

Impact on Glycemic Variation Caused by a Change in the Dietary Intake Sequence

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Quasiexperimental Study Design
- Generation of data: A series of body measurements, an indirect calorimetry test, and the development of a food reminder were developed in the participant to have an approximation of the nutritional status of the participant and to be able to propose the type of interventions in the sequence of macronutrient intake to follow so that there is no decompensation in the current type of food intake.
- Implantation of the continuous glucose monitoring sensor: In each test, a new interstitial glucose sensor was implanted to generate data on glucose dynamics.
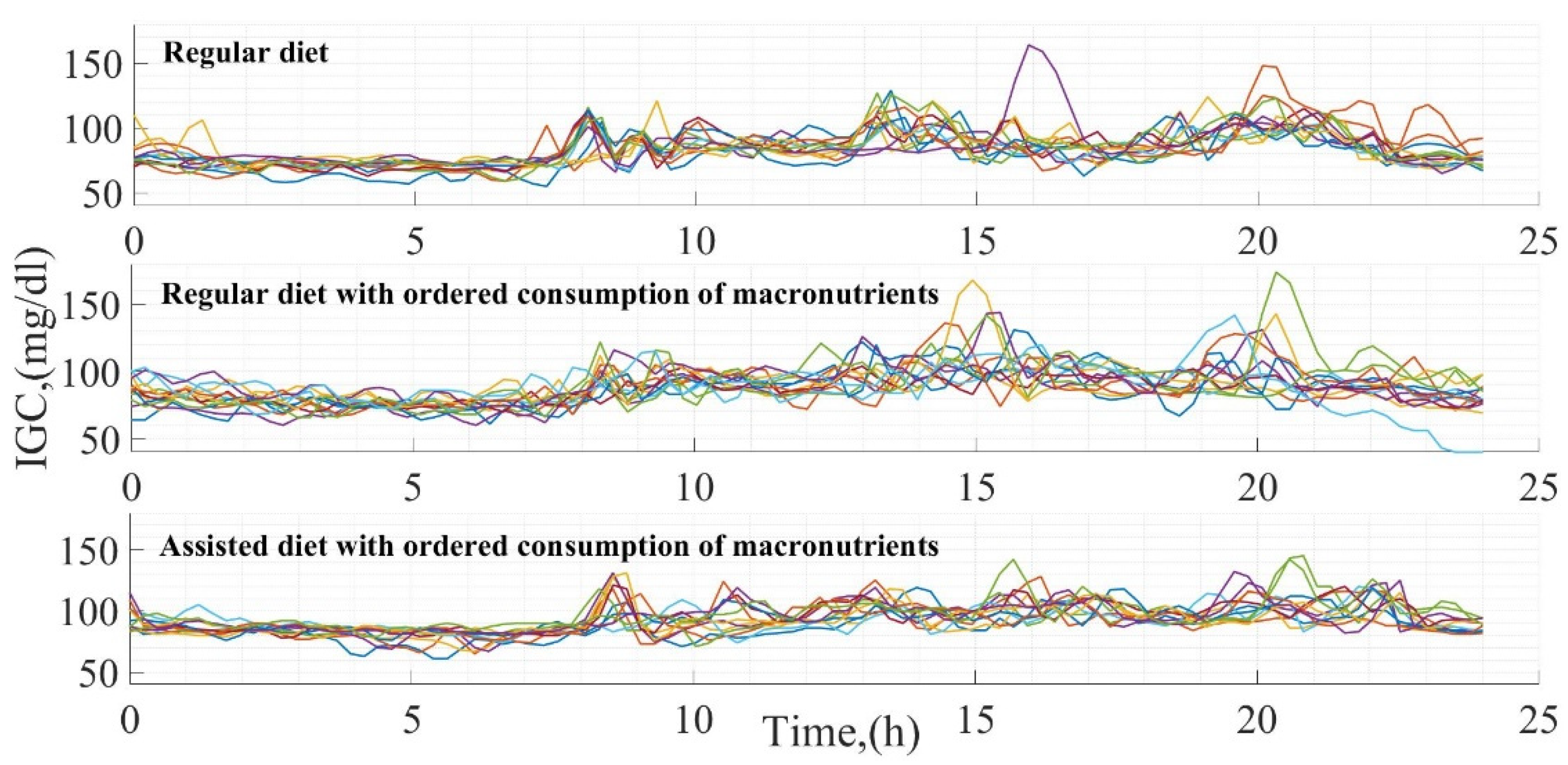
- Daily diet (Test 1): Subsequently, Test 1 was developed, where glucose measurements were generated and focused on describing the variation of glucose levels in the face of the study subject’s daily diet (mixture of macronutrients without having any order in food consumption).
