Changes in Ultra-Processed Food Consumption and Lifestyle Behaviors Following COVID-19 Shelter-in-Place: A Retrospective Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Site
2.2. Survey Description
2.3. Data Collection
2.4. Key Outcome Measures
2.4.1. Demographic, Anthropometric, and Behavioral Measures
2.4.2. Dietary Intake
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Changes in Lifestyle Behaviors, Diet, and Weight during Shelter-in-Place
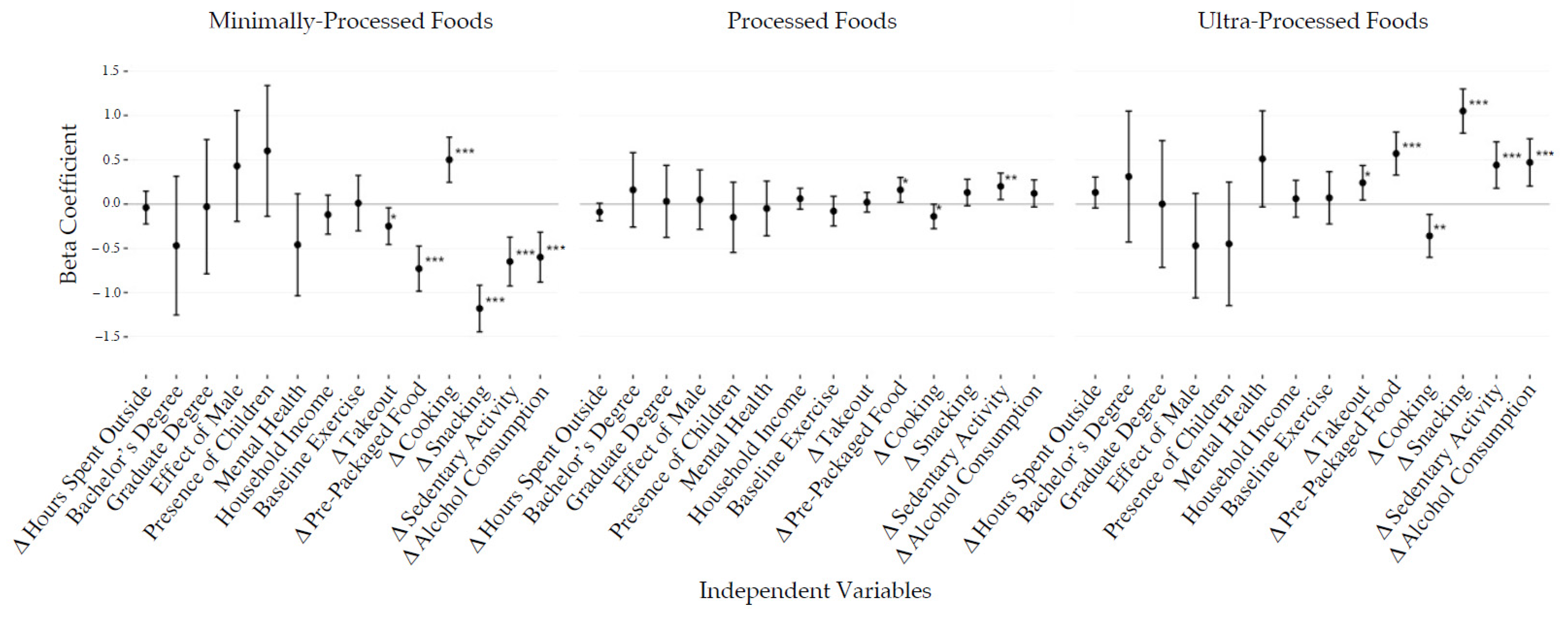
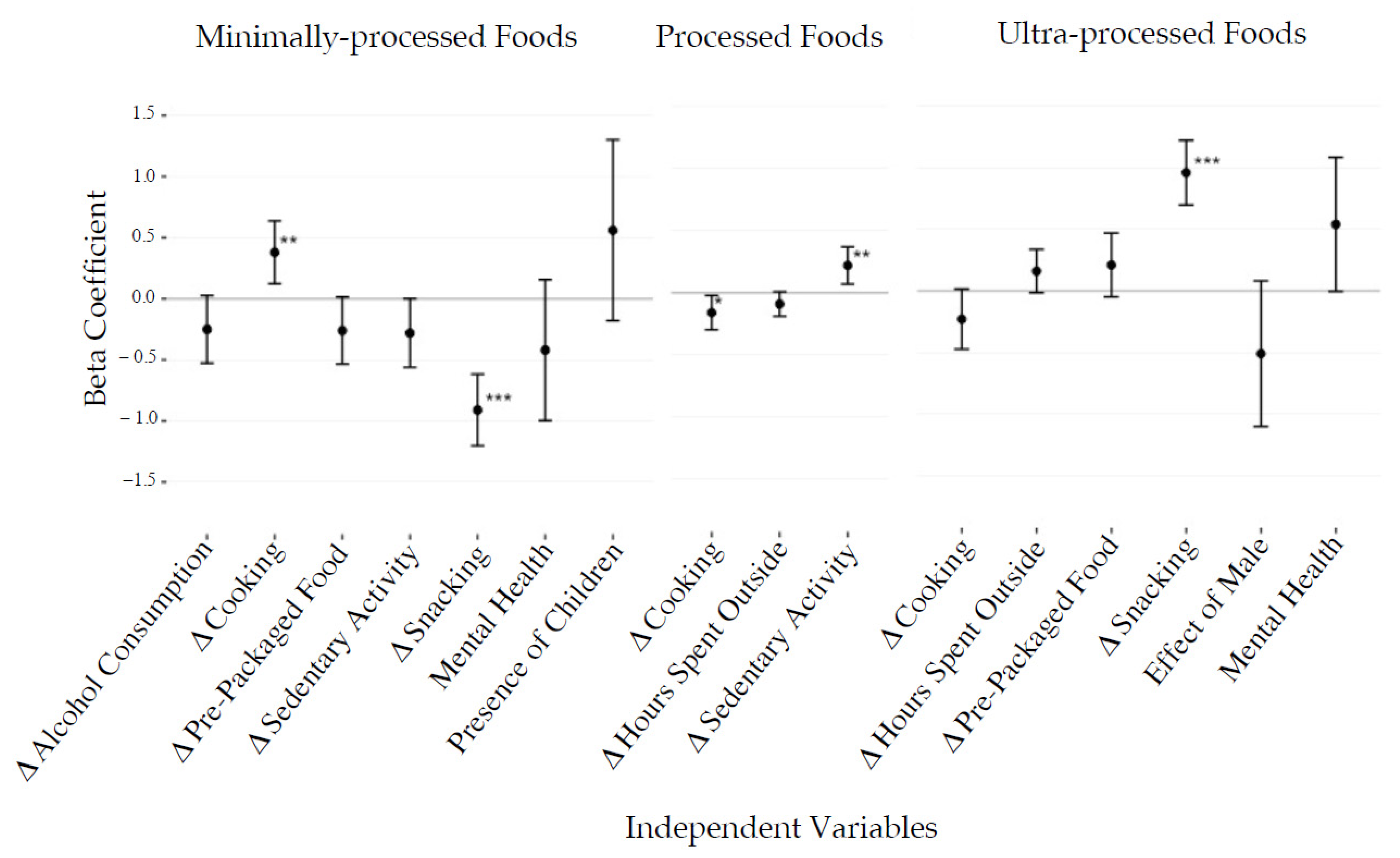
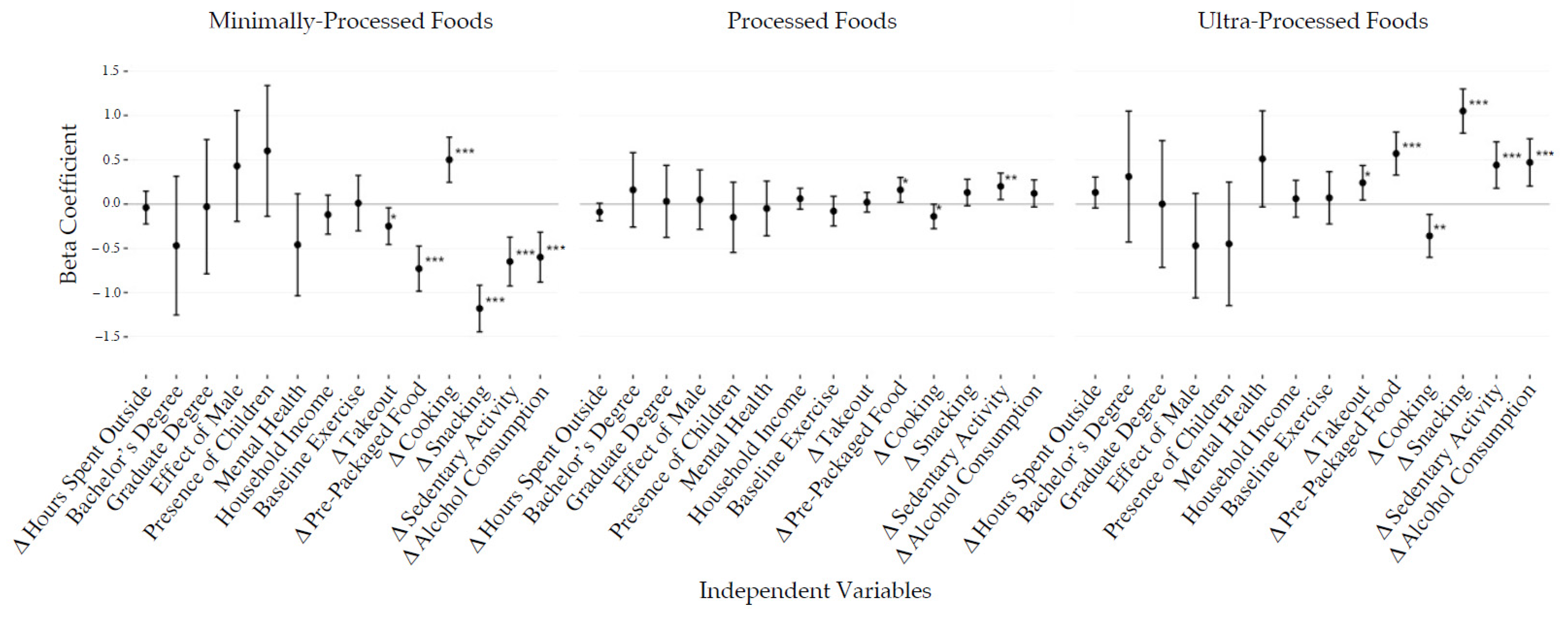
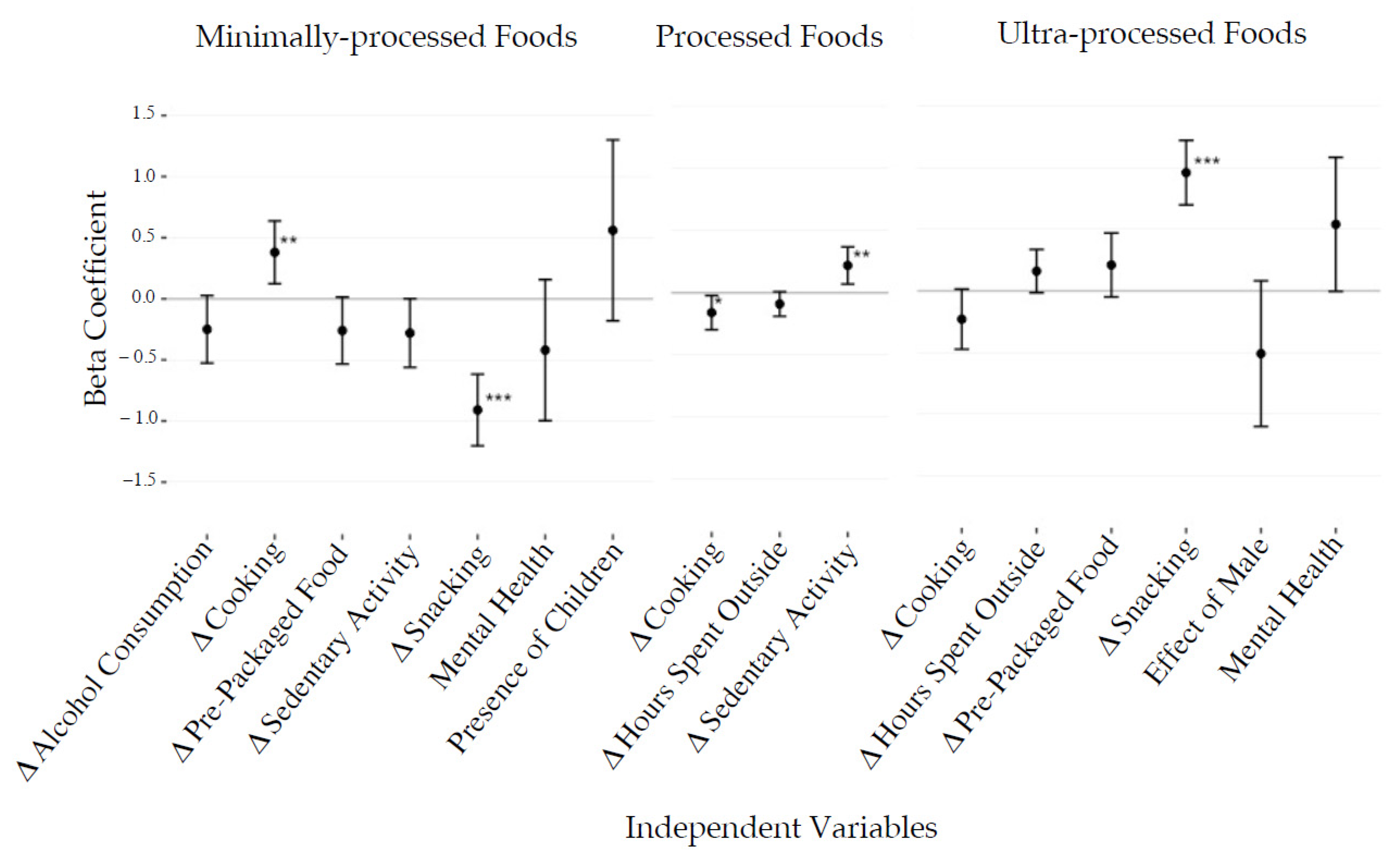
3.3. Demographic and Behavioral Factors Related to Diet Change
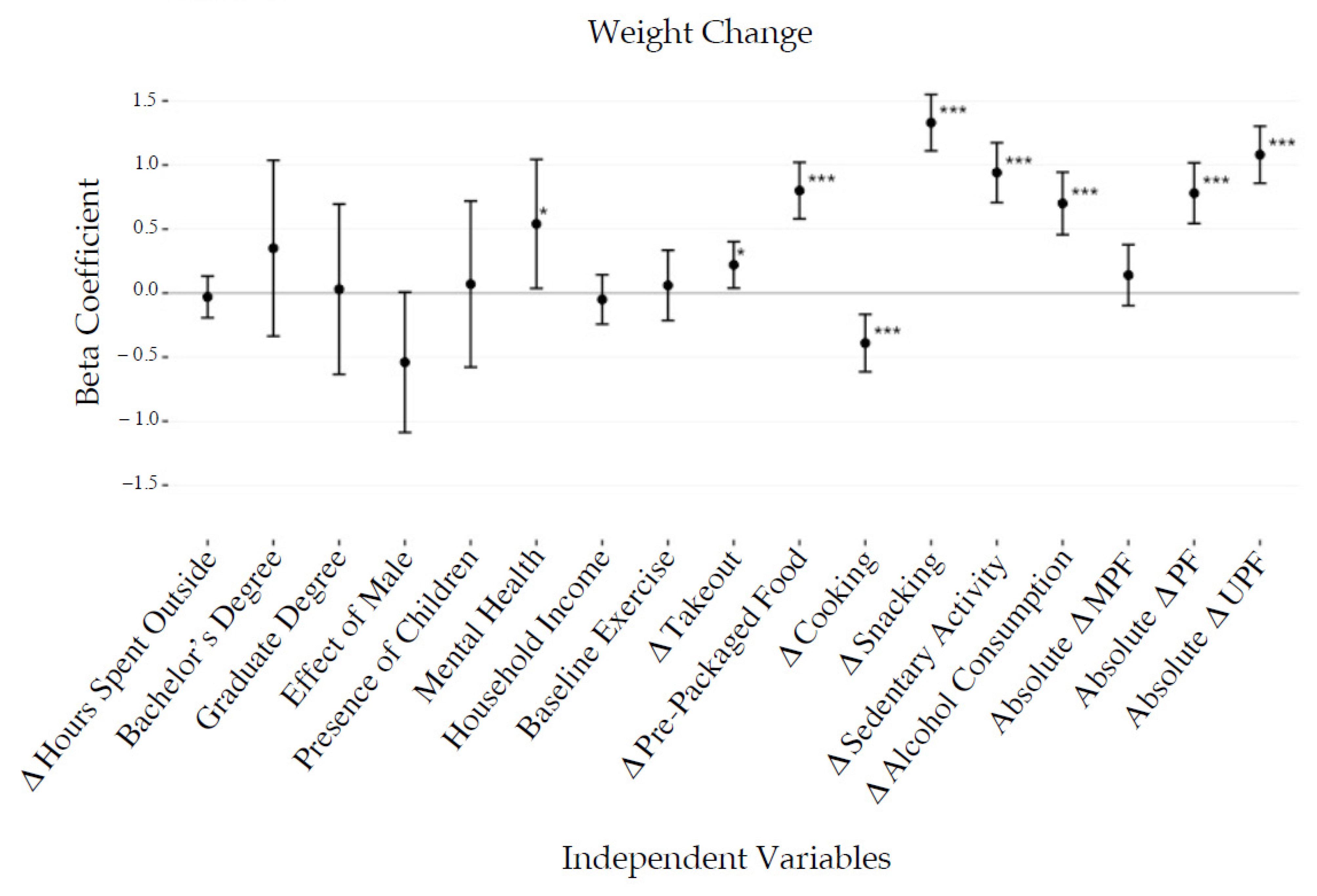
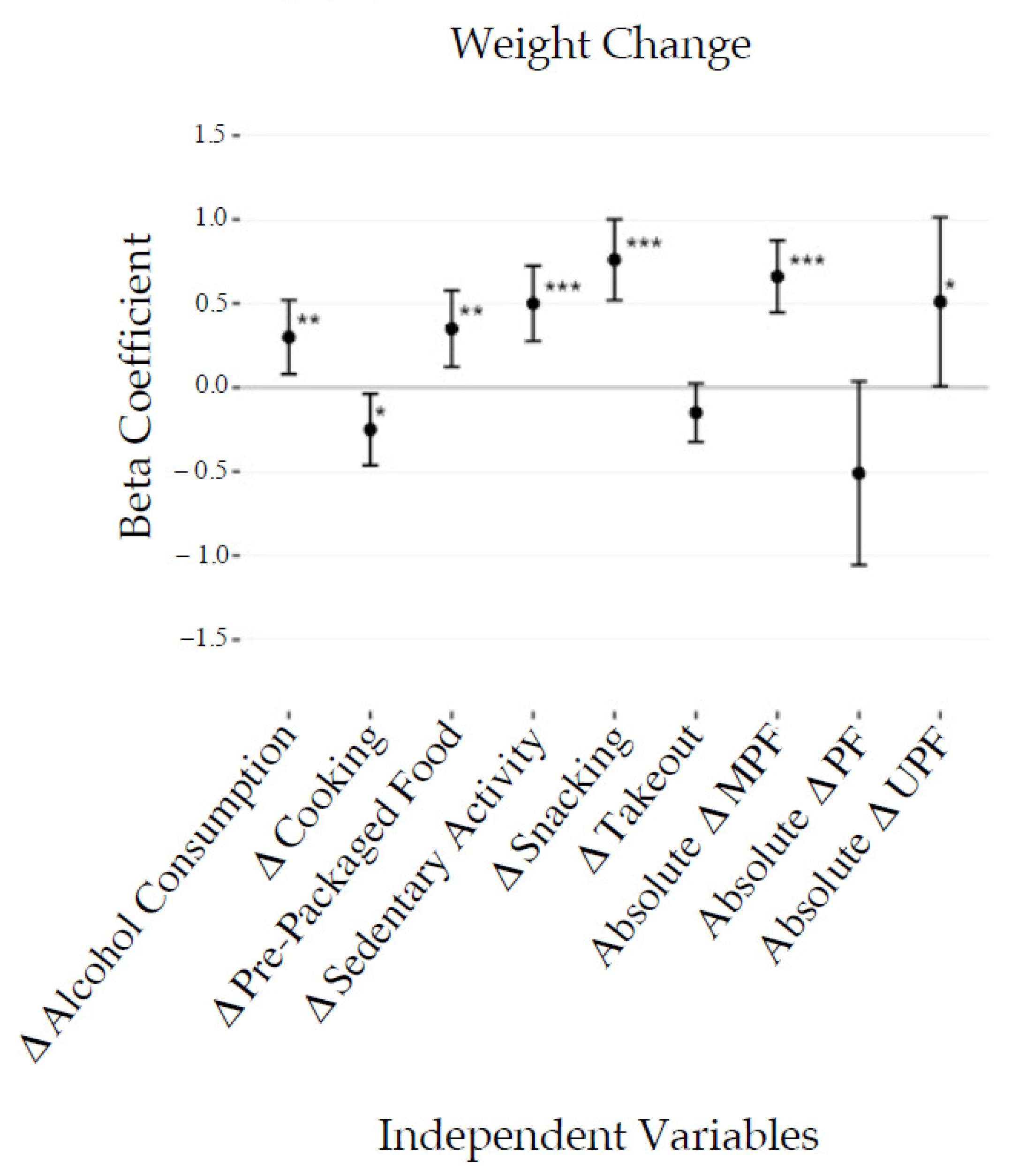
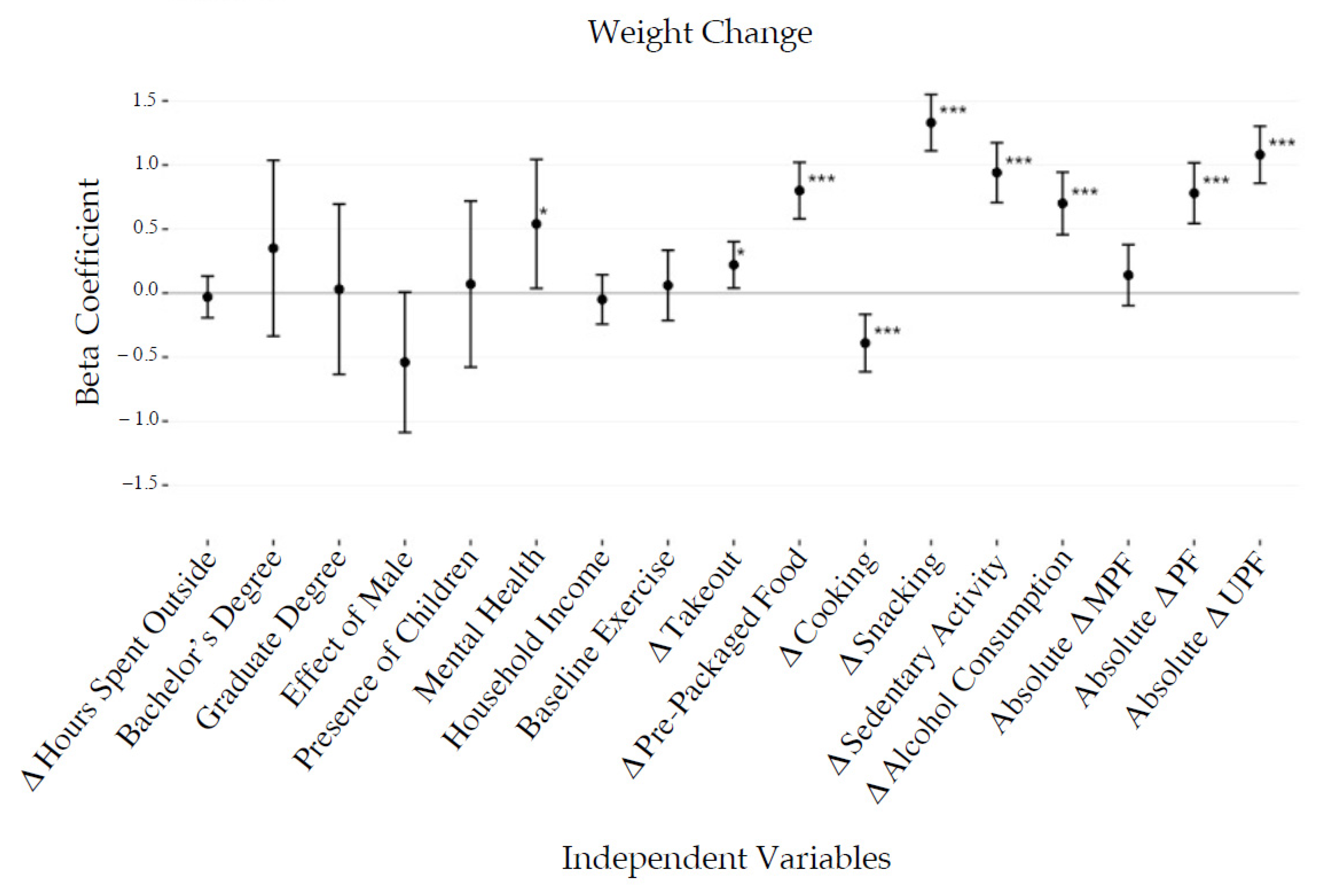
3.4. Anthropometric, Demographic, and Behavioral Factors Related to Weight Change
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gostin, L.O.; Wiley, L.F. Governmental Public Health Powers During the COVID-19 Pandemic: Stay-at-home Orders, Business Closures, and Travel Restrictions. JAMA 2020, 323, 2. [Google Scholar] [CrossRef] [PubMed]
