
Effects of β-Cryptoxanthin on Improvement in Osteoporosis Risk: A Systematic Review and Meta-Analysis of Observational Studies

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search and Selection Criteria
2.2. Data Extraction
2.3. Data Synthesis
2.4. Sensitivity Analysis
2.5. Quality Assessment
3. Results
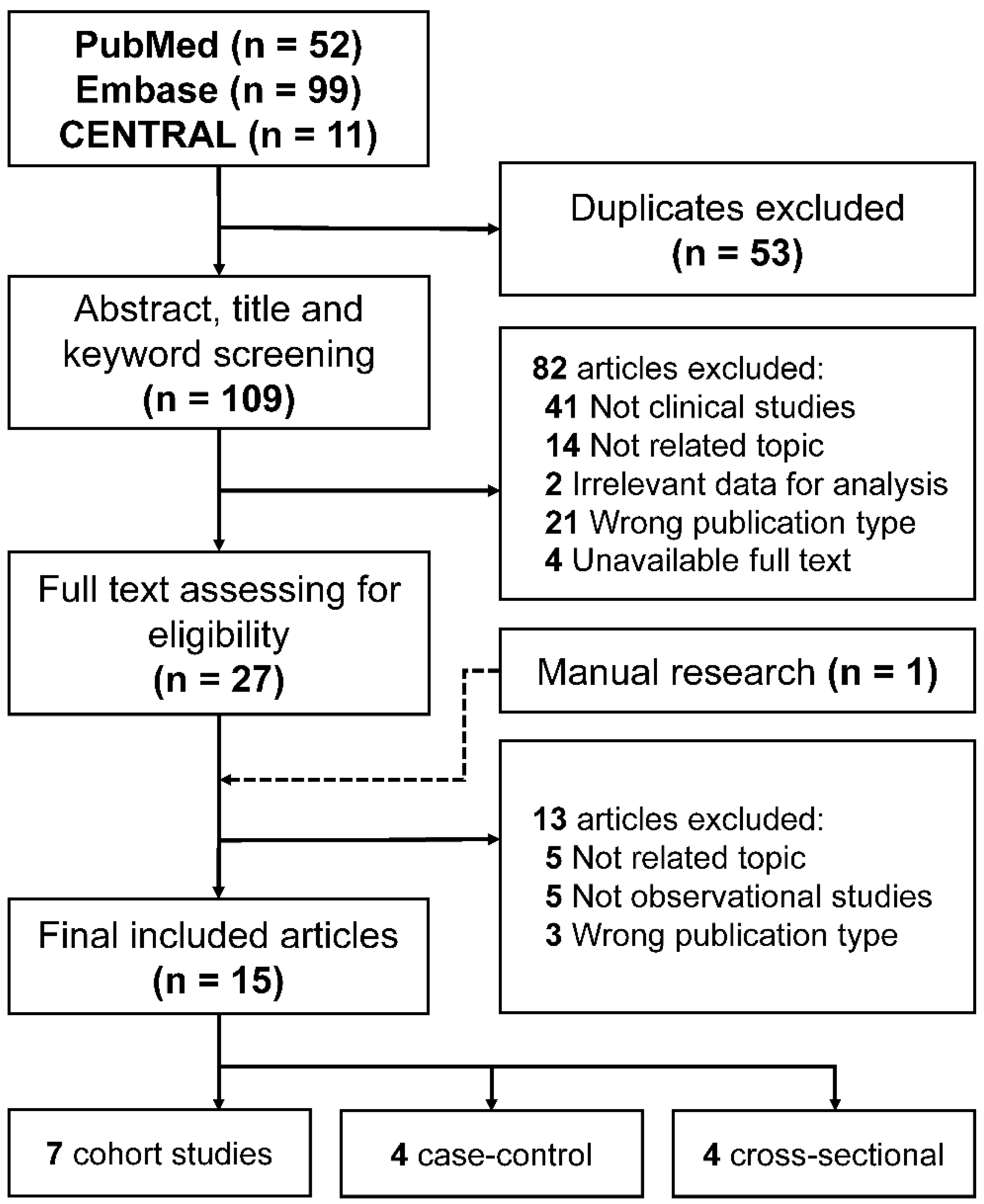
3.1. Literature Selection
3.2. Methodological Quality
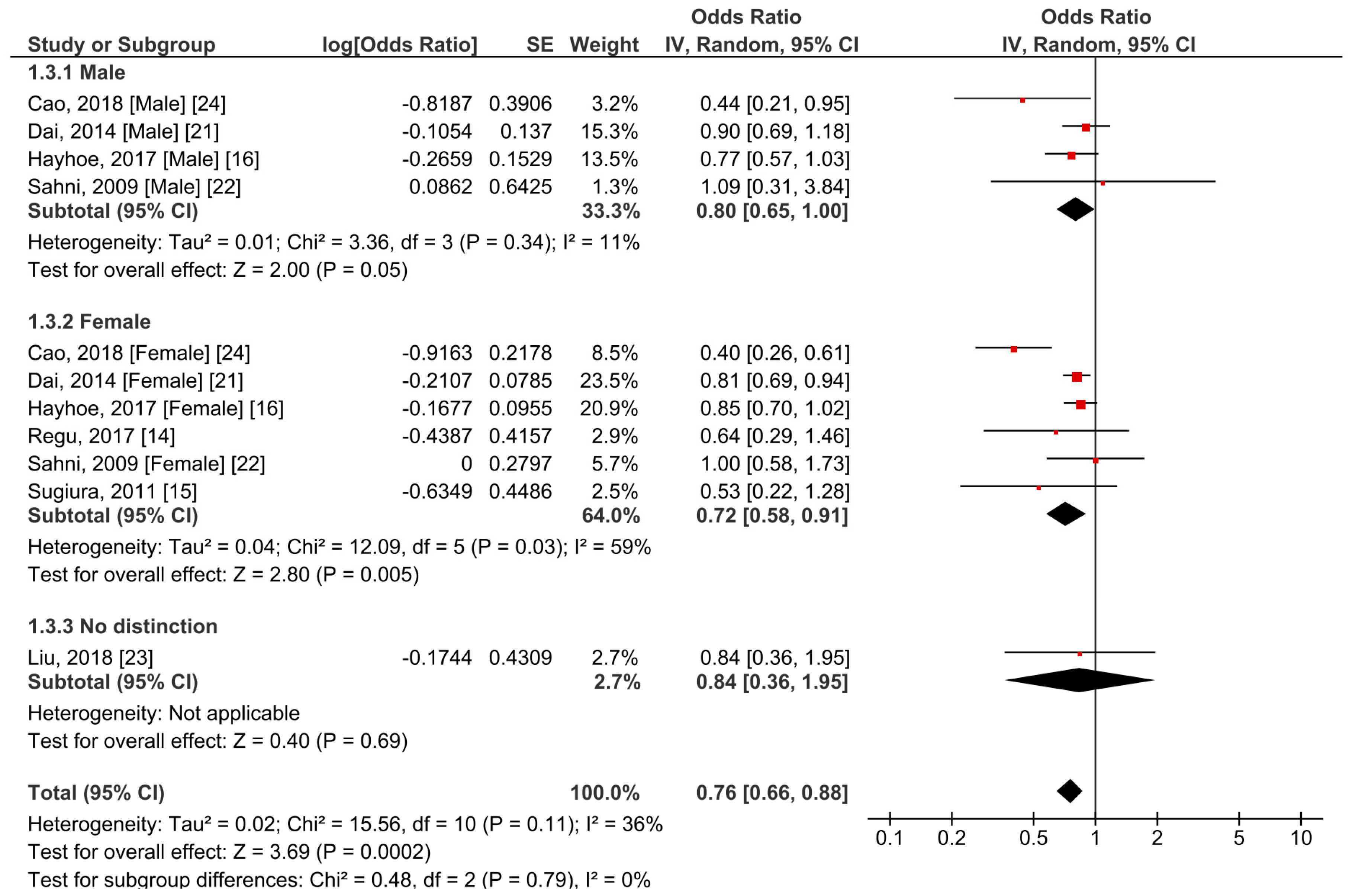
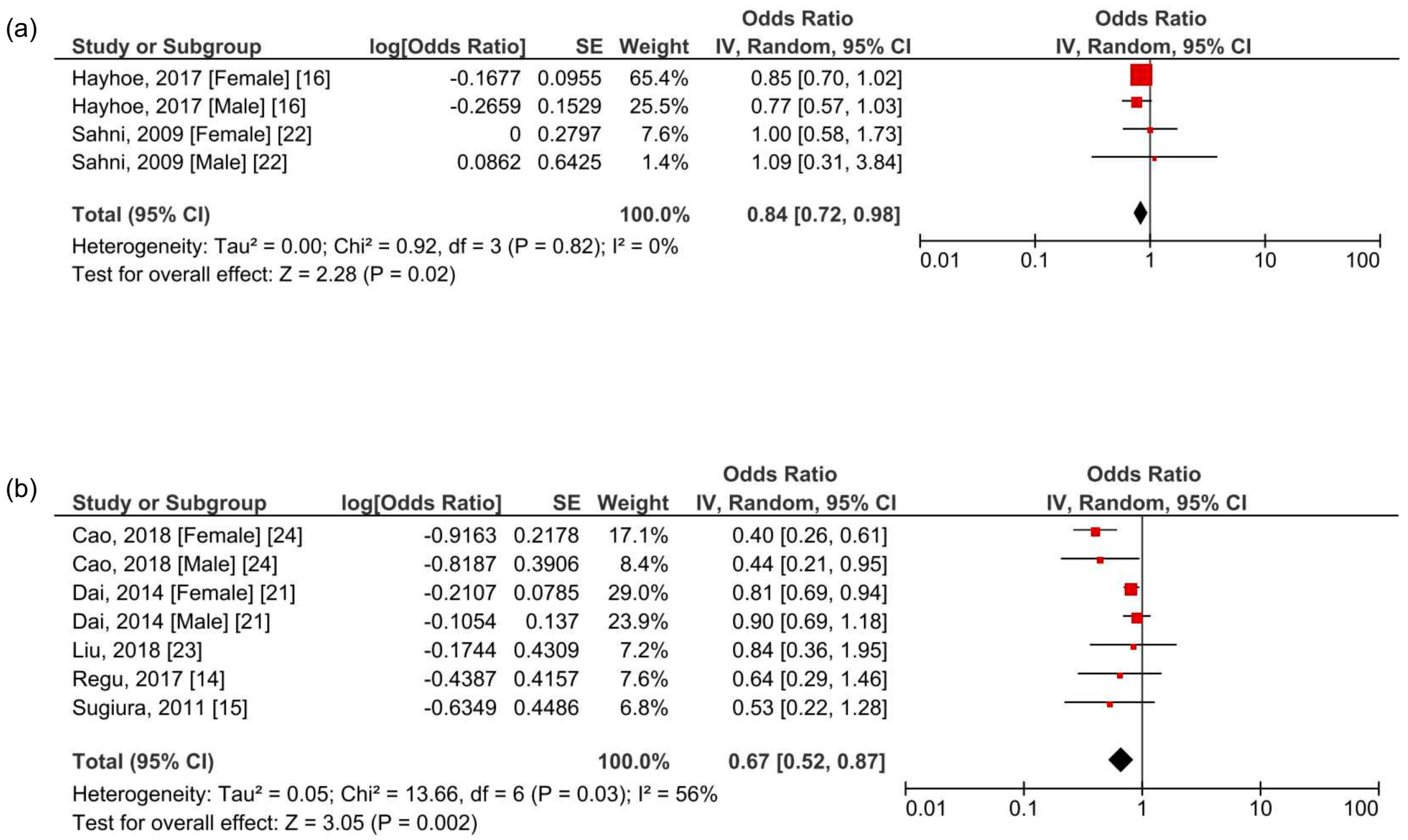
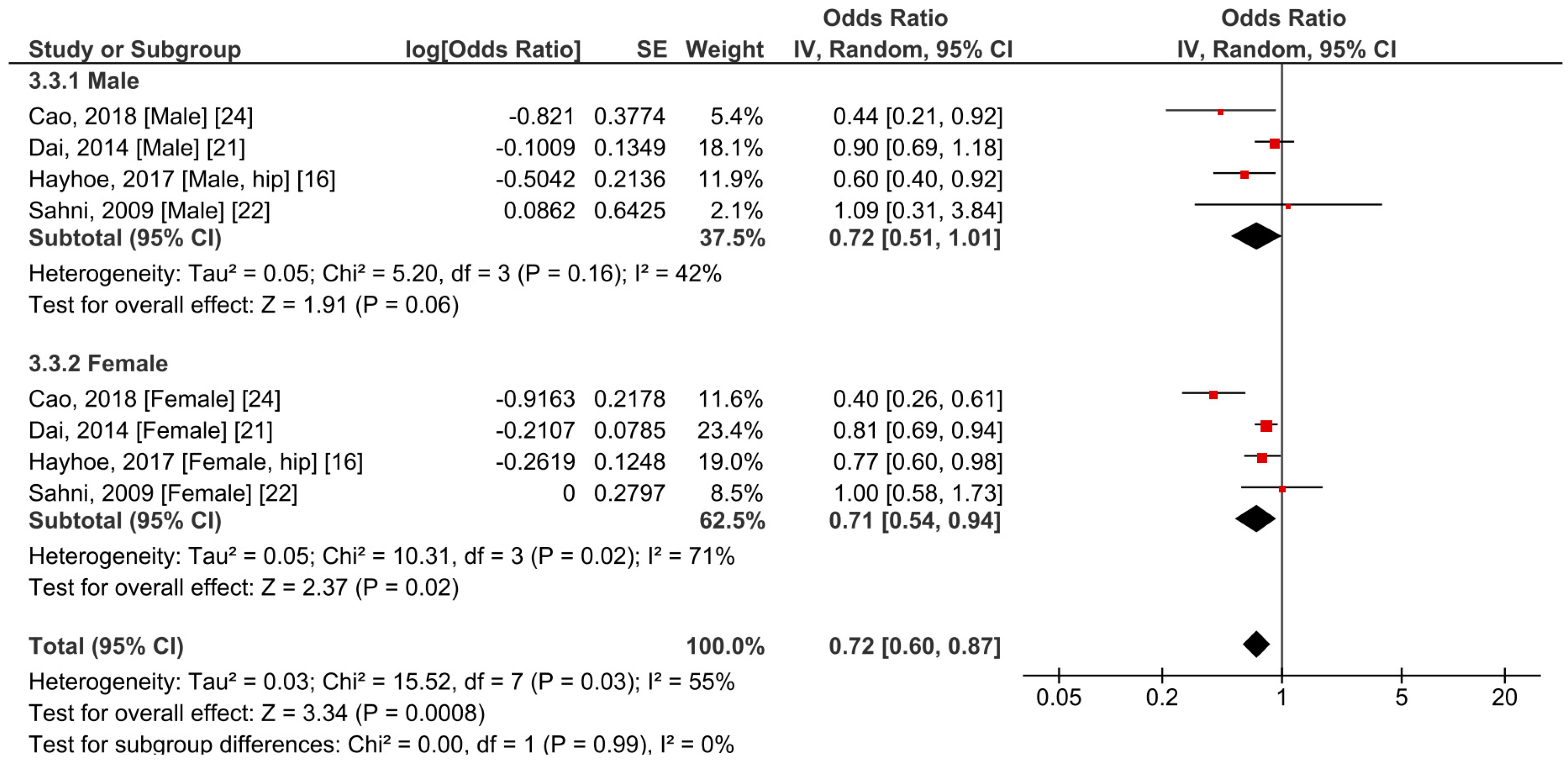
3.3. Meta-Analysis of the Effects of β-Cryptoxanthin on Osteoporosis
3.4. Sensitivity Analysis
3.5. Other Observational Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. The Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Barrett-Connor, E.; Sajjan, S.G.; Siris, E.S.; Miller, P.D.; Chen, Y.T.; Markson, L.E. Wrist fracture as a predictor of future fractures in younger versus older postmenopausal women: Results from the National Osteoporosis Risk Assessment (NORA). Osteoporos. Int. 2008, 19, 607–613. [Google Scholar] [CrossRef]
- Munoz-Garach, A.; Garcia-Fontana, B.; Munoz-Torres, M. Nutrients and Dietary Patterns Related to Osteoporosis. Nutrients 2020, 12, 1986. [Google Scholar] [CrossRef]
- Higgs, J.; Derbyshire, E.; Styles, K. Nutrition and osteoporosis prevention for the orthopaedic surgeon: A wholefoods approach. EFORT Open Rev. 2017, 2, 300–308. [Google Scholar] [CrossRef]
- Stránský, M.; Rysavá, L. Nutrition as prevention and treatment of osteoporosis. Physiol. Res. 2009, 58 (Suppl. S1), S7–S11. [Google Scholar]
- Burri, B.J.; La Frano, M.R.; Zhu, C. Absorption, metabolism, and functions of β-cryptoxanthin. Nutr. Rev. 2016, 74, 69–82. [Google Scholar] [CrossRef]
- Lim, J.Y.; Wang, X.-D. Mechanistic understanding of β-cryptoxanthin and lycopene in cancer prevention in animal models. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2020, 1865, 158652. [Google Scholar] [CrossRef]
- Diep, T.T.; Pook, C.; Rush, E.C.; Yoo, M.J. Quantification of Carotenoids, α-Tocopherol, and Ascorbic Acid in Amber, Mulligan, and Laird’s Large Cultivars of New Zealand Tamarillos (Solanum betaceum Cav.). Foods 2020, 9, 769. [Google Scholar] [CrossRef]
- Lorenzo, J.M.; Munekata, P.E. Dietary Carotenoids for Reduction of Cancer Risk. In Studies in Natural Products Chemistry; Atta-ur, R., Ed.; Elsevier: Amsterdam, The Netherlands, 2016; Chapter 6; Volume 51, pp. 223–251. [Google Scholar]
- Van Hoang, D.; Pham, N.M.; Lee, A.H.; Tran, D.N.; Binns, C.W. Dietary Carotenoid Intakes and Prostate Cancer Risk: A Case-Control Study from Vietnam. Nutrients 2018, 10, 70. [Google Scholar] [CrossRef]
