Knowledge in Transition in Healthcare




Abstract
:1. Introduction
2. Literature Review
2.1. Knowledge in Transition Conceptualization
2.2. Dynamic Knowledge versus Static Knowledge
3. Methodology
3.1. Research Context
3.2. Data Collection and Analysis
4. Findings
4.1. Static and Dynamic Knowledge Transition Processes in the Filed—the Perceptions of the Health Professionals
4.1.1. Individual Knowledge
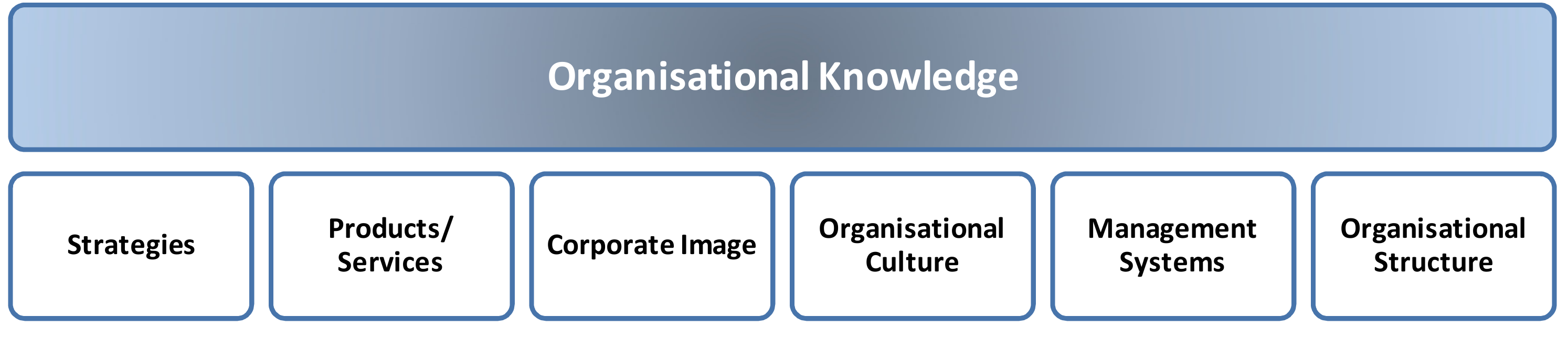
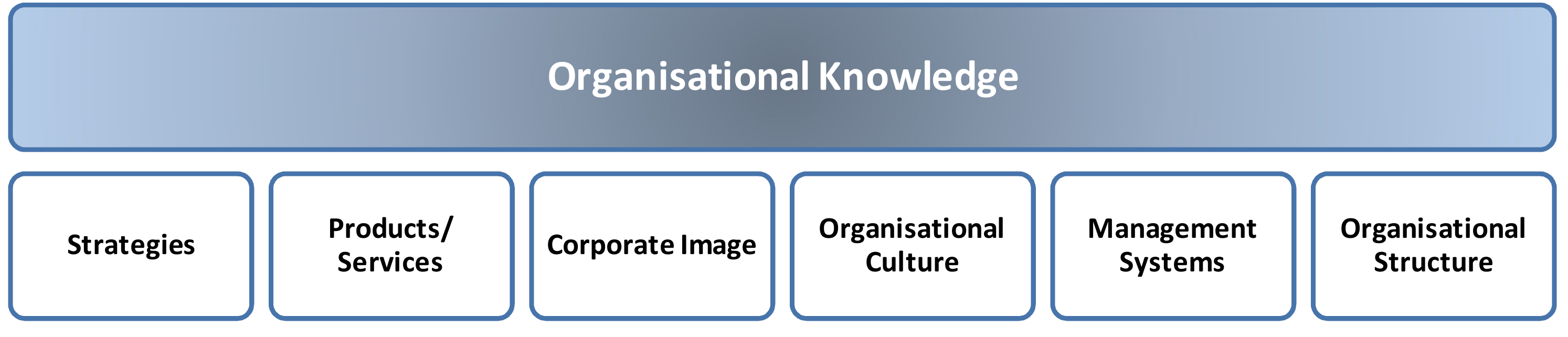
4.1.2. Organizational Knowledge
4.2. Knowledge Transition Mechanisms
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Interview Script
- Which is the main organizational knowledge that is important to frame your individual knowledge?
