
Glycemic Index of Gluten-Free Bread and Their Main Ingredients: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Information Sources
2.4. Search Strategy
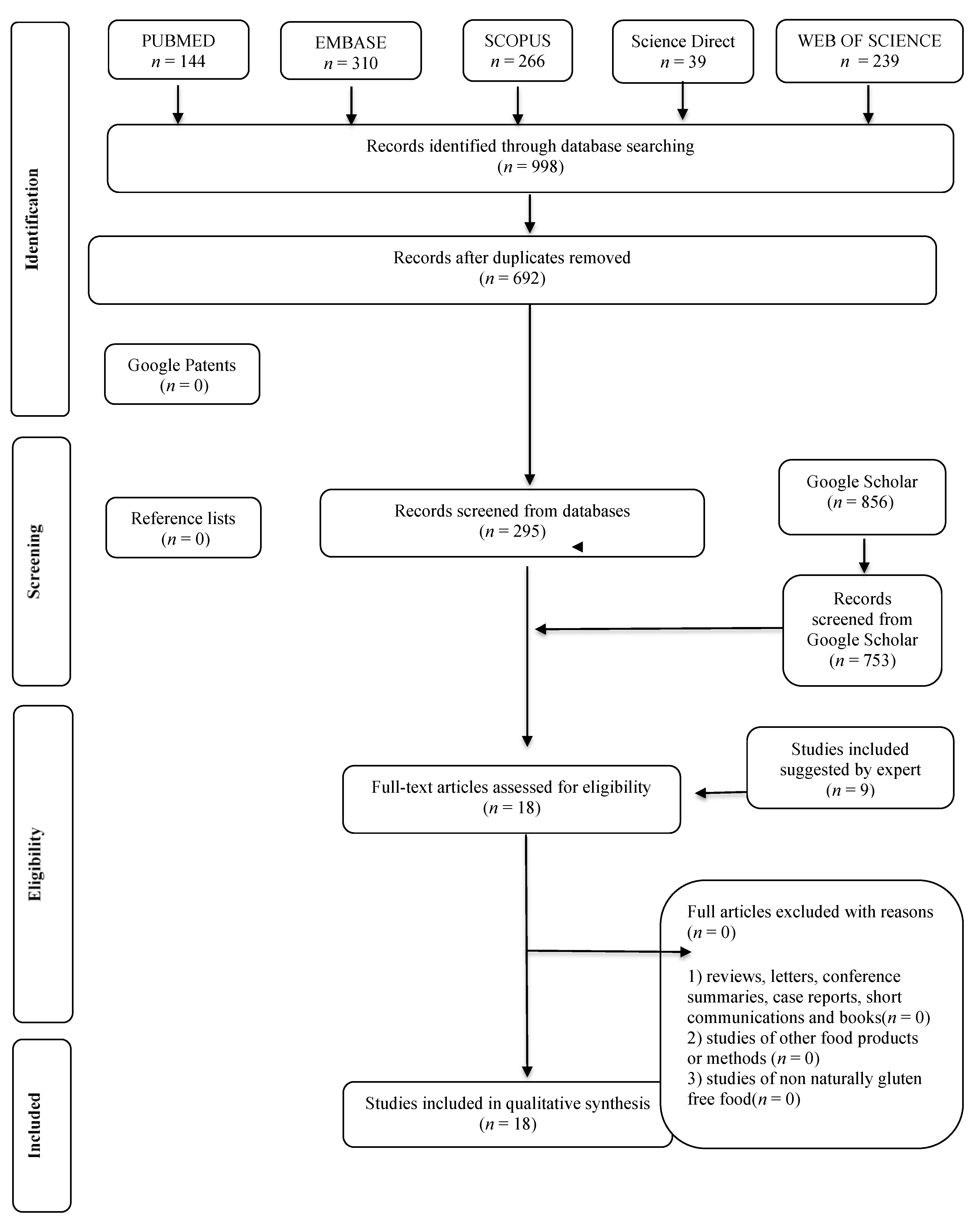
2.5. Study Selection
2.6. Data Collection Process
2.7. Risk of Bias
2.8. Meta-Analysis
3. Results
Studies General Characteristics
4. Discussion
4.1. Differences between the Used Methods to Evaluate the GI
4.2. Gluten-Free Bread Samples: GI and Main Ingredients
4.3. Glycemic Index Role in GRD
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pellegrini, N.; Agostoni, C. Nutritional aspects of gluten-free products. J. Sci. Food Agric. 2015, 95, 2380–2385. [Google Scholar] [CrossRef]
- Menga, V.; Amato, M.; Phillips, T.D.; Angelino, D.; Morreale, F.; Fares, C. Gluten-free pasta incorporating chia (Salvia hispanica L.) as thickening agent: An approach to naturally improve the nutritional profile and the in vitro carbohydrate digestibility. Food Chem. 2017, 221, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Missbach, B.; Schwingshackl, L.; Billmann, A.; Mystek, A.; Hickelsberger, M.; Bauer, G.; König, J. Gluten-free food database: The nutritional quality and cost of packaged gluten-free foods. PeerJ 2015, 3, e1337. [Google Scholar] [CrossRef] [PubMed]
- Cross, C. Gluten-free industry is healthy, but is the food? CMAJ 2013, 185, 4555. [Google Scholar] [CrossRef] [PubMed]
- Bohn, T.; Carriere, F.; Day, L.; Deglaire, A.; Egger, L.; Freitas, D.; Golding, M.; Le Feunteun, S.; Macierzanka, A.; Menard, O.; et al. Correlation between in vitro and in vivo data on food digestion. What can we predict with static in vitro digestion models? Crit. Rev. Food Sci. Nutr. 2017, 8398, 2239–2261. [Google Scholar] [CrossRef]
- Diabetes Canada. Glycemic Index Food Guide; Diabetes Canada: Toronto, ON, Canada, 2016. [Google Scholar]
- American Diabetes Association, A.D. Glycemic Targets: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S61–S70. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.; McMillan-Price, J.; Steinbeck, K.; Caterson, I. Dietary glycemic index: Health implications. J. Am. Coll. Nutr. 2009, 28, 446S–449S. [Google Scholar] [CrossRef] [PubMed]
- FMCG NEWS GLOBAL Global Bread and Bakery Consumption Continues to Experience Modest Growth. Available online: https://www.bizcommunity.com/Article/1/162/176273.html#:~:text=Global%20bread%20and%20bakery%20consumption%20continues%20to%20experience%20moest%20growth,23%20Apr%202018&text=The%20global%20bread%20and%20baery,to%20129%2C000%20tonnes%20in%202016 (accessed on 21 November 2020).
