
Efficacy of Plant Sterol-Enriched Food for Primary Prevention and Treatment of Hypercholesterolemia: A Systematic Literature Review

 , ,
, ,  , and
, and 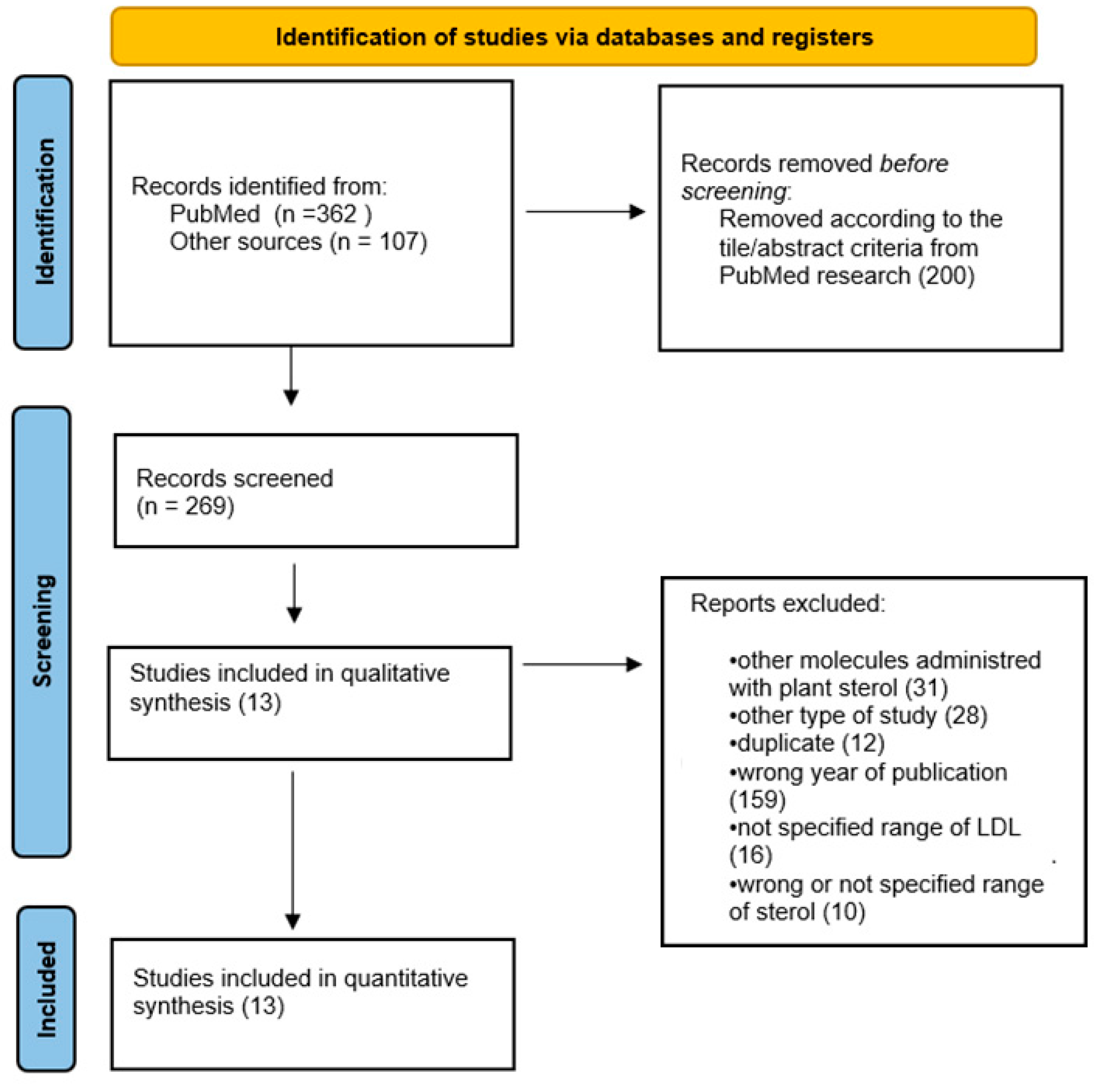