- Regular diet with ordered consumption of macronutrients (Test 2): Test 2 has the objective of obtaining the glucose dynamics when the sequence in the order of macronutrient consumption is modified without generating any change in the participant’s regular diet.
- Assisted diet with ordered consumption of macronutrients (Test 3): This test consists of generating measurements of glucose variation in the face of a modification in the participant’s daily diet considering the change in the sequence of macronutrient intake.
- Statistical analysis: Once the three different tests were generated, a statistical analysis of the results obtained was generated, which was the study’s core. In this analysis, the impact of the sequence in macronutrient consumption was quantified and contrasted concerning the postprandial glucose curves generated in each dietary intake. For this purpose, the proportions of macronutrients consumed per intake were used and related to glucose concentrations, magnitudes of the postprandial glucose peaks, and times in which postprandial glucose stabilizes.
2.2. Ethics of Research
2.3. Instrumentation
2.4. Subject of Study
2.5. Food Sequence
2.6. Proportions of Macronutrients Ingested
2.7. Diet for Each Test Developed
- Test 1: Breakfast, smoothie with the following items, 1 banana (100 g), 33 g amaranth, 84 g oatmeal, and milk (500 mL), 2 eggs, and 2 corn tortillas (developed at 7:50 h). Lunch, 15 g of chickpeas, a piece of bread, and 500 mL of water (developed at 13:10 h). Snack 1, smoothie with the following items, 25 g whey protein, and 350 mL of milk (developed at 19:00 h). Dinner, 1 sandwich consisting of 40 g turkey ham and 25 g of cheese, and 350 mL of milk (developed at 19:15 h). Snack 2, 30 peanuts (developed at 21:00 h).
- Test 2: Breakfast, 240 mL of whole milk, 2 scrambled eggs, 2 corn tortillas, and 500 mL of water (developed at 7:40 h). Snack 1, a smoothie with the following items, 25 g whey protein, 84 g oatmeal, 1 banana (100 g), and 500 mL of water (developed 13:20 h). Snack 2, 3 nuts (developed at 21:30 h). Lunch, a salad (lettuce and tomato), 60 g rice, 100 g beef steak, 3 corn tortillas, 15 peanuts, and 500 mL of water (developed at 15:30 h). Dinner, 60 g chicken breast, 120 g salad (potato, carrot, and pea), 50 g jicama, 18 pieces of grapes, and 500 mL water (developed at 20:30 h).
- Test 3: Breakfast, 2 slices of white bread, 40 g of turkey ham, 60 g of salad (alfalfa sprouts, lettuce, and tomato), 23 g avocado, and 500 mL of water (developed at 8:15 h). Snack 1, 25 g whey protein, 100 g Greek yogurt, and 110 g apple (developed at 11:30 h). Lunch, 60 g chicken, 60 g bell peppers and onion, 2 tortillas, 100 g, and 1000 mL water (developed at 16:15 h). Dinner, 2 baked corn tostadas, 90 g tuna, 50 g onion and tomato, 23 g avocado, and 750 mL of water (developed at 19:00 h). Snack 2, 150 g of pineapple, 100 g of jicama, 15 peanuts, and 500 mL of water (developed at 21:40 h.).