- Eglite, A.; Kunkulberga, D. Bread choice and consumption trends. Foodbalt 2017, 1, 178–182. [Google Scholar] [CrossRef]
- The World Bank. Global Consumption Database: Bread. Available online: https://datatopics.worldbank.org/consumption/product/Bread (accessed on 21 November 2020).
- Houben, A.; Höchstötter, A.; Becker, T. Possibilities to increase the quality in gluten-free bread production: An overview. Eur. Food Res. Technol. 2012, 235, 195–208. [Google Scholar] [CrossRef]
- Zollo, L.; Yoon, S.; Rialti, R.; Ciappei, C. Ethical consumption and consumers’ decision making: The role of moral intuition. Manag. Decis. 2018, 56, 692–710. [Google Scholar] [CrossRef]
- Sanchez, H.D.; Osella, C.A.; Torre, M.A. Optimization of Gluten-Free Bread Prepared from Cornstarch, Rice Flour, and Cassava Starch. J. Food Sci. 2002, 67, 416–419. [Google Scholar] [CrossRef]
- Johnston, C.; Snyder, D.; Smith, C. Commercially available gluten-free pastas elevate postprandial glycemia in comparison to conventional wheat pasta in healthy adults: A double-blind randomized crossover trial. Food Funct. 2017. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.; Frampton, G.; Glanville, J.; Greiner, M.; Higgins, J.P.; Lovei, G.; Oconnor, A.; Pullin, A.; Rajic, A. Application of systematic review methodology to food and feed safety assessments to support decision making. EFSA J. 2010, 8, 1637. [Google Scholar] [CrossRef]
- Handu, D.; Moloney, L.; Wolfram, T.; Ziegler, P.; Acosta, A.; Steiber, A. Academy of Nutrition and Dietetics Methodology for Conducting Systematic Reviews for the Evidence Analysis Library. J. Acad. Nutr. Diet. 2016, 116, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewer’s Manual, 2014th ed.; University of Adelaide: Adelaide, Australia, 2014; ISBN 978-1-920684-11-2. [Google Scholar]
- Capriles, V.A.J. Effects of prebiotic inulin-type fructans on structure, quality, sensory acceptance and glycemic response of gluten-free breads Food & Function. Food Funct. 2013, 4, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Fratelli, C.; Muniz, D.G.; Santos, F.G.; Capriles, V.D. Modelling the effects of psyllium and water in gluten-free bread: An approach to improve the bread quality and glycemic response. J. Funct. Foods 2018, 42, 339–345. [Google Scholar] [CrossRef]
- Giuberti, G.; Fortunati, P.; Gallo, A. Can different types of resistant starch influence the in vitro starch digestion of gluten free breads? J. Cereal Sci. 2016, 70, 253–255. [Google Scholar] [CrossRef]
- Novotni, D.; Čukelj, N.; Smerdel, B.; Bituh, M.; Dujmić, F.; Ćurić, D. Glycemic index and firming kinetics of partially baked frozen gluten-free bread with sourdough. J. Cereal Sci. 2012, 55, 120–125. [Google Scholar] [CrossRef]
- Wolter, A.; Hager, A.S.; Zannini, E.; Arendt, E.K. In vitro starch digestibility and predicted glycaemic indexes of buckwheat, oat, quinoa, sorghum, teff and commercial gluten-free bread. J. Cereal Sci. 2013, 58, 431–436. [Google Scholar] [CrossRef]
- Sciarini, L.S.; Bustos, M.C.; Vignola, M.B.; Paesani, C.; Salinas, C.N.; Pérez, G.T. A study on fibre addition to gluten free bread: Its effects on bread quality and in vitro digestibility. J. Food Sci. Technol. 2017, 54, 244–252. [Google Scholar] [CrossRef]
- Shumoy, H.; Van Bockstaele, F.; Devecioglu, D.; Raes, K. Effect of sourdough addition and storage time on in vitro starch digestibility and estimated glycemic index of tef bread. Food Chem. 2018, 264, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Romão, B.; Botelho, R.B.A.; Alencar, E.R.; da Silva, V.S.N.; Pacheco, M.T.B.; Zandonadi, R.P. Chemical composition and glycemic index of gluten-free bread commercialized in Brazil. Nutrients 2020, 12, 2234. [Google Scholar] [CrossRef] [PubMed]
- Graça, C.; Mota, J.; Lima, A.; Ferreira, R.B.; Raymundo, A.; Sousa, I. Glycemic response and bioactive properties of gluten-free bread with yoghurt or curd-cheese addition. Foods 2020, 9, 1410. [Google Scholar] [CrossRef]
- Liu, X.; Mu, T.; Sun, H.; Zhang, M.; Chen, J.; Fauconnier, M.L. Influence of different hydrocolloids on dough thermo-mechanical properties and in vitro starch digestibility of gluten-free steamed bread based on potato flour. Food Chem. 2018, 239, 1064–1074. [Google Scholar] [CrossRef] [PubMed]
