Perceptions about Healthy Eating and Emotional Factors Conditioning Eating Behaviour: A Study Involving Portugal, Brazil and Argentina

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
3.1. Sample Characterization
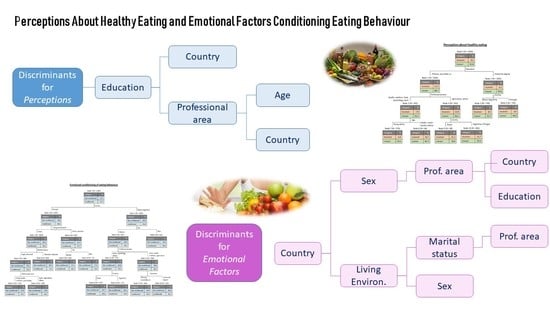
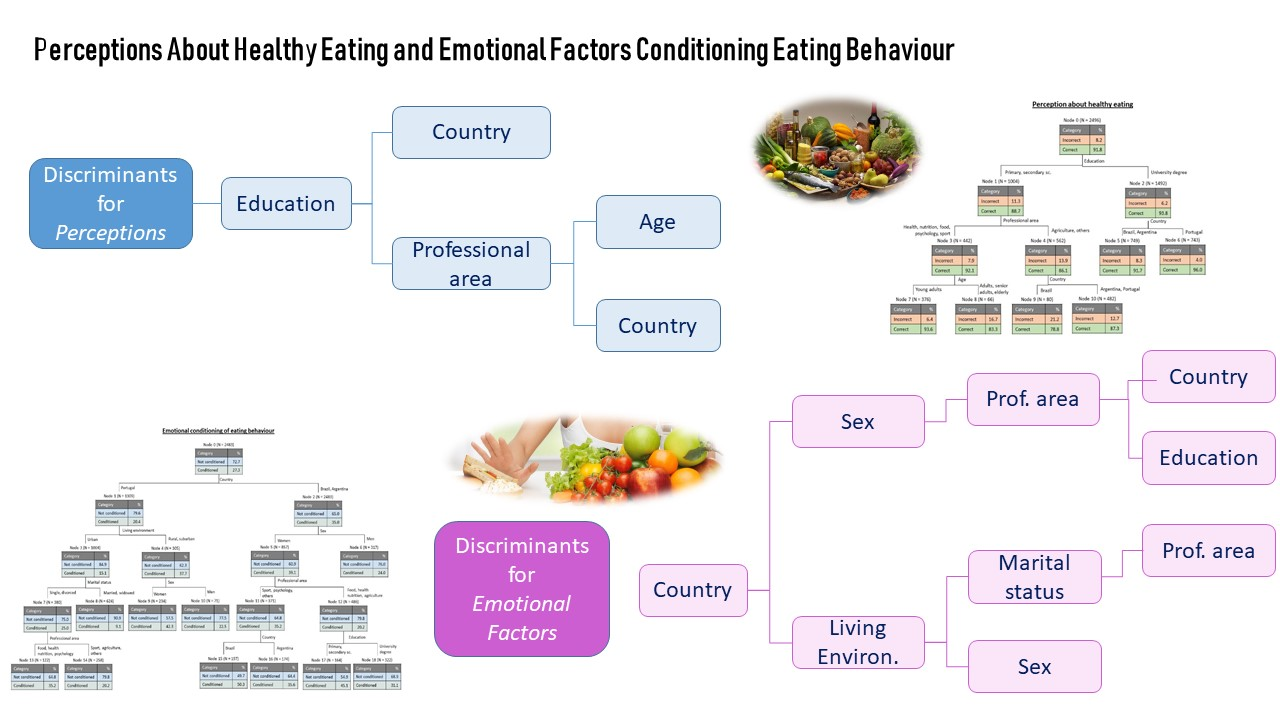
3.2. Perceptions About Healthy Diet
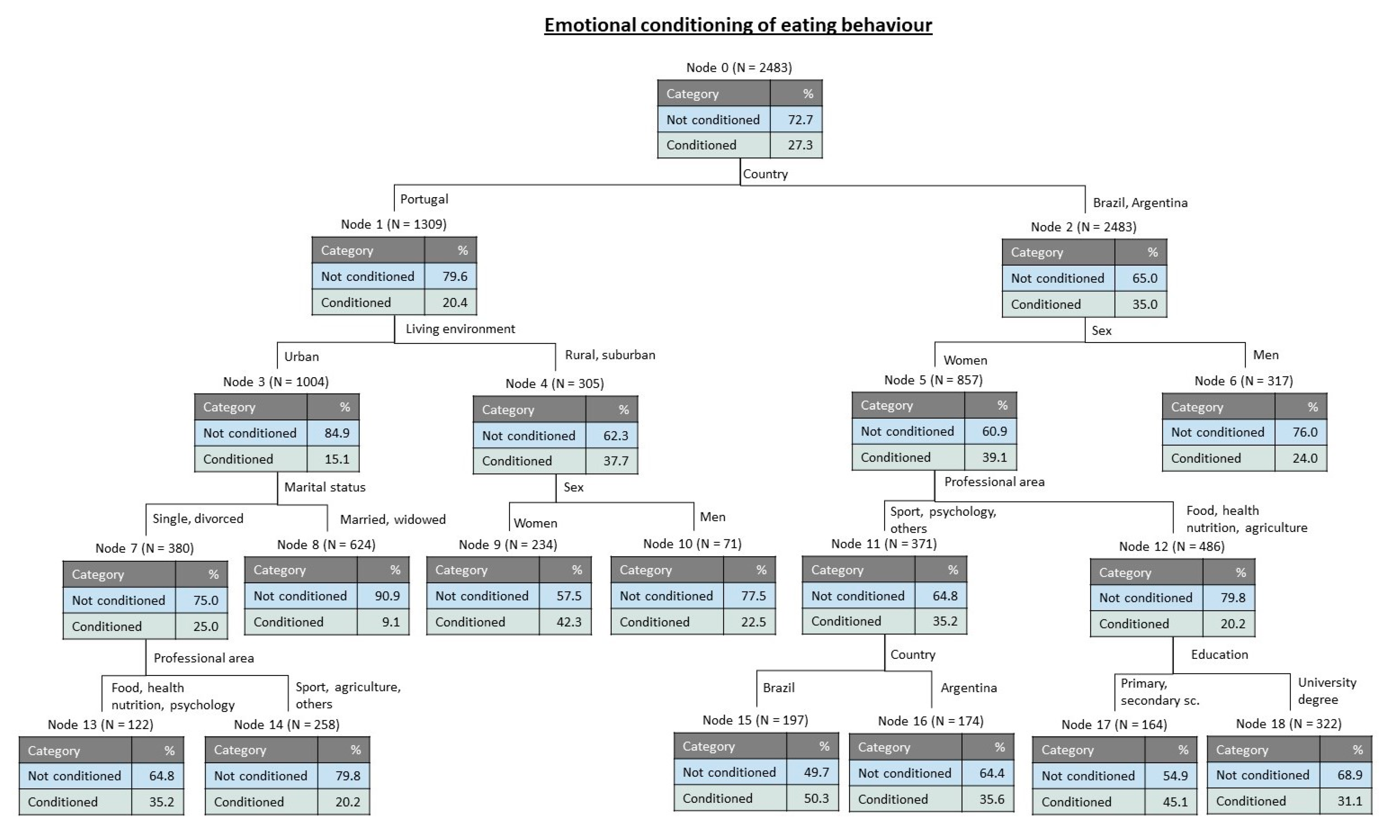
3.3. Emotional Factors Conditioning the Eating Behaviour
4. Discussion
5. Conclusions and Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Köster, E.P. Diversity in the determinants of food choice: A psychological perspective. Food Qual. Prefer. 2009, 20, 70–82. [Google Scholar] [CrossRef]
- Lent, R. Cem Bilhões de Neurónios: Conceitos Fundamentais de Neurociencia; Atheneu: São Paulo, Brasil, 2004. [Google Scholar]
- Fonseca, V. Importância das emoções na aprendizagem: Uma abordagem neuropsicopedagógica. Rev. Psicopedag. 2016, 33, 365–384. [Google Scholar]
- Ogden, J. The Psychology of Eating: From Healthy to Disordered Behavior; John Wiley & Sons: Malden, MA, USA, 2002; ISBN 978-0-631-23374-9. [Google Scholar]
- GHDX. Global Burden of Disease Study 2017; Institute for Health Metrics and Evaluation: Washington, DC, USA, 2017. [Google Scholar]
- Annunziata, A.; Vecchio, R. Organic farming and sustainability in food choices: An analysis of consumer preference in southern Italy. Agric. Sci. Procedia 2016, 8, 193–200. [Google Scholar] [CrossRef]
- Danner, H.; Menapace, L. Using online comments to explore consumer beliefs regarding organic food in German-speaking countries and the United States. Food Qual. Prefer. 2020, 83, 103912. [Google Scholar] [CrossRef]
- Rana, J.; Paul, J. Consumer behavior and purchase intention for organic food: A review and research agenda. J. Retail. Consum. Serv. 2017, 38, 157–165. [Google Scholar] [CrossRef]