- Kanu, F.A.; Smith, E.E.; Offutt-Powell, T.; Hong, R.; Delaware Case Investigation and Contact Tracing Teams; Dinh, T.; Pevzner, E. Declines in SARS-CoV-2 Transmission, Hospitalizations, and Mortality After Implementation of Mitigation Measures—Delaware, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1691–1694. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Karaca-Mandic, P.; Georgiou, A. Association of Stay-at-Home Orders with COVID-19 Hospitalizations in 4 States. JAMA 2020, 323, 2522. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Brynjolfsson, E.; Horton, J.; Ozimek, A. COVID-19 and Remote Work: An Early Look at US Data; National Bureau of Economic Research: Boston, MA, USA, 2020; Volume 3. [Google Scholar]
- Ozimek, A. The Future of Remote Work. SSRN J. 2020. [Google Scholar] [CrossRef]
- Bick, A.; Blandin, A.; Mertens, K. Work from Home after the COVID-19 Outbreak; Federal Reserve Bank of Dallas: Dallas, TX, USA, 2020; Volume 23. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, M.; Nieto, C.; Barquera, S. Good Deeds and Cheap Marketing: The Food Industry in the Time of COVID-19. Obesity 2020, 28, 1578–1579. [Google Scholar] [CrossRef]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e3. [Google Scholar] [CrossRef] [Green Version]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef]