- Feizollahi, E.; Mirmoghtadaie, L.; Mohammadifar, M.A.; Jazaeri, S.; Hadaegh, H.; Nazari, B.; Lalegani, S. Sensory, digestion, and texture quality of commercial gluten-free bread: Impact of broken rice flour type. J. Texture Stud. 2018, 49, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Wolter, A.; Hager, A.S.; Zannini, E.; Arendt, E.K. Influence of sourdough on in vitro starch digestibility and predicted glycemic indices of gluten-free breads. Food Funct. 2014, 5, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Berti, C.; Riso, P.; Monti, L.D.; Porrini, M. In vitro starch digestibility and in vivo glucose response of gluten-free foods and their gluten counterparts. Eur. J. Nutr. 2004, 43, 198–204. [Google Scholar] [CrossRef]
- Scazzina, F.; Dall’Asta, M.; Casiraghi, M.C.; Sieri, S.; Del Rio, D.; Pellegrini, N.; Brighenti, F. Glycemic index and glycemic load of commercial Italian foods. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Rizzello, C.G.; Montemurro, M.; Gobbetti, M. Characterization of the Bread Made with Durum Wheat Semolina Rendered Gluten Free by Sourdough Biotechnology in Comparison with Commercial Gluten-Free Products. J. Food Sci. 2016, 81, H2263–H2272. [Google Scholar] [CrossRef]
- Matos Segura, M.E.; Rosell, C.M. Chemical Composition and Starch Digestibility of Different Gluten-free Breads. Plant Foods Hum. Nutr. 2011, 66, 224–230. [Google Scholar] [CrossRef]
- Calle, J.; Benavent-Gil, Y.; Rosell, C.M. Development of gluten free breads from Colocasia esculenta flour blended with hydrocolloids and enzymes. Food Hydrocoll. 2019, 98, 105243. [Google Scholar] [CrossRef]
- Packer, S.C.; Dornhorst, A.; Frost, G.S. The glycaemic index of a range of gluten-free foods. Diabet. Med. 2000, 17, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Goñi, I.; Garcia-Alonso, A.; Saura-Calixto, F. A starch hydrolysis procedure to estimate glycemic index. Nutr. Res. 1997, 17, 427–437. [Google Scholar] [CrossRef]
- Brennan, C.S.; Tudorica, C.M. Carbohydrate-based fat replacers in the modification of the rheological, textural and sensory quality of yoghurt: Comparative study of the utilisation of barley beta-glucan, guar gum and inulin. Int. J. Food Sci. Technol. 2008, 43, 824–833. [Google Scholar] [CrossRef]
- FAO. Chapter 4—The role of the glycemic index in food choice. Carbohydrates Hum. Nutr. 1998, 1, 1–6. [Google Scholar]
- Wolever, T.M.S.; Nuttall, F.Q.; Lee, R.; Wong, G.S.; Josse, R.G.; Csima, A.; Jenkins, D.J. Prediction of the relative blood glucose response of mixed meals using the white bread glycemic index. Diabetes Care 1985, 8, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Brighenti, F.; Pellegrini, N.; Casiraghi, M.C. In vitro studies to predict physiological effects of dietary fibre. Eur. J. Clin. Nutr. 1995, 1, 81–88. [Google Scholar]
- Brouns, F.; Bjorck, I.; Frayn, K.N.; Gibbs, A.L. Glycaemix Index Methodology. Nutr. Res. Rev. 2005, 1, 145–171. [Google Scholar] [CrossRef] [PubMed]
- Dartois, A.; Singh, J.; Kaur, L. Influence of Guar Gum on the In Vitro Starch Digestibility—Rheological and Microstructural Characteristics. Food Biphysics 2010, 1, 6–14. [Google Scholar] [CrossRef]
- Atkinson, F.S.; Kaye Foser-Powell, K.; Brand- Miller, J.C. International Tables of Glycemic Index and Glycemic Load Values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Venter, C.S.; Slabber, M.; Vorster, H.H. Labelling of foods for glycaemic index—Advantages and problems. Afr. J. Clin. Nutr. 2007, 1, 1–12. [Google Scholar]
- Aziz, A.; Dumais, L.; Barber, J. Health Canada’s evaluation of the use of glycemic index claims on food labels. Am. J. Clin. Nutr. 2013, 98, 269–274. [Google Scholar] [CrossRef]
- Canadian Food Inspection Agency. Carbohydrate Claims on Foods Sold in Canada; Canadian Food Inspection Agency: Morden, MB, Canada, 2016.
- American Diabetes Association, American Diabetes Association Applauds FDA’s Revised Nutrition Label Rules; American Diabetes Association: Arlington, VA, USA, 2016.
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
- ANVISA. Sistema de Rotulagem Nutricional; ANVISA: Brasília, Brazil, 2009.
- European Food Safety Authority. Nutrition Applications: Regulations and Guidance; European Food Safety Authority: Parma, Italy, 2010. [Google Scholar]
- Standards Australia. Australian Standard Glycemic Index of Foods; Standards Australia: Sydney, Australia, 2007. [Google Scholar]
- FDA. Labeling & Nutrition; FDA: White Oak, MD, USA, 2009.