{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Strategy
2.2. Selection Criteria
2.3. Data extraction and Quality Assessment
2.4. Data Analysis
3. Results
3.1. Studies Description
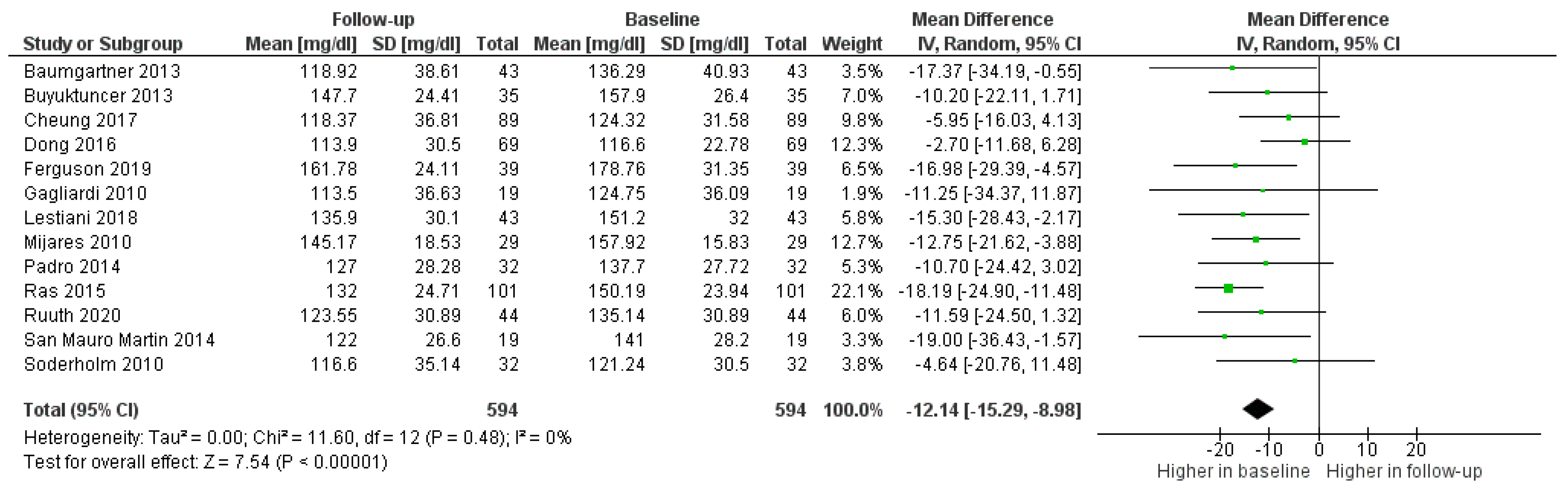
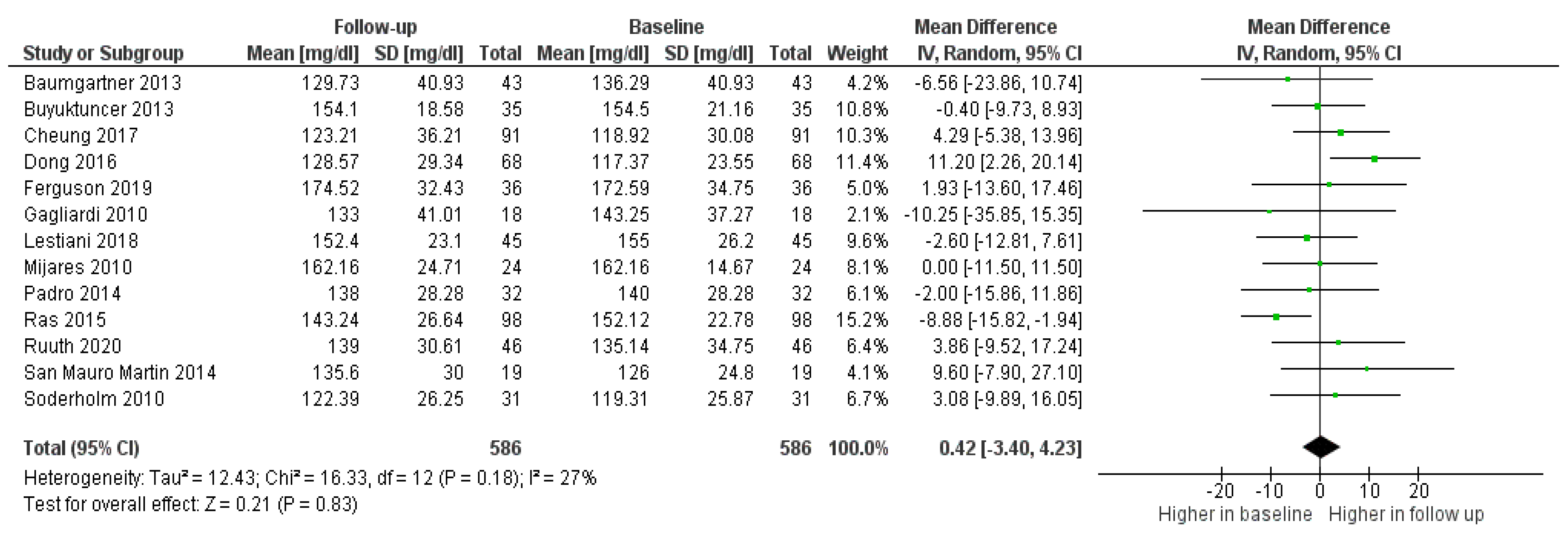
3.2. Impact of Foods Enriched with PSs
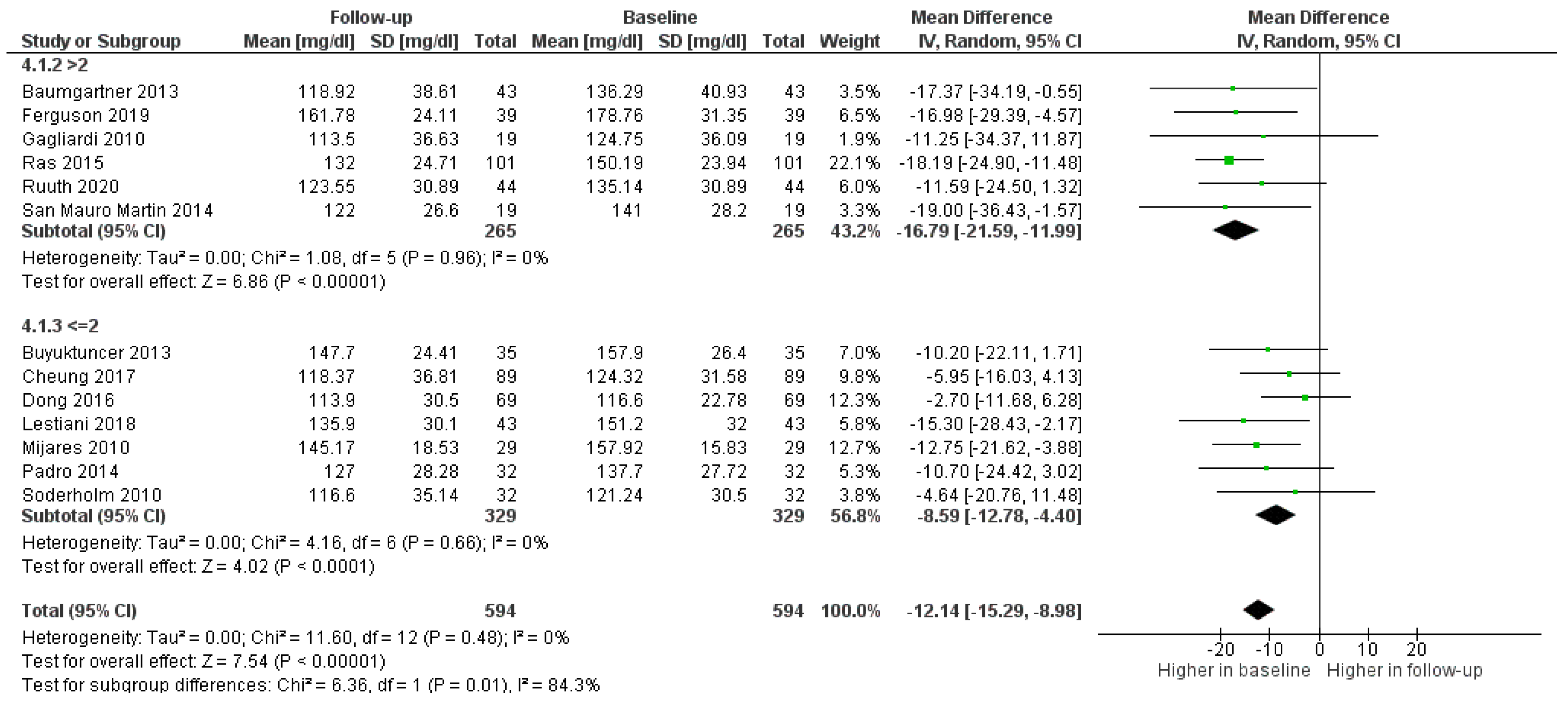
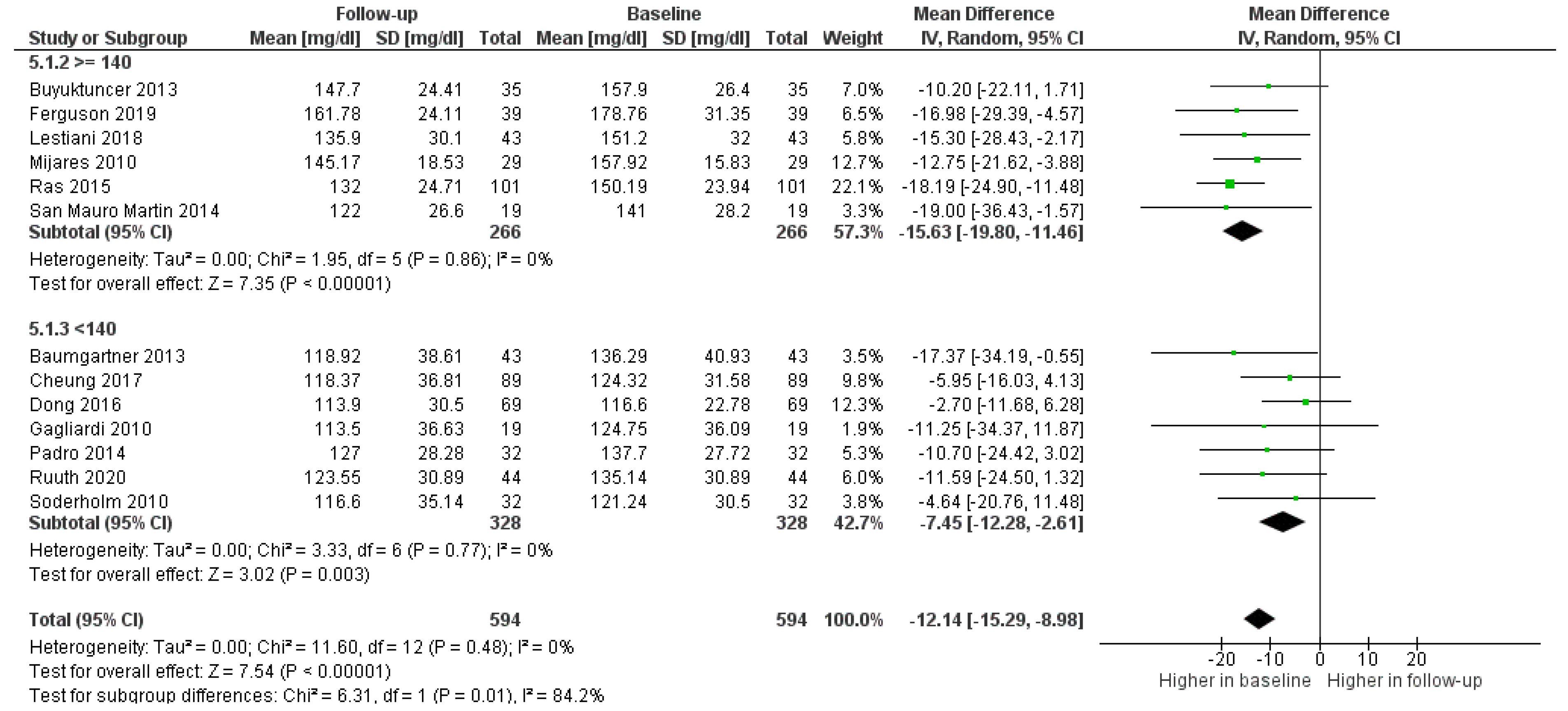