- Costa, C.; García-Lestón, J.; Costa, S.; Coelho, P.; Silva, S.; Pingarilho, M.; Valdiglesias, V.; Mattei, F.; Dall’Armi, V.; Bonassi, S.; et al. Is organic farming safer to farmers’ health? A comparison between organic and traditional farming. Toxicol. Lett. 2014, 230, 166–176. [Google Scholar] [CrossRef]
- Kamp, M.E.; Saridakis, I.; Verkaik-Kloosterman, J. Iodine content of semi-skimmed milk available in the Netherlands depending on farming (organic versus conventional) and heat treatment (pasteurized versus UHT) and implications for the consumer. J. Trace Elem. Med. Biol. 2019, 56, 178–183. [Google Scholar] [CrossRef]
- Armesto, J.; Rocchetti, G.; Senizza, B.; Pateiro, M.; Barba, F.J.; Domínguez, R.; Lucini, L.; Lorenzo, J.M. Nutritional characterization of Butternut squash (Cucurbita moschata D.): Effect of variety (Ariel vs. Pluto) and farming type (conventional vs. organic). Food Res. Int. 2020, 132, 109052. [Google Scholar] [CrossRef]
- Martí, R.; Leiva-Brondo, M.; Lahoz, I.; Campillo, C.; Cebolla-Cornejo, J.; Roselló, S. Polyphenol and l-ascorbic acid content in tomato as influenced by high lycopene genotypes and organic farming at different environments. Food Chem. 2018, 239, 148–156. [Google Scholar] [CrossRef]
- Reeve, J.R.; Hoagland, L.A.; Villalba, J.J.; Carr, P.M.; Atucha, A.; Cambardella, C.; Davis, D.R.; Delate, K. Chapter six—Organic farming, soil health, and food quality: Considering possible links. In Advances in Agronomy; Sparks, D.L., Ed.; Academic Press: Cambridge, MA, USA, 2016; Volume 137, pp. 319–367. [Google Scholar]
