,
, , , , ,  , , ,
, , ,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection
2.3. Cotinine and Creatinine Analysis
2.4. Element Analysis
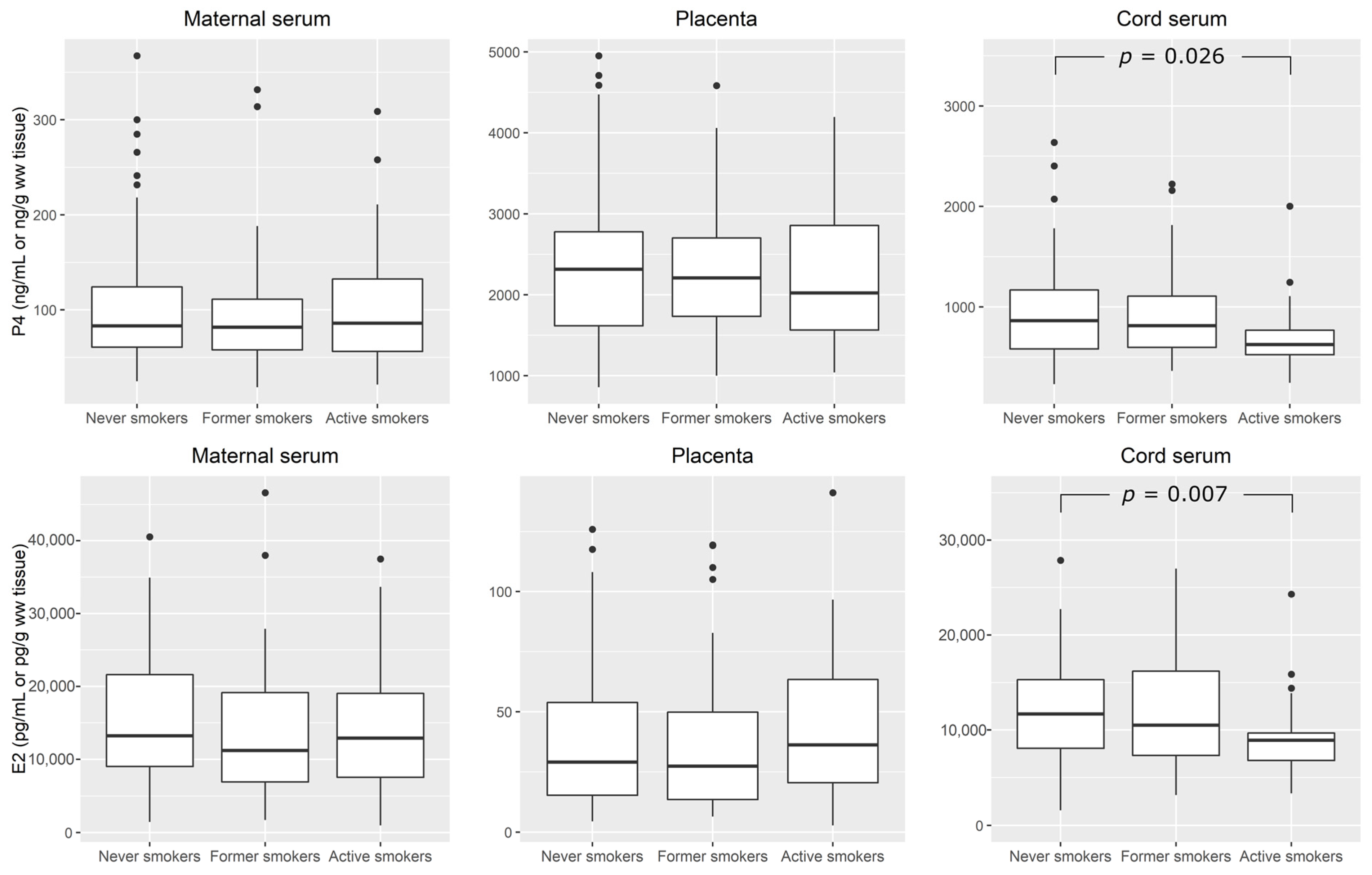
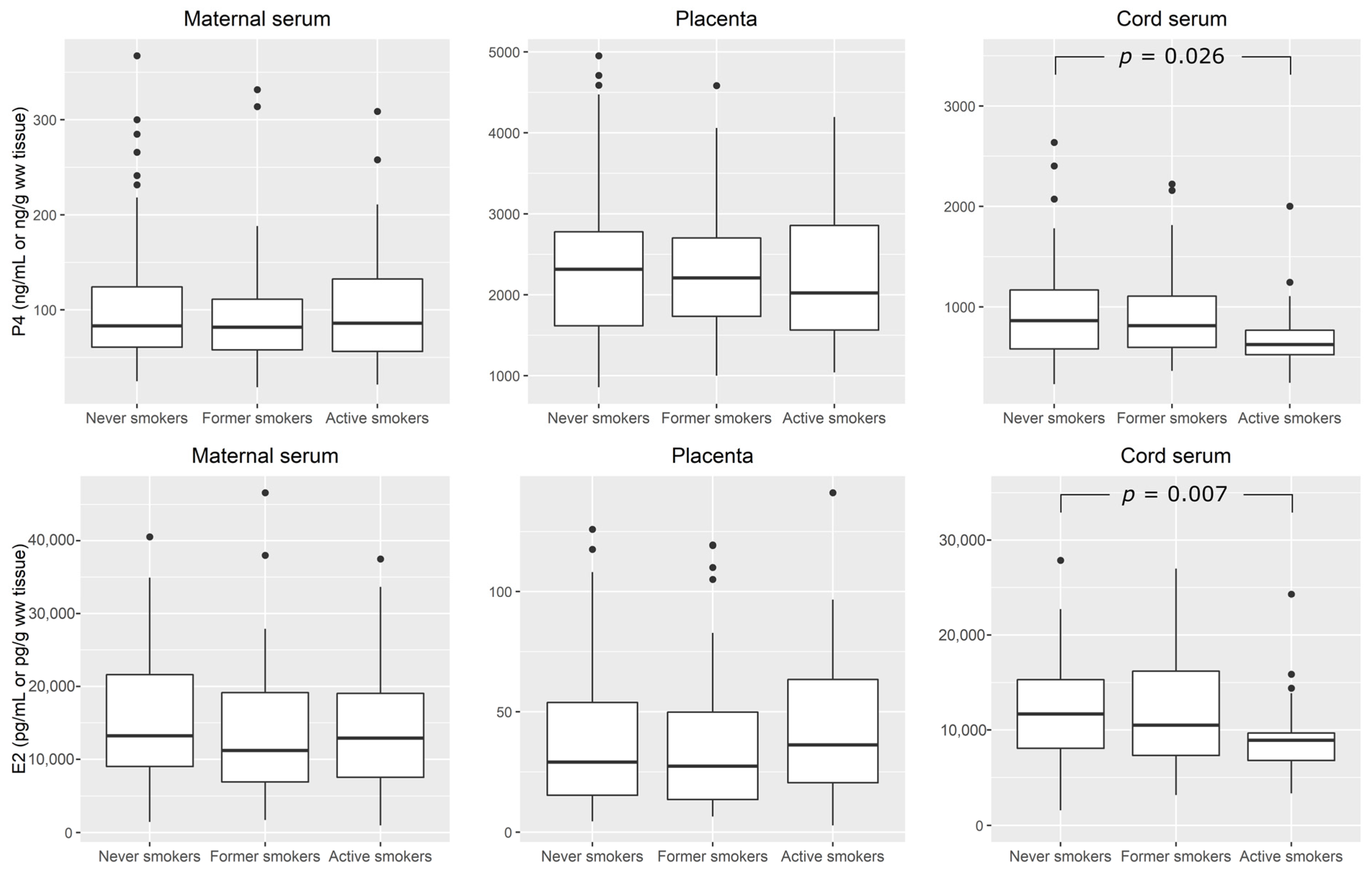
2.5. Progesterone and Estradiol Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Trace Elements in Mother–Infant Pairs
4.2. Cigarette Smoking, Trace Elements, and Steroid Hormones during Pregnancy
4.3. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stevenson, K.; Lillycrop, K.A.; Silver, M.J. Fetal programming and epigenetics. Curr. Opin. Endoc. Metabol. Res. 2020, 3, 1–6. [Google Scholar] [CrossRef]
- Gicquel, C.; El-Osta, A.; Le Bouc, Y. Epigenetic regulation and fetal programming. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 1–16. [Google Scholar] [CrossRef]
- Barker, D.J.; Gluckman, P.D.; Godfrey, K.M.; Harding, J.E.; Owens, J.A.; Robinson, J.S. Fetal nutrition and cardiovascular disease in adult life. Lancet 1993, 341, 938–941. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef]
- Haugen, A.C.; Schug, T.T.; Collman, G.; Heindel, J.J. Evolution of DOHaD: The impact of environmental health sciences. J. Dev. Orig. Health Dis. 2015, 6 (Suppl. S2), 55–64. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, G.F.; Costa, M. Handbook on the Toxicology of Metals, Volume I & II, 5th ed.; Academic Press: New York, NY, USA, 2022. [Google Scholar]
- Piasek, M.; Henson, M.C.; Blanuša, M.; Kostial, K. Assessment of steroid disruption and metal concentrations in human placenta: Effects of cigarette smoking. In Handbook of Smoking and Health (Public Health in the 21st Century); Koskinene, C.J., Ed.; Nova Science Publishers Inc.: New York, NY, USA, 2011; pp. 321–365. [Google Scholar]
- Smith, T.F.; Maccani, M.A.; Knopik, V.S. Symposium—Maternal smoking during pregnancy and offspring health outcomes: The role of epigenetic research in informing legal policy and practice. Hastings L. J. 2013, 64, 1619. [Google Scholar]
- Knopik, V.S.; Maccani, M.A.; Francazio, S.; McGeary, J.E. The epigenetics of maternal cigarette smoking during pregnancy and effects on child development. Dev. Psychopathol. 2012, 24, 1377–1390. [Google Scholar] [CrossRef]
- Maccani, J.Z.J.; Maccani, M.A. Altered placental DNA methylation patterns associated with maternal smoking, current perspectives. Adv. Genom. Genet. 2015, 2015, 205–214. [Google Scholar] [CrossRef]
- Morales-Prieto, D.M.; Fuentes-Zacarías, P.; Murrieta-Coxca, J.M.; Gutierrez-Samudio, R.N.; Favaro, R.R.; Fitzgerald, J.S.; Markert, U.R. Smoking for two- effects of tobacco consumption on placenta. Mol. Asp. Med. 2021, 87, 101023. [Google Scholar] [CrossRef]
- Crews, D.; McLachlan, J.A. Epigenetics, evolution, endocrine disruption, health, and disease. Endocrinology 2006, 147, S4–S10. [Google Scholar] [CrossRef]
- Henson, M.C.; Piasek, M.; Chedrese, P.J.; Castracane, V.D. Metal toxicity in mammalian reproduction. In Endocrine Toxicology, 3rd ed.; Eldridge, J.C., Stevens, J.T., Eds.; Target Organ Toxicology Series; Informa Healthcare Publishers: New York, NY, USA; London, UK, 2010; pp. 256–279. [Google Scholar]