- Cohen, K.; Liu, Y.; Luo, J.; Appleton, C.M.; Colditz, G.A. Plasma carotenoids and the risk of premalignant breast disease in women aged 50 and younger: A nested case–control study. Breast Cancer Res. Treat. 2017, 162, 571–580. [Google Scholar] [CrossRef]
- Jayedi, A.; Rashidy-Pour, A.; Parohan, M.; Zargar, M.S.; Shab-Bidar, S. Dietary Antioxidants, Circulating Antioxidant Concentrations, Total Antioxidant Capacity, and Risk of All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Observational Studies. Adv. Nutr. 2018, 9, 701–716. [Google Scholar] [CrossRef]
- Yamaguchi, M. Role of carotenoid β-cryptoxanthin in bone homeostasis. J. Biomed. Sci. 2012, 19, 36. [Google Scholar] [CrossRef]
- Regu, G.M.; Kim, H.; Kim, Y.J.; Paek, J.E.; Lee, G.; Chang, N.; Kwon, O. Association between Dietary Carotenoid Intake and Bone Mineral Density in Korean Adults Aged 30–75 Years Using Data from the Fourth and Fifth Korean National Health and Nutrition Examination Surveys (2008–2011). Nutrients 2017, 9, 1025. [Google Scholar] [CrossRef]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Ando, F.; Shimokata, H.; Yano, M. Dietary patterns of antioxidant vitamin and carotenoid intake associated with bone mineral density: Findings from post-menopausal Japanese female subjects. Osteoporos. Int. 2011, 22, 143–152. [Google Scholar] [CrossRef]
- Hayhoe, R.P.G.; Lentjes, M.A.H.; Mulligan, A.A.; Luben, R.N.; Khaw, K.T.; Welch, A.A. Carotenoid dietary intakes and plasma concentrations are associated with heel bone ultrasound attenuation and osteoporotic fracture risk in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk cohort. Br. J. Nutr. 2017, 117, 1439–1453. [Google Scholar] [CrossRef]
- Neville, C.E.; Young, I.S.; Gilchrist, S.E.; McKinley, M.C.; Gibson, A.; Edgar, J.D.; Woodside, J.V. Effect of increased fruit and vegetable consumption on bone turnover in older adults: A randomised controlled trial. Osteoporos. Int. 2014, 25, 223–233. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Igarashi, A.; Uchiyama, S.; Sugawara, K.; Sumida, T.; Morita, S.; Ogawa, H.; Nishitani, M.; Kajimoto, Y. Effect of beta-Crytoxanthin on Circulating Bone Metabolic Markers: Intake of Juice (Citrus Unshiu) Supplemented witt beta-Cryptoxanthin Has an Effect in Menopausal Women. J. Health Sci. 2006, 52, 758–768. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Xu, J.; Song, C.; Song, X.; Zhang, X.; Li, X. Carotenoids and risk of fracture: A meta-analysis of observational studies. Oncotarget 2017, 8, 2391–2399. [Google Scholar] [CrossRef]
- Dai, Z.; Wang, R.; Ang, L.W.; Low, Y.L.; Yuan, J.M.; Koh, W.P. Protective effects of dietary carotenoids on risk of hip fracture in men: The Singapore Chinese Health Study. J. Bone Miner. Res. 2014, 29, 408–417. [Google Scholar] [CrossRef]