- Hyland, C.; Bradman, A.; Gerona, R.; Patton, S.; Zakharevich, I.; Gunier, R.B.; Klein, K. Organic diet intervention significantly reduces urinary pesticide levels in U.S. children and adults. Environ. Res. 2019, 171, 568–575. [Google Scholar] [CrossRef]
- Melgarejo, M.; Mendiola, J.; Koch, H.M.; Moñino-García, M.; Noguera-Velasco, J.A.; Torres-Cantero, A.M. Associations between urinary organophosphate pesticide metabolite levels and reproductive parameters in men from an infertility clinic. Environ. Res. 2015, 137, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Kuang, L.; Hou, Y.; Huang, F.; Hong, H.; Sun, H.; Deng, W.; Lin, H. Pesticide residues in breast milk and the associated risk assessment: A review focused on China. Sci. Total Environ. 2020, 727, 138412. [Google Scholar] [CrossRef]
- Sabarwal, A.; Kumar, K.; Singh, R.P. Hazardous effects of chemical pesticides on human health–Cancer and other associated disorders. Environ. Toxicol. Pharmacol. 2018, 63, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Martin, F.L.; Martinez, E.Z.; Stopper, H.; Garcia, S.B.; Uyemura, S.A.; Kannen, V. Increased exposure to pesticides and colon cancer: Early evidence in Brazil. Chemosphere 2018, 209, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Philippat, C.; Barkoski, J.; Tancredi, D.J.; Elms, B.; Barr, D.B.; Ozonoff, S.; Bennett, D.H.; Hertz-Picciotto, I. Prenatal exposure to organophosphate pesticides and risk of autism spectrum disorders and other non-typical development at 3 years in a high-risk cohort. Int. J. Hyg. Environ. Health 2018, 221, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.; Silverstein, J. Organic foods: Health and environmental advantages and disadvantages. Pediatrics 2012, 130, e1406–e1415. [Google Scholar] [CrossRef]
- USDA. Pesticide Data Program; United States Department of Agriculture: Washington, DC, USA, 2016.