- Iavicoli, I.; Fontana, L.; Bergamaschi, A. The effects of metals as endocrine disruptors. J. Toxicol. Environ. Health Part B 2009, 12, 206–223. [Google Scholar] [CrossRef] [PubMed]
- Gore, A.C.; Chappell, V.A.; Fenton, S.E.; Flaws, J.A.; Nadal, A.; Prins, G.S.; Toppari, J.; Zoeller, R.T. EDC–2: The Endocrine Society’s second scientific statement on endocrine-disrupting chemicals. Endocr. Rev. 2015, 36, E1–E150. [Google Scholar] [PubMed]
- Hill, M.; Pašková, A.; Kančeva, R.; Velíková, M.; Kubátová, J.; Kancheva, L.; Adamcová, K.; Mikešová, M.; Žižka, Z.; Koucký, M.; et al. Steroid profiling in pregnancy: A focus on the human fetus. J. Steroid. Biochem. Mol. Biol. 2014, 139, 201–222. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.L.; Auchus, R.J. The molecular biology, biochemistry, and physiology of human steroidogenesis and its disorders. Endocr. Rev. 2011, 32, 81–151. [Google Scholar] [PubMed]
- Sanderson, J.T. Placental and fetal steroidogenesis. Methods Mol. Biol. 2009, 550, 127–136. [Google Scholar] [PubMed]
- Tuckey, R.C. Progesterone synthesis by the human placenta. Placenta 2005, 26, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Pasqualini, J.R.; Chetrite, G.S. The formation and transformation of hormones in maternal, placental and fetal compartments, biological implications. Horm. Mol. Biol. Clin. Investig. 2016, 27, 11–28. [Google Scholar]
- McLachlan, J.A. Environmental signaling, from environmental estrogens to endocrine-disrupting chemicals and beyond. Andrology 2016, 4, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Needham, L.L. What additional factors beyond state-of-the-art analytical methods are needed for optimal generation and interpretation of biomonitoring data? Environ. Health Perspect. 2009, 117, 1481–1484. [Google Scholar] [CrossRef]
- Esteban, M.; Castaño, A. Non-invasive matrices in human biomonitoring: A review. Environ. Int. 2009, 35, 438–449. [Google Scholar]
- Knudsen, L.E.; Merlo, F.D.; Larsen, A.D. Ethics and communication in human biomonitoring: European perspectives. Workshop on ethics and communication in Copenhagen, Denmark, 11–13 March 2007. Environ. Health 2008, 7 (Suppl. S1), S1–S13. [Google Scholar] [CrossRef]
- World Health Organization. Human Biomonitoring: Facts and Figures; WHO Regional Office for Europe: Copenhagen, Denmark, 2015; Available online: https://apps.who.int/iris/handle/10665/164588 (accessed on 30 June 2023).
- Smolders, R.; Schramm, K.-W.; Stenius, U.; Grellier, J.; Khan, A.; Trnovec, T.; Sram, R.; Schoeters, G. A review on the practical application of human biomonitoring in integrated environmental health impact assessment. J. Toxicol. Environ Health B 2009, 12, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, T.W.; Nordberg, G.F.; Sager, P.R. Biological monitoring of metals with special references to the early stages of the life cycle. J. UOEH 1987, 9, 50–58. [Google Scholar] [PubMed]
- Miller, R.K.; Mattison, D.R.; Plowchalk, D. Biological monitoring of the human placenta. In Biological Monitoring of Toxic Metals; Clarkson, T.W., Friberg, L., Nordberg, G.F., Sager, P.R., Eds.; Plenum Press: New York, NY, USA, 1988; pp. 567–602. [Google Scholar]