- Sahni, S.; Hannan, M.T.; Blumberg, J.; Cupples, L.A.; Kiel, D.P.; Tucker, K.L. Protective effect of total carotenoid and lycopene intake on the risk of hip fracture: A 17-year follow-up from the Framingham Osteoporosis Study. J. Bone Miner. Res. 2009, 24, 1086–1094. [Google Scholar] [CrossRef]
- Liu, J.; Yang, S.; Luo, M.J.; Zhao, X.; Zhang, Y.M.; Luo, Y. Association of Dietary Carotenoids Intake with Skeletal Fluorosis in the Coal-burning Fluorosis Area of Guizhou Province. Biomed. Environ. Sci. 2018, 31, 438–447. [Google Scholar] [CrossRef]
- Cao, W.T.; Zeng, F.F.; Li, B.L.; Lin, J.S.; Liang, Y.Y.; Chen, Y.M. Higher dietary carotenoid intake associated with lower risk of hip fracture in middle-aged and elderly Chinese: A matched case-control study. Bone 2018, 111, 116–122. [Google Scholar] [CrossRef]
- Zhang, Z.Q.; Cao, W.T.; Liu, J.; Cao, Y.; Su, Y.X.; Chen, Y.M. Greater serum carotenoid concentration associated with higher bone mineral density in Chinese adults. Osteoporos. Int. 2016, 27, 1593–1601. [Google Scholar] [CrossRef]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Yano, M. High Vitamin C Intake with High Serum β-Cryptoxanthin Associated with Lower Risk for Osteoporosis in Post-Menopausal Japanese Female Subjects: Mikkabi Cohort Study. J. Nutr. Sci. Vitaminol. 2016, 62, 185–191. [Google Scholar] [CrossRef]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Yano, M. High serum carotenoids associated with lower risk for bone loss and osteoporosis in post-menopausal Japanese female subjects: Prospective cohort study. PLoS ONE 2012, 7, e52643. [Google Scholar] [CrossRef]
- Imagama, S.; Hasegawa, Y.; Seki, T.; Matsuyama, Y.; Sakai, Y.; Ito, Z.; Ishiguro, N.; Ito, Y.; Hamajima, N.; Suzuki, K. The effect of β-carotene on lumbar osteophyte formation. Spine 2011, 36, 2293–2298. [Google Scholar] [CrossRef]
- Sahni, S.; Hannan, M.T.; Blumberg, J.; Cupples, L.A.; Kiel, D.P.; Tucker, K.L. Inverse association of carotenoid intakes with 4-y change in bone mineral density in elderly men and women: The Framingham Osteoporosis Study. Am. J. Clin. Nutr. 2009, 89, 416–424. [Google Scholar] [CrossRef]
- Sugiura, M.; Nakamura, M.; Ogawa, K.; Ikoma, Y.; Ando, F.; Yano, M. Bone mineral density in post-menopausal female subjects is associated with serum antioxidant carotenoids. Osteoporos. Int. 2008, 19, 211–219. [Google Scholar] [CrossRef]
- Yang, Z.; Zhang, Z.; Penniston, K.L.; Binkley, N.; Tanumihardjo, S.A. Serum carotenoid concentrations in postmenopausal women from the United States with and without osteoporosis. Int. J. Vitam. Nutr. Res. 2008, 78, 105–111. [Google Scholar] [CrossRef]