3.3. Effect of PS Dosage
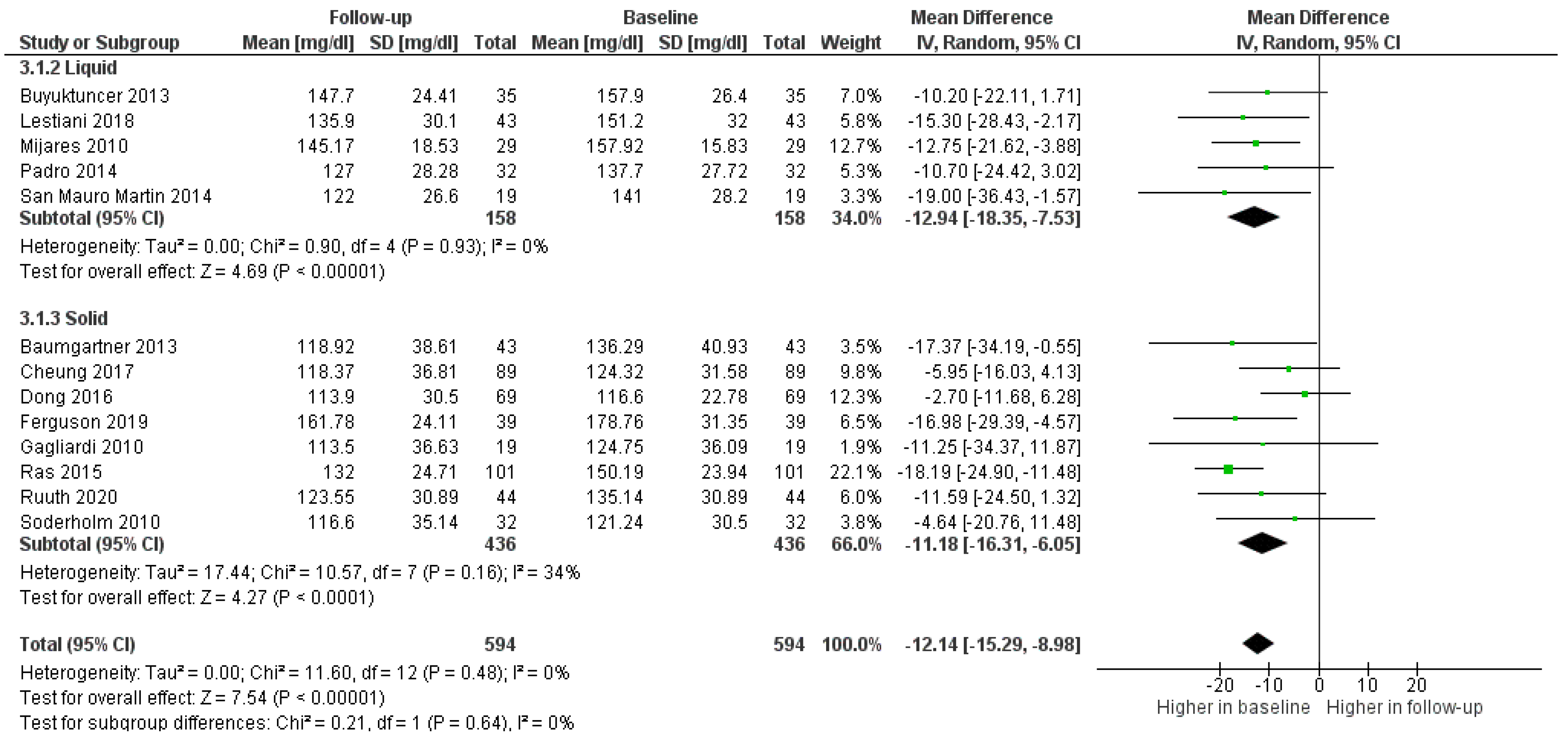
3.4. Impact of Matrix
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- WHO. Mortality and Global Health Estimates. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 16 July 2021).
- ISS. Colesterolo e Ipercolesterolemia. Available online: https://www.epicentro.iss.it/colesterolo/ (accessed on 16 July 2021).