- Esteban-Vasallo, M.D.; Aragonés, N.; Pollan, M.; López-Abente, G.; Perez-Gomez, B. Mercury, cadmium, and lead levels in human placenta: A systematic review. Environ. Health Perspect. 2012, 120, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, G.V.; Rapp, A. Human placenta as a ‘dual’ biomarker for monitoring fetal and maternal environment with special reference to potentially toxic trace elements. Part 2: Essential minor, trace and other (non-essential) elements in human placenta. Sci. Total Environ. 2001, 280, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Lagerkvist, B.J.; Sandberg, S.; Frech, W.; Jin, T.; Nordberg, G.F. Is placenta a good indicator of cadmium and lead exposure? Arch. Environ. Health 1996, 51, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Myllynen, P.; Pasanen, M.; Pelkonen, O. Human placenta: A human organ for developmental toxicology research and biomonitoring. Placenta 2005, 26, 361–371. [Google Scholar]
- Piasek, M.; Blanuša, M.; Kostial, K.; Laskey, J.W. Placental cadmium and progesterone concentrations in cigarette smokers. Reprod. Toxicol. 2001, 156, 673–681. [Google Scholar]
- Piasek, M.; Laskey, J.W.; Kostial, K.; Blanuša, M. Assessment of steroid disruption using cultures of whole ovary and/or placenta in rat and in human placental tissue. Int. Arch. Occup. Environ. Health 2002, 75, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Piasek, M.; Mikolić, A.; Sekovanić, A.; Sulimanec Grgec, A.; Jurasović, J. Cadmium in placenta—A valuable biomarker of exposure during pregnancy in biomedical research. J. Toxicol. Environ. Health A 2014, 77, 1071–1074. [Google Scholar] [CrossRef]
- Sekovanić, A.; Jurasović, J.; Piasek, M.; Pašalić, D.; Orct, T.; Sulimanec Grgec, A.; Stasenko, S.; Branović Čakanić, K.; Jazbec, A. Metallothionein 2A gene polymorphism and trace elements in mother-newborn pairs in the Croatian population. J. Trace Elem. Med. Biol. 2018, 45, 163–170. [Google Scholar]
- Pizent, A.; Lazarus, M.; Kovačić, J.; Tariba Lovaković, B.; Brčić Karačonji, I.; Živković Semren, T.; Sekovanić, A.; Orct, T.; Branović-Čakanić, K.; Brajenović, N.; et al. Cigarette smoking during pregnancy: Effects on antioxidant enzymes, metallothionein and trace elements in mother-newborn pairs. Biomolecules 2020, 10, 892. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.F.; Choudhuri, S.; Muldoon-Jacobs, K. Epigenetic targets of some toxicologically relevant metals: A review of the literature. J. Appl. Toxicol. 2012, 32, 643–653. [Google Scholar] [CrossRef]
- Thompson, L.P.; Al-Hasan, Y. Impact of oxidative stress in fetal programming. J. Pregnancy 2012, 2012, 582748. [Google Scholar] [CrossRef] [PubMed]
- Stasenko, S.; Bradford, E.M.; Piasek, M.; Henson, M.C.; Varnai, V.M.; Jurasović, J.; Kušec, V. Metals in human placenta: Focus on the effects of cadmium on steroid hormones and leptin. J. Appl. Toxicol. 2010, 30, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Health Interview Survey—Glossary. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 1 June 2023).