- Jackson, B.; Cooper, M.L.; Mintz, L.; Albino, A. Motivations to eat: Scale development and validation. J. Res. Personal. 2003, 37, 297–318. [Google Scholar] [CrossRef]
- Gibson, E.L. Emotional influences on food choice: Sensory, physiological and psychological pathways. Physiol. Behav. 2006, 89, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Gold, P.W.; Chrousos, G.P. Organization of the stress system and its dysregulation in melancholic and atypical depression: High vs low CRH/NE states. Mol. Psychiatry 2002, 7, 254–275. [Google Scholar] [CrossRef]
- Paans, N.P.G.; Gibson-Smith, D.; Bot, M.; van Strien, T.; Brouwer, I.A.; Visser, M.; Penninx, B.W.J.H. Depression and eating styles are independently associated with dietary intake. Appetite 2019, 134, 103–110. [Google Scholar] [CrossRef]
- Love, H.; Bhullar, N.; Schutte, N.S. Psychological aspects of diet: Development and validation of three measures assessing dietary goal-desire incongruence, motivation, and satisfaction with dietary behavior. Appetite 2019, 138, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Lazarevich, I.; Camacho, M.E.I.; Velázquez-Alva, M.d.C.; Zepeda, M. Relationship among obesity, depression, and emotional eating in young adults. Appetite 2016, 107, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Ferrão, A.C.; Guine, R.P.F.; Correia, P.M.R.; Ferreira, M.; Lima, J.D. Development of a questionnaire to assess people’s food choices determinants. Curr. Nutr. Food Sci. 2019, 15, 281–295. [Google Scholar] [CrossRef]
- Ferrão, A.C.; Correia, P.; Ferreira, M.; Guiné, R.P.F. Perceptions towards healthy diet of the portuguese according to area of work or studies. Zdr Varst 2019, 58, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Ferrão, A.C.; Guiné, R.P.F.; Correia, P.; Ferreira, M.; Cardoso, A.P.; Duarte, J.; Lima, J. Perceptions towards a healthy diet among a sample of university people in Portugal. Nutr. Food Sci. 2018, 48, 669–688. [Google Scholar] [CrossRef]
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 1–55. [Google Scholar]
- Pestana, M.H.; Gageiro, J.N. Análise de Dados para Ciências Sociais—A complementaridade do SPSS; Edições Sílabo: Lisbon, Portugal, 2014. [Google Scholar]
- Witten, R.; Witte, J. Statistics, 9th ed.; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Lê, J.; Dallongeville, J.; Wagner, A.; Arveiler, D.; Haas, B.; Cottel, D.; Simon, C.; Dauchet, L. Attitudes toward healthy eating: A mediator of the educational level-diet relationship. Eur. J. Clin. Nutr. 2013, 67, 808–814. [Google Scholar] [CrossRef]
- Thow, A.M.; Verma, G.; Soni, D.; Soni, D.; Beri, D.K.; Kumar, P.; Siegel, K.R.; Shaikh, N.; Khandelwal, S. How can health, agriculture and economic policy actors work together to enhance the external food environment for fruit and vegetables? A qualitative policy analysis in India. Food Policy 2018, 77, 143–151. [Google Scholar] [CrossRef]
- Sharps, M.; Robinson, E. Encouraging children to eat more fruit and vegetables: Health vs. descriptive social norm-based messages. Appetite 2016, 100, 18–25. [Google Scholar] [CrossRef]
- Park, H.; Yu, S. Policy review: Implication of tax on sugar-sweetened beverages for reducing obesity and improving heart health. Health Policy Technol. 2019, 8, 92–95. [Google Scholar] [CrossRef]