- Askari, M.; Heshmati, J.; Shahinfar, H.; Tripathi, N.; Daneshzad, E. Ultra-processed food and the risk of overweight and obesity: A systematic review and meta-analysis of observational studies. Int. J. Obes. 2020, 44, 2080–2091. [Google Scholar] [CrossRef]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Alles, B.; Debras, C.; Druesne-Pecollo, N.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultraprocessed Food Consumption and Risk of Type 2 Diabetes among Participants of the NutriNet-Santé Prospective Cohort. JAMA Intern. Med. 2020, 180, 283. [Google Scholar] [CrossRef]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Alles, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, l1451. [Google Scholar] [CrossRef] [Green Version]
- Fiolet, T.; Srour, B.; Sellem, L.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Alles, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnabel, L.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Srour, B.; Hercberg, S.; Buscail, C.; Julia, C. Association between Ultraprocessed Food Consumption and Risk of Mortality Among Middle-aged Adults in France. JAMA Intern. Med. 2019, 179, 490. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hu, E.A.; Rebholz, C.M. Ultra-processed food intake and mortality in the USA: Results from the Third National Health and Nutrition Examination Survey (NHANES III, 1988–1994). Public Health Nutr. 2019, 22, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Rojo, R.; Sandoval-Insausti, H.; López-Garcia, E.; Graciani, A.; Ordovás, J.M.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Consumption of Ultra-Processed Foods and Mortality: A National Prospective Cohort in Spain. Mayo Clin. Proc. 2019, 94, 2178–2188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The Impact of COVID-19 Stay-At-Home Orders on Health Behaviors in Adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Kriaucioniene, V.; Bagdonaviciene, L.; Rodríguez-Pérez, C.; Petkeviciene, J. Associations between Changes in Health Behaviours and Body Weight during the COVID-19 Quarantine in Lithuania: The Lithuanian COVIDiet Study. Nutrients 2020, 12, 3119. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attina, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Alles, B.; Andreeva, V.