- Brčić Karačonji, I.; Skender, L.; Karačić, V. Determination of nicotine and cotinine in urine by headspace solid phase microextraction gas chromatography with mass spectrometric detection. Acta Chim. Slov. 2007, 54, 74–78. [Google Scholar]
- Heindel, J.J. Role of exposure to environmental chemicals in the developmental basis of reproductive disease and dysfunction. Semin. Reprod. Med. 2006, 24, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Heindel, J.J.; Balbus, J.; Birnbaum, L.; Brune-Drisse, M.N.; Grandjean, P.; Gray, K.; Landrigan, P.J.; Sly, P.D.; Suk, W.; Cory Slechta, D.; et al. Developmental origins of health and disease: Integrating environmental influences. Endocrinology 2015, 156, 3416–3421. [Google Scholar]
- Arbuckle, T.E.; Liang, C.L.; Fisher, M.; Caron, N.J.; Fraser, W.D.; MIREC Study Group. Exposure to tobacco smoke and validation of smoking status during pregnancy in the MIREC study. J. Expo. Sci. Environ. Epidemiol. 2018, 28, 461–469. [Google Scholar] [CrossRef]
- Nordberg, G.F.; Bernard, A.; Diamond, G.L.; Duffus, J.H.; Illing, P.; Nordberg, M.; Bergdahl, I.A.; Jin, T.; Skerfving, S. Risk assessment of effects of cadmium on human health (IUPAC Technical Report). J. Pure Appl. Chem. 2018, 90, 755–808. [Google Scholar]
- Lamkarkach, F.; Ougier, E.; Garnier, R.; Viau, C.; Kolossa-Gehring, M.; Lange, R.; Apel, P. Human biomonitoring initiative (HBM4EU): Human biomonitoring guidance values (HBM-GVs) derived for cadmium and its compounds. Environ. Int. 2021, 147, 106337. [Google Scholar] [CrossRef] [PubMed]
- Baeyens, W.; Vrijens, J.; Gao, Y.; Croes, K.; Schoeters, G.; Den Hond, E.; Sioen, I.; Bruckers, L.; Nawrot, T.; Nelen, V.; et al. Trace metals in blood and urine of newborn/mother pairs, adolescents and adults of the Flemish population (2007–2011). Int. J. Hyg. Environ. Health 2014, 217, 878–890. [Google Scholar] [CrossRef]
- Arbuckle, T.E.; Liang, C.L.; Morisset, A.S.; Fisher, M.; Weiler, H.; Cirtiu, C.M.; Legrand, M.; Davis, K.; Ettinger, A.S.; Fraser, W.D.; et al. Maternal and fetal exposure to cadmium, lead, manganese and mercury: The MIREC study. Chemosphere 2016, 163, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Report on Human Exposure to Environmental Chemicals. Biomonitoring Data Tables for Environmental Chemicals; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. Available online: https://www.cdc.gov/exposurereport/data_tables.html (accessed on 1 June 2023).
- European Chemicals Agency. ECHA Scientific Report for Evaluation of Limit Values for Cadmium and Its Inorganic Compounds at the Workplace; European Chemicals Agency: Helsinki, Finland, 2020. Available online: https://echa.europa.eu/documents/10162/2c23f940-fff8-59ab-43b1-05aadb30042e (accessed on 1 June 2023).