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef] [PubMed]
- Hirowatari, Y.; Manita, D.; Kamachi, K.; Tanaka, A. Effect of dietary modification by calorie restriction on cholesterol levels in lipoprotein(a) and other lipoprotein classes. Ann. Clin. Biochem. 2017, 54, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Cusack, L.K.; Fernandez, M.L.; Volek, J.S. The Food Matrix and Sterol Characteristics Affect the Plasma Cholesterol Lowering of Phytosterol/Phytostanol. Adv. Nutr. 2013, 4, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Talati, R.; Sobieraj, D.M.; Makanji, S.S.; Phung, O.J.; Coleman, C.I. The Comparative Efficacy of Plant Sterols and Stanols on Serum Lipids: A Systematic Review and Meta-Analysis. J. Am. Diet. Assoc. 2010, 110, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Seppo, L.; Jauhiainen, T.; Nevala, R.; Poussa, T.; Korpela, R. Plant stanol esters in low-fat milk products lower serum total and LDL cholesterol. Eur. J. Nutr. 2007, 46, 111–117. [Google Scholar] [CrossRef]
- AbuMweis, S.S.; Barake, R.; Jones, P.J. Plant sterols/stanols as cholesterol lowering agents: A meta-analysis of randomized controlled trials. Food Nutr. Res. 2008, 52, 1–18. [Google Scholar] [CrossRef]
- Rocha, M.; Bañuls, C.; Bellod, L.; Jover, A.; Victor, V.; Mijares, A.H. A Review on the Role of Phytosterols: New Insights into Cardiovascular Risk. Curr. Pharm. Des. 2012, 17, 4061–4075. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, I. Factors Affecting Intestinal Absorption of Cholesterol and Plant Sterols and Stanols. J. Oleo Sci. 2015, 64, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Ash, M.M.; Hang, J.; Dussault, P.H.; Carr, T.P. Phytosterol stearate esters elicit similar responses on plasma lipids and cholesterol absorption but different responses on fecal neutral sterol excretion and hepatic free cholesterol in male Syrian hamsters. Nutr. Res. 2011, 31, 537–543. [Google Scholar] [CrossRef]
- Lu, T.T.; Makishima, M.; Repa, J.; Schoonjans, K.; Kerr, T.A.; Auwerx, J.; Mangelsdorf, D.J. Molecular Basis for Feedback Regulation of Bile Acid Synthesis by Nuclear Receptors. Mol. Cell 2000, 6, 507–515. [Google Scholar] [CrossRef]
- Gylling, H.; Simonen, P. Phytosterols, Phytostanols, and Lipoprotein Metabolism. Nutrients 2015, 7, 7965–7977. [Google Scholar] [CrossRef] [PubMed]
- Blom, W.A.M.; Koppenol, W.P.; Hiemstra, H.; Stojakovic, T.; Scharnagl, H.; Trautwein, E.A. A low-fat spread with added plant sterols and fish omega-3 fatty acids lowers serum triglyceride and LDL-cholesterol concentrations in individuals with modest hypercholesterolaemia and hypertriglyceridaemia. Eur. J. Nutr. 2019, 58, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- Catapano, A.L.; Reiner, Z.; De Backer, G.; Graham, I.; Taskinen, M.-R.; Wiklund, O.; Agewall, S.; Alegria, E.; Chapman, M.J.; Durrington, P.; et al. ESC/EAS Guidelines for the management of dyslipidaemias. Atherosclerosis 2011, 217, S1–S44. [Google Scholar] [CrossRef] [PubMed]
- Cater, N.B.; Garcia-Garcia, A.-B.; Vega, G.L.; Grundy, S.M. Responsiveness of Plasma Lipids and Lipoproteins to Plant Stanol Esters. Am. J. Cardiol. 2005, 96, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.J.A.; Wolska, A.; Remaley, A.T.; Stojanovski, E.; MacDonald-Wicks, L.; Garg, M.L. Bread enriched with phytosterols with or without curcumin modulates lipoprotein profiles in hypercholesterolaemic individuals. A randomised controlled trial. Food Funct. 2019, 10, 2515–2527. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, A.C.M.; Maranhão, R.C.; de Sousa, H.P.; Schaefer, E.J.; Santos, R.D. Effects of margarines and butter consumption on lipid profiles, inflammation markers and lipid transfer to HDL particles in free-living subjects with the metabolic syndrome. Eur. J. Clin. Nutr. 2010, 64, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.L.; Ho, D.K.C.; Sing, C.W.; Tsoi, M.F.; Cheng, V.K.F.; Lee, G.K.Y.; Ho, Y.N.; Cheung, B.M.Y. Randomized controlled trial of the effect of phytosterols-enriched low-fat milk on lipid profile in Chinese. Sci. Rep. 2017, 7, 41084. [Google Scholar] [CrossRef]