- Carbone, S.; Lavie, C.J.; Elagizi, A.; Arena, R.; Ventura, H.O. The impact of obesity in heart failure. Heart Fail. Clin. 2020, 16, 71–80. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; Lucan, S.C.; O’Keefe, J.H. The evidence for saturated fat and for sugar related to coronary heart disease. Prog. Cardiovasc. Dis. 2016, 58, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, B.; Afonso, C.; Sousa, A.S.; Guerra, R.S.; Santos, A.; Borges, N.; Moreira, P.; Padrão, P.; Amaral, T.F. Adherence to a mediterranean dietary pattern status and associated factors among Portuguese older adults: Results from the nutrition up 65 cross-sectional study. Nutrition 2019, 65, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Dammann, K.W.; Smith, C. Food-related environmental, behavioral, and personal factors associated with body mass index among urban, low-income African-American, American Indian, and Caucasian women. Am. J. Health Promot. 2011, 25, e1–e10. [Google Scholar] [CrossRef]
- Rustad, C.; Smith, C. Nutrition knowledge and associated behavior changes in a holistic, short-term nutrition education intervention with low-income women. J. Nutr. Educ. Behav. 2013, 45, 490–498. [Google Scholar] [CrossRef]
- Strien, T. Causes of emotional eating and matched treatment of obesity. Curr. Diab. Rep. 2018, 18. [Google Scholar] [CrossRef]
- Chambers, D.; Phan, U.T.X.; Chanadang, S.; Maughan, C.; Sanchez, K.; Di Donfrancesco, B.; Gomez, D.; Higa, F.; Li, H.; Chambers, E.; et al. Motivations for Food Consumption during specific eating occasions in Turkey. Foods 2016, 5, 39. [Google Scholar] [CrossRef]
- Ashurst, J.; van Woerden, I.; Dunton, G.; Todd, M.; Ohri-Vachaspati, P.; Swan, P.; Bruening, M. The association among emotions and food choices in first-year college students using mobile-ecological momentary assessments. BMC Public Health 2018, 18, 573. [Google Scholar] [CrossRef]
- Bennett, J.; Greene, G.; Schwartz-Barcott, D. Perceptions of emotional eating behavior. A qualitative study of college students. Appetite 2013, 60, 187–192. [Google Scholar] [CrossRef]
- Boggiano, M.M. Palatable eating motives scale in a college population: Distribution of scores and scores associated with greater BMI and binge-eating. Eat. Behav. 2016, 21, 95–98. [Google Scholar] [CrossRef]
- Bartkiene, E.; Steibliene, V.; Adomaitiene, V.; Juodeikiene, G.; Cernauskas, D.; Lele, V.; Klupsaite, D.; Zadeike, D.; Jarutiene, L.; Guiné, R.P.F. Factors affecting consumer food preferences: Food taste and depression-based evoked emotional expressions with the use of face reading technology. Bio. Med. Res. Int. 2019, 2019, 2097415. [Google Scholar] [CrossRef] [PubMed]
- Guiné, R.; Ferrão, A.C.; Ferreira, M.; Correia, P.; Cardoso, A.P.; Duarte, J.; Rumbak, I.; Shehata, A.-M.; Vittadini, E.; Papageorgiou, M. The motivations that define eating patterns in some Mediterranean countries. Nutr. Food Sci. 2019, 49, 1126–1141. [Google Scholar] [CrossRef]