- Bergdahl, I.A.; Skerfving, S. Lead, Ch. 19. In Handbook on the Toxicology of Metals, 5th ed.; Nordberg, G.F., Costa, M., Eds.; Academic Press: New York, NY, USA, 2022; Volume II: Specific Metals, pp. 427–493. [Google Scholar]
- Barbosa, F., Jr.; Tanus-Santos, J.E.; Gerlach, R.F.; Parsons, P.J. A critical review of biomarkers used for monitoring human exposure to lead: Advantages, limitations, and future needs. Environ. Health Perspect. 2005, 113, 1669–1674. [Google Scholar] [CrossRef] [PubMed]
- Kljaković-Gašpić, Z.; Pizent, A.; Jurasović, J. Influence of abatement of lead exposure in Croatia on blood lead and ALAD activity. Environ. Sci. Pollut. Res. 2016, 23, 898–907. [Google Scholar]
- Lermen, D.; Weber, T.; Göen, T.; Bartel-Steinbach, M.; Gwinner, F.; Mueller, S.C.; Conrad, A.; Rüther, M.; von Briesen, H.; Kolossa-Gehring, M. Long-term time trend of lead exposure in young German adults—Evaluation of more than 35 Years of data of the German Environmental Specimen Bank. Int. J. Hyg. Environ. Health 2021, 231, 113665. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, M.; Lundh, T.; Sommar, J.N.; Bergdahl, I.A. Time trends and exposure determinants of lead and cadmium in the adult population of northern Sweden 1990–2014. Environ. Res. 2017, 159, 111–117. [Google Scholar] [CrossRef]
- Bocca, B.; Ruggieri, F.; Pino, A.; Rovira, J.; Calamandrei, G.; Martínez, M.Á.; Domingo, J.L.; Alimonti, A.; Schuhmacher, M. Human biomonitoring to evaluate exposure to toxic and essential trace elements during pregnancy. Part A. concentrations in maternal blood, urine and cord blood. Environ. Res. 2019, 177, 108599. [Google Scholar] [CrossRef]
- European Food Safety Authority. Panel on contaminants in the food chain: Scientific opinion on lead in food. EFSA J. 2010, 8, 1570. [Google Scholar]
- Piasek, M.; Jurasović, J.; Sekovanić, A.; Brajenović, N.; Brčić Karačonji, I.; Mikolić, A.; Sulimanec Grgec, A.; Stasenko, S. Placental cadmium as an additional noninvasive bioindicator of active maternal tobacco smoking. J. Toxicol. Environ. Health A 2016, 79, 443–446. [Google Scholar] [CrossRef]
- Mazurek, D.; Łoźna, K.; Bronkowska, M. The concentration of selected elements in the placenta according to selected sociodemographic factors and their effect on birth mass and birth length of newborns. J. Trace Elem. Med. Biol. 2020, 58, 126425. [Google Scholar] [CrossRef] [PubMed]
- Northrop-Clewes, C.A.; Thurnham, D.I. Monitoring micronutrients in cigarette smokers. Clin. Chim. Acta 2007, 377, 14–38. [Google Scholar] [CrossRef] [PubMed]
- Ashford, K.; Rayens, E.; Wiggins, A.T.; Rayens, M.K.; Malany Sayre, M.; O’Brien, J. Associations of demographic factors and tobacco use with progesterone and estradiol during pregnancy. SAGE Open Nurs. 2018, 4, 2377960818806285. [Google Scholar] [CrossRef] [PubMed]
- Henson, M.C.; Chedrese, P.J. Endocrine disruption by cadmium, a common environmental toxicant with paradoxical effects on reproduction. Exp. Biol. Med. 2004, 229, 383–392. [Google Scholar] [CrossRef]
- Soldin, O.P.; Makambi, K.H.; Soldin, S.J.; O’Mara, D.M. Steroid hormone levels associated with passive and active smoking. Steroids 2011, 76, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Ernst, A.; Kristensen, S.L.; Toft, G.; Thulstrup, A.M.; Håkonsen, L.B.; Olsen, S.F.; Ramlau-Hansen, C.H. Maternal smoking during pregnancy and reproductive health of daughters: A follow-up study spanning two decades. Hum. Reprod. 2012, 27, 3593–3600. [Google Scholar] [CrossRef]
- Ramlau-Hansen, C.H.; Thulstrup, A.M.; Olsen, J.; Ernst, E.; Andersen, C.Y.; Bonde, J.P. Maternal smoking in pregnancy and reproductive hormones in adult sons. Int. J. Androl. 2008, 31, 565–572. [Google Scholar] [CrossRef]
- Hollier, L.P.; Keelan, J.A.; Hickey, M.; Maybery, M.T.; Whitehouse, A.J.O. Measurement of androgen and estrogen concentrations in cord blood: Accuracy, biological interpretation, and applications to understanding human behavioral development. Front Endocrinol. 2014, 5, 64. [Google Scholar] [CrossRef]