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March–May 2020): Results from the French NutriNet-Santé cohort study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Mazidii, M.; Leeming, E.; Merino, J.; Nguyen, L.; Selvachandran, S.; Maher, T.; Kadé, K.; Murray, B.; Graham, M.; Sudre, C.; et al. Impact of COVID-19 on Health Behaviours and Body Weight: A Prospective Observational Study in a Cohort of 1.1 Million UK and US Individuals. Res. Sq. 2021. In Review. [Google Scholar] [CrossRef]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Lamarche, B.; Brassard, D.; Lapointe, A.; Laramée, C.; Kearney, M.; Côté, M.; Bélranger-Gravel, A.; Desroches, S.; Lemieux, S.; Plante, C. Changes in diet quality and food security among adults during the COVID-19–related early lockdown: Results from NutriQuébec. Am. J. Clin. Nutr. 2021, 113, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Poskute, A.S.; Nzesi, A.; Geliebter, A. Changes in food intake during the COVID-19 pandemic in New York City. Appetite 2021, 163, 105191. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.; Benson, T.; McCloat, A.; Mooney, E.; Elliott, C.; Dean, M.; Lavelle, F. Changes in Consumers’ Food Practices during the COVID-19 Lockdown, Implications for Diet Quality and the Food System: A Cross-Continental Comparison. Nutrients 2020, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- Marty, L.; de Lauzon-Guillain, B.; Labesse, M.; Nicklaus, S. Food choice motives and the nutritional quality of diet during the COVID-19 lockdown in France. Appetite 2021, 157, 105005. [Google Scholar] [CrossRef] [PubMed]
- Buckland, N.J.; Swinnerton, L.F.; Ng, K.; Price, M.; Wilkinson, L.L.; Myers, A.; Dalton, M. Susceptibility to increased high energy dense sweet and savoury food intake in response to the COVID-19 lockdown: The role of craving control and acceptance coping strategies. Appetite 2021, 158, 105017. [Google Scholar] [CrossRef] [PubMed]
- Fracassa, D. Bay Area Shelter-in-Place Orders will Be Extended to End of May. SF Chronicle. Available online: https://www.sfchronicle.com/bayarea/article/Bay-Area-counties-extend-coronavirus-stay-at-home-15229291.php (accessed on 19 April 2021).
- Jay, J.A.; D’Auria, R.; Nordby, J.C.; Rice, D.A.; Cleveland, D.A.; Friscia, A.; Kissinger, S.; Levis, M.; Malan, H.; Rajagopal, D.; et al. Reduction of the carbon footprint of college freshman diets after a food-based environmental science course. Clim. Chang. 