- How does the organization use the worker’s individual knowledge to help solve emergency room problems?
- Do you help to answer the everyday emergency room problems? Could you describe a situation where that has happened?
- Which activities and related competencies are needed to perform your job?
- a)
- Activities
- b)
- Technical Competencies
- c)
- Organizational Competencies
- d)
- Cognitive Competencies
- e)
- Social Competencies
- What are the procedures when a problem occurs? Could you describe a situation where there was a problem, and how you solved it?
- Describe some situations to help promote the transition of knowledge?
- Which types of knowledge are in transition?
Appendix B. Tables of Competencies

{kind=link}
{kind=link}
{kind=link}
| Activities |
| 1) Direct Care |
| 2) Indirect Patient-Centred Care |
| 3) Personal Development |
| 4) Writing Services |
| 5) Non-Nursing Duties |
| 6) Patient Assessment |
| 7) Patient Education |
| Technical Competencies |
| Human development stages |
| Anatomy |
| Physiology |
| Pharmacology |
| Organizational Competencies |
| Informed consent |
| Handling of evidence |
| Mandatory reporting of child and elder abuse |
| Rules, norms, and internal regulations |
| Organisational structure |
| Cognitive competencies |
| Problem-solving |
| Critical Thinking |
| Emotional intelligence |
| Social Competencies |
| Working habits |
| Communication |
| Leadership skills |
| Teamwork |
| Empathy |
| Activities |
| Cardiac First Responder |
| Occupational First Aider |
| Emergency First Responder |
| Intermediate Life Support |
| Technical Competencies |
| Administration of medicines |
| Bleeding control |
| Management of burns |
| Splinting of suspected fractures and spinal injuries |
| Childbirth |
| Cardiopulmonary resuscitation |
| Semi-automatic defibrillation |
| Oral suctioning |
| Insertion of oropharyngeal and nasopharyngeal airways |
| Pulse oximetry |
| Blood glucose monitoring |
| Auscultation of lung sounds |
| Administration of medications |
| Organizational Competencies |
| Handling of evidence |
| Mandatory reporting of child and elder abuse |
| Rules, norms, and internal regulations |
| Organisational structure |
| Cognitive competencies |
| Problem-Solving |
| Critical Thinking |
| Emotional intelligence |
| Conflict resolution |
| Social Competencies |
| Working habits |
| Communication |
| Leadership skills |
| Teamwork |
| Empathy |
| Activities |
| Setting up specialised hospital equipment |
| Assisting physicians with the application of casts |
| Transporting patients |
| Providing routine personal care to patients |
| Technical Competencies |
| Anatomy |
| Physiology |
| Cognitive impairments |
| Nutrition |
| Mental health issues |
| Infection control |
| Personal care skills |
| Record-keeping skills |
| Organizational Competencies |
| Handling of evidence |
| Mandatory reporting of conflict situations |
| Rules, norms, and internal regulations |
| Organisational structure |
| Cognitive competencies |
| Problem-Solving |
| Critical Thinking |
| Emotional intelligence |
| Conflict resolution |
| Social Competencies |
| Working habits |
| Communication |
| Teamwork |
| Empathy |
References
- Parent, R.; Roy, M.; St-Jacques, D. A systems-based dynamic knowledge transfer capacity model. J. Knowl. Manag. 2007, 11, 81–93. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, G.D. Management strategies for individual knowledge and organizational knowledge. J. Knowl. Manag. 2002, 6, 31–39. [Google Scholar] [CrossRef]
- Wan, Z.; Haggerty, N.; Wang, Y. Individual level knowledge transfer in virtual settings: A review and synthesis. Int. J. Knowl. Manag. 2015, 11, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Blackler, F. Knowledge, Knowledge Work and Organizations: An Overview and Interpretation. Organ. Stud. 1995, 16, 1021–1046. [Google Scholar] [CrossRef] [Green Version]
- Amin, A.; Roberts, J. Knowing in action: Beyond communities of practice. Res. Policy 2008, 37, 353–369. [Google Scholar] [CrossRef]