- Maggio, D.; Polidori, M.C.; Barabani, M.; Tufi, A.; Ruggiero, C.; Cecchetti, R.; Aisa, M.C.; Stahl, W.; Cherubini, A. Low levels of carotenoids and retinol in involutional osteoporosis. Bone 2006, 38, 244–248. [Google Scholar] [CrossRef]
- Tucker, K.L. Osteoporosis prevention and nutrition. Curr. Osteoporos. Rep. 2009, 7, 111–117. [Google Scholar] [CrossRef]
- Malmir, H.; Shab-Bidar, S.; Djafarian, K. Vitamin C intake in relation to bone mineral density and risk of hip fracture and osteoporosis: A systematic review and meta-analysis of observational studies. Br. J. Nutr. 2018, 119, 847–858. [Google Scholar] [CrossRef]
- Tucker, K.L. Vegetarian diets and bone status. Am. J. Clin. Nutr. 2014, 100 (Suppl. S1), 329S–335S. [Google Scholar] [CrossRef]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary Patterns in Relation to Low Bone Mineral Density and Fracture Risk: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 219–236. [Google Scholar] [CrossRef]
- Denova-Gutierrez, E.; Mendez-Sanchez, L.; Munoz-Aguirre, P.; Tucker, K.L.; Clark, P. Dietary Patterns, Bone Mineral Density, and Risk of Fractures: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1922. [Google Scholar] [CrossRef]
- Lim, D.W.; Lee, Y.; Kim, Y.T. Preventive effects of Citrus unshiu peel extracts on bone and lipid metabolism in OVX rats. Molecules 2014, 19, 783–794. [Google Scholar] [CrossRef]
- Shen, C.L.; von Bergen, V.; Chyu, M.C.; Jenkins, M.R.; Mo, H.; Chen, C.H.; Kwun, I.S. Fruits and dietary phytochemicals in bone protection. Nutr. Res. 2012, 32, 897–910. [Google Scholar] [CrossRef]
- Ozaki, K.; Okamoto, M.; Fukasawa, K.; Iezaki, T.; Onishi, Y.; Yoneda, Y.; Sugiura, M.; Hinoi, E. Daily intake of β-cryptoxanthin prevents bone loss by preferential disturbance of osteoclastic activation in ovariectomized mice. J. Pharmacol. Sci. 2015, 129, 72–77. [Google Scholar] [CrossRef]
- Uchiyama, S.; Yamaguchi, M. beta-Cryptoxanthin stimulates cell proliferation and transcriptional activity in osteoblastic MC3T3-E1 cells. Int. J. Mol. Med. 2005, 15, 675–681. [Google Scholar]
- Uchiyama, S.; Yamaguchi, M. β-cryptoxanthin stimulates cell differentiation and mineralization in osteoblastic MC3T3-E1 cells. J. Cell. Biochem. 2005, 95, 1224–1234. [Google Scholar] [CrossRef]
- Weng, Z.; Wang, C.; Zhang, C.; Xu, J.; Chai, Y.; Jia, Y.; Han, P.; Wen, G. All-Trans Retinoic Acid Promotes Osteogenic Differentiation and Bone Consolidation in a Rat Distraction Osteogenesis Model. Calcif. Tissue Int. 2019, 104, 320–330. [Google Scholar] [CrossRef]