- Rivera-Núñez, Z.; Ashrap, P.; Barrett, E.S.; Watkins, D.J.; Cathey, A.L.; Vélez-Vega, C.M.; Rosario, Z.; Cordero, J.F.; Alshawabkeh, A.; Meeker, J.D. Association of biomarkers of exposure to metals and metalloids with maternal hormones in pregnant women from Puerto Rico. Environ. Int. 2021, 147, 106310. [Google Scholar] [CrossRef]
- Lagiou, P.; Hsieh, C.-C.; Samoli, E.; Lagiou, A.; Biao, X.; Yu, G.-P.; Onoyama, S.; Chie, L.; Vatten, L.J.; Adami, H.-O.; et al. Associations of placental weight with maternal and cord blood hormones. Ann. Epidemiol. 2013, 23, 669–673. [Google Scholar] [CrossRef]
- Lagiou, P.; Samoli, E.; Hsieh, C.-C.; Lagiou, A.; Xu, B.; Yu, G.-P.; Onoyama, S.; Adami, H.-O.; Vatten, L.J.; Trichopoulos, D.; et al. Maternal and cord blood hormones in relation to birth size. Eur. J. Epidemiol. 2014, 29, 343–351. [Google Scholar] [CrossRef]
- Hickey, M.; Hart, R.; Keelan, J.A. The relationship between umbilical cord estrogens and perinatal characteristics. Cancer Epidemiol. Biomark. Prev. 2014, 23, 946–952. [Google Scholar] [CrossRef]
- Varvarigou, A.A.; Liatsis, S.G.; Vassilakos, P.; Decavalas, G.; Beratis, N.G. Effect of maternal smoking on cord blood estriol, placental lactogen, chorionic gonadotropin, FSH, LH, and cortisol. J. Perinat. Med. 2009, 37, 364–369. [Google Scholar] [CrossRef]
- Adamcová, K.; Kolátorová, L.; Chlupáčová, T.; Šimková, M.; Jandíková, H.; Pařízek, A.; Stárka, L.; Dušková, M. Changes to fetal steroidogenesis caused by maternal smoking. Physiol. Res. 2017, 66, 375–386. [Google Scholar] [CrossRef]

{kind=link}
| Never Smokers (n = 71) | Former Smokers (n = 48) | Active Smokers (n = 36) | p | |
|---|---|---|---|---|
| Maternal characteristics | ||||
| Age (years) | 33 (21–44) a | 33 (24–42) a | 29 (21–38) b | 0.007 |
| Education | 0.0002 | |||
| Primary school | 3 (4.2%) | 2 (4.2%) | 5 (14%) | |
| Secondary school | 25 (35%) | 21 (44%) | 25 (69%) | |
| University degree | 43 (61%) | 25 (52%) | 6 (17%) | |
| Prepregnancy BMI (kg/m2) | 24 ± 3.9 23 (16–36) | 24 ± 3.3 23 (18–31) | 23 ± 4.5 23 (15–37) | 0.874 |
| BMI ≤ 18.5/18.5–24.9/≥ 25 (n) | 2/48/21 | 2/30/16 | 5/19/12 | |
| Weight gain during pregnancy (kg) | 14 ± 4.5 13 (4.0–24) | 15 ± 6.3 14 (5.0–38) | 15 ± 5.3 14 (6.0–30) | 0.763 |
| Parity | 2 (1–6) | 2 (1–4) | 2 (1–6) | 0.097 |
| Smoking habit † | ||||
| Started smoking (age, years) | / | 21 (15–32) a | 18 (11–27) b | 0.005 |
| Smoking duration (years) | / | 8 (2–21) | 10 (2–20) | 0.073 |
| Smoking index 1 | / | 86 (28–202) | 98 (2–235) | 0.733 |
| Passive smoking (n) | 39 | 23 | 25 | 0.081 |
| Cotinine in urine (µg/g creatinine) | 1.6 (0.1–22) a | 4.9 (0.1–502) a | 1315 (2.6–5660) b | <0.001 |
| Newborn characteristics | ||||
| All newborns | ||||
| Birth weight (g) | 3602 ± 504 | 3603 ± 511 | 3410 ± 433 | 0.159 |
| Birth length (cm) | 51 ± 1.8 | 51 ± 2.2 | 51 ± 1.9 | 0.471 |
| Trimmed placental weight (g) | 409 ± 90 | 397 ± 89 | 408 ± 76 | 0.493 |
| Birth weight:placental weight ratio | 9.1 ± 1.8 a,b | 9.3 ± 1.3 a | 8.5 ± 1.3 b | 0.015 |
| Boys/Girls, n | 46/25 | 25/23 | 23/13 | 0.356 |
| Girls | ||||
| Birth weight (g) | 3413 ± 502 | 3476 ± 379 | 3344 ± 392 | 0.444 |
| Birth length (cm) | 50 ± 1.9 | 50 ± 1.9 | 50 ± 1.4 | 0.839 |
| Trimmed placental weight (g) | 405 ± 90 | 385 ± 65 | 402 ± 63 | 0.635 |
| Birth weight:placental weight ratio | 8.6 ± 1.3 | 9.2 ± 1.1 | 8.4 ± 0.93 | 0.084 |
| Boys | ||||
| Birth weight (g) | 3704 ± 480 | 3720 ± 591 | 3448 ± 459 | 0.148 |
| Birth length (cm) | 51 ± 1.7 | 51 ± 2.4 | 50 ± 2.2 | 0.298 |
| Trimmed placental weight (g) | 411 ± 92 | 408 ± 106 | 411 ± 84 | 0.826 |
| Birth weight:placental weight ratio | 9.3 ± 1.9 | 9.4 ± 1.5 | 8.6 ± 1.5 | 0.095 |
| Never Smokers (n = 71) | Former Smokers (n = 48) | Active Smokers (n = 36) | p | |