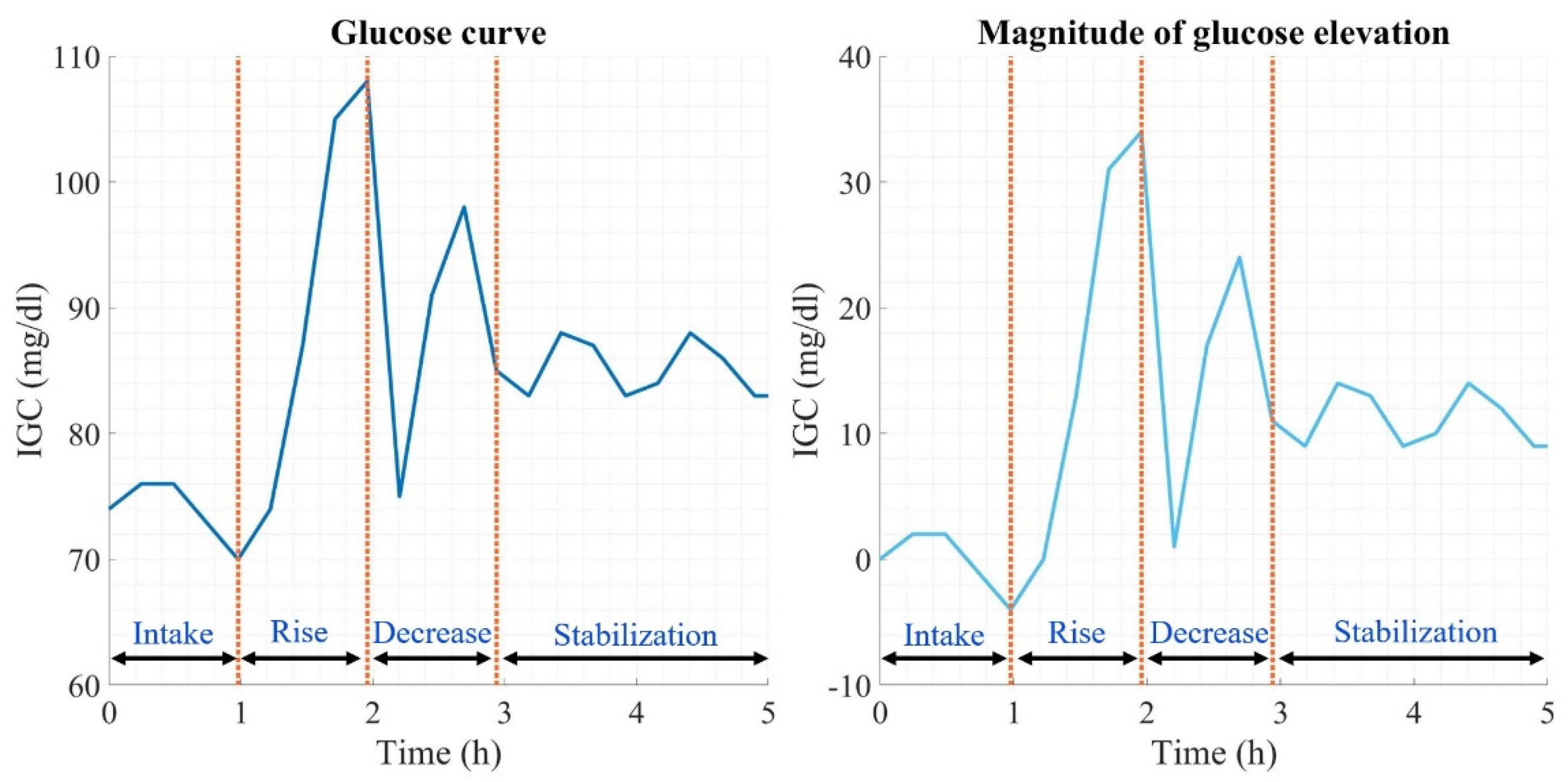
2.8. Glucose Curve
3. Results
3.1. Glucose Measurement
3.2. Food Sequence Modification Effect on Glucose
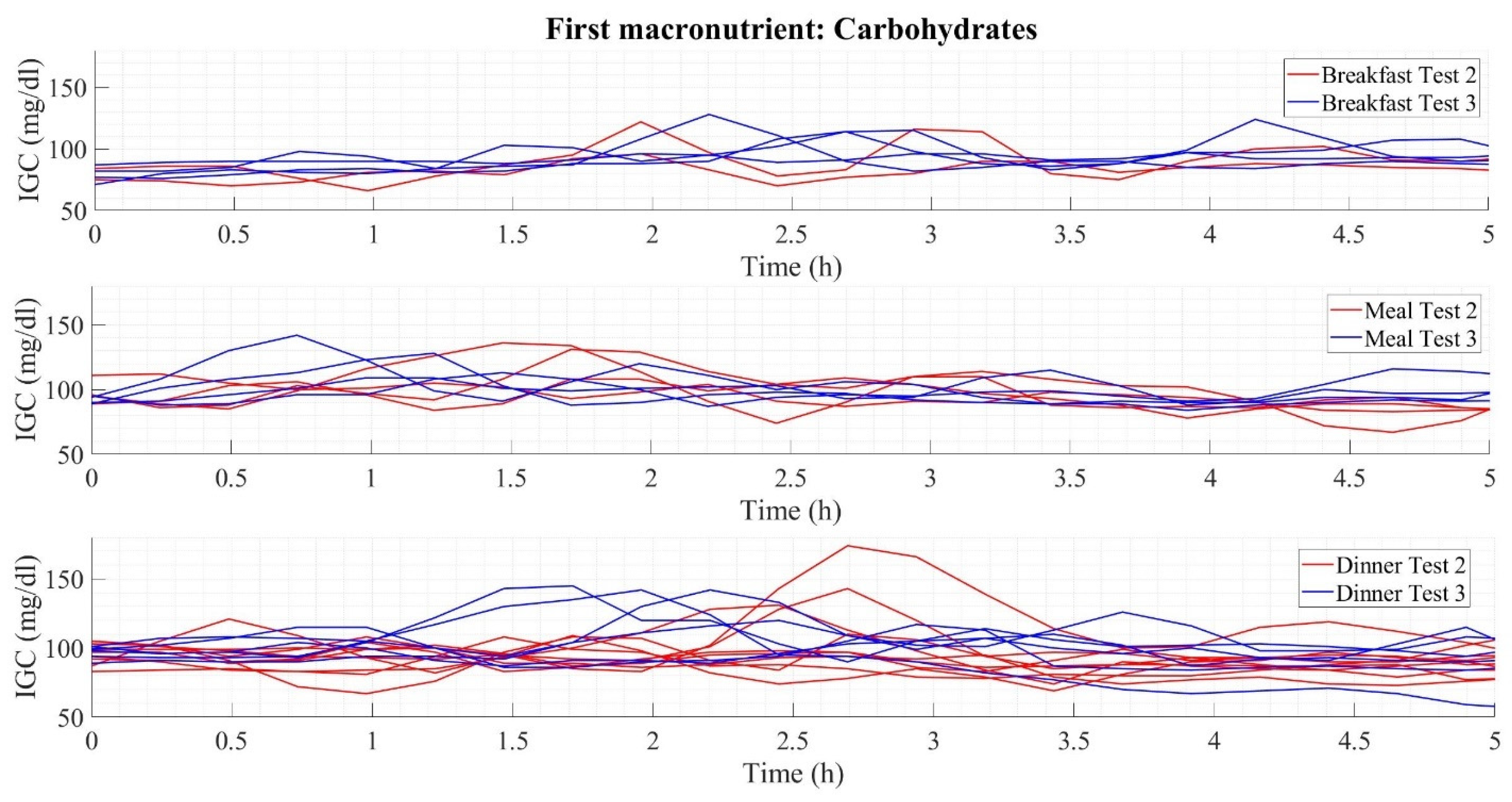
- Carbohydrate intake at the beginning;
- Vegetable and fiber intake at the beginning;
- Animal protein intake at the beginning.
4. Discussion
- Development of an analytical study on the effect of food sequence on postprandial glucose curves and the impact on glucose levels throughout the research period, with statistical analysis being a fundamental part of generating the results obtained;
- Experimentation time of 42 days divided into three different tests;
- Periodic change in meal plans to achieve patient adherence to experimentation;
- Contrast between three different conditions of glycemic variation derived from the tests proposed (the basis for experimentation on a more significant number of population).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Healthy Diet. 2019. Available online: www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 23 February 2023).
- Tschritter, O.; Fritsche, A.; Shirkavand, F.; Machicao, F.; Häring, H.; Stumvoll, M. Assessing the Shape of the Glucose Curve During an Oral Glucose Tolerance Test. Diabetes Care 2003, 26, 1026–1033. [Google Scholar] [CrossRef]
- Soeters, M.R. Food intake sequence modulates postprandial glycemia. Clin. Nutr. 2020, 39, 2335–2336. [Google Scholar] [CrossRef]
- Nusca, A.; Tuccinardi, D.; Albano, M.; Cavallaro, C.; Ricottini, E.; Manfrini, S.; Pozzilli, P.; Di Sciascio, G. Glycemic variability in the development of cardiovascular complications in diabetes. Diabetes Metab. Res. Rev. 2018, 34, e3047. [Google Scholar] [CrossRef]
- Ruijgrok, C.; Blaak, E.E.; Egli, L.; Dussort, P.; Vinoy, S.; Rauh, S.P.; Beulens, J.W.; Robertson, M.D.; Alssema, M. Reducing postprandial glucose in dietary intervention studies and the magnitude of the effect on diabetes-related risk factors: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 259–273. [Google Scholar] [CrossRef]
- Monnier, L.; Colette, C.; Owens, D. Glucose variability and diabetes complications: Risk factor or biomarker? Can we disentangle the “Gordian Knot”? Diabetes Metab. 2021, 47, 101225. [Google Scholar] [CrossRef]
- Bellary, S.; Kyrou, I.; Brown, J.E.; Bailey, C.J. Type 2 diabetes mellitus in older adults: Clinical considerations and management. Nat. Rev. Endocrinol. 2021, 17, 534–548. [Google Scholar] [CrossRef]