- Sahin, K.; Orhan, C.; Akdemir, F.; Tuzcu, M.; Sahin, N.; Yılmaz, I.; Juturu, V. β-Cryptoxanthin ameliorates metabolic risk factors by regulating NF-κB and Nrf2 pathways in insulin resistance induced by high-fat diet in rodents. Food Chem. Toxicol. 2017, 107, 270–279. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Weitzmann, M.N. The bone anabolic carotenoids p-hydroxycinnamic acid and β-cryptoxanthin antagonize NF-κB activation in MC3T3 preosteoblasts. Mol. Med. Rep. 2009, 2, 641–644. [Google Scholar] [CrossRef]
- Novack, D.V. Role of NF-kappaB in the skeleton. Cell Res. 2011, 21, 169–182. [Google Scholar] [CrossRef]
- Hirata, N.; Ichimaru, R.; Tominari, T.; Matsumoto, C.; Watanabe, K.; Taniguchi, K.; Hirata, M.; Ma, S.; Suzuki, K.; Grundler, F.M.W.; et al. Beta-Cryptoxanthin Inhibits Lipopolysaccharide-Induced Osteoclast Differentiation and Bone Resorption via the Suppression of Inhibitor of NF-κB Kinase Activity. Nutrients 2019, 11, 368. [Google Scholar] [CrossRef]
- Granado-Lorencio, F.; Lagarda, M.J.; Garcia-López, F.J.; Sánchez-Siles, L.M.; Blanco-Navarro, I.; Alegría, A.; Pérez-Sacristán, B.; Garcia-Llatas, G.; Donoso-Navarro, E.; Silvestre-Mardomingo, R.A.; et al. Effect of β-cryptoxanthin plus phytosterols on cardiovascular risk and bone turnover markers in post-menopausal women: A randomized crossover trial. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1090–1096. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Igarashi, A.; Uchiyama, S.; Morita, S.; Sugawara, K.; Sumida, T. Prolonged Intake of Juice (Citrus Unshiu) Reinforced with beta-Crypthoxanthin Has an Effect on Circulating Bone Biochemical Markers in Normal Individuals. J. Health Sci. 2004, 50, 619–624. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Igarashi, A.; Morita, S.; Sumida, T.; Sugawara, K. Relationship between Serum beta-Cryptoxanthin and Circulating Bone Metabolic Markers in Healthy Individuals with the Intake of Juice (Citrus unshiu) Containing beta-Cryptoxanthin. J. Health Sci. 2005, 51, 738–743. [Google Scholar] [CrossRef]
- Hu, D.; Cheng, L.; Jiang, W. Fruit and vegetable consumption and the risk of postmenopausal osteoporosis: A meta-analysis of observational studies. Food Funct. 2018, 9, 2607–2616. [Google Scholar] [CrossRef]
- Redmond, J.; Jarjou, L.M.; Zhou, B.; Prentice, A.; Schoenmakers, I. Ethnic differences in calcium, phosphate and bone metabolism. Proc. Nutr. Soc. 2014, 73, 340–351. [Google Scholar] [CrossRef]
- Guerado, E.; Sandalio, R.M.; Caracuel, Z.; Caso, E. Understanding the pathogenesis of hip fracture in the elderly, osteoporotic theory is not reflected in the outcome of prevention programmes. World J. Orthop. 2016, 7, 218–228. [Google Scholar] [CrossRef]
- Barrett-Connor, E.; Siris, E.S.; Wehren, L.E.; Miller, P.D.; Abbott, T.A.; Berger, M.L.; Santora, A.C.; Sherwood, L.M. Osteoporosis and fracture risk in women of different ethnic groups. J. Bone Miner. Res. 2005, 20, 185–194. [Google Scholar] [CrossRef]