- Bock, G.-W.; Zmud, R.W.; Kim, Y.-G.; Lee, J.-N. Behavioral intention formation in knowledge sharing: Examining the roles of extrinsic motivators, social-psychological forces, and organizational climate. Mis Q. Manag. Inf. Syst. 2005, 29, 87–111. [Google Scholar] [CrossRef]
- Majchrzak, A.; Wagner, C.; Yates, D. The impact of shaping on knowledge reuse for organizational improvement with Wikis. Mis Q. Manag. Inf. Syst. 2013, 37, 455–469. [Google Scholar] [CrossRef]
- Dal Mas, F.; Massaro, M.; Lombardi, R.; Garlatti, A. From Output to Outcome Measures in the Public Sector. A Structured Literature Review. Int. J. Organ. Anal. 2019, 27, 1631–1656. [Google Scholar] [CrossRef]
- Reay, S.; Collier, G.; Kennedy-Good, J.; Old, A.; Douglas, R.; Bill, A. Designing the future of healthcare together: Prototyping a hospital co-design space. CoDesign 2017, 13, 227–244. [Google Scholar] [CrossRef]
- Secundo, G.; Toma, A.; Schiuma, G.; Passiante, G. Knowledge transfer in open innovation: A classification framework for healthcare ecosystems. Bus. Process. Manag. J. 2019, 25, 144–163. [Google Scholar] [CrossRef]
- Bowser, J.; Saxena, S.; Fraser, H.; Marshall, A. A Healthy Outlook: Digital Reinvention in Healthcare; IBM Institute for Business Value: Armonk, NY, USA, 2019. [Google Scholar]
- Dal Mas, F.; Piccolo, D.; Edvinsson, L.; Skrap, M.; D’Auria, S. Strategy Innovation, Intellectual Capital Management and the Future of Healthcare. The case of Kiron by Nucleode. In Knowledge, People, and Digital Transformation: Approaches for a Sustainable Future; Matos, F., Vairinhos, V., Salavisa, I., Edvinsson, L., Massaro, M., Eds.; Springer: Cham, Germany, 2020; pp. 119–131. [Google Scholar]
- Presch, G.; Dal Mas, F.; Piccolo, D.; Sinik, M.; Cobianchi, L. The World Health Innovation Summit (WHIS) platform for sustainable development. From the digital economy to knowledge in the healthcare sector. In Intellectual Capital in the Digital Economy; Ordonez de Pablos, P., Edvinsson, L., Eds.; Routledge: London, UK, 2020; pp. 19–28. [Google Scholar]
- Dal Mas, F.; Piccolo, D.; Ruzza, D. Overcoming cognitive bias through intellectual capital management. The case of pediatric medicine. In Intellectual Capital in the Digital Economy; Ordonez de Pablos, P., Edvinsson, L., Eds.; Routledge: London, UK, 2020; pp. 123–133. [Google Scholar]
- Howdon, D.; Rice, N. Health care expenditures, age, proximity to death and morbidity: Implications for an ageing population. J. Health Econ. 2018, 57, 60–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaro, M.; Dumay, J.; Garlatti, A. Public sector knowledge management: A structured literature review. J. Knowl. Manag. 2015, 19, 530–558. [Google Scholar] [CrossRef]
- Coget, J.-F.; Keller, E. The critical decision vortex: Lessons from the emergency room. J. Manag. Inq. 2010, 19, 56–67. [Google Scholar] [CrossRef] [Green Version]
- Cobianchi, L.; Pugliese, L.; Peloso, A.; Dal Mas, F.; Angelos, P. To a New Normal: Surgery and COVID-19 during the Transition Phase. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Lopes, H. Estratégias e Competências; Estratégias Empresariais e Competências Chave: Lisbon, Portugal, 1999. [Google Scholar]
- Sousa, M.J. Innovation: The key for creating and sharing knowledge. In Effective Project Management through the Integration of Knowledge and Innovation; Jamil, G., Ed.; IGI Global: Hershey, PA, USA, 2015. [Google Scholar]
- Shotter, J. Knowledge in transition: The role of prospective, descriptive concepts in a practice-situated, hermeneutical-phronetic social science. Manag. Learn. 2012, 43, 245–260. [Google Scholar] [CrossRef]
- Prusak, L.; Davenport, T.H. Working Knowledge: How Organizations Manage. what They Know; Harvard Business Press: Cambridge, UK, 1998. [Google Scholar]
- Argote, L.; Ingram, P. Knowledge Transfer: A Basis for Competitive Advantage in Firms. Organ. Behav. Hum. Decis. Process. 2000, 82, 150–169. [Google Scholar] [CrossRef] [Green Version]