- Andreadi, A.; Bellia, A.; Di Daniele, N.; Meloni, M.; Lauro, R.; Della-Morte, D.; Lauro, D. The molecular link between oxidative stress, insulin resistance, and type 2 diabetes: A target for new therapies against cardiovascular diseases. Curr. Opin. Pharmacol. 2021, 62, 85–96. [Google Scholar] [CrossRef]
- Andreadi, A.; Muscoli, S.; Tajmir, R.; Meloni, M.; Minasi, A.; Muscoli, C.; Ilari, S.; Mollace, V.; Della Morte, D.; Bellia, A.; et al. Insulin Resistance and Acne: The Role of Metformin as Alternative Therapy in Men. Pharmaceuticals 2023, 16, 27. [Google Scholar] [CrossRef]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Pedreanez, A.; Mosquera, J.; Munoz, N.; Robalino, J.; Tene, D. Diabetes, heart damage, and angiotensin II. What is the relationship link between them? A minireview. Endocr. Regul. 2022, 56, 55–65. [Google Scholar] [CrossRef]
- Daneshzad, E.; Larijani, B.; Azadbakht, L. Diet quality indices and cardiovascular diseases risk factors among diabetic women. J. Sci. Food Agric. 2019, 99, 5926–5933. [Google Scholar] [CrossRef]
- Juan, J.; Yang, H. Prevalence, Prevention, and Lifestyle Intervention of Gestational Diabetes Mellitus in China. Int. J. Environ. Res. Public Health 2020, 17, 9517. [Google Scholar] [CrossRef]
- Alonso-Bastida, A.; Adam-Medina, M.; Posada-Gómez, R.; Salazar-Piña, D.A.; Osorio-Gordillo, G.-L.; Vela-Valdés, L.G. Dyn amic of Glucose Homeostasis in Virtual Patients: A Comparison between Different Behaviors. Int. J. Environ. Res. Public Health 2022, 19, 716. [Google Scholar] [CrossRef]
- Das, A.K.; Saboo, B.; Maheshwari, A.; Nair, V.M.; Banerjee, S.; Jayakumar, C.; Benny, P.V.; Prasobh, P.S.; Mohan, A.R.; Potty, V.S.; et al. Health care delivery model in India with relevance to diabetes care. Heliyon 2022, 8, e10904. [Google Scholar] [CrossRef]
- Erzse, A.; Stacey, N.; Chola, L.; Tugendhaft, A.; Freeman, M.; Hofman, K. The direct medical cost of type 2 diabetes mellitus in South Africa: A cost of illness study. Glob. Health Action 2019, 12, 1636611. [Google Scholar] [CrossRef]
- Standl, E.; Khunti, K.; Hansen, T.B.; Schnell, O. The global epidemics of diabetes in the 21st century: Current situation and perspectives. Eur. J. Prev. Cardiol. 2019, 26 (Suppl. 2), 7–14. [Google Scholar] [CrossRef]
- Man, A.W.C.; Li, H.; Xia, N. Impact of Lifestyles (Diet and Exercise) on Vascular Health: Oxidative Stress and Endothelial Function. Oxidative Med. Cell. Longev. 2020, 2020, 1496462. [Google Scholar] [CrossRef]
- Dahl, K.; Brooks, A.; Almazedi, F.; Hoff, S.T.; Boschini, C.; Bækdal, T.A. Oral semaglutide improves postprandial glucose and lipid metabolism, and delays gastric emptying, in subjects with type 2 diabetes. Diabetes Obes. Metab. 2021, 23, 1594–1603. [Google Scholar] [CrossRef]