- Finkelstein, J.S.; Lee, M.L.; Sowers, M.; Ettinger, B.; Neer, R.M.; Kelsey, J.L.; Cauley, J.A.; Huang, M.H.; Greendale, G.A. Ethnic variation in bone density in premenopausal and early perimenopausal women: Effects of anthropometric and lifestyle factors. J. Clin. Endocrinol. Metab. 2002, 87, 3057–3067. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Location | Included to Meta-Analysis | Study Design | Total Population (Age as a Range or Mean ± SD) | Sex | BCX Exposure | Outcome Variables | Bias Variables Adjustment | Summary | Quality Rating † (Risk of Bias) |
|---|---|---|---|---|---|---|---|---|---|
| Regu, 2017, South Korea [14] | Yes | Cross-sectional | 8022 (age 30–74) | Male, pre-/postmenopausal female | Quintile of BCX intake (postmenopausal female): Q1 (0.0003–0.01 mg/day) Q2 (0.01–0.04 mg/day) Q3 (0.04–0.10 mg/day) Q4 (0.10–0.59 mg/day) Q5 (0.60–18.53 mg/day) | Coefficient of BCX intake with the BMDs of femur neck, total hip, lumber spine, and whole body; odds ratios for femur neck, total hip, lumber spine, and total osteopenia. | Yes | On pre-menopausal women, BCX consumption was positively correlated with femur neck BMD and total hip BMD. BCX consumption was also positively correlated with total hip BMD. | Fair |
| Sugiura, 2011, Japan [15] | Yes | Cross-sectional | 293 (age 60.2 ± 6.2) | Postmenopausal female | Tertile of BCX intake Q1 (0.00–0.30 mg/day) Q2 (0.31–1.21 mg/day) Q3 (1.22–7.91 mg/day) | Odds ratios for BMD | Yes | Higher daily intake of BCX significantly prevented the risk of osteoporosis. | Fair |
| Hayhoe, 2017, United Kingdom [16] | Yes | Prospective cohort (12.5 mean years) | Fracture analysis data, 25,566; ultrasound analysis data, 14,877 (age 39–79) | Male, pre-/postmenopausal female | Quintile of BCX intake, quintile of serum BCX concentration | Calcaneal broadband ultrasound attenuation (BUA); total fracture; hip fracture; spine fracture; wrist fracture | Yes | The amount of BCX intake is positively related to the higher BUA value in women. In men, the hip fracture risk was significantly lower in the 5th quintile as compared with the 1st quintile with a 0.65 hazard ratio. | Good |
| Dai, 2014, Singapore [21] | Yes | Prospective cohort (9.9 mean years) | 63154 (age 45–74) | Male, female | Quartile of BCX intake | Incidence of hip fracture | Yes | Intake of BCX was insignificant in reducing the risk of hip fracture in both males and females. | Good |
| Sahni, 2009 (2), United States [22] | Yes | Prospective cohort (17 years) | 929 (age 75 ± 5) | Male, pre-/postmenopausal female | Tertile of BCX intake | Hazard ratios for hip fracture | Yes | There was an absence of evidence that the intake of BCX plays a role in the reduction of the risk of hip fracture. | Fair |