- Capriles, V.; Arêas, J. Approaches to reduce the glycemic response of gluten-free products: In vivo and in vitro studies. Food Funct. 2016, 7, 1266–1272. [Google Scholar] [CrossRef]
- Santos, F.G.; Aguiar, E.V.; Capriles, V.D. Analysis of ingredient and nutritional labeling of commercially available gluten-free bread in Brazil. Int. J. Food Sci. Nutr. 2019, 70, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Pineli, L.d.L.d.O.; Zandonadi, R.P.; Botelho, R.B.A.; de Oliveira, V.R.; Figueiredo, L.F.d.A. The use of sorghum to produce gluten-free breads (GFB): A systematic review. J. Adv. Nutr. Hum. Metab. 2015, 2, e944. [Google Scholar] [CrossRef]
- Argyri, K.; Athanasatou, A.; Bouga, M.; Kapsokefalou, M. The potential of an in vitro digestion method for predicting glycemic response of foods and meals. Nutrients 2016, 8, 209. [Google Scholar] [CrossRef]
- Magaletta, R.L.; DiCataldo, S.N.; Liu, D.; Li, H.L.; Borwankar, R.P.; Martini, M.C. In Vitro Method for Predicting Glycemic Index of Foods Using Simulated Digestion and an Artificial Neural Network. Cereal Chem. 2010, 87, 363–369. [Google Scholar] [CrossRef]
- Capriles, V.D.; Guerra-Matias, A.C.; Arêas, J. Marcador in vitro da resposta glicêmica dos alimentos como ferramenta de auxílio à prescrição e avaliação de dietas [In vitro indicator of the glycemic response to foods as a tool for diet prescriptions and evaluation]. Rev. Nutr. 2009, 22, 549–557. [Google Scholar] [CrossRef]
- Wolever, T.M.S.; Brand-Miller, J.C.; Abernethy, J.; Astrup, A.; Atkinson, F.; Axelsen, M.; Björck, I.; Brighenti, F.; Brown, R.; Brynes, A.; et al. Measuring the glycemic index of foods: Interlaboratory study. Am. J. Clin. Nutr. 2008, 87, 247S–257S. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.; Cummings, J.H.; Englyst, H.N.; Key, T.; Liu, S.; Riccardi, G.; Summerbell, C.; Uauy, R.; van Dam, R.M.; Venn, B.; et al. FAO/WHO Scientific Update on carbohydrates in human nutrition: Conclusions. Eur. J. Clin. Nutr. 2007, 61, S132–S137. [Google Scholar] [CrossRef] [PubMed]
- Gentilcore, D.; Chaikomin, R.; Jones, K.L.; Russo, A.; Feinle-Bisset, C.; Wishart, J.M.; Rayner, C.K.; Horowitz, M. Effects of Fat on Gastric Emptying of and the Glycemic, Insulin, and Incretin Responses to a Carbohydrate Meal in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2006, 91, 2062–2067. [Google Scholar] [CrossRef] [PubMed]
- Cahyana, Y.; Wijaya, E.; Halimah, T.S.; Marta, H.; Suryadi, E.; Kurniati, D. The effect of different thermal modifications on slowly digestible starch and physicochemical properties of green banana flour (Musa acuminata colla). Food Chem. 2019, 274, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Ziobro, R.; Korus, J.; Witczak, M.; Juszczak, L. Influence of modified starches on properties of gluten-free dough and bread. Part II: Quality and staling of gluten-free bread. Food Hydrocoll. 2012, 29, 68–74. [Google Scholar] [CrossRef]
- Alencar, N.M.M.; Steel, C.J.; Alvim, I.D.; de Morais, E.C.; Bolini, H.M.A. Addition of quinoa and amaranth flour in gluten-free breads: Temporal profile and instrumental analysis. LWT Food Sci. Technol. 2015, 62, 1011–1018. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Thorne, M.J.; Wolever, T.M.; Jenkins, A.L.; Rao, A.V.; Thompson, L.U. The effect of starch-protein interaction in wheat on the glycemic response and rate of in vitro digestion. Am. J. Clin. Nutr. 1987, 45, 946–951. [Google Scholar] [CrossRef]
- Gallagher, E.; Gormley, T.R.; Arendt, E.K. Recent advances in the formulation of gluten-free cereal-based products. Trends Food Sci. Technol. 2004, 15, 143–152. [Google Scholar] [CrossRef]
- Cappa, C.; Barbosa-Cánovas, G.V.; Lucisano, M.; Mariotti, M. Effect of high pressure processing on the baking aptitude of corn starch and rice flour. LWT 2016, 73, 20–27. [Google Scholar] [CrossRef]
- Capriles, V.D.; Arêas, J.A.G. Novel Approaches in Gluten-Free Breadmaking: Interface between Food Science, Nutrition, and Health. Compr. Rev. Food Sci. Food Saf. 2014, 13, 871–890. [Google Scholar] [CrossRef]
- Zandonadi, R.P.; Botelho, R.B.A.; Araújo, W.M.C. Psyllium as a Substitute for Gluten in Bread. J. Am. Diet. Assoc. 2009, 109, 1781–1784. [Google Scholar] [CrossRef] [PubMed]
- Aplevicz, K.S.; Demiate, I.M. Caracterização de amidos de mandioca nativos e modificados e utilização em produtos panificados. Ciência e Tecnol. Aliment. 2007, 27, 478–484. [Google Scholar] [CrossRef]
- Moreno, L.A.; Tresaco, B.; Bueno, G.; Fleta, J.; Rodríguez, G.; Garagorri, J.M.; Bueno, M. Psyllium fibre and the metabolic control of obese children and adolescents. J. Physiol. Biochem. 2003, 59, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Verduci, E.; Moretti, F.; Brambilla, M.; Gasparri, C.; Fedeli, S.; Ghisleni, D.; Banderali, G. Daily nutrients intake, glycemic index and glycemic load in Italian children with celiac disease: A case–control study. Dig. Liver Dis. 2016, 48, e274. [Google Scholar] [CrossRef]