2019, 154, 547–564. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and alidity of a Semiquantitative Food Frequency Questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Malan, H.; Amsler Challamel, G.; Silverstein, D.; Hoffs, C.; Spang, E.; Pace, S.A.; Malagueño, B.L.R.; Gardner, C.D.; Wang, M.C.; Slusser, W.; et al. Impact of a Scalable, Multi-Campus “Foodprint” Seminar on College Students’ Dietary Intake and Dietary Carbon Footprint. Nutrients 2020, 12, 2890. [Google Scholar] [CrossRef]
- Smaira, F.I.; Mazzolani, B.C.; Esteves, G.P.; André, H.C.S.; Amarante, M.C.; Castanho, D.F.; Campos, K.J.; Benatti, F.B.; Pinto, A.J.; Roschel, H.; et al. Poor Eating Habits and Selected Determinants of Food Choice Were Associated With Ultraprocessed Food Consumption in Brazilian Women During the COVID-19 Pandemic. Front Nutr. 2021, 8, 672372. [Google Scholar] [CrossRef]
- Dunford, E.; Popkin, B. Disparities in Snacking Trends in US Adults over a 35 Year Period from 1977 to 2012. Nutrients 2017, 9, 809. [Google Scholar] [CrossRef] [Green Version]
- Alves Melo, E. Dietary Guidelines for the Brazilian Population; Ministry of Health Brazil: Brasilia, Brazil, 2015; Volume 152.