|---|---|---|---|---|
| Cadmium (Cd) | ||||
| Maternal urine (µg/g creatinine) | 0.25 ± 0.12 0.22 (0.15–0.32) a | 0.31 ± 0.19 0.25 (0.19–0.37) a,b | 0.34 ± 0.18 0.32 (0.23–0.40) b | 0.004 |
| Maternal blood (µg/L) | 0.28 ± 0.13 0.25 (0.19–0.34) a | 0.35 ± 0.18 0.31 (0.21–0.47) a | 1.3 ± 1.6 0.68 (0.52–1.2) b | <0.001 |
| Placenta (µg/kg) | 6.0 ± 2.5 5.4 (4.3–7.7) a | 7.3 ± 3.2 6.6 (4.8–9.2) a,b | 9.0 ± 4.3 7.9 (5.6–12) b | 0.001 |
| Cord blood (µg/L) | 0.02 ± 0.01 0.02 (0.01–0.03) a | 0.02 ± 0.01 0.02 (0.01–0.03) a | 0.03 ± 0.01 0.03 (0.02–0.04) b | <0.001 |
| Lead (Pb) | ||||
| Maternal urine (µg/g creatinine) | 0.57 ± 0.24 0.53 (0.38–0.73) | 0.59 ± 0.31 0.56 (0.36–0.74) | 0.66 ± 0.30 0.65 (0.45–0.78) | 0.226 |
| Maternal blood (µg/L) | 9.3 ± 4.5 7.9 (6.1–11) | 8.9 ± 4.1 8.7 (5.9–11) | 10 ± 3.5 9.3 (8.0–11) | 0.133 |
| Placenta (µg/kg) | 2.2 ± 2.0 1.6 (1.1–2.5) a | 2.5 ± 1.8 2.1 (1.4–3.0) a,b | 3.1 ± 2.1 2.5 (1.8–3.5) b | 0.002 |
| Cord blood (µg/L) | 6.1 ± 2.7 5.8 (4.1–7.2) | 6.4 ± 3.4 5.8 (4.3–8.2) | 6.8 ± 2.4 6.6 (5.2–8.1) | 0.164 |
| Never Smokers (n = 71) | Former Smokers (n = 48) | Active Smokers (n = 36) | p | |
|---|---|---|---|---|
| Iron (Fe) | ||||
| Maternal urine (mg/g creatinine) | 0.03 ± 0.03 0.02 (0.01–0.03) | 0.03 ± 0.03 0.03 (0.02–0.04) | 0.02 ± 0.02 0.02 (0.01–0.02) | 0.061 |
| Maternal blood (mg/L) | 443 ± 60 458 (410–480) | 428 ± 70 445 (391–474) | 433 ± 48 437 (404–467) | 0.324 |
| Placenta (mg/kg) | 104 ± 29 99 (79–122) a | 111 ± 34 108 (86–129) a | 89 ± 27 85 (65–109) b | 0.004 |
| Cord blood (mg/L) | 575 ± 64 574 (532–613) | 580 ± 74 583 (548–640) | 561 ± 53 567 (524–592) | 0.173 |
| Zinc (Zn) | ||||
| Maternal urine (mg/g creatinine) | 0.46 ± 0.24 0.44 (0.27–0.58) | 0.47 ± 0.23 0.45 (0.31–0.55) | 0.58 ± 0.36 0.47 (0.32–0.78) | 0.372 |
| Maternal blood (mg/L) | 6.2 ± 0.84 6.4 (5.7–6.7) | 6.0 ± 0.95 6.0 (5.5–6.5) | 6.0 ± 0.73 6.1 (5.7–6.6) | 0.112 |
| Placenta (mg/kg) | 11.5 ± 1.25 11 (11–12) | 11.5 ± 1.3 11 (11–12) | 12 ± 1.6 12 (11–13) | 0.098 |
| Cord blood (mg/L) | 2.0 ± 0.38 2.0 (1.7–2.2) | 2.0 ± 0.40 2.0 (1.7–2.3) | 1.9 ± 0.53 1.8 (1.6–2.1) | 0.230 |
| Copper (Cu) | ||||
| Maternal urine (mg/g creatinine) | 0.02 ± 0.01 0.02 (0.01–0.02) | 0.02 ± 0.01 0.02 (0.02–0.02) | 0.02 ± 0.01 0.02 (0.01–0.02) | 0.082 |
| Maternal blood (mg/L) | 1.6 ± 0.29 1.6 (1.4–1.8) | 1.6 ± 0.28 1.6 (1.5–1.7) | 1.6 ± 0.24 1.6 (1.5–1.7) | 0.958 |
| Placenta (mg/kg) | 1.2 ± 0.14 1.0 (0.96–1.1) | 1.05 ± 0.115 1.0 (0.96–1.1) | 1.1 ± 0.13 1.1 (0.98–1.2) | 0.744 |
| Cord blood (mg/L) | 0.60 ± 0.07 0.60 (0.55–0.65) | 0.595 ± 0.073 0.60 (0.57–0.64) | 0.60 ± 0.08 0.59 (0.56–0.63) | 0.88 |
| Selenium (Se) | ||||
| Maternal urine (mg/g creatinine) | 0.03 ± 0.01 0.03 (0.02–0.03) a | 0.03 ± 0.02 0.03 (0.02–0.03) a | 0.02 ± 0.01 0.02 (0.02–0.03) b | 0.019 |
| Maternal blood (mg/L) | 0.10 ± 0.02 0.10 (0.09–0.11) | 0.10 ± 0.02 0.10 (0.09–0.11) | 0.09 ± 0.01 0.09 (0.09–0.10) | 0.061 |
| Placenta (mg/kg) | 0.17 ± 0.02 0.17 (0.16–0.18) | 0.17 ± 0.02 0.17 (0.16–0.18) | 0.16 ± 0.02 0.16 (0.15–0.17) | 0.344 |
| Cord blood (mg/L) | 0.10 ± 0.02 0.09 (0.09–0.11) | 0.10 ± 0.02 0.10 (0.09–0.11) | 0.09 ± 0.01 0.09 (0.09–0.10) | 0.276 |
| P4 Cord Serum | E2 Cord Serum | Cd Maternal Urine | Cd Maternal Blood | Cd Placenta | Cd Cord Blood | Pb Placenta | Fe Placenta | |
|---|---|---|---|---|---|---|---|---|
| Intercept | 6.6 [6.0, 7.3] p < 0.001 | 9.5 [8.8, 10] p < 0.001 | −3.1 [−3.8, −2.4] p < 0.001 | −1.8 [−2.7, −0.94] p < 0.001 | 0.81 [0.14, 1.5] p = 0.017 | −4.1 [−5.2, −2.9] p < 0.001 | 0.07 [−1.0, 1.2] p = 0.905 | 4.4 [4.0, 4.9] p < 0.001 |
| Smoking b | ||||||||
| Active smokers | −0.19 [−0.38, −0.004] p = 0.045 | −0.29 [−0.49, −0.08] p = 0.006 | 0.32 [0.12, 0.52] p = 0.002 | 1.1 [0.85, 1.4] p < 0.001 | 0.37 [0.17, 0.56] p < 0.001 | 0.66 [0.34, 0.98] p < 0.001 | 0.44 [0.12, 0.76] p = 0.007 | −0.13 [−0.27, −0.003] p = 0.045 |