- Rayner, C.K.; Watson, L.E.; Phillips, L.K.; Lange, K.; Bound, M.J.; Grivell, J.; Wu, T.; Jones, K.L.; Horowitz, M.; Ferrannini, E.; et al. Effects of Sustained Treatment With Lixisenatide on Gastric Emptying and Postprandial Glucose Metabolism in Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2020, 43, 1813–1821. [Google Scholar] [CrossRef]
- Vlachos, D.; Malisova, S.; Lindberg, F.A.; Karaniki, G. Glycemic Index (GI) or Glycemic Load (GL) and Dietary Interventions for Optimizing Postprandial Hyperglycemia in Patients with T2 Diabetes: A Review. Nutrients 2020, 12, 1561. [Google Scholar] [CrossRef]
- Yabe, D.; Kuwata, H.; Fujiwara, Y.; Sakaguchi, M.; Moyama, S.; Makabe, N.; Murotani, K.; Asano, H.; Ito, S.; Mishima, H.; et al. Dietary instructions focusing on meal-sequence and nutritional balance for prediabetes subjects: An exploratory, cluster-randomized, prospective, open-label, clinical trial. J. Diabetes Complicat. 2019, 33, 107450. [Google Scholar] [CrossRef] [PubMed]
- Shapira, N. The Metabolic Concept of Meal Sequence vs. Satiety: Glycemic and Oxidative Responses with Reference to Inflammation Risk, Protective Principles and Mediterranean Diet. Nutrients 2019, 11, 2373. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Goh, H.J.; Govindharajulu, P.; Leow, M.K.-S.; Henry, C.J. Postprandial glucose, insulin and incretin responses differ by test meal macronutrient ingestion sequence (PATTERN study). Clin. Nutr. 2020, 39, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Kubota, S.; Liu, Y.; Iizuka, K.; Kuwata, H.; Seino, Y.; Yabe, D. A Review of Recent Findings on Meal Sequence: An Attractive Dietary Approach to Prevention and Management of Type 2 Diabetes. Nutrients 2020, 12, 2502. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Blum, A. Freestyle Libre Glucose Monitoring System. Clin. Diabetes 2018, 36, 203–204. [Google Scholar] [CrossRef]
- Leelarathna, L.; Beck, R.W.; Bergenstal, R.M.; Thabit, H.; Hovorka, R. Glucose Management Indicator (GMI): Insights and Validation Using Guardian 3 and Navigator 2 Sensor Data. Diabetes Care 2019, 42, e60–e61. [Google Scholar] [CrossRef]
- Interpretation of continuous glucose monitoring data: Glycemic variability and quality of glycemic control. Diabetes Technol. Ther. 2009, 11 (Suppl. 1), S55–S67. [CrossRef]
- Xiao, Q.; Garaulet, M.; Scheer, F.A. Meal timing and obesity: Interactions with macronutrient intake and chronotype. Int. J. Obes. 2019, 43, 1701–1711. [Google Scholar] [CrossRef]
- Paoli, A.; Tinsley, G.; Bianco, A.; Moro, T. The Influence of Meal Frequency and Timing on Health in Humans: The Role of Fasting. Nutrients 2019, 11, 719. [Google Scholar] [CrossRef]