- Hansen, M.; Nohria, N.; Tierney, T. What’s your strategy for managing knowledge? Harv. Bus. Rev. 1999, 77, 106–116. [Google Scholar]
- Massaro, M.; Bardy, R.; Lepeley, M.T.; Dal Mas, F. Intellectual capital development in Business Schools. The role of “soft skills” in Italian Business Schools. In Proceedings of the 5th European Conference on Intellectual Capital, Bilbao, Spain, 11–12 April 2013; Academic Publishing Limited: Reading, UK, 2014; pp. 1–8. [Google Scholar]
- Jacquinet, M.; Curado, H.; Nobre, A.L.; Sousa, M.J.; Arraya, M.; Pimenta, R.; Martins, A.E. Management of Tacit Knowledge and the Issue of Empowerment of Patients and Stakeholders in the Health Care Sector in Healthcare Policy and Reform: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2019. [Google Scholar]
- Sousa, M.J.; Cascais, T.; Rodrigues, J.P. Action Research Study on Individual Knowledge Use in Organizational Innovation Processes. In Advances in Intelligent Systems and Computing; Rocha, A., Ed.; Springer: Cham, Germany, 2015; pp. 105–113. [Google Scholar]
- Levin, D.Z.; Cross, R. The Strength of Weak Ties You Can Trust: The Mediating Role of Trust in Effective Knowledge Transfer. Manag. Sci. 2004, 50, 1463–1613. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Choi, B. Knowledge management enablers, processes, and organizational performance: An integrative view and empirical examination. J. Manag. Inf. Syst. 2003, 20, 179–288. [Google Scholar]
- Sousa, M.J. Dynamic knowledge: An Action Research Project. Int. J. Knowl. Cult. Chang. Manag. 2010, 10, 317–331. [Google Scholar] [CrossRef]
- Sousa, M.J. Knowledge profiles boosting innovation. Knowl. Manag. 2013, 12, 35–46. [Google Scholar] [CrossRef]
- Sousa, M.J. Knowledge Integration in Problem Solving Processes. In Advances in Intelligent Systems and Computing; Rocha, Á., Correia, A.M., Wilson, T., Stroetmann, K.A., Eds.; Springer: Cham, Germany, 2013. [Google Scholar]
- Cummings, J.N. Work Groups, Structural Diversity, and Knowledge Sharing in a Global Organization. Manag. Sci. 2004, 50, 352–364. [Google Scholar] [CrossRef] [Green Version]
- Cannavacciuolo, L.; Iandoli, L.; Ponsiglione, C.; Maracine, V.; Scarlat, E.; Nica, A.S. Mapping knowledge networks for organizational re-design in a rehabilitation clinic. Bus. Process. Manag. J. 2017, 23, 329–348. [Google Scholar] [CrossRef]
- Zanin, F.; Massaro, M.; Bagnoli, C. Towards a Competitive Knowledge Management Strategy Approach in the University Setting: The Case of Ca’Foscari; University of Venice: Venice, Italy, 2013; ISBN 9781466644359. [Google Scholar]
- Renaudin, M.; Dal Mas, F.; Garlatti, A.; Massaro, M. Knowledge Management and cultural change in a knowledge-intensive public organization. In 4th Knowledge Management and Intellectual Capital Excellence Awards; Remeniy, D., Ed.; Academic Conferences and Publishing International Limited: Reading, UK, 2018; pp. 85–96. [Google Scholar]
- Nonaka, I.; Toyama, R.; Konno, N. SECI, Ba and Leadership: A Unified Model of Dynamic Knowledge Creation. Long Range Plan. 2000, 33, 5–34. [Google Scholar] [CrossRef]
- Herschel, R.T.; Nemati, H.; Steiger, D. Tacit to explicit knowledge conversion: Knowledge exchange protocols. J. Knowl. Manag. 2001, 5, 107–116. [Google Scholar] [CrossRef]
- Addis, M. Tacit and explicit knowledge in construction management. Constr. Manag. Econ. 2016, 32, 439–445. [Google Scholar] [CrossRef] [Green Version]
- Chilton, M.A.; Bloodgood, J.M. The dimensions of tacit & explicit knowledge: A description and measure. Int. J. Knowl. Manag. 2008, 4, 75–91. [Google Scholar]
- Jørgensen, R.; Scarso, E.; Edwards, K.; Ipsen, C. Communities of practice in healthcare: A framework for managing knowledge sharing in operations. Knowl. Process. Manag. 2019, 26, 152–162. [Google Scholar] [CrossRef]
- Sims, J.M. Communities of practice: Telemedicine and online medical communities. Technol. Soc. Chang. 2018, 126, 53–63. [Google Scholar] [CrossRef]