- Hidalgo-Mora, J.J.; García-Vigara, A.; Sánchez-Sánchez, M.L.; García-Pérez, M.-Á.; Tarín, J.; Cano, A. The Mediterranean diet: A historical perspective on food for health. Maturitas 2020, 132, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Latha, S. Vuca in engineering education: Enhancement of faculty competency for capacity building. Procedia Comput. Sci. 2020, 172, 741–747. [Google Scholar] [CrossRef]
- Bezanilla, M.J.; Fernández-Nogueira, D.; Poblete, M.; Galindo-Domínguez, H. Methodologies for teaching-learning critical thinking in higher education: The teacher’s view. Think. Ski. Creat. 2019, 33, 100584. [Google Scholar] [CrossRef]
- Castro, J.M.; Bellisle, F.; Feunekes, G.I.J.; Dalix, A.-M.; De Graaf, C. Culture and meal patterns: A comparison of the food intake of free-living American, Dutch, and French students. Nutr. Res. 1997, 17, 807–829. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | Groups | % | Variable | Groups | % |
|---|---|---|---|---|---|
| Age 1 | Young adults | 43.4 | Country | Argentina | 20.9 |
| Adults | 39.5 | Brazil | 26.6 | ||
| Senior adults | 14.5 | Portugal | 52.5 | ||
| Elderly | 2.6 | Living environment | Rural | 9.6 | |
| Sex | Women | 69.8 | Urban | 84.4 | |
| Men | 30.2 | Suburban | 6.0 | ||
| Education | Basic school | 0.6 | Area of study/work | Nutrition | 10.7 |
| Secondary school | 39.6 | Food | 5.1 | ||
| University degree | 59.8 | Agriculture | 2.2 | ||
| Marital status | Single | 46.7 | Sport | 3.3 | |
| Married | 44.1 | Psychology | 2.6 | ||
| Divorced | 6.5 | Health | 19.8 | ||
| Widowed | 2.8 | Others | 56.4 |
| Perceptions About Healthy Eating | Percentage of Answers According to Scale Points | ||||
|---|---|---|---|---|---|
| 1 (%) | 2 (%) | 3 (%) | 4 (%) | 5 (%) | |
| 1. Healthy eating is based on counting calories | 17.2 | 27.9 | 18.2 | 25.6 | 11.1 |
| 2. We should never consume sugary products | 15.7 | 56.9 | 14.2 | 10.6 | 2.6 |
| 3. Fruits and vegetables are important for a healthy diet | 0.6 | 0.2 | 1.1 | 25.1 | 73.1 |
| 4. A healthy diet must be balanced, varied and complete | 0.6 | 0.2 | 1.8 | 22.5 | 75.0 |
| 5. We can eat everything as long as it is in small quantities | 4.4 | 24.4 | 11.5 | 35.0 | 24.7 |
| 6. I believe that a healthy diet is expensive | 16.8 | 28.4 | 21.9 | 24.1 | 8.8 |
| 7. In my opinion it is strange that some people have cravings for sweets | 31.7 | 50.7 | 12.4 | 4.0 | 1.2 |
| 8. I believe that tradition is very important for healthy eating | 10.8 | 25.0 | 25.1 | 30.3 | 8.9 |
| 9. I believe that food coming from organic farming is healthier | 1.5 | 5.7 | 22.8 | 37.4 | 32.6 |
| 10. We should never consume high fat foods | 13.3 | 50.7 | 17.9 | 13.5 | 4.6 |
| Variable | Perception | Chi-Square Test | Cramer’s Coefficient | |
|---|---|---|---|---|
| Correct | Incorrect | |||
| (%) | (%) | p | V | |
| Country | 0.018 | 0.057 | ||
| Argentina | 90.8 | 9.2 | ||
| Brazil | 89.7 | 10.3 | ||
| Portugal | 93.2 | 6.8 | ||
| Education | <0.0005 | 0.092 | ||
| Basic school | 93.3 | 6.7 | ||
| Secondary school | 88.7 | 11.3 | ||
| University degree | 93.8 | 6.2 | ||
| Emotional Factors Conditioning the Eating Behaviour | Percentage of Answers According to Scale Points | ||||
|---|---|---|---|---|---|
| 1 (%) | 2 (%) | 3 (%) | 4 (%) | 5 (%) | |
| 1. Food helps me deal with stress | 8.8 | 35.7 | 19.7 | 28.8 | 7.1 |