| Liu, 2018, China [23] | Yes | Case-control | Case, 196 (age 44.0–60.0); control, 196 (age 43.2–60.0) | Male, pre-/postmenopausal female | Quartile of BCX intake (mean value): Q1 (0.0762 mg/day) Q2 (0.1589 mg/day) Q3 (0.3139 mg/day) Q4 (0.8341 mg/day) | Odds ratios for skeletal fluorosis | Yes | Intake of BCX was ineffective in reducing the risk of skeletal fluorosis. | Fair |
| Cao, 2018, China [24] | Yes | Case-control | Case, 1070 (age 52–83); control, 1070 (age 52–83) | Male, postmenopausal female | Quartile of BCX intake (mean value): Q1 (0.030–0.031 mg/day) Q2 (0.063–0.064 mg/day) Q3 (0.096–0.097 mg/day) Q4 (0.151–0.164 mg/day) | Odds ratios for hip fracture | Yes | The highest consumption quartile of BCX showed significantly reduced odd ratios on hip fractures. Subgroup analysis by gender revealed a corresponding result in terms of reducing hip fracture risk. | Good |
| Zhang, 2016, China [25] | No | Prospective cohort (3.1 mean years) | 2831 (age 50–75) | Male, postmenopausal female | Quartile of serum BCX concentration | BMD of the whole body, hip (total), femur neck, trochanter, intertrochanter | Yes | The serum level of BCX was positively correlated to the higher value of lumber spine and femur neck BMD in postmenopausal women. | Fair |
| Sugiura, 2016, Japan [26] | No | Prospective cohort (4 years) | 187 (age 60.5 ± 5.8) | Postmenopausal female | Low (0.24–1.84 μM) or high (1.88–10.53 μM) level of serum BCX concentration | Odds ratios for osteoporosis | Yes | The higher serum concentration of BCX with a higher intake of Vitamin C showed a significantly reduced risk of osteoporosis compared to the lower serum concentration of BCX with a low intake of vitamin C. | Fair |
| Sugiura, 2012, Japan [27] | No | Prospective cohort (4 years) | 187 (age 60.5 ± 5.8) | Postmenopausal female | Tertile of serum BCX concentration Q1 (0.24–1.41 μM) Q2 (1.43–2.39 μM) Q3 (2.41–10.53 μM) | Odds ratios for osteoporosis and osteopenia | Yes | The higher serum concentration of BCX was significantly related to the reduced risk of osteopenia and osteoporosis. | Good |
| Imagama, 2011, Japan [28] | No | Cross-sectional | 286 (age 50–85) | Male, female | Serum cryptoxanthin concentration (mean ± SD) Case, 0.25 ± 0.16 μM; control, 0.35 ± 0.33 μM | Existence of lumbar osteophyte | Not reported | The serum level of cryptoxanthin was significantly higher in ‘no osteophytes’ group. | Fair |
| Sahni. 2009 (1), United States [29] | No | Prospective cohort (4 years) | 874 (age 75 ± 5) | Male, pre-/postmenopausal female | Tertile of BCX intake | Femur BMD; spine BMD; radius BMD | Yes | The intake of BCX was not related to the changes in any type of BMD. | Fair |