- Wimmer, H.; Yoon, V.Y.; Sugumaran, V. A multi-agent system to support evidence based medicine and clinical decision making via data sharing and data privacy. Decis. Support. Syst. 2016, 88, 51–66. [Google Scholar] [CrossRef]
- Panahi, S.; Watson, J.; Partridge, H. Conceptualising social media support for tacit knowledge sharing: physicians’ perspectives and experiences. J. Knowl. Manag. 2016, 20, 344–363. [Google Scholar] [CrossRef]
- Mura, M.; Lettieri, E.; Radaelli, G.; Spiller, N. Behavioural operations in healthcare: A knowledge sharing perspective. Int. J. Oper. Prod. Manag. 2016, 36, 1222–1246. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research Design and Methods, 5th ed.; Sage Publications, Inc: London, UK, 2014; ISBN 978-1-4522-4256-9. [Google Scholar]
- Massaro, M.; Moro, A.; Aschauer, E.; Fink, M. Trust, control and knowledge transfer in small business networks. Rev. Manag. Sci. 2019, 13, 267–301. [Google Scholar] [CrossRef] [Green Version]
- Ridder, H.-G.; Hoon, C.; McCandless Baluch, A. Entering a Dialogue: Positioning Case Study Findings towards Theory. Br. J. Manag. 2014, 25, 373–387. [Google Scholar] [CrossRef]
- Massaro, M.; Dumay, J.; Bagnoli, C. Transparency and the rhetorical use of citations to Robert Yin in case study research. Med. Acc. Res. 2019, 27, 44–71. [Google Scholar] [CrossRef]
- Cobianchi, L.; Dal Mas, F.; Piccolo, D.; Peloso, A.; Secundo, G.; Massaro, M.; Takeda, A.; Garcia Vazquez, A.; Verde, J.M.; Swanstrom, L.L.; et al. Digital transformation in healthcare. The challenges of translating knowledge in a primary research, educational and clinical centre. In Proceedings of the International Business Information Management Conference (35th IBIMA), Seville, Spain, 1–2 April 2020; Soliman, K.S., Ed.; IBIMA: Seville, Spain, 2020; pp. 6877–6888. [Google Scholar]
- Dal Mas, F.; Biancuzzi, H.; Massaro, M.; Miceli, L. Adopting a knowledge translation approach in healthcare co-production. A case study. Manag. Decis. 2020, in press. [Google Scholar]
- Lemire, N.; Souffez, K.; Laurendeau, M.C. Facilitating a Knowledge Translation Process. Knowledge review and facilitation tool; Institut Publique de Santé du Quebec: Quebec, 2013; ISBN 9782550575474. [Google Scholar]
- Savory, C. Translating knowledge to build technological competence. Manag. Decis. 2006, 44, 1052–1075. [Google Scholar] [CrossRef]
- Nonaka, I.; Takeuchi, I. The Knowledge-Creating Organization; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Tsoukas, H. The firm as a distributed knowledge system: A constructionist approach. Strat. Manag. J. 1996, 17, 11–25. [Google Scholar] [CrossRef]
- Polanyi, M. Knowing and Being: Essays; Chicago University Press: Chicago, IL, USA, 1969. [Google Scholar]
- Leonard, D.; Sensiper, S. The role of tacit knowledge in group innovation. Calif. Manag. Rev. 1998, 40, 112–132. [Google Scholar] [CrossRef]
- Le Boterf, G. Spécificité et valeur ajoutée de la pédagogie de la simulation; Éducation permanente: Paris, France, 1999. [Google Scholar]
- Green, R. The psychology of human error. Eur. J. Anaesthesiol. 2011, 16, 148–155. [Google Scholar] [CrossRef]

| Dynamic Knowledge | Static Knowledge |
|---|---|
| Opinions, behaviours, ideas, and informal conversation. Workshops, communities of practice, and meetings. | Reports, memos, document procedures, databases, and other kind of organisational documentation. |
| Competencies | Description |
| Technical Competencies | They integrate concepts about technical knowledge, including context and processes, and operational methods and means. They are the basis for the organisations’ strategic management of competencies. This kind of knowledge is easily shared because of its explicit nature. |
| Application in the Case Study | |
| The Healthcare Organisation does not have these competencies mapped. However, the participants in the interviews assumed the importance of developing a process of identifying the most valuable competencies for the organisation, not only technical competencies, but also organisational and social competencies, and creating some tables of competencies to identify the crucial competencies for each job position (Operation Assistants, Emergency Room Nurses, and Emergency Medical Technicians). | |