- Dong, S.; Zhang, R.; Ji, Y.-C.; Hao, J.-Y.; Ma, W.-W.; Chen, X.-D.; Xiao, R.; Yu, H.-L. Soy milk powder supplemented with phytosterol esters reduced serum cholesterol level in hypercholesterolemia independently of lipoprotein E genotype: A random clinical placebo-controlled trial. Nutr. Res. 2016, 36, 879–884. [Google Scholar] [CrossRef]
- Söderholm, P.P.; Alfthan, G.; Koskela, A.; Adlercreutz, H.; Tikkanen, M. The effect of high-fiber rye bread enriched with nonesterified plant sterols on major serum lipids and apolipoproteins in normocholesterolemic individuals. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Ruuth, M.; Äikäs, L.; Tigistu-Sahle, F.; Käkelä, R.; Lindholm, H.; Simonen, P.; Kovanen, P.T.; Gylling, H.; Öörni, K. Plant Stanol Esters Reduce LDL (Low-Density Lipoprotein) Aggregation by Altering LDL Surface Lipids: The BLOOD FLOW Randomized Intervention Study. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2310–2321. [Google Scholar] [CrossRef] [PubMed]
- Ras, R.T.; Fuchs, D.; Koppenol, W.P.; Garczarek, U.; Greyling, A.; Keicher, C.; Verhoeven, C.; Bouzamondo, H.; Wagner, F.; Trautwein, E.A. The effect of a low-fat spread with added plant sterols on vascular function markers: Results of the Investigating Vascular Function Effects of Plant Sterols (INVEST) study. Am. J. Clin. Nutr. 2015, 101, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Lestiani, L.; Chandra, D.N.; Laitinen, K.; Ambarwati, F.D.; Kuusisto, P.; Lukito, W. Double-Blind Randomized Placebo Controlled Trial Demonstrating Serum Cholesterol Lowering Efficacy of a Smoothie Drink with Added Plant Stanol Esters in an Indonesian Population. Cholesterol 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Baumgartner, S.; Mensink, R.P.; Husche, C.; Lütjohann, D.; Plat, J. Effects of plant sterol- or stanol-enriched margarine on fasting plasma oxyphytosterol concentrations in healthy subjects. Atherosclerosis 2013, 227, 414–419. [Google Scholar] [CrossRef][Green Version]
- Padro, T.; Vilahur, G.; Sánchez-Hernández, J.; Hernández, M.; Antonijoan, R.M.; Perez, A.; Badimon, L. Lipidomic changes of LDL in overweight and moderately hypercholesterolemic subjects taking phytosterol- and omega-3-supplemented milk. J. Lipid Res. 2015, 56, 1043–1056. [Google Scholar] [CrossRef]
- Hernández-Mijares, A.; Bañuls, C.; Rocha, M.; Morillas, C.; Martínez-Triguero, M.L.; Víctor, V.M.; Lacomba, R.; Alegría, A.; Barberá, R.; Farré, R.; et al. Effects of phytosterol ester-enriched low-fat milk on serum lipoprotein profile in mildly hypercholesterolaemic patients are not related to dietary cholesterol or saturated fat intake. Br. J. Nutr. 2010, 104, 1018–1025. [Google Scholar] [CrossRef]
- San Mauro Martín, I.; Collado Yurrita, L.; Cuadrado Cenzual, M.Á.; Hernández Cabria, M.; Calle Purón, M.E. Manejo del riesgo de enfermedad cardiovascular con leche enriquecida en esteroles en población joven adulta; ensayo clínico controlado aleatorizado y cruzado. Nutr. Hosp. 2014, 30, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Buyuktuncer, Z.; Fisunoğlu, M.; Guven, G.S.; Unal, S.; Besler, H.T. The cholesterol lowering efficacy of plant stanol ester yoghurt in a Turkish population: A double-blind, placebo-controlled trial. Lipids Heal. Dis. 2013, 12, 91–98. [Google Scholar] [CrossRef]
- Moreau, R.A.; Nyström, L.; Whitaker, B.D.; Winkler-Moser, J.K.; Baer, D.J.; Gebauer, S.K.; Hicks, K.B. Phytosterols and their derivatives: Structural diversity, distribution, metabolism, analysis, and health-promoting uses. Prog. Lipid Res. 2018, 70, 35–61. [Google Scholar] [CrossRef]