- Verhoeven, A.A.C.; Adriaanse, M.A.; de Ridder, D.T.D.; de Vet, E.; Fennis, B.M. Less is more: The effect of multiple implementation intentions targeting unhealthy snacking habits: Multiple implementation intentions. Eur. J. Soc. Psychol. 2013, 43, 344–354. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Meyer, S.M.; Landry, M.J.; Gustat, J.; Lemon, S.C.; Webster, C.A. Physical distancing ≠ physical inactivity. Transl. Behav. Med. 2021, 11, 941–944. [Google Scholar] [CrossRef]
- Keller, A. What is an Acceptable Survey Response Rate? National Social Norms Center. Available online: http://socialnorms.org/what-is-an-acceptable-survey-response-rate/ (accessed on 20 April 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Response | % (n = 589) |
|---|---|---|
| Sex | Male | 26.1% (154) |
| Female | 73.9% (435) | |
| Race or ethnicity | Black | 2.0% (12) |
| Native American | 0.3% (2) | |
| Asian | 10.7% (63) | |
| Native Hawaiian or Pacific Islander | 0.2% (1) | |
| Hispanic | 4.8% (28) | |
| Caucasian | 73.7% (434) | |
| Bi- or Multi-racial | 5.1% (30) | |
| Other | 3.2% (19) | |
| BMI (kg/m2) | Mean (SD) | 27.36 (5.91) |
| Smoking status | Smokers | 2.5% (15) |
| Parents of children requiring attention | Yes | 16.6% (98) |
| Self-reported mental health challenges | Yes | 35.3% (208) |
| Highest educational attainment | <Bachelor’s degree | 18.7% (110) |
| Bachelor’s degree | 36.5% (215) | |
| Graduate degree | 44.8% (264) | |
| Monthly household income | <USD 1000 | 2.7% (16) |
| USD 1000–2499 | 5.4% (32) | |
| USD 2500–4999 | 16.6% (98) | |
| USD 5000–9999 | 30.6% (180) | |
| USD 10,000–24,999 | 25.8% (152) | |
| >USD 25,000 | 18.8% (111) | |
| Exercise frequency | Never | 2.5% (15) |
| 1–4 sessions per month | 11.9% (70) | |
| 1–3 sessions per week | 32.1% (189) | |
| 4–7 sessions per week | 46.5% (274) | |
| >7 sessions per week | 7.0% (41) |
| Health Behaviors | Changes % (n) | ||
|---|---|---|---|
| Increased | Decreased | No Change | |
| Lifestyle Behaviors | |||
| Takeout food | 24.1% (142) | 52.8% (311) | 22.5% (149) |
| Ready-to-eat packaged food | 14.4% (85) | 48.9% (288) | 47.6% (315) |
| Cooking | 64.3% (379) | 10.9% (64) | 25.1% (166) |
| Snacking | 36.7% (216) | 16.1% (95) | 47.3% (313) |
| Sedentary activity | 67.1% (395) | 9.7% (57) | 22.8% (151) |
| Hours outside the home | 1.5% (9) | 82.2% (484) | 17.2% (114) |
| Proportion of Calories Consumed by Level of Processing | |||
| Proportion MPF calories | 35.3% (208) | 50.4% (297) | 14.2% (90) |
| Proportion PF calories | 42.3% (268) | 43.3% (255) | 14.0% (91) |
| Proportion UPF calories | 49.1% (289) | 36.3% (214) | 14.2% (92) |
| Weight | |||
| Weight | 48.4% (285) | 25.1% (148) | 27.4% (181) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobba, W.; Landry, M.J.; Cunanan, K.M.; Marcone, A.; Gardner, C.D. Changes in Ultra-Processed Food Consumption and Lifestyle Behaviors Following COVID-19 Shelter-in-Place: A Retrospective Study. Foods 2021, 10, 2553. https://doi.org/10.3390/foods10112553
Sobba W, Landry MJ, Cunanan KM, Marcone A, Gardner CD. Changes in Ultra-Processed Food Consumption and Lifestyle Behaviors Following COVID-19 Shelter-in-Place: A Retrospective Study. Foods. 2021; 10(11):2553. https://doi.org/10.3390/foods10112553
Chicago/Turabian StyleSobba, Walter, Matthew J. Landry, Kristen M. Cunanan, Alessandra Marcone, and Christopher D. Gardner. 2021. "Changes in Ultra-Processed Food Consumption and Lifestyle Behaviors Following COVID-19 Shelter-in-Place: A Retrospective Study" Foods 10, no. 11: 2553. https://doi.org/10.3390/foods10112553
APA StyleSobba, W., Landry, M. J., Cunanan, K. M., Marcone, A., & Gardner, C. D. (2021). Changes in Ultra-Processed Food Consumption and Lifestyle Behaviors Following COVID-19 Shelter-in-Place: A Retrospective Study. Foods, 10(11), 2553. https://doi.org/10.3390/foods10112553