| 2. I usually eat food that helps me control my weight | 3.6 | 16.2 | 21.0 | 50.2 | 9.0 |
| 3. I often consume products that keep me awake and alert (such as coffee, cola, energy drinks) | 29.0 | 33.4 | 11.1 | 19.8 | 6.8 |
| 4. I often consume products that help me relax (such as, for example, infusions of herbs with calming properties) | 10.4 | 23.2 | 17.2 | 37.4 | 11.8 |
| 5. Food makes me feel good | 1.4 | 4.3 | 17.0 | 60.7 | 16.7 |
| 6. When I feel alone, I comfort myself/take refuge in food | 21.7 | 45.0 | 15.5 | 12.9 | 4.9 |
| 7. I eat more when I have nothing to do | 15.1 | 31.7 | 14.2 | 30.0 | 9.0 |
| 8. For me, food serves as an emotional consolation | 22.2 | 40.9 | 16.6 | 15.2 | 5.2 |
| 9. When I’m depressed, I have more cravings for sweets | 20.5 | 36.0 | 13.7 | 20.4 | 9.4 |
| Variable | Eating Habits | Chi-Square Test | Cramer’s Coefficient | |
|---|---|---|---|---|
| Conditioned | Not Conditioned | |||
| (%) | (%) | p | V | |
| Country | <0.0005 | 0.166 | ||
| Argentina | 33.2 | 66.8 | ||
| Brazil | 36.4 | 63.6 | ||
| Portugal | 20.4 | 79.6 | ||
| Education | 0.006 | 0.064 | ||
| Basic school | 26.7 | 73.3 | ||
| Secondary school | 30.8 | 69.2 | ||
| University degree | 25.0 | 75.0 | ||
| Age 1 | <0.0005 | 0.156 | ||
| Young adults | 34.0 | 66.0 | ||
| Adults | 25.3 | 74.7 | ||
| Senior adults | 15.2 | 84.8 | ||
| Elderly | 12.5 | 87.5 | ||
| Sex | <0.0005 | 0.146 | ||
| Women | 31.6 | 68.4 | ||
| Men | 17.4 | 82.6 | ||
| Marital status | <0.0005 | 0.160 | ||
| Single | 34.1 | 65.9 | ||
| Married | 21.0 | 79.0 | ||
| Divorced | 30.4 | 69.6 | ||
| Widowed | 7.2 | 92.8 | ||
| Living environment | <0.0005 | 0.116 | ||
| Rural | 37.7 | 62.3 | ||
| Urban | 25.1 | 74.9 | ||
| Suburban | 41.6 | 58.4 | ||
| Area of study/work | <0.0005 | 0.154 | ||
| Nutrition | 37.6 | 62.4 | ||
| Food | 37.8 | 62.2 | ||
| Agriculture | 20.4 | 79.6 | ||
| Sport | 26.8 | 73.2 | ||
| Psychology | 46.2 | 53.8 | ||
| Health | 32.2 | 67.8 | ||
| Others | 22.1 | 77.9 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardoso, A.P.; Ferreira, V.; Leal, M.; Ferreira, M.; Campos, S.; Guiné, R.P.F. Perceptions about Healthy Eating and Emotional Factors Conditioning Eating Behaviour: A Study Involving Portugal, Brazil and Argentina. Foods 2020, 9, 1236. https://doi.org/10.3390/foods9091236
Cardoso AP, Ferreira V, Leal M, Ferreira M, Campos S, Guiné RPF. Perceptions about Healthy Eating and Emotional Factors Conditioning Eating Behaviour: A Study Involving Portugal, Brazil and Argentina. Foods. 2020; 9(9):1236. https://doi.org/10.3390/foods9091236
Chicago/Turabian StyleCardoso, Ana Paula, Vanessa Ferreira, Marcela Leal, Manuela Ferreira, Sofia Campos, and Raquel P. F. Guiné. 2020. "Perceptions about Healthy Eating and Emotional Factors Conditioning Eating Behaviour: A Study Involving Portugal, Brazil and Argentina" Foods 9, no. 9: 1236. https://doi.org/10.3390/foods9091236
APA StyleCardoso, A. P., Ferreira, V., Leal, M., Ferreira, M., Campos, S., & Guiné, R. P. F. (2020). Perceptions about Healthy Eating and Emotional Factors Conditioning Eating Behaviour: A Study Involving Portugal, Brazil and Argentina. Foods, 9(9), 1236. https://doi.org/10.3390/foods9091236