- Henry, C.J.; Kaur, B.; Quek, R.Y.C. Chrononutrition in the management of diabetes. Nutr. Diabetes 2020, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- King, D.G.; Walker, M.; Campbell, M.D.; Breen, L.; Stevenson, E.J.; West, D.J. A small dose of whey protein co-ingested with mixed-macronutrient breakfast and lunch meals improves postprandial glycemia and suppresses appetite in men with type 2 diabetes: A randomized controlled trial. Am. J. Clin. Nutr. 2018, 107, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Juárez-Ramírez, C.; Théodore, F.L.; Villalobos, A.; Allen-Leigh, B.; Jiménez-Corona, A.; Nigenda, G.; Lewis, S. The importance of the cultural dimension of food in understanding the lack of adherence to diet regimens among Mayan people with diabetes. Public Health Nutr. 2019, 22, 3238–3249. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.; Martins, S.; Fernandes, L. Adherence to Medication, Physical Activity and Diet in Older Adults With Diabetes: Its Association With Cognition, Anxiety and Depression. J. Clin. Med. Res. 2019, 11, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Yong, G.; Jing, Q.; Yao, Q.; Yang, K.; Ye, X. Changing Meal Sequence Affects Glucose Excursions in Gestational Diabetes Mellitus. J. Diabetes Res. 2022, 2022, 7083106. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Physiological Characteristics | Test 1 | Test 2 | Test 3 |
|---|---|---|---|
| Body weight (kg) | 65.4 | 67.1 | 64.6 |
| Body mass index (kg/m2) | 20.6 | 21.2 | 20.4 |
| Abdominal circumference (m) | 0.79 | 0.79 | 0.79 |
| Muscle percentage (%) | 42.0 | 41.8 | 43.7 |
| Fat percentage (%) | 14.8 | 15.6 | 12.4 |
| Visceral fat percentage (%) | 3 | 3 | 3 |
| Test 2. Regular Diet with Ordered Food Consumption | |||||
| Day | Breakfast | Snack 1 | Lunch | Dinner | Snack 2 |
| 1 | D-P-CH | D-CH-FR | VF-CH-P-FT | P-CH-VF-FR | FT |
| 2 | P-CH-D | D-CH-FR | CH-P-CH-FT-VF | CH-VF-FR-P | FT |
| 3 | D-P-CH | D-CH-FR | P-CH-FT-VF-CH | VF-FR-P-CH | FT |
| 4 | P-CH-D | D-CH-FR | CH-FT-VF-CH-P | FR-P-CH-VF | FT |
| 5 | D-P-CH | D-CH-FR | FT-VF-CH-P-CH | P-CH-VF-FR | FT |
| 6 | P-CH-D | D-CH-FR | VF-CH-P-CH-FT | CH-VF-FR-P | FT |
| 7 | D | D-CH-FR | CH-P-CH-FT-VF | VF-FR-P-CH | FT |
| 8 | P-CH-D | D-CH-FR | P-CH-FT-VF-CH | FR-P-CH-VF | FT |
| 9 | D-P-CH | D-CH-FR | CH-FT-VF-CH-P | FT-CH-VF-FR | FT |
| 10 | P-CH-D | D-CH-FR | FT-VF-CH-P-CH | CH-VF-FR-FT | FT |
| 11 | D-P-CH | D-CH-FR | VF-CH-P-CH-FT | VF-FR-FT-CH | FT |
| 12 | P-CH-D | D-CH-FR | CH-P-CH-FT-VF | FR-FT-CH-VF | FT |
| 13 | D-P-CH | D-CH-FR | P-CH-FT-VF-CH | CH-P-VF-FT | FT |
| 14 | D | D-CH-FR | CH-FT-VF-CH-P | CH-P-FT | FT |
| Test 3. Assisted diet with ordered food consumption | |||||