- von Bergmann, K.; Sudhop, T.; Lütjohann, D. Cholesterol and Plant Sterol Absorption: Recent Insights. Am. J. Cardiol. 2005, 96, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.T.; Wesley, R.; Shamburek, R.D.; Pucino, F.; Csako, G. Meta-Analysis of Natural Therapies for Hyperlipidemia: Plant Sterols and Stanols versus Policosanol. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2005, 25, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Gylling, H.; Hallikainen, M.; Nissinen, M.J.; Miettinen, T.A. The effect of a very high daily plant stanol ester intake on serum lipids, carotenoids, and fat-soluble vitamins. Clin. Nutr. 2010, 29, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.; Malarski, A.; Reuther, C.; Kertscher, R.; Kiehntopf, M.; Jahreis, G. Milk phospholipid and plant sterol-dependent modulation of plasma lipids in healthy volunteers. Eur. J. Nutr. 2013, 52, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Vásquez-Trespalacios, E.M.; Romero-Palacio, J. Efficacy of yogurt drink with added plant stanol esters (Benecol®, Colanta) in reducing total and LDL cholesterol in subjects with moderate hypercholesterolemia: A randomized placebo-controlled crossover trial NCT01461798. Lipids Health Dis. 2014, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mannarino, E.; Pirro, M.; Cortese, C.; Lupattelli, G.; Siepi, D.; Mezzetti, A.; Bertolini, S.; Parillo, M.; Fellin, R.; Pujia, A.; et al. Effects of a phytosterol-enriched dairy product on lipids, sterols and 8-isoprostane in hypercholesterolemic patients: A multicenter Italian study. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Bouhairie, V.E.; Goldberg, A.C. Familial Hypercholesterolemia. Endocrinol. Metab. Clin. North Am. 2016, 45, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Paramsothy, P.; Knopp, R.H.; Kahn, S.E.; Retzlaff, B.M.; Fish, B.; Ma, L.; Ostlund, R.E. Plasma sterol evidence for decreased absorption and increased synthesis of cholesterol in insulin resistance and obesity. Am. J. Clin. Nutr. 2011, 94, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Gylling, H.; Laaksonen, D.E.; Atalay, M.; Hallikainen, M.; Niskanen, L.; Miettinen, T.A. Markers of absorption and synthesis of cholesterol in men with type 1 diabetes. Diabetes/Metabolism Res. Rev. 2006, 23, 372–377. [Google Scholar] [CrossRef]
- Demonty, I.; Ras, R.T.; van der Knaap, H.C.M.; Duchateau, G.S.M.J.E.; Meijer, L.; Zock, P.L.; Geleijnse, J.M.; Trautwein, E.A. Continuous Dose-Response Relationship of the LDL-Cholesterol–Lowering Effect of Phytosterol Intake. J. Nutr. 2009, 139, 271–284. [Google Scholar] [CrossRef]
- Gylling, H.; Hallikainen, M.; Nissinen, M.J.; Simonen, P.; Miettinen, T.A. Very high plant stanol intake and serum plant stanols and non-cholesterol sterols. Eur. J. Nutr. 2010, 49, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, K.; Gylling, H. Dose-dependent LDL-cholesterol lowering effect by plant stanol ester consumption: Clinical evidence. Lipids Health Dis. 2012, 11, 140. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.; Derosa, G.; Pisciotta, L.; Barbagallo, C.; for the SISA-PUFACOL Study Group. Testing the Short-Term Efficacy of a Lipid-Lowering Nutraceutical in the Setting of Clinical Practice: A Multicenter Study. J. Med. Food 2015, 18, 1270–1273. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turini, E.; Sarsale, M.; Petri, D.; Totaro, M.; Lucenteforte, E.; Tavoschi, L.; Baggiani, A. Efficacy of Plant Sterol-Enriched Food for Primary Prevention and Treatment of Hypercholesterolemia: A Systematic Literature Review. Foods 2022, 11, 839. https://doi.org/10.3390/foods11060839
Turini E, Sarsale M, Petri D, Totaro M, Lucenteforte E, Tavoschi L, Baggiani A. Efficacy of Plant Sterol-Enriched Food for Primary Prevention and Treatment of Hypercholesterolemia: A Systematic Literature Review. Foods. 2022; 11(6):839. https://doi.org/10.3390/foods11060839
Chicago/Turabian StyleTurini, Elisa, Miriana Sarsale, Davide Petri, Michele Totaro, Ersilia Lucenteforte, Lara Tavoschi, and Angelo Baggiani. 2022. "Efficacy of Plant Sterol-Enriched Food for Primary Prevention and Treatment of Hypercholesterolemia: A Systematic Literature Review" Foods 11, no. 6: 839. https://doi.org/10.3390/foods11060839
APA StyleTurini, E., Sarsale, M., Petri, D., Totaro, M., Lucenteforte, E., Tavoschi, L., & Baggiani, A. (2022). Efficacy of Plant Sterol-Enriched Food for Primary Prevention and Treatment of Hypercholesterolemia: A Systematic Literature Review. Foods, 11(6), 839. https://doi.org/10.3390/foods11060839