- Calvo-Lerma, J.; Crespo-Escobar, P.; Martínez-Barona, S.; Fornés-Ferrer, V.; Donat, E.; Ribes-Koninckx, C. Differences in the macronutrient and dietary fibre profile of gluten-free products as compared to their gluten-containing counterparts. Eur. J. Clin. Nutr. 2019, 73, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Laleg, K.; Cassan, D.; Barron, C.; Prabhasankar, P.; Micard, V. Structural, culinary, nutritional and anti-nutritional properties of high protein, gluten free, 100% legume pasta. PLoS ONE 2016, 11, 1–19. [Google Scholar] [CrossRef]
- Roman, L.; Belorio, M.; Gomez, M. Gluten-Free Breads: The Gap between Research and Commercial Reality. Compr. Rev. Food Sci. Food Saf. 2019, 18, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Sabanis, D.; Lebesi, D.; Tzia, C. Effect of dietary fibre enrichment on selected properties of gluten-free bread. LWT Food Sci. Technol. 2009, 42, 1380–1389. [Google Scholar] [CrossRef]
- Alvarez-Jubete, L.; Auty, M.; Arendt, E.K.; Gallagher, E. Baking properties and microstructure of pseudocereal flours in gluten-free bread formulations. Eur. Food Res. Technol. 2009, 230, 437–445. [Google Scholar] [CrossRef]
- Omar, M.; Shehzad, A.; Shakeel, A.; Shoaib, M.; Sharif, H.R.; Raza, H.; Rakha, A.; Ansari, A.; Niazi, S. Inulin: Properties, health benefits and food applications. Carbohydr. Polym. 2016, 147, 444–454. [Google Scholar] [CrossRef]
- Miremadi, F.; Shah, N.P. Applications of inulin and probiotics in health and nutrition. Int. Food Res. J. 2012, 19, 1337–1350. [Google Scholar] [CrossRef]
- Antonic, B.; Jancikova, S.; Dordevic, D.; Tremlova, B. Apple pomace as food fortification ingredient: A systematic review and meta-analysis. J. Food Sci. 2020, 85, 2977–2985. [Google Scholar] [CrossRef] [PubMed]
- Perera, A.; Meda, V.; Tyler, R.T. Resistant starch: A review of analytical protocols for determining resistant starch and of factors affecting the resistant starch content of foods. Food Res. Int. 2010, 43, 1959–1974. [Google Scholar] [CrossRef]
- Sajilata, M.G.; Singhal, R.S.; Kulkarni, P.R. Resistant Starch? A Review. Compr. Rev. Food Sci. Food Saf. 2006, 5, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Sapone, A.; Bai, J.C.; Ciacci, C.; Dolinsek, J.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M.; et al. Spectrum of gluten-related disorders: Consensus on new nomenclature and classification. BMC Med. 2012, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Farage, P.; Zandonadi, R.P.; Ginani, V.C.; Gandolfi, L.; Nakano, E.Y.; Pratesi, R. Gluten-free diet: From development to assessment of a check-list designed for the prevention of gluten cross-contamination in food services. Nutrients 2018, 10, 1274. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.A. Timing of Initial Exposure to Cereal Grains and the Risk of Wheat Allergy. Pediatrics 2006, 117, 2175–2182. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.Y.; Neal, B.; Trevena, H.; Crino, M.; Stuart-Smith, W.; Faulkner-Hogg, K.; Yu Louie, J.C.; Dunford, E. Are gluten-free foods healthier than non-gluten-free foods? An evaluation of supermarket products in Australia. Br. J. Nutr. 2015, 114, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Brand-miller, J.C.; Stockmann, K.; Atkinson, F.; Petocz, P.; Denyer, G. Glycemic index, postprandial glycemia, and the shape of the curve in healthy subjects: Analysis of a database of more than 1000 foods. Am. J. Clin. Nutr. 2009, 89, 97–105. [Google Scholar] [CrossRef]
- Cappa, C.; Lucisano, M.; Mariotti, M. Influence of Psyllium, sugar beet fibre and water on gluten-free dough properties and bread quality. Carbohydr. Polym. 2013. [Google Scholar] [CrossRef] [PubMed]
- Mancebo, C.M.; San Miguel, M.Á.; Martínez, M.M.; Gómez, M. Optimisation of rheological properties of gluten-free doughs with HPMC, psyllium and different levels of water. J. Cereal Sci. 2015. [Google Scholar] [CrossRef]
- Katina, K.; Arendt, E.; Liukkonen, K.H.; Autio, K.; Flander, L.; Poutanen, K. Potential of sourdough for healthier cereal products. Trends Food Sci. Technol. 2005, 16, 104–112. [Google Scholar] [CrossRef]
- Poutanen, K.; Flander, L.; Katina, K. Sourdough and cereal fermentation in a nutritional perspective. Food Microbiol. 2009, 26, 693–699. [Google Scholar] [CrossRef]
- Carlier, H.; Bernard, A.; Caselli, C. Digestion and absorption of polyunsaturated fatty acids. Reprod. Nutr. Dev. 2007, 31, 475–500. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Panda, P.A.; Lal, M.K.; Ngangkham, U.; Sahu, C.; Soren, K.R.; Subudhi, H.N.; Samantaray, S.; Sharma, S. Addition of Pulses, Cooking Oils, and Vegetables Enhances Resistant Starch and Lowers the Glycemic Index of Rice (Oryza sativa L.). Starch Stärke 2020, 72, 1900081. [Google Scholar] [CrossRef]
- Moravek, D.; Duncan, A.M.; VanderSluis, L.B.; Turkstra, S.J.; Rogers, E.J.; Wilson, J.M.; Hawke, A.; Ramdath, D.D. Carbohydrate replacement of rice or potato with lentils reduces the postprandial glycemic response in healthy adults in an acute, randomized, crossover trial. J. Nutr. 2018, 148, 535–541. [Google Scholar] [CrossRef]