| Day | Breakfast | Snack 1 | Lunch | Dinner | Snack 2 |
| 1 | CH-P-VF | D-FR | P-VF-CH | CH-P-VF-FT | FR-VF-FT |
| 2 | P-CH-VF | D-FR | CH-P-CH-VF | FT-P-CH-VF | FT-FR-VF |
| 3 | VF-P-CH | D-FR | CH-VF-P-CH | P-FT-VF-CH | VF-FT-FR |
| 4 | VF-P-CH | D-FR | VF-CH-P | VF-CH-FT-P | FR-VF-FT |
| 5 | CH-P-VF | D-FR | P-VF-CH | CH-P-D-VF | FR-CH-FT |
| 6 | P-CH-VF | D-FR-D | CH-P-VF-CH | VF-D-CH-P | FT-FR-CH |
| 7 | VF-P-CH | D-FR-D | VF-CH-P-CH | CH-VF-D-P | CH-FT-FR |
| 8 | VF-CH-P | D-FR-D | CH-VF-P | VF-D-P-CH | FR-CH-FT |
| 9 | P-D-VF-CH | D-FR | P-CH-VF-CH | CH-D-VF-FT | FR-CH-FT |
| 10 | VF-CH-P-D | D-FR | CH-P-CH-VF | VF-FT-CH-D | CH-FR-FT |
| 11 | CH-P-D-VF | D-FR | VF-CH-P-CH | FT-D-VF-CH | FT-CH-FR |
| 12 | P-D-VF-CH | D-FR-D | P-VF-CH | D-VF-FT-CH | FR-CH-FT |
| 13 | VF-P-D-CH | D-FR-D | CH-P-CH-VF | CH-P-VF-FT | CH-FT-FR |
| 14 | CH-P-D-VF | D-FR-D | VF-CH-P | CH-D-VF-FT | FT-FR-CH |
| Aspect Analyzed | Test 1 | Test 2 | Test 3 |
|---|---|---|---|
| Total calories (Cal) | Breakfast: 1079.60 95 Lunch: 919.29 332 Dinner: 707.47 Snack 1: 435.66 12 Snack 2: 241.13 | Breakfast: 332.27 Lunch: 1197.30.0 Dinner: 572.44 218 Snack 1: 316.50 Snack 2: 86.23 | Breakfast: 335.00 Lunch: 490.01 Dinner: 387.36 Snack 1: 596.21 27 Snack 2: 260.38 44 |
| Carbohydrates (g) | Breakfast: 141.50 Lunch: 136.46 85 Dinner: 79.38 Snack 1: 36.51 7 Snack 2: 28.03 | Breakfast: 40.82 Lunch: 182.10 70 Dinner: 52.98 13 Snack 1: 40.51 33 Snack 2: 2.69 1 | Breakfast: 30.18 Lunch: 65.43 Dinner: 33.85 5 Snack 1: 73.10 6 Snack 2: 41.50 6 |
| Carbohydrate (Cal) (%) Energy proportion | Breakfast: 566.00 (52 3)% Lunch: 545.86 343 (55 17)% Dinner: 317.53 (44 7)% Snack 1: 146.04 31 (33 6)% Snack 2: 112.13 (47 18)% | Breakfast: 162.87 (47 15)% Lunch: 728.40 282 (58 12)% Dinner: 211.94 54 (39 11)% Snack 1: 149.74 137 (40 17)% Snack 2: 10.76 4 (12 3)% | Breakfast: 120.74 (35 5)% Lunch: 261.72 (54 8)% Dinner: 135.40 20 (34 1)% Snack 1: 292.42 26 (48 2)% Snack 2: 166.03 26 (63 1)% |
| Lipids (g) | Breakfast: 37.30 Lunch: 26.96 11 Dinner: 25.22 Snack 1: 16.02 0.2 Snack 2: 8.28 | Breakfast: 7.61 Lunch: 33.15 12 Dinner: 26.36 5 Snack 1: 4.25 4 Snack 2: 7.18 2 | Breakfast: 14.07 2 Lunch: 8.40 2 Dinner: 15.73 Snack 1: 17.32 0.1 Snack 2: 8.59 2 |
| Lipid Calories (Cal) (%) Energy proportion | Breakfast: 335.42 (30 4)% Lunch: 242.70 (30 15)% Dinner: 227.02 (30 6)% Snack 1: 144.26 (33 1)% Snack 2: 74.56 49 (35 )% | Breakfast: 68.54 42 (18 8)% Lunch: 301.14 113 (27 10)% Dinner: 105.44 23 (39 17)% Snack 1: 38.26 18 (12 5)% Snack 2: 64.65 23 (75 6)% | Breakfast: 126.68 24 (38 5)% Lunch: 75.64 24 (15 2)% Dinner: 141.58 45 (36 7)% Snack 1: 155.95 1 (26 1)% Snack 2: 77.36 18 (29 2)% |