| Sugiura, 2008, Japan [30] | No | Cross-sectional | 699 (age 30–70) | Male, pre-/postmenopausal female | Quartile of serum BCX concentration Q1 (0.22–1.07 mM) Q2–4 (1.10–10.53 mM) | Correlation analysis; odds ratios for low level of BMD | Yes | Positive correlations between serum BCX and BMD were observed in the postmenopausal female. | Fair |
| Yang, 2008, United States [31] | No | Case-control | Case, 30 (age 63.3 ± 10.8); control, 29 (age 62.1 ± 6.2) | Postmenopausal female | Serum BCX concentration (mean ± SD) Case, 0.27 ± 0.18 μM; control, 0.43 ± 0.36 μM Dietary BCX intake (mean ± SD) Case, 0.16 ± 0.19 mg/day; control, 0.09 ± 0.15 mg/day | Incidence of osteoporosis | Yes | The average serum concentration of BCX was significantly high in the control group compared to the osteoporosis group. Dietary BCX showed an opposite aspect as the overall intake of BCX was higher in the osteoporosis group. | Fair |
| Maggio, 2006, Italy [32] | No | Case-control | Case, 45 (age 70.3 ± 6.4); control, 45 (age 70.1 ± 5.9) | Postmenopausal female | Plasma BCX concentration Case, μM; 0.230 (0.129–0.397); control, 0.580 (0.363–0.715) μM | Incidence of osteoporosis | Not reported | The plasma concentration of BCX was significantly higher in control compared to the osteoporotic group. | Fair |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.J.; Anh, N.H.; Diem, N.C.; Park, S.; Cho, Y.H.; Long, N.P.; Hwang, I.G.; Lim, J.; Kwon, S.W. Effects of β-Cryptoxanthin on Improvement in Osteoporosis Risk: A Systematic Review and Meta-Analysis of Observational Studies. Foods 2021, 10, 296. https://doi.org/10.3390/foods10020296
Kim SJ, Anh NH, Diem NC, Park S, Cho YH, Long NP, Hwang IG, Lim J, Kwon SW. Effects of β-Cryptoxanthin on Improvement in Osteoporosis Risk: A Systematic Review and Meta-Analysis of Observational Studies. Foods. 2021; 10(2):296. https://doi.org/10.3390/foods10020296
Chicago/Turabian StyleKim, Sun Jo, Nguyen Hoang Anh, Nguyen Co Diem, Seongoh Park, Young Hyun Cho, Nguyen Phuoc Long, In Guk Hwang, Johan Lim, and Sung Won Kwon. 2021. "Effects of β-Cryptoxanthin on Improvement in Osteoporosis Risk: A Systematic Review and Meta-Analysis of Observational Studies" Foods 10, no. 2: 296. https://doi.org/10.3390/foods10020296
APA StyleKim, S. J., Anh, N. H., Diem, N. C., Park, S., Cho, Y. H., Long, N. P., Hwang, I. G., Lim, J., & Kwon, S. W. (2021). Effects of β-Cryptoxanthin on Improvement in Osteoporosis Risk: A Systematic Review and Meta-Analysis of Observational Studies. Foods, 10(2), 296. https://doi.org/10.3390/foods10020296