- Dhaheri, A.S.A.; Ma’awali, A.K.A.; Laleye, L.C.; Washi, S.A.; Jarrar, A.H.; Meqbaali, F.T.A.; Mohamad, M.N.; Masuadi, E.M. The effect of nutritional composition on the glycemic index and glycemic load values of selected Emirati foods. BMC Nutr. 2015, 1, 1–8. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef]
- Diamanti, A.; Capriati, T.; Basso, M.S.; Panetta, F.; Laurora, V.M.D.C.; Bellucci, F.; Cristofori, F.; Francavilla, R. Celiac disease and overweight in children: An update. Nutrients 2014, 6, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Dickey, W.; Kearney, N. Overweight in Celiac Disease: Prevalence, Clinical Characteristics, and Effect of a Gluten-Free Diet. Am. J. Gastroenterol. 2006, 101, 2356–2359. [Google Scholar] [CrossRef] [PubMed]
- Rostami, K.; Tucker, E.; Prabhakaran, S.; Al Dulaimi, D. Patients with Coeliac Disease Are Increasingly Overweight or Obese on Presentation. J. Gastrointest. Liver Dis. 2012, 21, 11–15. [Google Scholar]
- Barada, K.; Abu Daya, H.; Rostami, K.; Catassi, C. Celiac Disease in the Developing World. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 773–796. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Jubete, L.; Arendt, E.K.; Gallagher, E. Nutritive value of pseudocereals and their increasing use as functional gluten-free ingredients. Trends Food Sci. Technol. 2010, 21, 106–113. [Google Scholar] [CrossRef]
- Presutti, R.J.; Cangemi, J.R.; Cassidy, H.D.; Hill, D.A. Celiac disease. Am. Fam. Physician 2007, 76, 1795–1802. [Google Scholar] [PubMed]
- Jnawali, P.; Kumar, V.; Tanwar, B. Celiac disease: Overview and considerations for development of gluten-free foods. Food Sci. Hum. Wellness 2016, 5, 169–176. [Google Scholar] [CrossRef]
- Lamacchia, C.; Camarca, A.; Picascia, S.; Di Luccia, A.; Gianfrani, C. Cereal-based gluten-free food: How to reconcile nutritional and technological properties of wheat proteins with safety for celiac disease patients. Nutrients 2014, 6, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T.; Dennis, M.; Higgins, L.A.; Lee, A.R.; Sharrett, M.K. Gluten-free diet survey: Are Americans with coeliac disease consuming recommended amounts of fibre, iron, calcium and grain foods? J. Hum. Nutr. Diet. 2005, 18, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Araújo, H.M.C.; Araújo, W.M.C.; Botelho, R.B.A.; Zandonadi, R.P. Doença celíaca, hábitos e práticas alimentares e qualidade de vida. Rev. Nutr. 2010, 23, 467–474. [Google Scholar] [CrossRef]
- Lee, A.R.; Ng, D.L.; Zivin, J.; Green, P.H.R. Economic burden of a gluten-free diet. J. Hum. Nutr. Diet. 2007, 20, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Robins, G.G.; Burley, V.J.; Howdle, P.D. Evidence of high sugar intake, and low fibre and mineral intake, in the gluten-free diet. Aliment. Pharmacol. Ther. 2010, 32, 573–581. [Google Scholar] [CrossRef]
- Camarca, M.E.; Mozzillo, E.; Nugnes, R.; Zito, E.; Falco, M.; Fattorusso, V.; Mobilia, S.; Buono, P.; Valerio, G.; Troncone, R.; et al. Celiac disease in type 1 diabetes mellitus. Ital. J. Pediatr. 2012, 38, 10. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Regalbuto, C.; Madè, A.; Magistrali, M.; Leonard, M.M.; Cena, H. Coexistence of excessive weight gain and celiac disease in children: An unusual familial condition. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.-Y.; Zhang, Y.-H.; Wang, P.; Qin, L.-Q. Meta-Analysis of Dietary Glycemic Load and Glycemic Index in Relation to Risk of Coronary Heart Disease. Am. J. Cardiol. 2012, 109, 1608–1613. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Reference | Country | Study Outline | GI Determination Method | Type of Flour/Starch Base | Enrichment | In vitro/In Vivo | Number of Samples/Subjects Tested |
|---|---|---|---|---|---|---|---|
| Segura, & Rosell [35] | Spain | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] | Corn starch and flour, potato starch, rice flour | Soy protein, lupin proteins | In vitro | Eleven brands of gluten-free bread from Spain’s market, with duplicates |
| Wolter et al. [24] | Ireland | Exploratory cross-sectional quantitative study | In vitro: Brennan, C.S., amd Tudorica, C.M. (2008). [39] | Buckwheat flour, oat flour, quinoa flour, sorghum flour, teff flour, wheat flour | - | In vitro | Six types of bread, with triplicates |
| Capriles & Arêas [20] | Brazil | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] In vivo: Capillary Blood, FAO/WHO, 1998. [40] | Rice flour, potato starch | Inulin-type fructans | In vitro and In vivo | Five types of bread, with triplicates One male and nine healthy female subjects |
| Giuberti et al. [22] | Italy | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] | Gluten-free flour mix, not specified | Resistant Starch | In vitro | Four types of bread, with triplicates |
| Shumoy et al. [26] | Belgium | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] | White and brown tef flour | Sourdough | In vitro | Four types of bread, with triplicates |