| Protein (g) | Breakfast: 44.53 4 Lunch: 32.68 Dinner: 40.72 Snack 1: 36.3 3 Snack 2: 13.60 | Breakfast: 25.26 Lunch: 42.11 11 Dinner: 26.36 5 Snack 1: 32.12 6 Snack 2: 2.70 1 | Breakfast: 21.89 Lunch: 38.16 15 Dinner: 27.59 6 Snack 1: 36.95 0.5 Snack 2: 4.24 1 |
| Protein Calories (Cal) (%) Energy proportion | Breakfast: 178.15 (16 3)% Lunch: 130.73 (14 3)% Dinner: 162.91 75 (24 9)% Snack 1: 145.3 (33 4)% Snack 2: 54.43 (16 15)% | Breakfast: 101.07 (26 10)% Lunch: 167.15 46 (14 3)% Dinner: 105.44 23 (21 10)% Snack 1: 128.48 25 (46 16)% Snack 2: 10.80 6 (12 4)% | Breakfast: 87.57 14 (26 3)% Lunch: 152.64 63 (30 7)% Dinner: 110.3 27 (28 7)% Snack 1: 147.83 2 (24 )% Snack 2: 16.98 4 (6 1)% |
| Test Number | Glucose Average (mg/dL) | Glucose Management Indicator (%) | Coefficient of Glucose Variation (%) |
|---|---|---|---|
| Test 1 | 13.77 | 5.32 | 16.39 |
| Test 2 | 14.49 | 5.43 | 16.31 |
| Test 3 | 11.93 | 5.53 | 12.81 |
| Intake | Test 1 (mg/dL) | Test 2 (mg/dL) | Test 3 (mg/dL) |
|---|---|---|---|
| Breakfast | 1.87 | 2.28 | 2.27 |
| Lunch | 4.02 | 5.60 | 2.83 |
| Dinner | 4.62 | 7.02 | 3.58 |
| Snack 1 | 3.66 | 4.59 | 2.26 |
| Snack 2 | 3.43 | 1.81 | 3.84 |
| First Macronutrient Ingested | Glucose Average (mg/dL) | Maximum Peak (mg/dL) | Peak Time (h) | Stabilization Time (h) |
|---|---|---|---|---|
| Carbohydrates | 4 3 7 | 11 12 20 | 1.2 1.8 1.3 | 1.0 1.2 0.8 |
| Vegetables and Fiber | 4 14 3 | 5 16 6 | 1.0 1.9 1.3 | 1.3 1.1 0.9 |
| Proteins of animal origin | 5 3 11 | 11 14 24 | 0.9 1.5 1.9 | 1.0 0.9 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Bastida, A.; Adam-Medina, M.; Salazar-Piña, D.-A.; Escobar-Jiménez, R.-F.; Parra-Cabrera, M.-S.; Cervantes-Bobadilla, M. Impact on Glycemic Variation Caused by a Change in the Dietary Intake Sequence. Foods 2023, 12, 1055. https://doi.org/10.3390/foods12051055
Alonso-Bastida A, Adam-Medina M, Salazar-Piña D-A, Escobar-Jiménez R-F, Parra-Cabrera M-S, Cervantes-Bobadilla M. Impact on Glycemic Variation Caused by a Change in the Dietary Intake Sequence. Foods. 2023; 12(5):1055. https://doi.org/10.3390/foods12051055
Chicago/Turabian StyleAlonso-Bastida, Alexis, Manuel Adam-Medina, Dolores-Azucena Salazar-Piña, Ricardo-Fabricio Escobar-Jiménez, María-Socorro Parra-Cabrera, and Marisol Cervantes-Bobadilla. 2023. "Impact on Glycemic Variation Caused by a Change in the Dietary Intake Sequence" Foods 12, no. 5: 1055. https://doi.org/10.3390/foods12051055
APA StyleAlonso-Bastida, A., Adam-Medina, M., Salazar-Piña, D.-A., Escobar-Jiménez, R.-F., Parra-Cabrera, M.-S., & Cervantes-Bobadilla, M. (2023). Impact on Glycemic Variation Caused by a Change in the Dietary Intake Sequence. Foods, 12(5), 1055. https://doi.org/10.3390/foods12051055