| Former smokers | −0.07 [−0.23, 0.09] p = 0.377 | −0.13 [−0.31, 0.04] p = 0.128 | 0.17 [−0.01, 0.34] p = 0.059 | 0.20 [−0.03, 0.42] p = 0.085 | 0.13 [−0.04, 0.29] p = 0.133 | −0.10 [−0.37, 0.18] p = 0.495 | 0.14 [−0.13, 0.41] p = 0.316 | 0.03 [−0.08, 0.14] p = 0.613 |
| Passive smoking | −0.02 [−0.16, 0.12] p = 0.797 | 0.02 [−0.14, 0.17] p = 0.822 | −0.003 [−0.16, 0.15] p = 0.974 | 0.21 [0.01, 0.41] p = 0.036 | 0.13 [−0.01, 0.28] p = 0.077 | −0.17 [−0.41, 0.08] p = 0.180 | 0.07 [−0.18, 0.31] p = 0.590 | −0.002 [−0.10, 0.10] p = 0.974 |
| Age | 0.001 [−0.02, 0.02] p = 0.905 | −0.01 [−0.03, 0.01] p = 0.492 | 0.04 [0.03, 0.06] p < 0.001 | 0.01 [−0.01, 0.04] p = 0.283 | 0.03 [0.02, 0.05] p < 0.001 | 0.02 [−0.01, 0.05] p = 0.250 | 0.02 [−0.01, 0.05] p = 0.201 | 0.01 [−0.002, 0.02] p = 0.096 |
| University degree | 0.05 [−0.11, 0.20] p = 0.565 | 0.01 [−0.16, 0.19] p = 0.874 | −0.17 [−0.34, −0.002] p = 0.047 | −0.12 [−0.34, 0.10] p = 0.294 | −0.09 [−0.25, 0.08] p = 0.293 | −0.04 [−0.32, 0.23] p = 0.747 | −0.11 [−0.38, 0.16] p = 0.414 | −0.05 [−0.16, 0.06] p = 0.413 |
| Prepregnancy BMI | 0.01 [−0.01, 0.02] p = 0.486 | 0.01 [−0.01, 0.03] p = 0.297 | 0.01 [−0.01, 0.03] p = 0.573 | −0.01 [−0.04, 0.01] p = 0.315 | −0.01 [−0.03, 0.01] p = 0.156 | −0.01 [−0.05, 0.02] p = 0.359 | −0.02 [−0.05, 0.01] p = 0.211 | 0.003 [−0.01, 0.02] p = 0.653 |
| Weight gain | 0.02 [0.01, 0.03] p = 0.004 | 0.01 [−0.01, 0.02] p = 0.429 | 0.01 [−0.003, 0.02] p = 0.132 | 0.01 [−0.01, 0.03] p = 0.262 | 0.01 [−0.003, 0.02] p = 0.112 | −0.02 [−0.04, 0.01] p = 0.171 | 0.03 [0.004, 0.05] p = 0.020 | −0.0002 [−0.01, 0.01] p = 0.961 |
| Parity | −0.15 [−0.23, −0.08] p < 0.001 | −0.12 [−0.21, −0.04] p = 0.003 | 0.02 [−0.06, 0.10] p = 0.655 | 0.07 [−0.03, 0.18] p = 0.188 | −0.03 [−0.10, 0.05] p = 0.511 | −0.03 [−0.16, 0.10] p = 0.658 | −0.04 [−0.17, 0.09] p = 0.514 | −0.09 [−0.14, −0.04] p = 0.001 |
| Adjusted R2 | 0.22 | 0.14 | 0.22 | 0.44 | 0.17 | 0.12 | 0.08 | 0.11 |
| Placental Weight | Birth Weight | Birth Length | Birth Weight:Placental Weight Ratio | |
|---|---|---|---|---|
| Maternal serum P4 | 0.22 | 0.23 | 0.13 | −0.10 |
| Placental P4 | −0.01 | 0.11 | 0.09 | 0.09 |
| Cord serum P4 | 0.06 | 0.16 | 0.16 | 0.06 |
| Maternal serum E2 | 0.04 | 0.04 | 0.05 | −0.01 |
| Placental E2 | −0.06 | −0.12 | −0.18 | −0.03 |
| Cord serum E2 | −0.10 | −0.01 | 0.06 | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piasek, M.; Škrgatić, L.; Sulimanec, A.; Orct, T.; Sekovanić, A.; Kovačić, J.; Katić, A.; Branović Čakanić, K.; Pizent, A.; Brajenović, N.; et al. Effects of Maternal Cigarette Smoking on Trace Element Levels and Steroidogenesis in the Maternal–Placental–Fetal Unit. Toxics 2023, 11, 714. https://doi.org/10.3390/toxics11080714
Piasek M, Škrgatić L, Sulimanec A, Orct T, Sekovanić A, Kovačić J, Katić A, Branović Čakanić K, Pizent A, Brajenović N, et al. Effects of Maternal Cigarette Smoking on Trace Element Levels and Steroidogenesis in the Maternal–Placental–Fetal Unit. Toxics. 2023; 11(8):714. https://doi.org/10.3390/toxics11080714
Chicago/Turabian StylePiasek, Martina, Lana Škrgatić, Antonija Sulimanec, Tatjana Orct, Ankica Sekovanić, Jelena Kovačić, Anja Katić, Karmen Branović Čakanić, Alica Pizent, Nataša Brajenović, and et al. 2023. "Effects of Maternal Cigarette Smoking on Trace Element Levels and Steroidogenesis in the Maternal–Placental–Fetal Unit" Toxics 11, no. 8: 714. https://doi.org/10.3390/toxics11080714
APA StylePiasek, M., Škrgatić, L., Sulimanec, A., Orct, T., Sekovanić, A., Kovačić, J., Katić, A., Branović Čakanić, K., Pizent, A., Brajenović, N., Jurič, A., Brčić Karačonji, I., Kljaković-Gašpić, Z., Tariba Lovaković, B., Lazarus, M., Stasenko, S., Miškulin, I., & Jurasović, J. (2023). Effects of Maternal Cigarette Smoking on Trace Element Levels and Steroidogenesis in the Maternal–Placental–Fetal Unit. Toxics, 11(8), 714. https://doi.org/10.3390/toxics11080714