| Wolter et al. [31] | Ireland | Exploratory cross-sectional quantitative study | In vitro: Brennan, C.S., and Tudorica, C.M. (2008). [39] | Buckwheat, flour, quinoa flour, sorghum flour, teff flour, wheat flour | Sourdough | In vitro | Five types of bread, with triplicates |
| Fratelli et al. [21] | Brazil | Exploratory cross-sectional quantitative study | In vivo: Capillary Blood, FAO/WHO, 1998. [40] Wolever, T.M.S., Jenkins, D.J.A., (1986). [41] | Rice flour, cassava starch | Psyllium | In vivo | Thirteen healthy subjects |
| Berti et al. [32] | Italy | Exploratory cross-sectional quantitative study | In vitro: Brighenti F, Pellegrini N, Casiraghi MC, Testolin G (1995) [42] In vivo: Intravenous blood FAO/WHO 1998. [40] | Not specified, brands from the local market | - | In vitro and in vivo | In vitro: two types of conventional bread In vivo: Seven healthy female subjects, six celiac female subjects |
| Feizollahi et al. [30] | Iran | Exploratory cross-sectional quantitative study | In vitro: Brennan, C.S., and Tudorica, C.M. (2008). [39] | Rice flour (four varieties of rice), potato flour, corn starch | - | In vitro | Four types of bread, with triplicates |
| Novotni et al. [23] | Croatia | Exploratory cross-sectional quantitative study | In vivo: Capillary Blood, FAO/WHO, 1998. [40] Brouns, F., Bjorck, I., Frayn, K.N., Gibbs, A.L., Lang, V., Slama, G., Wolever, T.M.S., (2005). [43] | Rice flour, potato flour, cornflour, buckwheat flour, potato, corn starch. | Sourdough | In vivo | Seven female and 4 male healthy subjects |
| Packer et al. [37] | United Kingdom | Exploratory cross-sectional quantitative study | In vivo Intravenous Blood: FAO/WHO, (1998). [40] | Wheat starch | Fiber | In vivo | Eleven diabetic (type 2) subjects |
| Scazzina et al. [33] | Italy | Exploratory cross-sectional quantitative study | In vivo: Capillary Blood FAO/WHO (1998) [40] | Rice flour, corn starch, potato starch, millet flour, rice starch | Soy protein, apple fiber, lupin protein, Sourdough | In vivo | Ten male and ten female healthy subjects |
| Sciarini et al. [25] | Argentina | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] | Rice flour, cassava starch, soy flour | Resistant starch RS3, oat fiber and inulin | In vitro | Three types of bread, with triplicates |
| Rizzello et al. [34] | Italy | Exploratory cross-sectional quantitative study | In vitro: Brennan, C.S., and Tudorica, C.M. (2008). [39] | Wheat starch without gluten; millet flour | Wheat sourdough without gluten 50% (water, durum wheat flour, lactic acid bacteria); | In vitro | One gluten-free bread. |
| Liu et al. [29] | China | Exploratory cross-sectional quantitative study | In vitro: Dartois, A, Singh J., Kaur L. Singh H. (2010). [44] | Fresh potato flour | Hydroxypropyl-MethylCelullose, CarboxymethylCellulose, Xanthan Gum, Apple Purée | In vitro | Twelve types of bread. |
| Calle et al. [36] | Spain | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] | Colocasia esculenta flour | HPMC, Xanthan Gum, Guar Gum, Gluzyme Mono 10.000 BG, iZyme BA | In vitro | Five Types of Bread |
| Romão et al. [27] | Brazil | Exploratory cross-sectional quantitative study | In vivo: Capillary Blood, FAO/WHO, 1998. [40] Brouns, F., Bjorck, I., Frayn, K.N., Gibbs, A.L., Lang, V., Slama, G., Wolever, T.M.S., (2005). [43] | Cassava and potato starches and rice flour | HPMC, Xanthan Gum, Guar Gum, Psyllium, Soy Protein, Lupin Protein, Apple Fiber | In Vivo | Twelve Types of Bread |
| Graça et al. [28] | Portugal | Exploratory cross-sectional quantitative study | In vitro: Goñi I, Garcia-Alonso A, Saura-Calixto F (1997) [38] | Buckwheat, potato starch, and rice flour | Yogurt and Cheese Curd | In vitro | Four Types of Bread |
| Study | Starch Sources | Stabilizing Agent/Enrichment Ingredient | GI | GI Classification [45] |
|---|---|---|---|---|
| Giuberti et al. [22] | Not Specified | None | 97 | High |
| RS 20% | 88 | High | ||
| RS3a 20% | 78 | High | ||
| RS3b 20% | 70 | High | ||
| Berti et al. [32] | Not Specified | Not Specified | 230 | High |
| Scazzina et al. [33] | Rice flour, corn starch, potato starch, millet flour, rice starch | Sourdough | 52 | Low |
| Soy Protein | 62 | Medium | ||
| Apple Fiber | 63 | Medium | ||
| Capriles and Arêas [20] | Rice flour, potato starch | None | 93 | High |
| 4% ITF | 89 | High | ||
| 8% ITF | 86 | High | ||
| 10% ITF | 84 | High | ||
| 12% ITF | 84 | High | ||
| Fratelli et al. [21] | Rice flour, cassava starch | None | 67 | Medium |
| Psyllium | 50 | Low | ||
| Wolter et al. [24] | Buckwheat Flour | None | 80 | High |
| Oat Flour | 71 | High | ||
| Quinoa Flour | 85 | High | ||
| Sorghum Flour | 72 | High | ||
| Teff Flour | 74 | High | ||
| Wolter et al. [31] | Buckwheat Flour | Control | 80 | High |
| WC | 89 | High | ||
| LP | 86 | High | ||
| Quinoa Flour | Control | 95 | High | |
| WC | 106 | High | ||
| LP | 103 | High | ||
| Sorghum Flour | Control | 72 | High | |
| WC | 81 | High | ||
| LP | 69 | Medium | ||
| Teff Flour | Control | 74 | High | |
| WC | 84 | High | ||
| LP | 78 | High | ||
| Segura et al. [35] | Corn Starch | Xanthan Gum | 87 | High |
| Xanthan Gum, guar gum, pectin, CMC | 90 | High | ||