| Transition Process—translate into tables all the activities and tasks, and related competencies (reported in Appendix B). | |
| Competencies | Description |
| Organisational Competencies | They are the basis for the organization to develop beyond services and complement the technical aspects of the work. They create a sense of community, which can lead to an increase of trust and commitment by the workers that share beliefs and behavioral rules. |
| Application in the Case Study | |
| In the Emergency Room department, the health professionals have different visions about the healthcare organization, especially about the structure, even if they have the same perceptions about knowledge sharing. This becomes obvious when we analyse the different healthcare professionals’ opinions and thoughts. These different perspectives of the organization may be a barrier to translate individual knowledge into the organizational dimension. | |
| Transition Process—use of a shared language and common understandings linked to organizational culture, which is necessary to facilitate efficient communications and common understandings that focus on the essential role of trust, shared norms, and common identification. | |
| Competencies | Description |
| Cognitive Competencies | They integrate complex thinking skills and analytical models used in problem-solving situations, including problem identification and definition, recognition, analysis, implementation, and monitoring. |
| Application in the Case Study | |
| In the Emergency Room department, the healthcare professional uses processes of reflection, including individual reflection and collaborative reflection, around specific and complex problems/situations. | |
| Transition Process—through ongoing learning, including formal training, informal learning, observations, and discussions, as well as work experiences, the healthcare professionals develop and refine their problem-solving capabilities. They approach many problems on a daily basis, without a great deal of conscious thought about method or approach. When complex problems emerge, they recognize that they face difficulties that require collaborative problem-solving and therefore needs the team help. | |
| Competencies | Description |
| Social Competencies | These competencies include working habits, communication styles, leadership skills, and teamwork. |
| Application in the Case Study | |
| The Healthcare Organization developed teamwork competencies, communication, and informal and formal relationships by working in teams on a daily basis. | |
| Transition Process—the complex environment demands that problem-solving should be carried on by teams with cross-functional collaboration and interaction using social competencies to support collaborative work. Effective problem-solving includes communication and conflict resolution skills. | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousa, M.J.; Dal Mas, F.; Garcia-Perez, A.; Cobianchi, L. Knowledge in Transition in Healthcare. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 733-748. https://doi.org/10.3390/ejihpe10030054
Sousa MJ, Dal Mas F, Garcia-Perez A, Cobianchi L. Knowledge in Transition in Healthcare. European Journal of Investigation in Health, Psychology and Education. 2020; 10(3):733-748. https://doi.org/10.3390/ejihpe10030054
Chicago/Turabian StyleSousa, Maria José, Francesca Dal Mas, Alexeis Garcia-Perez, and Lorenzo Cobianchi. 2020. "Knowledge in Transition in Healthcare" European Journal of Investigation in Health, Psychology and Education 10, no. 3: 733-748. https://doi.org/10.3390/ejihpe10030054
APA StyleSousa, M. J., Dal Mas, F., Garcia-Perez, A., & Cobianchi, L. (2020). Knowledge in Transition in Healthcare. European Journal of Investigation in Health, Psychology and Education, 10(3), 733-748. https://doi.org/10.3390/ejihpe10030054