| Guar gum, pectin, CMC | 83 | High | ||
| Potato starch, corn starch | Casein, soy protein, HPMC, xanthan gum | 87 | High | |
| Corn Starch, rice flour | Guar gum, HPMC, lupine protein, vegetal fiber | 91 | High | |
| Corn Starch | Xantham Gum | 91 | High | |
| Xantham Gum, HPMC | 91 | High | ||
| Xantham Gum | 89 | High | ||
| Xantham Gum | 96 | High | ||
| Xantham Gum | 89 | High | ||
| Xantham Gum | 88 | High | ||
| Shumoy et al. [26] | White Teff Flour | Sourdough | ||
| Fresh: 0%, 10%, 20%, 30% | 72, 82, 77, 86 | High | ||
| 1 day: 0%, 10%, 20%, 30% | 58, 67, 62, 54 | Low, Medium, Medium, Low | ||
| 2 days: 0%, 10%, 20%, 30% | 51, 55, 62, 60 | Low, Low, Medium, Medium | ||
| 5 days: 0%, 10%, 20%, 30% | 39, 50, 45, 52 | Low, Low, Low, Low | ||
| Brown Teff Flour | Fresh: 0%, 10%, 20%, 30% | 75, 83, 85, 89 | High, High, High, High | |
| 1 day: 0%, 10%, 20%, 30% | 72, 70, 74, 74 | High, High, High, High | ||
| 2 days: 0%, 10%, 20%, 30% | 66, 69, 74, 74 | Medium, Medium, High, High | ||
| 5 days: 0%, 10%, 20%, 30% | 66, 69, 74, 73 | Medium, Medium, High, High | ||
| Feizollahi et al. [30] | Tarom rice flour | Non specified stabilizers | 81 | High |
| Hashemi rice flour | 89 | High | ||
| Khouzestan rice flour | 66 | Medium | ||
| Lenian rice flour | 64 | Medium | ||
| Novotni et al. [23] | Rice flour, potato flour, cornflour, buckwheat flour, potato purée, corn starch | 7.5 g Sourdough | 59 | Low |
| 15 g sourdough | 52 | Low | ||
| 22.5 g sourdough | 54 | Low | ||
| 30 g sourdough | 61 | Medium | ||
| Packer and Frost [37] | GF wheat starch commercial unsliced white bread | None | 101 | High |
| GF wheat starch commercial sliced white bread | 114 | High | ||
| GF wheat starch commercial sliced fiber-enriched bread | Unspecified fiber | 99 | High | |
| GF wheat starch commercial fiber-enriched white bread | 109 | High | ||
| Sciarini et al. [25] | Rice flour, cassava starch, soy flour | None | 84 | High |
| 5% Oat fiber | 93 | High | ||
| 10% Oat fiber | 71 | High | ||
| 5% Inulin | 91 | High | ||
| 10% Inulin | 81 | High | ||
| 5% Resistant Starch | 81 | High | ||
| 10% Resistant Starch | 70 | High | ||
| Rizzello et al. [34]. | Wheat starch without gluten; millet flour | Wheat sourdough without gluten 50% (water, durum wheat flour, lactic acid bacteria); | 74 | High |
| Liu et al. [29] | Fresh potato flour | 0.5% HPMC | 65.02 | Medium |
| 1% HPMC | 60.52 | Medium | ||
| 2% HPMC | 58.89 | Medium | ||
| 0.5% CMC | 66.25 | Medium | ||
| 1% CMC | 68.38 | Medium | ||
| 2% CMC | 66.57 | Medium | ||
| 0.5% XG | 62.71 | Medium | ||
| 1% XG | 62.70 | Medium | ||
| 2.0% XG | 63.28 | Medium | ||
| 0.5% AP | 65.09 | Medium | ||
| 1.5% AP | 64.83 | Medium | ||
| 2.0% AP | 65.12 | Medium | ||
| Calle et al. [36] | Colocasia esculenta flour | HPMC | 24.58 | Low |
| Xanthan Gum | 23.90 | Low | ||
| Guar Gum | 23.15 | Low | ||
| Gluzyme Mono 10.000 BG | 26.20 | Low | ||
| iZyme BA | 26.32 | Low | ||
| Alcalase 1.5 MG Type FG | 23.10 | Low | ||
| Potato Starch | 32.81 | Low | ||
| Romão et al. [27] | Cassava and potato starches and rice flour (Local Market samples) | GFB 1 | 67.97 | Medium |
| GFB 2 | 64.00 | Medium | ||
| GFB 3 | 70.14 | High | ||
| GFB 4 | 78.72 | High | ||
| GFB 5 | 77.69 | High | ||
| GFB 6 | 79.94 | High | ||
| GFB 7 | 76.53 | High | ||
| GFB 8 | 75.39 | High | ||
| WGFB 1 | 67.66 | Medium | ||
| WGFB 2 | 61.46 | Medium | ||
| WGFB 3 | 69.23 | Medium | ||
| WGFB 4 | 75.40 | High | ||
| Graça et al. [28] | Gluten-free flour mix: Buckwheat, potato starch, and rice flour | YgB 10% | 82.80 | High |
| YgB 20% | 76.50 | High | ||
| CcB 10% | 68.00 | Medium | ||
| CcB 20% | 62.70 | Medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romão, B.; Falcomer, A.L.; Palos, G.; Cavalcante, S.; Botelho, R.B.A.; Nakano, E.Y.; Raposo, A.; Shakeel, F.; Alshehri, S.; Mahdi, W.A.; et al. Glycemic Index of Gluten-Free Bread and Their Main Ingredients: A Systematic Review and Meta-Analysis. Foods 2021, 10, 506. https://doi.org/10.3390/foods10030506
Romão B, Falcomer AL, Palos G, Cavalcante S, Botelho RBA, Nakano EY, Raposo A, Shakeel F, Alshehri S, Mahdi WA, et al. Glycemic Index of Gluten-Free Bread and Their Main Ingredients: A Systematic Review and Meta-Analysis. Foods. 2021; 10(3):506. https://doi.org/10.3390/foods10030506
Chicago/Turabian StyleRomão, Bernardo, Ana Luísa Falcomer, Gabriela Palos, Sandra Cavalcante, Raquel Braz Assunção Botelho, Eduardo Yoshio Nakano, António Raposo, Faiyaz Shakeel, Sultan Alshehri, Wael A. Mahdi, and et al. 2021. "Glycemic Index of Gluten-Free Bread and Their Main Ingredients: A Systematic Review and Meta-Analysis" Foods 10, no. 3: 506. https://doi.org/10.3390/foods10030506
APA StyleRomão, B., Falcomer, A. L., Palos, G., Cavalcante, S., Botelho, R. B. A., Nakano, E. Y., Raposo, A., Shakeel, F., Alshehri, S., Mahdi, W. A., & Zandonadi, R. P. (2021). Glycemic Index of Gluten-Free Bread and Their Main Ingredients: A Systematic Review and Meta-Analysis. Foods, 10(3), 506. https://doi.org/10.3390/foods10030506